
Abstract
This study evaluated the efficacy of a mentoring program on improving psychosocial functioning of young people with a visual impairment (VI). Furthermore, the impact of experimentally matching mentees to mentors with or without VI on youth outcomes was examined. A total of 76 adolescents with VI (15–22 year; 46% boys) were randomized into a yearlong mentoring program (n = 51) or care-as-usual (n = 25). Mentoring involved one-on-one activities within community settings. Psychosocial functioning was improved in all participants during the study (d = 0.35–1.06); however, mentoring outperformed care-as-usual only for autonomy (95% CI: 0.003, 0.31; d = 0.44) and competence satisfaction (95% CI: 0.02, 0.34; d = 0.55), and not for the other six psychosocial outcomes (d < 0.36). Matching similarity was not significantly related to the outcomes assessed. Mentoring was of limited benefit for psychosocial functioning of youth with VI. This trial is registered in the Netherlands Trial Register NTR4768.
Keywords
Introduction
Growing up with a disability requires psychosocial adaptations (Wolman et al., 1994). Compared to the general population, people with a visual impairment (VI) report more psychosocial difficulties across development (Kef, 2002; Nyman et al., 2010; Pinquart & Pfeiffer, 2011). Lower wellbeing was reported by young people with VI compared to their sighted peers, and stronger declines of psychosocial wellbeing were found among adults with VI. Most intervention programs addressing psychosocial functioning of people with VI have been focusing on elderly people, given the heightened incidence of VI in this age group (Nyman et al., 2012). However, psychosocial difficulties during adolescence may have long-term impact on adult development as these may interfere with important developmental issues such as the reconstruction of the autonomous self and individualization from parents or caregivers (Arnett, 2000; Stewart et al., 2014). Therefore, effective interventions addressing psychosocial function of young people with VI are needed. As previous studies showed that mentoring could be effective for increasing psychological wellbeing of youth at risk, this study evaluated the effect of a community-based mentoring program especially designed for adolescents with VI.
Psychosocial functioning
Healthy psychosocial functioning is especially important during adolescence and the transition to adulthood (Arnett, 2000). Adolescence is viewed as a window of opportunity to prevent maladaptive developmental pathways. However, for young people with (visual) disabilities, the transition to adulthood is more complex and of longer duration compared with typically developing youth (Kef, 1999; Stewart et al., 2014). Psychosocial functioning is therefore often used as indicators for adjustment in adolescence (Kef, 1999). Psychosocial functioning is a separate but complementary construct to quality of life, as it also encompasses a person’s ability to interact with others in a mutually satisfying manner (Lam et al., 2011). Outcomes of psychosocial functioning like wellbeing, loneliness, competence, autonomy, relatedness, and self-esteem are closely related to experiences within the social environment. Self-determination theory (Ryan & Deci, 2002) explains how wellbeing and aspects of psychosocial functioning are linked to the social environment. Social-environments that support basic psychological needs (autonomy, competence, and relatedness) stimulate human functioning and development (Deci & Ryan, 2000). Intervening to increase the provision of the three basic psychological needs by the social environment could therefore enhance psychosocial functioning of young people with VI transitioning into adulthood.
Community-based mentoring
A meta-analysis by Nyman and colleagues (2012) examined facilitators of psychosocial functioning among people with VI. Social support was an important predictor of wellbeing, and helped people to accept and cope with their VI. One way to leverage social support for enhancing psychosocial functioning of young people with VI is participation in a community-based mentoring program. Community-based mentoring programs involve a supporting and caring relationship between a non-parental older person and a young person (Rhodes et al., 2006). Positive effects of such mentoring on social and emotional functioning within different risk populations have been repeatedly demonstrated (DuBois et al., 2011; Raposa et al., 2019). This type of supportive relationship is particularly beneficial for enhancing overall wellbeing when youth are involved in an equal, long-lasting, and high quality mentoring relationship (Erdem et al., 2016; Rhodes et al., 2014). Rhodes (2002) suggested that mentoring mentees with mentors might create opportunities for young people to escape daily stress, improve social relationships, and regulate emotions. A sensitive and consistent relationship with mentors can provide young people with a secure base and enable them to be more open to and aware of emotions. Therefore, mentoring could also improve psychosocial functioning.
Mentoring youth with disabilities
Mentoring has been found to be associated with increased self-efficacy and academic success among youth with disabilities (Britner et al., 2006; McDonald et al., 2005; Shpigelman et al., 2009). Only two studies examined the effect of mentoring on young people with VI (Bell, 2012; O’Mally & Antonelli, 2016). The programs in these studies mainly addressed educational and career-related outcomes, and effects of mentoring on psychosocial functioning were not evaluated. In both studies, legally blind mentees were matched to legally blind mentors. It was assumed that mentoring youth with VI would be most effective when mentees and mentors both had the same VI (Bell, 2012; O’Mally & Antonelli, 2016). To the best of our knowledge, only one study experimentally examined the effect of sharing a disability on youth outcomes (Sowers et al., 2016). Adolescents with a variety of disabilities (e.g., Attention deficit disorder/Attention deficit hyperactivity disorder, hearing/visual/physical, or autism spectrum) were randomly assigned to either a mentor with similar disability-related challenges or a mentor without similar disability-related challenges. No significant differences were found between mentees matched to mentors with or without similar disability challenges. While these results did not indicate benefit of matching based on similarity in disability, this hypothesis had not been tested for youth with VI only. Sharing the same disability could be different from sharing the same disability-related challenges. Furthermore, because Sowers and colleagues’ (2016) focused on academic and career outcomes, it is still unclear what the effect of matching on similar disability could do for psychosocial outcomes.
Current study
This current study is part of a larger evaluation study on the efficacy of a community-based mentoring program, called Mentor Support, for adolescents with VI (Heppe et al., 2015; Heppe et al., 2018; Heppe et al., 2019). In a previous report, the efficacy of this community-based mentoring program on social participation outcomes and the effect of match similarity with respect to disability was tested (Heppe et al., 2019). Results showed that randomization to the mentoring program did not benefit adolescents with a VI compared to care-as-usual. A small effect was found between match similarity and one of the social participation outcomes. After the mentoring program was completed, adolescents matched to a mentor with VI were more satisfied with their social support compared to adolescents receiving support from a mentor without VI. Although this report only portraits limited evidence that social participation of youth with VI benefits from community-based mentoring, secondary benefits for psychosocial functioning may still be possible. Especially, since several mentoring studies showed a positive effect of mentoring programs on behavioral, social, and emotional outcomes (DuBois et al., 2011). The primary aim of this current report was to evaluate the efficacy of the mentoring program on psychosocial functioning of adolescents with VI. The secondary aim of this study was to explore the impact of matching mentees with mentors on VI for psychosocial functioning. This investigation of the effect of community-based mentoring on indicators of psychosocial functioning may shed light on possible alternative benefits of mentoring for youth with VI.
Methods
Design
The efficacy of a community-based mentoring program was tested with a randomized-controlled-trial design with two experimental groups and one care-as-usual group. Participants with a VI were randomized in blocks of 15 persons to one of the three groups: (1) the mentoring condition consisting of mentors with VI (VI mentor group), (2) the mentoring condition consisting of mentors without VI (no-VI mentor group), and (3) care-as-usual control group. Stratification on geographic proximity guaranteed equal allocation to country district and curtailed mentors’ travel time to mentees’ homes. An independent researcher used a computerized random number generator to ensure allocation concealment. Trained research assistants who were blind to condition, conducted all fully structured computer-assisted telephone interviews (CATI) at baseline (T1), 12 months (T2), and 18 months (T3) follow-up. Participants in all three conditions were not prevented from receiving their usual care provided by rehabilitation centers in the Netherlands. Prior to the study, the Ethics Committee of the Vrije Universiteit Amsterdam (VCWE.1310.010) approved the study protocol. Furthermore, the study protocol has been registered in the Netherlands Trial Register (NTR4768) and published in Trials an open access peer reviewed journal (Heppe et al., 2015). Reporting is conform to the CONSORT Statement (Moher et al., 2010).
Procedure
Participants for the study were recruited in September 2014 until May 2017. Several recruitment strategies were used: sending out information sheets to potential eligible participants registered at national rehabilitation centers for people with VI in The Netherlands and spreading adverts by social media and online banners. Eligibility for the study was based on country of residence, age (between 15 and 22 years old), having a VI (being blind or partially sighted), comorbidity (no severe additional intellectual, psychological, physical, or hearing disability), and being able to speak the Dutch language. Participants could sign up for the study via the recruitment website, which was especially designed for this study and accessible for people with VI. The first screening of eligibility of participants for the study was via email. This was followed by a telephone interview discussing participants’ needs and desires for participating in a community-based mentoring program. All eligible participants received two documents: an information sheet and consent form via email. Both these documents were also sent to parents if eligible participants were under the age of 18 years. Within the information sheet, the study design and the allocation process to one of the three conditions of the trail was thoroughly explained. Before signing the consent form, any questions participants or parents had were answered over the phone or via email. Participants could sign the consent form by filling out their name, the date, and placing and X on the consent form after the word Signed. This process of signing was approved by the Ethics Committee of the Vrije Universiteit Amsterdam, as manually signing could be challenging for people with VI.
After provided consent and before the start of mentoring program, all participants participated in the first interview (T1) by the use of CATI. After this baseline measurement, participants were randomly allocated to one of the three study conditions of the trail. Randomization results were shared with participants in different ways, depending on group of allocation. Participants allocated to one of the mentoring conditions (n = 51) received an email that welcomed them to the mentoring program and with additional information about the matching process. Participants assigned to the care-as-usual control group (n = 25) were informed about the randomization results over the telephone and via email. This randomization process and matching mentees to mentors was all performed within 1 month after baseline measurements were completed. Matching procedures were based on three criteria: (1) randomization (mentor with or without VI), (2) geographic proximity of the homes of the mentor and the mentee, and (3) having similar interests. Mentees and mentors were introduced to each other via email. The first group of participants started with the community-based mentoring program in May of 2015 and a second group started in November of 2015. All participants from both mentoring conditions and the control group were invited for a second post-interview interview after 12 months (T2). The third and last measurement with all three conditions took place after 18 months (T3). All three measurements were performed by extensively trained and blinded research assistants. Figure 1 shows participants flow of all participants through the study. Matching on the first criteria (randomization) was not always possible due to the low incidence of people with VI. Therefore, data of nine mentor–mentee dyads were excluded from analysis on the effect of match similarity on psychosocial outcomes.
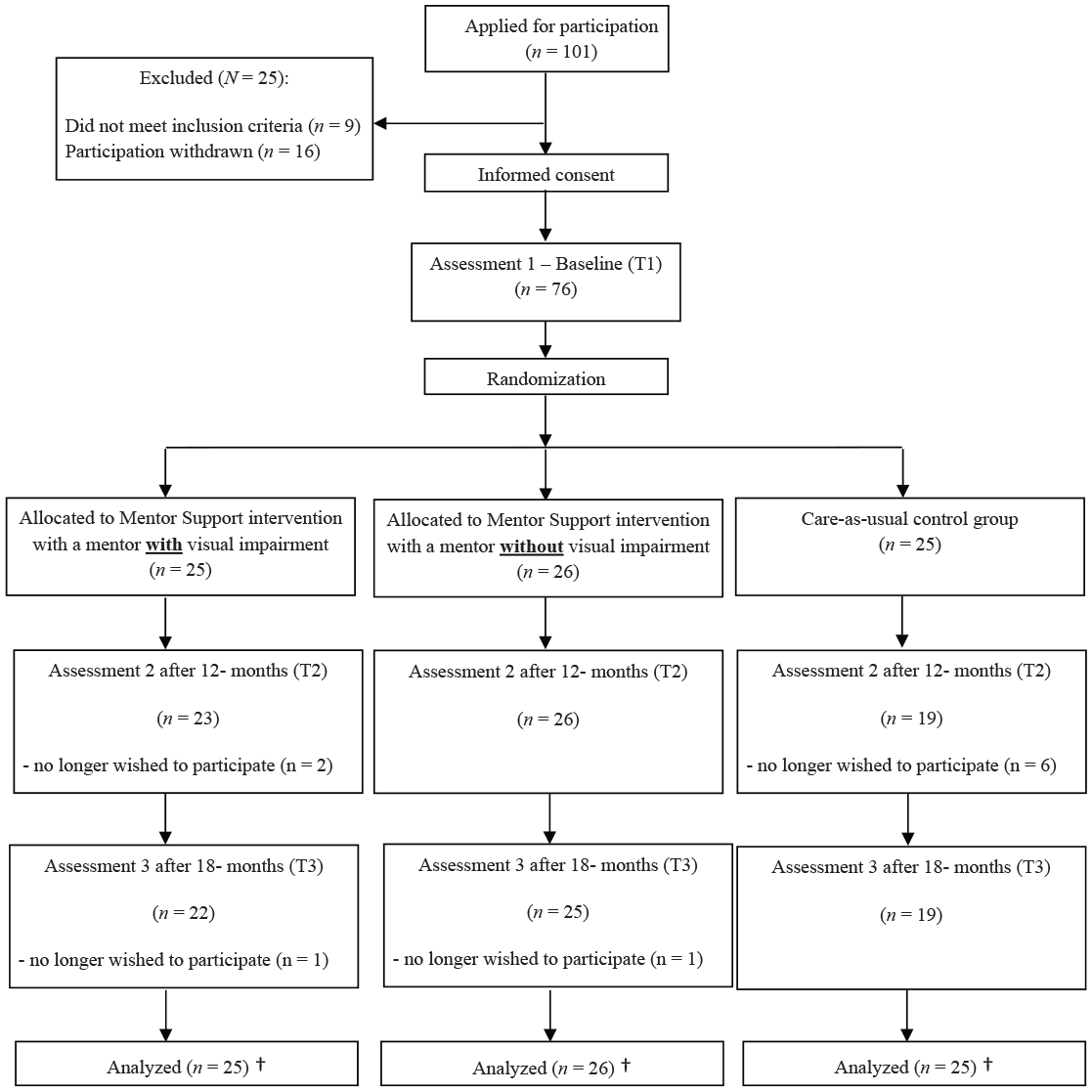
Participant flow through study.
Participants
The age of the participants (54% female) randomized into the three conditions of the trial ranged from 15 to 22 years (M = 18.45; standard deviation [SD] = 2.01; N = 76). VI meant legal blindness for 40% of the sample and severe VI for 33%. VI was present at birth for 70%, with 49% developing VI due to an inherited condition. For 51%, no comorbid problems were reported. A minority of 33% never received special education, and 29% held a paid job. Participants in the three randomized conditions did not significantly differ on any of these background characteristics (p > .05). The sample size of 76 yielded sufficient statistical power (.80) to detect a within (pretest–posttest–follow-up) by between (VI mentor, no-VI mentor, care-as-usual) interaction effect of d = 0.57 or more (using G*power v3.1.9; Faul et al., 2007).
The community-based mentoring program
The community-based mentoring program, called Mentor Support, was developed using the Elements of Effective Practice for Mentoring (EEPM) and was similar in both mentoring conditions of the randomized controlled trail. Mentor Support consisted of monthly face-to-face meetings between a participant (mentee) and a mentor over a period of 12 months (number of meetings; M = 6.45; SD = 4.28). These match meetings took place in or near the home of the mentee. The mentoring program did not contain a mandatory program, and content was self-designed. Positive thinking and having success experiences during their joined activities were the focus of every match meeting. Performed activities during the match meetings were mainly based on the mentees’ own interest or goals within one of the domains of social participation (school/work, leisure activities, and social relationships). Examples of activities are going to a concert or theater, inviting friends over for parties or diners, participating in cooking- or pottery-workshops, trying new sports like fitness, yoga, or duo-carting. A community-based mentoring handbook, specifically designed for mentoring youth with a VI, listed several exercises and ideas for activities. None of the materials provided to the mentor–mentee matches contained obligatory activities. Mentor–mentee dyads received a budget of 420 euros to support the costs of their activities performed during the mentoring program above and beyond an unlimited budget for traveling costs. Furthermore, mentees and mentors had weekly contact via telephone calls, WhatsApp, or email. During these contact moments, the mentors’ role was to listen, support, and guide the mentee when problems occurred within daily routine situations and give advice, if needed, by suggesting different kind of coping strategies for handling stressful situations.
Volunteers could be included as mentors when they met the inclusion criteria for being between the age of 18 and 45 years, having a high level of social participation, no mental health illness, and not in the need of searching new friends or being overcommitted. Volunteers that wanted to become a mentor signed up for the community-based mentoring program via the recruitment website. Advertisements about the mentoring program were placed on social media platforms, volunteer organization, brochures, and advertisement in newsletters. All mentors received pre-match mentoring training after they passed the first selection process of being questioned over the telephone, using a highly structured in-depth interview protocol. The content of this selection interview protocol was also based on the EEPM. It contained questions on a volunteer’s thought, ideas, and experiences with community-based mentoring (e.g., expectations of being a mentor, understanding the responsibility of being a mentor, ideas on how to establish a strong and long-lasting mentoring relationship, level of commitment to the program). The second part of the selection process, the pre-match mentor training, consisted of a 2 day, 4 hr in person workshop. Within the workshop, volunteers received information about the mentoring program, having a VI, rules within the mentoring program, and filled out several questionnaires. Furthermore, volunteers practiced their mentor relational and conversional skills by exercises with role-playing methods. Besides succeeding this training workshop, volunteers had to submit a certificate of good conduct from their town council and sign the consent form before they were eligible to participate as mentors. No material incentives were provided to mentors in this study. After this thorough selection procedure, 50 mentors were eligible to participate in the community-based mentoring program and could be matched to a mentee. During the matching process, three more mentors were excluded from the study because of long travel distance to all mentees. Some mentors were matched to more than one mentee. Of the final group of mentors (n = 47), 40% was male. Their age ranged between 22 and 44 years (M = 31.64; SD = 6.53), and 17% were unemployed. Of the mentors with a paid job, 34% of them were educated or working in a helping profession. Furthermore, two-thirds of the mentors were involved in a romantic relationship and 28 mentors were visually impaired.
Measures of psychosocial functioning
Wellbeing was assessed using a Dutch translation of the Cantrill Wellbeing measure (Cantrill, 1965). This questionnaire consists of one item asking “How do you feel in general?” which can be answered on a 10-point response scale ranging from 1 meaning “feel really bad” to 10 meaning “feel really good.” Higher scores on this scale indicated higher levels of wellbeing.
Loneliness was assessed using an 11-item scale (De Jong Gierveld & Van Tilburg, 1999). The questionnaire consisted of items with a negative emotional valence assessing absence of relationships (e.g., “I miss having a really close friend”), and items with a positive valence assessing feelings of belongingness (e.g., “There is always someone I can talk to about my day-to-day problems”). Questions were answered on a three-point rating scale ranging from 0 for “yes,” 1 for “more or less,” and 2 for “no.” Responses of “more or less” were dichotomized to either “yes” or “no” depending upon the direction of the items (negative or positive). Item responses were summed with scale scores ranging from 0 (complete absence of loneliness) to 11 (no social embeddedness at all). In the current sample, the internal consistency of the questionnaire at each of the three assessment times was excellent, α: T1 = .86, T2 = .85, and T3 = .83. In a previous study among adolescents with VI (n = 316; M age: 18 years), the internal consistency was also good (α = .78) (Kef, 1999).
Self-determination was assessed with the Basic Psychological Needs Satisfaction and Frustration Scale measuring satisfaction of the three basic psychological needs (Chen et al., 2015). This 24-item questionnaire assesses both satisfaction and frustration of the three basic psychological needs defined in Self-determination Theory, namely autonomy, relatedness, and competence. Each psychological need was assessed using a total of eight items with four being positive in valence (e.g., for autonomy satisfaction “I feel a sense of choice and freedom in the things I undertake”) and four being negative in valence (e.g., for autonomy frustration “I feel forced to do many things I wouldn’t choose to do”). Questions were answered using a five-point rating scale ranging from 1 for “completely untrue” to 5 for “completely true.” All negative items were reverse scored, and mean scores were computed for each of the three subscales. Higher scores on each of the three scales indicated greater satisfaction with basic psychological needs. The internal consistency for each scale of psychological needs was good at each of three time points, α for autonomy satisfaction: T1 = .76, T2 = .75, and T3 = .81; α for relatedness satisfaction: T1 = .78, T2 = .80, and T3 = .80; and α for competence satisfaction: T1 = .77, T2 = .77, and T3 = .76. In a previous study among typically developing adolescents (n = 685; M age = 17 years), the internal consistencies were also acceptable and ranged between .64 and .89 (Chen et al., 2015).
Self-concept was measured by three questionnaires: (1) self-esteem questionnaire, (2) acceptance of the impairment questionnaire, and (3) perceived self-competence questionnaire. Self-esteem was assessed with a Dutch version of the Rosenberg Self-esteem Scale (Rosenberg, 1979). This questionnaire consists of 10 items such as “On the whole, I am satisfied with myself.” All items were answered on a four-point rating scale ranging from “strongly agree” to “strongly disagree.” A mean score was computed and used in the analyses with higher scores reflecting higher levels of self-esteem. The internal consistency of the questionnaire at each of the three assessment times was excellent, α: T1 = .88, T2 = .89, and T3 = .85. In a previous study among adolescents with VI (n = 316; M: 18 years), the internal consistency was also good (α = .83) (Kef, 1999).
Acceptance of impairment was assessed with a nine-item subscale of the Nottingham Adjustment Scale (Dodds et al., 1991). An example of an item is “I feel bad when I realize what sighted people can do and what I can’t do.” Questions were answered using a five-point rating scale ranging from 1 for “strongly disagree” to 5 for “strongly agree.” Based on the requests of participants in previous studies of this population in the Netherlands, an item with a positive valence was added to the questionnaire: “My visual impairment is part of me, but doesn’t determine what I do or think” (Kef, 1999). A mean score of all 10 items was used in the analyses, with a higher score indicating greater acceptance of the VI. The internal consistency of the questionnaire at each of the three assessment times was excellent, α: T1 = .88, T2 = .89, and T3 = .85. In a previous study among adolescents with VI (n = 316; M: 18 years), the internal consistency was also good (α = .83) (Kef, 1999).
Perceived self-competence was assessed with the Self-Perception Profile for Adolescences (Harter, 2012). The scale consists of four subscales with a total of 20 items. Each item consists of two opposing statements, measuring social competence (e.g., “Some teenagers find it hard to make friends BUT other teenagers find it pretty easy to make friends”), physical appearance (e.g., “Some teenagers are not happy with the way they look BUT other teenagers are happy with the way they look”), close friendship (e.g., “Some teenagers are able to make really close friends BUT other teenagers find it hard to make really close friends”), and romantic appeal (e.g., “Some teenagers feel that they are romantically interested in someone, that person will like them back BUT other teenagers worry that when they like someone romantically, that person won’t like them back”). Questions were answered in two steps. First, participants were asked to decide which kind of teenager he or she is most like; second, they were asked to decide whether the description was “really true for me” or “sort of true for me.” Each response was scored on a four-point rating scale, where the score of 1 indicated the lowest perceived self-competence and the score of 4 indicated the highest level of perceived self-competence. A mean score of the four subscales (20 items) was calculated with higher scores reflecting higher levels of perceived self-competence. In the current sample, the internal consistency at each of the three assessment times was acceptable, α: T1 = .75, T2 = .66, and T3 = .75. In a previous study among typically developing adolescents (n = 146; M age: 17 years), the internal consistency was also good (α = .88) (Harter, 2012).
Results
Plan of analyses
Variables were checked on outliers and skewness. No outliers were found, but moderate negative skewness was detected, indicating relative high scores on the variables of wellbeing, self-esteem, perceived self-competence, relatedness satisfaction, and competence satisfaction (ranging from −1.07 [standard error (SE) = .17] to −.39 [SE = .17]). The loneliness scale was positively skewed (.91, SE = .17), pointing to the high frequency of low scores on this scale.
In this longitudinal study with a nested data structure, growth modeling with multilevel analyses in SPSS Mixed Models was used to study individual change in psychosocial functioning over time (IBM SPSS, Armonk, NY; Statistics version 23). The nested structure refers to the repeated measurements (level 1) that were nested within individuals (level 2). Mixed models refer to a model with predictors and outcomes at both levels. Growth modeling allows the estimation of individual trajectories of change, so that not only mean change but also individual variation in change can be assessed. Individual variation is relevant because we were interested in the associations between predictors and individual differences in baseline and rate of change over time. Intra-class correlations, indicated intra-individual dependency, exceeded .05, and design effects were larger than 2.0, warranting the use of multilevel modeling (Peugh, 2010).
In our study, the multilevel model explained the dependency among measurement points (level 1) within individual mentees (level 2). The intercept was estimated as a random effect. Three models were specified. First, time was added as a random effect to test random slopes. Random intercepts and slopes were specified to model inter-individual variation at baseline and in change in psychosocial functioning over time. Second, condition (mentoring vs control condition) and the interaction between condition and time were entered into the model, to test the effect of the mentoring program on the slope (change over time). Third, the procedure was repeated with the three group variable of condition (VI mentor group and control group, vs no-VI mentor group). All analyses were performed for each outcome separately.
Estimators of individual growth curves were bootstrapped (i.e., stratified method, percentile confidence intervals) to compensate for non-normality and low statistical power. Multivariate bootstrapped statistics were only interpreted when the deviance statistic indicated significant model fit improvement. Results were interpreted as significant when the 95% confidence interval excluded the value of zero.
Preliminary analysis
Table 1 provides means and SDs of the dependent psychosocial functioning and self-determination outcomes. Participants in the three intervention arms did on average not differ on dependent variables. The exception was that participants randomized to the mentoring intervention groups had significantly lower levels of competence satisfaction at baseline than in the control group.
Mean score and standard deviations of psychosocial functioning of both conditions, at the first assessment (T1), after 12 months at the second assessment (T2), and after 18 months at the third assessment (T3).
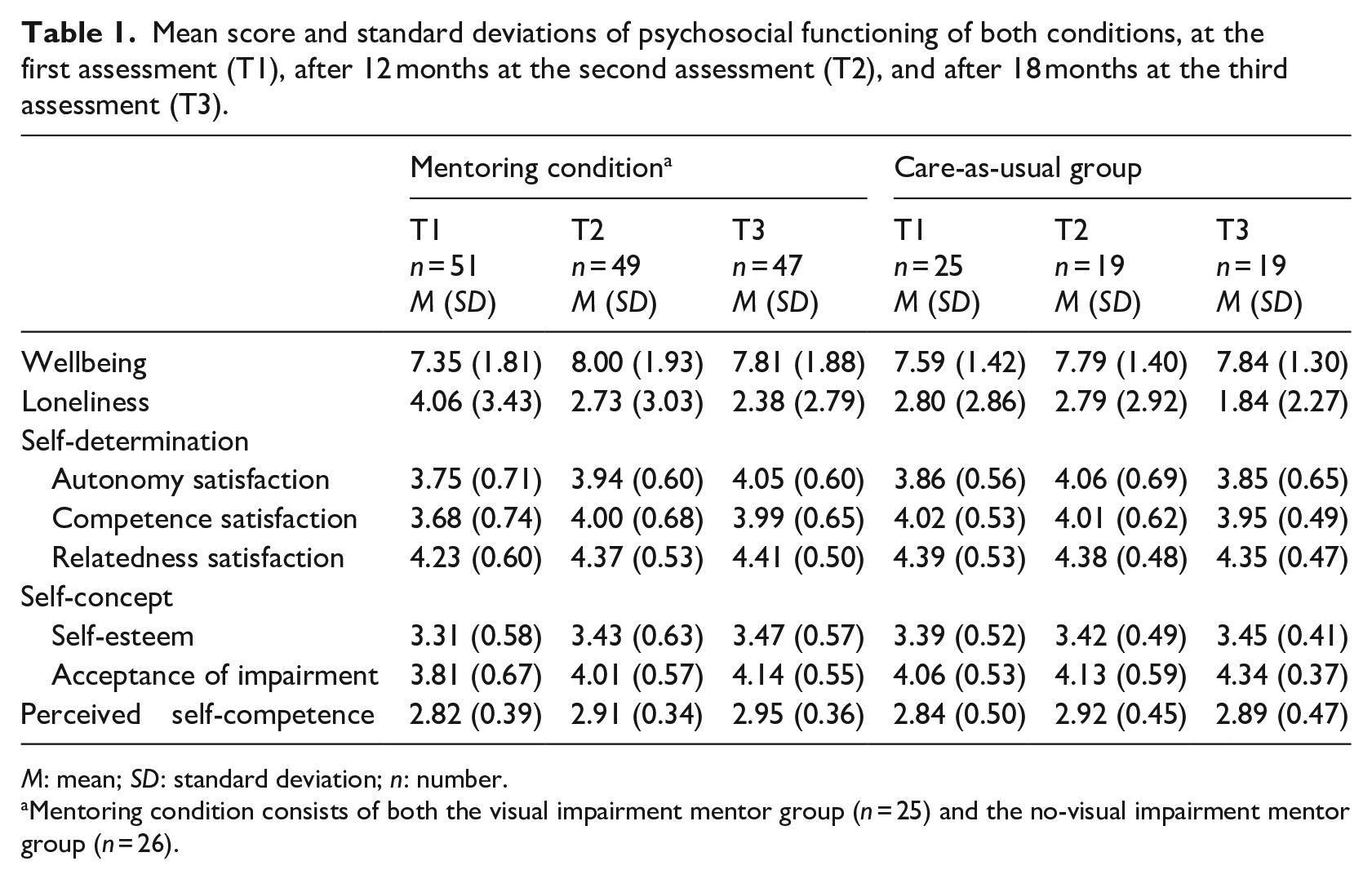
M: mean; SD: standard deviation; n: number.
Mentoring condition consists of both the visual impairment mentor group (n = 25) and the no-visual impairment mentor group (n = 26).
Psychosocial functioning outcomes
Effect of time
Table 2 shows increases from baseline to follow-up in wellbeing, self-esteem, acceptance of the impairment, perceived self-competence, autonomy satisfaction, and competence satisfaction. These increases, irrespective of randomization to either one of the three conditions in the trial, showed moderate to large effect sizes (Cohen’s d = 0.35–1.06). Satisfaction of the basic human need to relatedness did not change (d = 0.45, non-significant) across the arms of the study.
Parameter estimates for multilevel model of evaluation of the community-based mentoring program on psychosocial functioning.
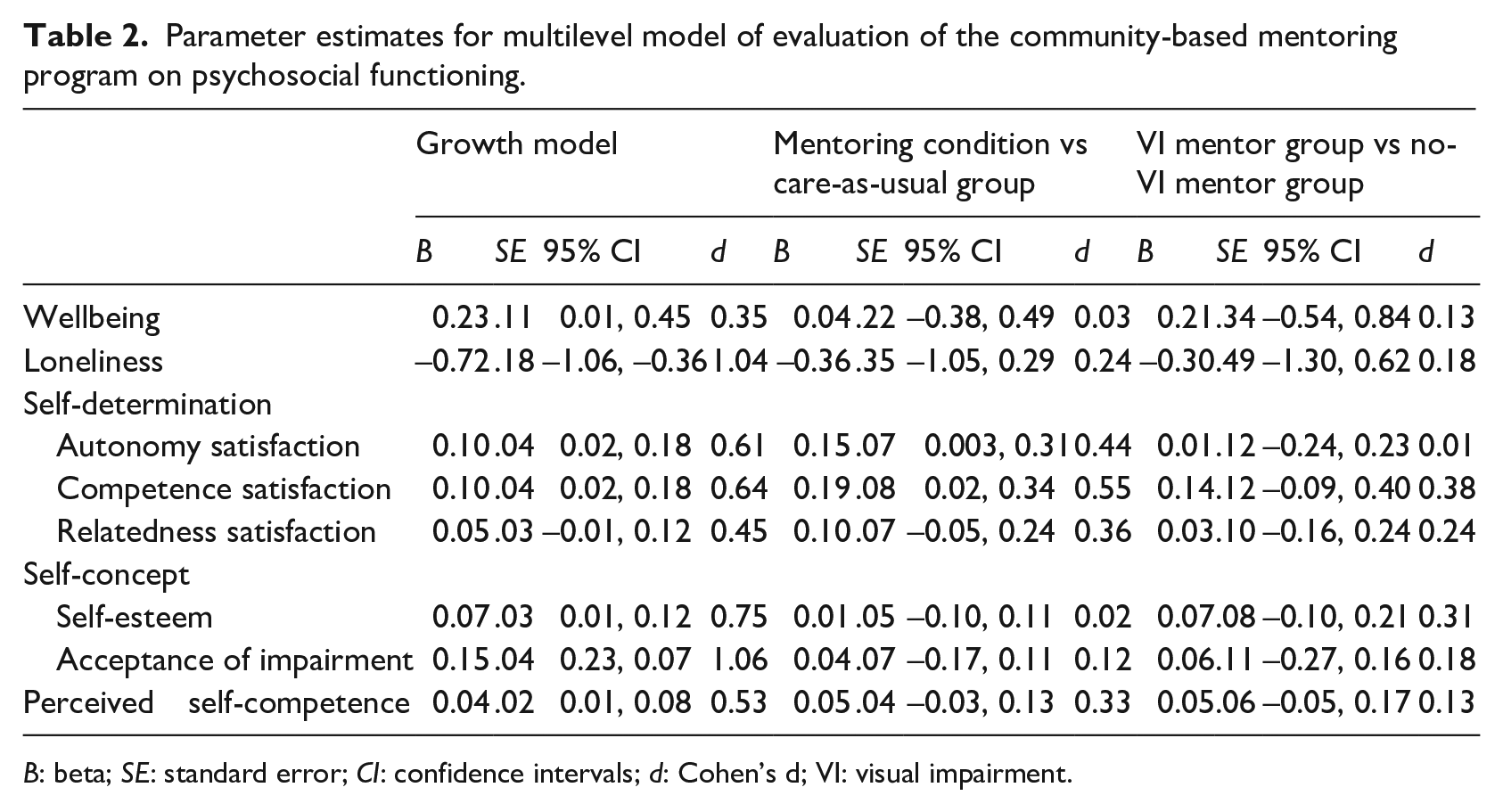
B: beta; SE: standard error; CI: confidence intervals; d: Cohen’s d; VI: visual impairment.
Effect of intervention
Randomization to one of the intervention conditions over care-as-usual increased satisfaction of basic need for autonomy and for competence independent of the overall growth. Effect sizes were in the small to moderate range (Cohen’s d = 0.44–0.55). Table 2 shows that no intervention effects were statistically significant on change in the other dependent variables (d = 0.02–0.36; not significant).
VI of mentors
No significant effects were found of randomization to either mentors with VI or mentors without VI. This was the case for all dependent variables (Cohen’s d = 0.01–0.38; not significant).
Discussion
Regardless of study group, all mentees reported significant and moderate to strong improvements on most psychosocial outcomes during the study period of 18 months. For autonomy and competence satisfaction, improvements in outcomes were even stronger for mentees participating in a community-based mentoring program compared to the care-as-usual control group: but effect sizes were small. Except for these two outcomes, this community-based mentoring program did not outperform care-as-usual on a wide array of psychosocial functioning outcomes, including wellbeing, self-esteem, acceptance of the impairment, perceived self-competence, loneliness, and relatedness satisfaction compared to care-as-usual. The overall efficacy of this mentor program for improving the psychosocial functioning of youth with a VI is therefore comparable to care-as-usual.
Furthermore, no differences were found for psychosocial functioning between mentees matched to mentors with or without VI. This means that matching young people with VI to mentors with VI did not enhance the efficacy of the community-based mentoring program compared to mentees matched to mentors without VI. This pattern of results is consistent with one earlier study examining the effect of matching mentees to mentors who shared the same disability challenges (Sowers et al., 2016). Matching based on other outcomes such as sharing the same attitude, interests, or personality traits might possibly result in a more powerful effect (Eby et al., 2013; Raposa, Ben-Eliyahu, et al., 2019). More research is needed on other populations of youth with disabilities to determine whether this pattern is generalizable to the impact of disability matching of mentors and mentees on youth outcomes or whether it is specific to this population. For example, disability matching should be examined for other specific disabilities such as having a hearing impairment, physical disability, or intellectual disability.
The tentative positive findings for the enhancement of two of the psychological needs are consistent with earlier findings of the positive effect of mentoring on psychological functioning in mentored youth. A meta-analysis conducted by DuBois and colleagues (2011) showed that the average small effect size of mentoring programs within the category of psychological/emotional outcomes (e.g., depression and self-esteem) was positive and did not significantly vary in magnitude from other categories such as academic/school and social/relational outcomes. Other studies have emphasized that mentoring relationships foster needs related to autonomy and competence satisfaction (Britner et al., 2006; Larose et al., 2005). Mentoring programs encourage mentees to make autonomous decisions in the context of the relationship, given mentees practice and feedback regarding their decision-making skills. For example, mentors are typically trained to solicit and honor the goals and preferences of mentees when setting up match meetings and activities. These cumulative experiences combined with performing activities with a mentor adds to the experiential basis on which mentees assess their own competence.
One possible explanation for the lack of superiority of the mentoring program for the other psychosocial outcomes could be reactivity among adolescents randomized to the care-as-usual control group. Almost 74% of the control group received care-as-usual provided by one of the Dutch national rehabilitation centers. In addition, 73% of the control group sought other forms of social or professional support. For example, 21% of the control group received psychological counseling. Seeking alternative support in randomized control groups has been observed in other trials as well (e.g., Petersen et al., 2014; Scholten et al., 2013) and diminishes the power of the control group design to detect experimental effects. Nevertheless, all participants improved on psychosocial outcomes during the study, indicating that adolescents with VI are amendable for different kinds of interventions. Although it is unclear in the current study how much the additional support in the control group may have attenuated the effect, the active support seeking completed by the control group underscores the need for support in adolescents with VI.
Most psychological interventions, like cognitive behavioral therapy or positive psychology interventions tested in randomized controlled trials, do outperform wait-list or care-as-usual controls (e.g., Hoffman et al., 2007; Sin & Lyubomirsky, 2009). However, often effect sizes are relatively small and most interventions do not outperform each other (Cuijpers et al., 2008). Common factors as therapeutic alliance, clear rationale about developed problems, and belief in treatment are possible explanations for finding equal effects. Within the mentoring literature, the strength of the mentoring relationship, a concept that is related to the therapeutic alliance, has also been shown to be a key factor for determining program effectiveness (Erdem et al., 2016; Rhodes et al., 2014). Further research might examine possible moderation of program effectiveness by mentoring relationship quality, as well as variation in allegiance toward mentoring as a viable intervention among mentors and mentees. Community-based mentoring programs are less well known in Europe compared to North America, and therefore, program participants may be more skeptical and less engaged in them.
Several limitations should be kept in mind when interpreting the study findings. First, recruitment yielded too few participants to achieve the a priori statistical power level that was set by the investigators, a problem that plagues randomized controlled trials frequently (Moher et al., 1994). Second, although severe comorbidity was an exclusion criteria for the study, 49% of the adolescents who participated in the current study did have one or more mild comorbid problem. Comorbidity may have introduced additional psychosocial challenges that could not be sufficiently addressed by a mentoring program utilizing unpaid volunteers.
Given these constraints, the current study should not be the end for exploring how mentoring programs may enhance psychosocial functioning in young people with disabilities. More insight is needed in the way care-as-usual facilitates the psychosocial development of young people with VI, and in what way a mentoring intervention could possibly outperform this kind of support and be of added value to care-as-usual. This study shows that community-based mentoring is as effective as care-as-usual, often consisting of intensive one-on-one treatment, in The Netherlands. Therefore, future research might examine who benefit the most from a community-based mentoring program and the cost-effectiveness of community-based mentoring programs for youth with VI. Research might also explore differences between care-as-usual in different countries. In the current study, adolescents received support from rehabilitations centers specialized in supporting people with VI. Possibly, the care provided by these centers is different in intensity, frequency, modality, or content than the care provided in other countries. Trials showing a positive effect of mentoring in predominantly US samples, control groups may receive less intense, frequent, in-person, or diverse care-as-usual services than the care-as-usual services received by youth in this current study.
From a practical perspective, other approaches toward mentoring might be explored to enhance psychosocial functioning. Establishing matches within peoples own social networks and age groups may yield more robust matches than matching people who come from unfamiliar social worlds. Within informal mentoring programs, youth are encouraged to recruit role models from their existing social networks (Schwartz et al., 2013). This type of youth-directed informal mentoring reduces the risk of relationship failure due to the fact that mentors are already familiar with the personal and contextual setting of the mentee, and therefore, matches may be more similar in ways that are central to the mentee’s goals and interests. Providing support in how to overcome barriers for young people with VI (Kef, 1997; Kef et al., 2000) toward enhancing social capital might benefit their psychosocial functioning.
In sum, the findings of the current study tentatively suggest that a community-based mentoring program may be more beneficial on autonomy and competence satisfaction compared to care-as-usual. However, the program did not outperform care-as-usual on a wide range of other psychosocial outcomes. Although there are many salutary effects of mentoring, it should continue to be examined in cross-cultural experimental studies in terms of its effectiveness as a strategy for enhancing psychosocial functioning of youth with VI in fully powered studies with larger samples and using well-designed control group(s).
Footnotes
Acknowledgements
The authors wish to thank the two national Dutch rehabilitation centers (Bartimeus and Royal Dutch Visio) for supporting us with the recruitment of participants. In addition, we would like to thank our research assistants for assisting with the data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Grant 94309005 by two organizations: Bartimeus Fonds and ZonMw, the Dutch organization for Health Research and Development, program InSight.