
Abstract
Cerebral visual impairment (CVI) is one of the most common causes of visual impairment in children. CVI is a complex visual disorder to understand and explain to others. Understanding one’s diagnosis and being able to explain it to others may facilitate adaptive functioning. To educate children and young people on their CVI and accompanying needs, the computerized psycho-educational programme ‘My CVI’ has been developed.
A mixed-methods study was conducted to evaluate the effect of this programme. The aims of the programme are to increase participants’ knowledge of CVI, as well as self-esteem (SDQ), adaptive coping (SCQ), and well-being (Cantril, PERIK, HRQoL). Thirty-nine children (aged 7–16 years; 51% boys) participated in a pre-test, post-test, and follow-up assessment. Qualitative interviews were conducted for a subjective evaluation of the programme.
Participation in the psycho-educational programme resulted in increased knowledge of CVI, as well as a better teacher-reported social and academic self-concept and less self-reported feelings of social exclusion. No effects of participation were found on self-reported self-esteem, coping or other measures for well-being. An increase in knowledge of CVI was not associated with changes in psychosocial functioning. Qualitative data revealed that children enjoyed participating in the programme; they learned there are others with CVI, and gained more knowledge and practical tools on how to deal with their CVI.
The results provide preliminary evidence that participation in the psycho-educational programme ‘My CVI’ increases children’s knowledge of their visual impairment as well as improves social outcomes and feelings of inclusion. The highest gains may be achieved through a personalized approach, depending on a child’s (developmental) age and parental involvement.
Keywords
Introduction
Cerebral visual impairment (CVI) is an increasingly common cause of visual impairment in children (Ben Itzhak et al., 2020). Around one-third of visual impairment in children in the developed world can be attributed to CVI (Ozturk et al., 2016). This impairment has increased over the past decades because of the increased survival rate of very premature infants (Kozeis, 2010). CVI is not a single disorder, but encompasses a spectrum of visual disturbances caused by brain damage or abnormal brain development. These disturbances are not explained by any (possibly co-occurring) eye-damage (Sakki et al., 2018). With the same diagnosis, different children with CVI can vary widely in what they can see (Ben Itzhak et al., 2022). In addition, their vision may vary depending on the circumstances of the child (e.g., tiredness) or the surroundings (e.g., level of illumination) (Roza et al., 2017). Because of this variability in what children with CVI can see, CVI is a complex visual disorder to understand and explain to others. Indeed, it has been found that sighted people have more difficulty understanding people with low vision than blindness (Roy & MacKay, 2002). This may be even more true for low vision caused by CVI compared with other visual impairments, because of its complex and diverse manifestation.
Children with visual impairment have sometimes been found to have lower self-esteem than their sighted peers (Augestad, 2017). This lower self-esteem can be explained by different challenges these children face in life, such as difficulties in understanding their impairment and abilities (Sacks, 2010), or lack of acceptance of one’s visual impairment (Dale et al., 2022). Which is also related, as one needs to understand one’s impairment to be able to accept it. Acceptance of oneself is a prerequisite for positive self-esteem, which is important for mental health and quality of life (Bolognini et al., 1996). In addition, young people with visual impairments are at a slightly higher risk to apply less adaptive coping skills, which in turn is associated with lower well-being (Kef, 2002). In general, understanding of the diagnosis facilitates coping with the associated impairment (Shilubane & Mazibuko, 2020).
A thorough understanding, and acceptance, of one’s visual impairment helps others to feel at ease and provides opportunities to establish positive relationships (Sanford & Burnett, 2006). In addition, this understanding of the impairment is important to be able to communicate this information on the visual impairment and associated needs to others (Guerette et al., 2011), which in turn facilitates children’s self-esteem (Sacks, 2006), as well as their adaptive coping (Kef, 2002). However, CVI is not only a difficult diagnosis to understand for the child him or herself, but also difficult to explain to others (Jackel, 2019). This can complicate building understanding social relationships, which are essential for psychological health and well-being (Nestmann & Hurrelmann, 2012). In addition, positive, understanding relationships with others have been associated with positive self-esteem (Augestad, 2017) and can help individuals cope with their impairment (Kef, 2002).
As CVI is a difficult diagnosis to understand and therefore also difficult to explain to others (Dutton & Jacobson, 2001), having CVI puts children at risk for maladaptive development. Increasing children’s understanding of their visual impairment may counter this negative trend. To educate children and young people on their CVI and accompanying needs, the computerized psycho-educational programme ‘My CVI’ has been developed.
Current study
In the current study we study the effect of ‘My CVI’. We hypothesized that participating in the psycho-educational programme would lead to (1) significant improvements in knowledge of CVI (primary outcome) and (2) improved self-esteem, adaptive coping and well-being (secondary outcomes). In addition, qualitative interviews were conducted with a subset of children, parents, and teachers to gather information on their subjective evaluation of the programme and the child’s functioning.
Method
Design
This study uses a mixed-methods design with quantitative pre-test, post-test, follow-up analyses of questionnaire responses from children and teachers. These data are supplemented with qualitative interviews with children, parents, and teachers for a more in-depth understanding of their experiences with the psycho-educational programme.
Participants
Participants were recruited at three organizations, specialized in care for visual impairments in The Netherlands and Belgium. Thirty-nine children, and for 29 children also their teacher, participated in the quantitative part of the study. The children were between 7 and 16 years of age (Mage = 10.8, SDage = 2.2), and 51.3% (n = 20) were boys; 61.5% of the children (n = 24) were enrolled in primary education (50% mainstream, 50% special education) and 38.5% in secondary education (n = 15; 40% mainstream, 60% special education). The degree of teacher-report was only associated with whether the child was enrolled in primary or secondary education; with no missing teacher-report of young people in secondary education and 41.7% missing report of teachers of children in primary education (χ2 = 8.41, p = .004). Most children had diagnosed CVI (90%), the other 10% (n = 4) had symptoms of CVI and were being evaluated to be diagnosed with CVI; 79.5% of participating children had additional impairments besides their visual impairment (54% physical impairment [ranging from hypermobility to cerebral palsy], 13% developmental delay, 8% Autism Spectrum Disorder, 5% ADHD, 5% hearing impairment and 26% other not further specified impairment). Of these 39 children, 15 children, 10 parents, and 10 teachers were randomly selected and approached for participation in a qualitative interview. Of these respondents, 13 children, 7 parents, and 7 teachers agreed to participate, providing information on a total of 17 children (see Table 3 for a description of this subsample).
Ethics approval
Approval for this study was obtained from the ethics committee of Vrije Universiteit, Amsterdam, Faculty of Behavioural and Movement Sciences (VCWE-2020-132). Written informed consent was obtained from the parents of the participating children. Verbal informed consent was obtained from all parents and teachers prior to the interview.
Psycho-educational programme ‘My CVI’
‘My CVI’ is a web-based psycho-educational programme (https://mijncvi.nl/en/), developed for children with CVI with a developmental age between 6 and 14 years. The programme consists of eight modules and can be done free of charge on an iPad or laptop/computer. The programme starts with a module on what CVI is and the other modules focus on practical aspects of this diagnosis such as ‘reading’, ‘the use of visual aids’ or ‘recognizing emotions’. Five young people diagnosed with CVI (3 girls, 2 boys; 4 Western European background, 1 Asian background) talk in short video clips about their experiences, followed by quiz questions. By participating, children and young people learn about CVI in general, but also about how CVI affects their lives. Participants select video clips in which they recognize their struggles related to their CVI and save these in a personal playlist. The videoclips in this playlist can be used to show to others (e.g., family members, teacher) to help explain the impact and practical implications of CVI; see Figure 1 for an impression of this personal playlist. Each module takes about 10–15 min to complete and participants are advised to finish one module every week. Overall, children managed to adhere to this schedule, shown in a mean period of less than 3 months between pre-test and post-test (M = 2.84, SD = 1.90).
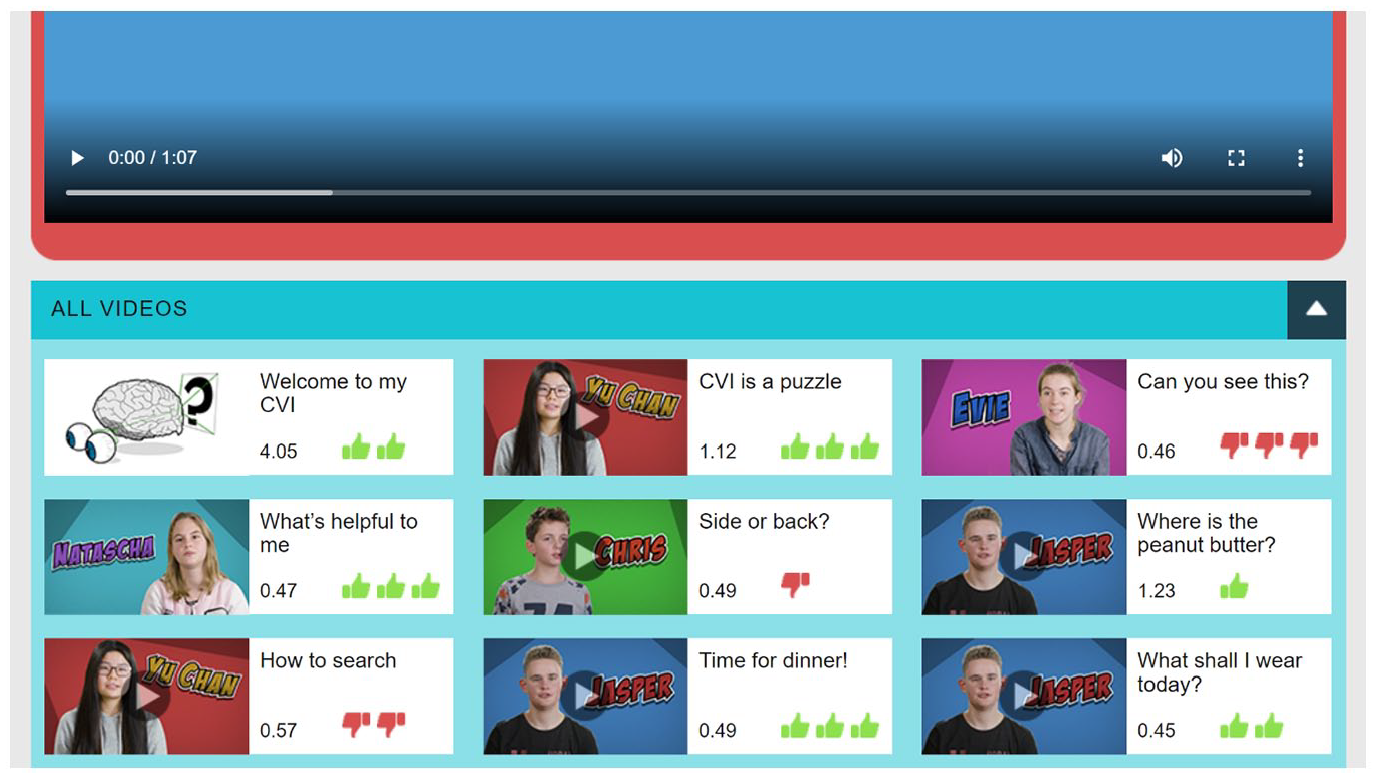
Print screen of personal playlist. After watching each videoclip, participants rate how recognizable they find this videoclip for their own situation by selecting 1–3 thumbs up or thumbs down.
Procedure
Data collection began in May 2019 and ended in February 2022. The first assessment took place before the start of the psycho-educational programme. A research assistant contacted the children at school, at home or digitally to fill out the questionnaires together. After the pre-test the children started with the programme ‘My CVI’. After finishing the psycho-educational programme (±2–3 months later), children were asked to fill out the same questionnaires again with the help of a research assistant. In addition, a random selection of the children, their parents, and teachers were contacted and asked for their willingness to participate in a qualitative interview. Three months after the post-test, children were contacted for the last time to complete a follow-up assessment. At these same three moments, teachers were asked to fill out online questionnaires.
Measures
Quantitative data
Primary outcome measure
Knowledge of CVI
To assess whether children learned more about their CVI after participating in the psycho-educational programme, they indicated for 20 statements on CVI whether they thought this statement was correct (thumbs up), incorrect (thumbs down) or they did not know whether the statement was correct (question mark). An example of a statement was ‘When children with CVI are tired, they have more difficulty with perceiving their surroundings. Do you think this is correct?’ The responses were recorded as correct (+1) or incorrect (−1). If the children did not know the answer (0), this was also recorded. A higher score means more knowledge of CVI.
Secondary outcome measures
Self-esteem of the participants was assessed with the Self-Description Questionnaire (SDQ; Marsh et al., 1998). Both teachers and children filled out this questionnaire. On a 4-point scale, participants reported on the child’s social self-concept (e.g., ‘I have/This child has more friends than other children’), academic self-concept (e.g., ‘I perform/This child performs well in different school tasks’) and general self-concept (e.g., ‘In general, I like who I am/ this child likes who he or she is’). Higher scores stand for a more positive self-concept. Internal consistency was adequate to good (see Table 1 for all internal consistency scores) and comparable to previously reported scores (Verschueren et al., 2012).
Means and standard deviations of outcome variables at three assessments (observed data), and effect statistics. Reliability of the questionnaires is also reported.
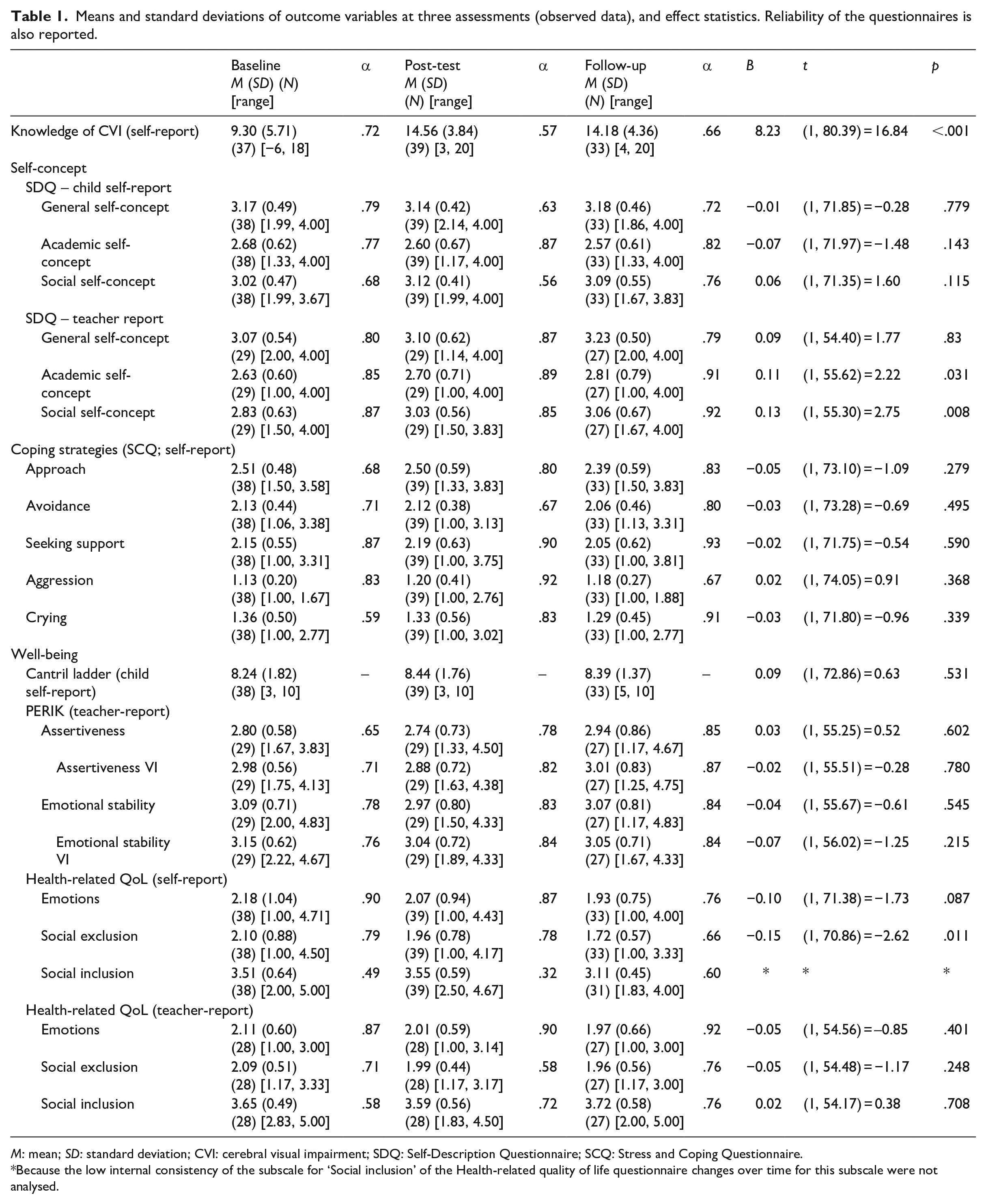
M: mean; SD: standard deviation; CVI: cerebral visual impairment; SDQ: Self-Description Questionnaire; SCQ: Stress and Coping Questionnaire.
Because the low internal consistency of the subscale for ‘Social inclusion’ of the Health-related quality of life questionnaire changes over time for this subscale were not analysed.
Coping strategies of participating children were assessed with the Stress and Coping Questionnaire for children (SCQ; Röder et al., 2002), which has been adapted for use with children with a visual impairment (Lievense et al., 2021). Four different school-related situations were presented to children. The situations described a scenario with difficulties related to CVI that children might encounter in school, for example, failing a school task because the child is not able to see it correctly. On a 4-point scale children respond to 14 items describing five coping strategies (approach, avoidance, support seeking, aggression, and crying). Coping strategies over the four different situations are averaged and a mean score per coping style is calculated. A higher score represents more use of this coping style.
Well-being was assessed with three instruments: the Cantril ladder (Cantril, 1965) for children, the PERIK (Mayr & Ulich, 2009) for teachers and the health-related Quality of Life questionnaire (HRQoL; Simeoni et al., 2007) for both children and teachers. The Cantril ladder asks children to rate how happy they are with their life on a 10-point scale, ranging from 1 (completely unhappy) to 10 (completely happy). The PERIK consists of six dimensions of which two are used within this study: self-assertiveness (6 items) and emotional stability/coping with stress (6 items). In addition, two newly developed items were added on self-assertive behaviour regarding the visual impairment and three items on emotional stable behaviour regarding the visual impairment. Teachers respond on a 6-point scale per item. Mean scores per subscale were calculated, and a higher score represents more of the associated behaviour. Internal consistency in previous studies was good (α ⩾ .81), and comparable to α’s in the current study (see Table 1). The HRQoL assesses the health-related quality of life of children with chronic disorders. The questionnaire originally covers six scales, of which three are used within this study: emotion (7 items, e.g., ‘Are you unhappy because of your visual impairment?’), social exclusion (6 items) and social inclusion (6 items). Respondents respond on a 5-point Likert-type scale. Because of the extremely low internal consistency of the subscale for self-reported social inclusion, this scale was dropped from further analyses. Higher scores represent more negative emotions regarding the visual impairment, more feelings of social exclusion and more social inclusion.
Qualitative data
Subjective evaluation
To assess the applicability, feasibility, and subjective effectiveness of the psycho-educational programme, children completed an adaptation of the Social Validity Scale with 14 items (Jonker et al., 2015). Items were rated on a 5-point Likert-type scale with a child-friendly thumbs up–thumbs down response system, and percentages of agreement are reported. Internal consistency was .63.
Interview
To complement quantitative data and put the results in perspective, qualitative interviews were done with a random selection of 13 children, 7 parents, and 7 teachers. Interviews were conducted by the research assistants who also filled out the questionnaires with children: face-to-face with children and online with parents and teachers. Interviews lasted on average 10–20 min, were audio-taped, and transcribed verbatim.
Statistical analyses
All analyses were performed with SPSS (version 27). Scores of children who finished the psycho-educational programme were included in analyses. First, all continuous outcome measures were checked for outliers (−3.29 < z < 3.29), and outliers were winsorized to the nearest non-outlier (9 values [0.4% of all values]). Because of the relatively small sample size, all analyses were performed both on observed and imputed data. Missing values of outcomes (16%, see also Table 1) were missing at random and therefore imputed by multiple imputation with five imputations and pooled outcomes of analyses are reported. A multilevel growth model was fitted to account for the change in scores of children from pre-test to post-test and follow-up. The fitted models consisted of two levels: time (level 1) and child (level 2). All models included a random intercept. In addition, for the model for knowledge of CVI also a random slope was fitted for each child. These random intercepts and slope allow for variation between children. Time and the quadratic effect of time (Time*Time) were added as predictors, because it was expected that children would increase more in their knowledge, skills and functioning during participation in the psycho-educational programme, than from post-test to follow-up. Age, primary/secondary education and type of education (mainstream vs. special education) were entered as covariates in each model when associated with the outcome variable. Gender was not associated with any outcome variable and therefore excluded as covariate. For parsimony, non-significant terms for each outcome were dropped (p > .05). Effect sizes (Cohen’s d) for imputed data are reported. As we expected change in knowledge of CVI to be associated with changes in children’s psychosocial functioning (self-esteem, coping, well-being), we next tested in a hierarchical regression analyses, adjusting for covariates, how change in knowledge of CVI (T2–T1) related to change in children’s functioning over a longer period of time (T3–T1).
For the qualitative analyses, transcripts of interviews were coded with Atlas.ti to discern different themes in answers to the interview questions. The first 10 interviews were independently coded by the first and third author. Codes were discussed to establish an agreed upon codebook, which was used to code the remaining 17 interviews by the first author.
Results
Quantitative data
Table 1 shows the means and standard deviations for the observed outcome variables. See Supplementary Table 1 for the means of the imputed outcome variables. Effect statistics are also reported in these tables.
Knowledge of CVI
After participating in the psycho-educational programme, knowledge of CVI improved linearly over time. This effect had a large effect size: Cohen’s d = 1.15. The quadratic trend of time was also significant, indicating the rate of increase flattened over time (observed: B = −2.90, t(1, 616.09) = −21.35, p < .001; imputed: B = −2.90, t = −5.41, p < .001; see Figure 2 for a visual depiction). Age was a significant covariate in this analysis (observed: B = 0.90, t(1, 39.01) = 3.96, p < .001; imputed: B = 0.89, t = 3.90, p < .001) – older children had more knowledge of CVI on pre-test and post-test.
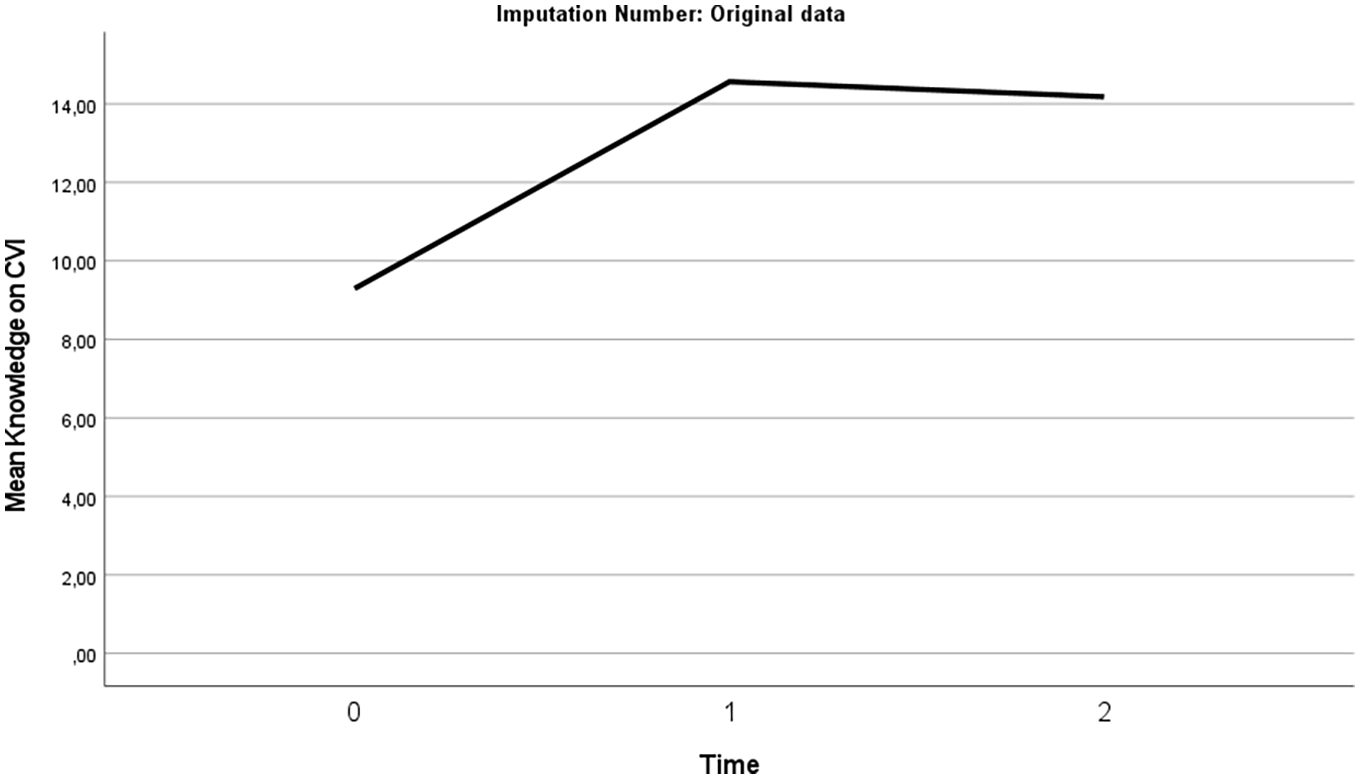
Change in children’s knowledge of CVI over time (original data).
Self-esteem
Analyses on observed data showed that after participating in ‘My CVI’ teacher-reported children’s academic and social self-concept improved linearly over time; see Figures 3 and 4. However, on imputed data these results were not found. The effect sizes were small: Cohen’s d = 0.20 for academic and 0.30 for social self-concept. No effect of participating in the psycho-educational programme ‘My CVI’ on self-reported measures for self-esteem were found over time, nor on the teacher-reported measures for general self-concept. Of the covariates, only the type of education a child attended was significantly associated with self-reported general self-concept (observed: B = 0.33, t(1, 38.96) = 2.64, p = .012; imputed: B = 0.29, t = 2.43, p = .015) – children in special education reported higher general self-concept at pre-test and post-test than children in main stream education.
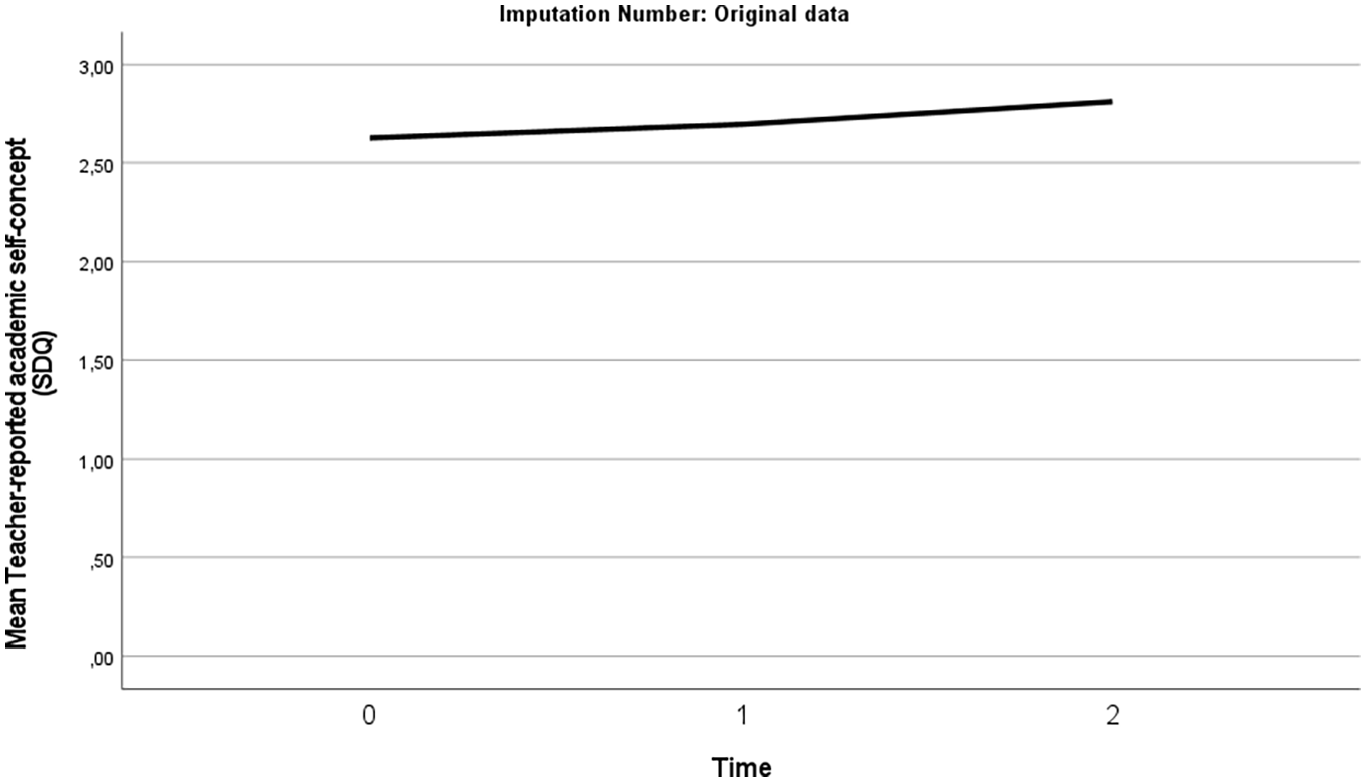
Change in teacher-reported child’s academic self-concept over time (original data).
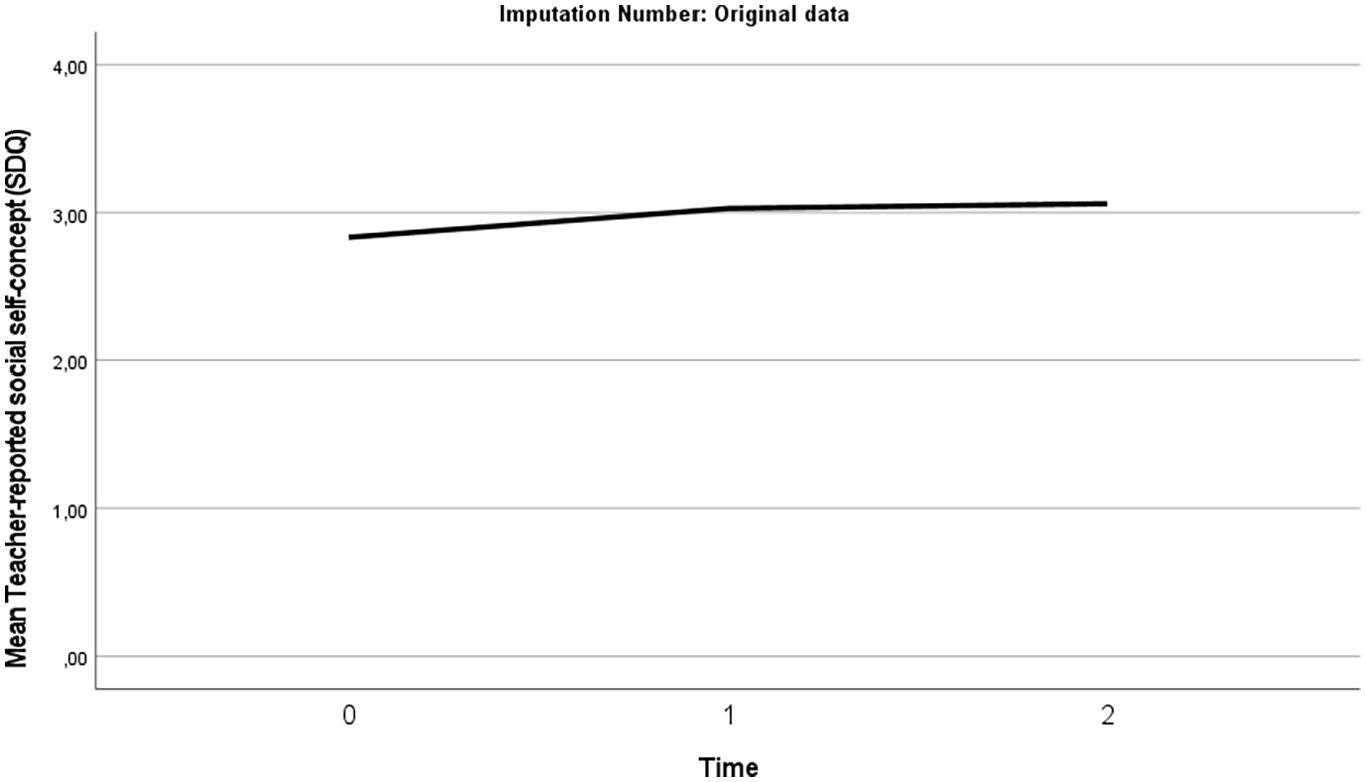
Change in teacher-reported child’s social self-concept over time (original data).
Coping
The analyses showed no change in coping-strategies over time after participating in ‘My CVI’.
Well-being
On the Cantril ladder, no effect of participation in ‘My CVI’ was found over time. Teacher-reported outcomes on the PERIK showed no effect of participation in the psycho-educational programme over time. For health-related quality of life, participating children reported less feelings of social exclusion over time. The effect size was small to medium (Cohen’s d: 0.41); see Figure 5. No effect of participating in ‘My CVI’ on the other subscale for self-reported or any of the teacher-reported subscales for health-related quality of life was found over time.
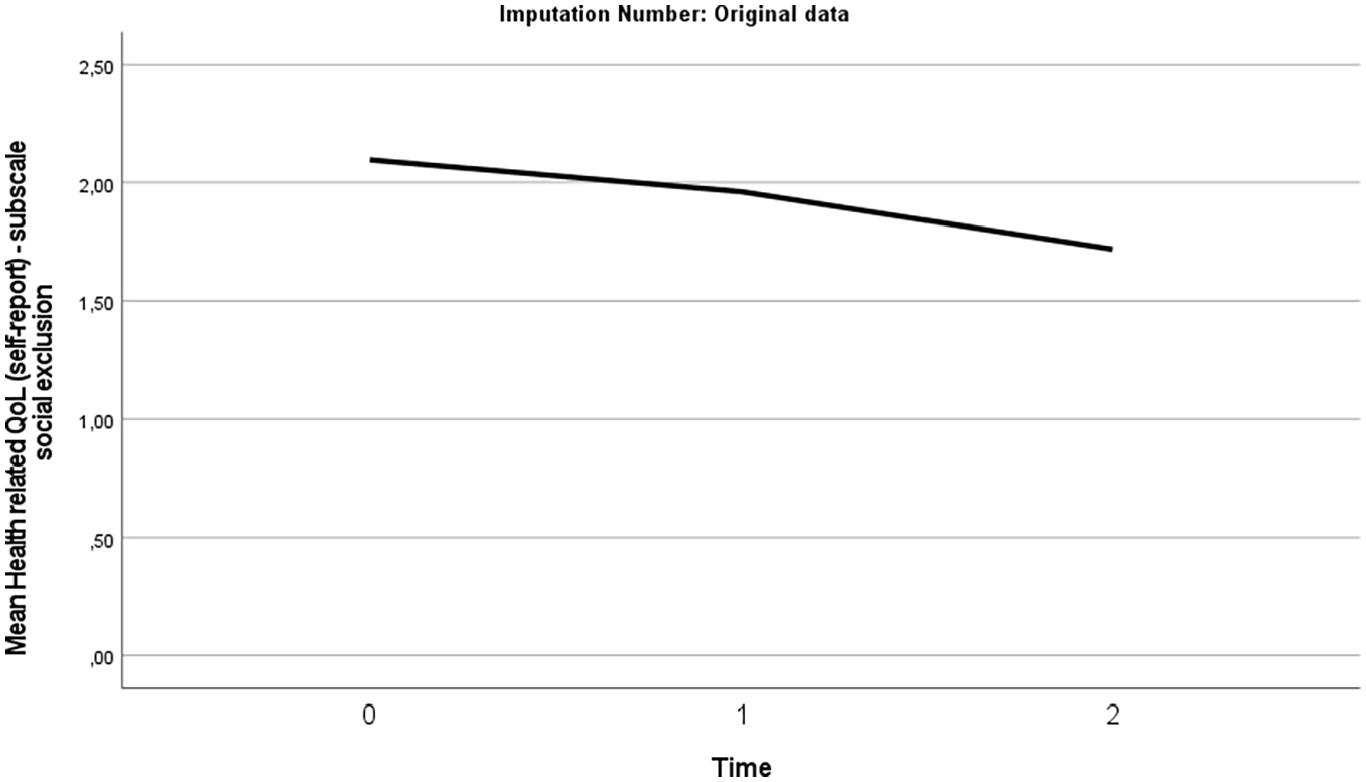
Change in self-reported feelings of social exclusion over time (original data).
Associations between change in knowledge of CVI and children’s psychosocial functioning
An increase in knowledge of CVI (T2–T1) was not associated with changes in any of the measures for child psychosocial functioning (T3–T1), neither on observed data nor on imputed data. See Supplementary Table 2 for a correlation matrix of these change scores, both on observed (Supplemental Table 2A) and imputed data (Supplemental Table 2B).
Qualitative data
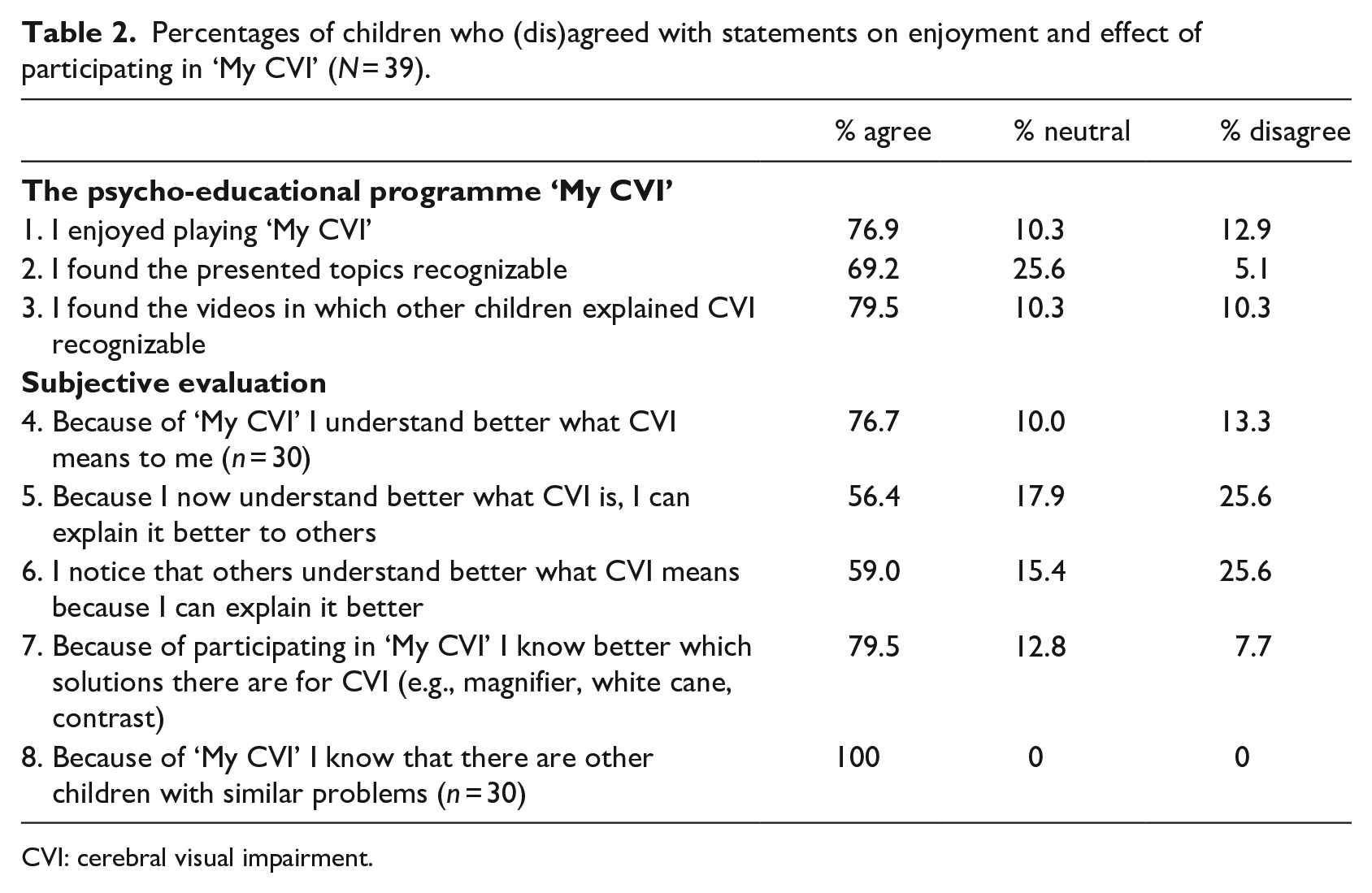
On the Social Validity Scale, most children responded they enjoyed participating in the programme and rated the discussed topics as recognizable and relevant to their situation (Table 2). The subjective statements of the Social Validity Scale corroborated the quantitative data by showing that 76.7% of the children answered that their understanding of CVI had improved, as well as their knowledge of available solutions to deal with their impairment (79.5%). In addition, a major effect of participating in the psycho-educational programme is that 100% of the children replied that they now realized there are children with comparable problems. Translating increased knowledge of CVI into being able to better explain to others what CVI means is still relatively difficult: slightly more than half of the children (56.4%–59%) responded positively to these statements.
Percentages of children who (dis)agreed with statements on enjoyment and effect of participating in ‘My CVI’ (N = 39).
CVI: cerebral visual impairment.
Qualitative interviews
A short description of the participants of the qualitative interviews can be found in Table 3.
Description of participating children, parents, and teachers in qualitative interviews.
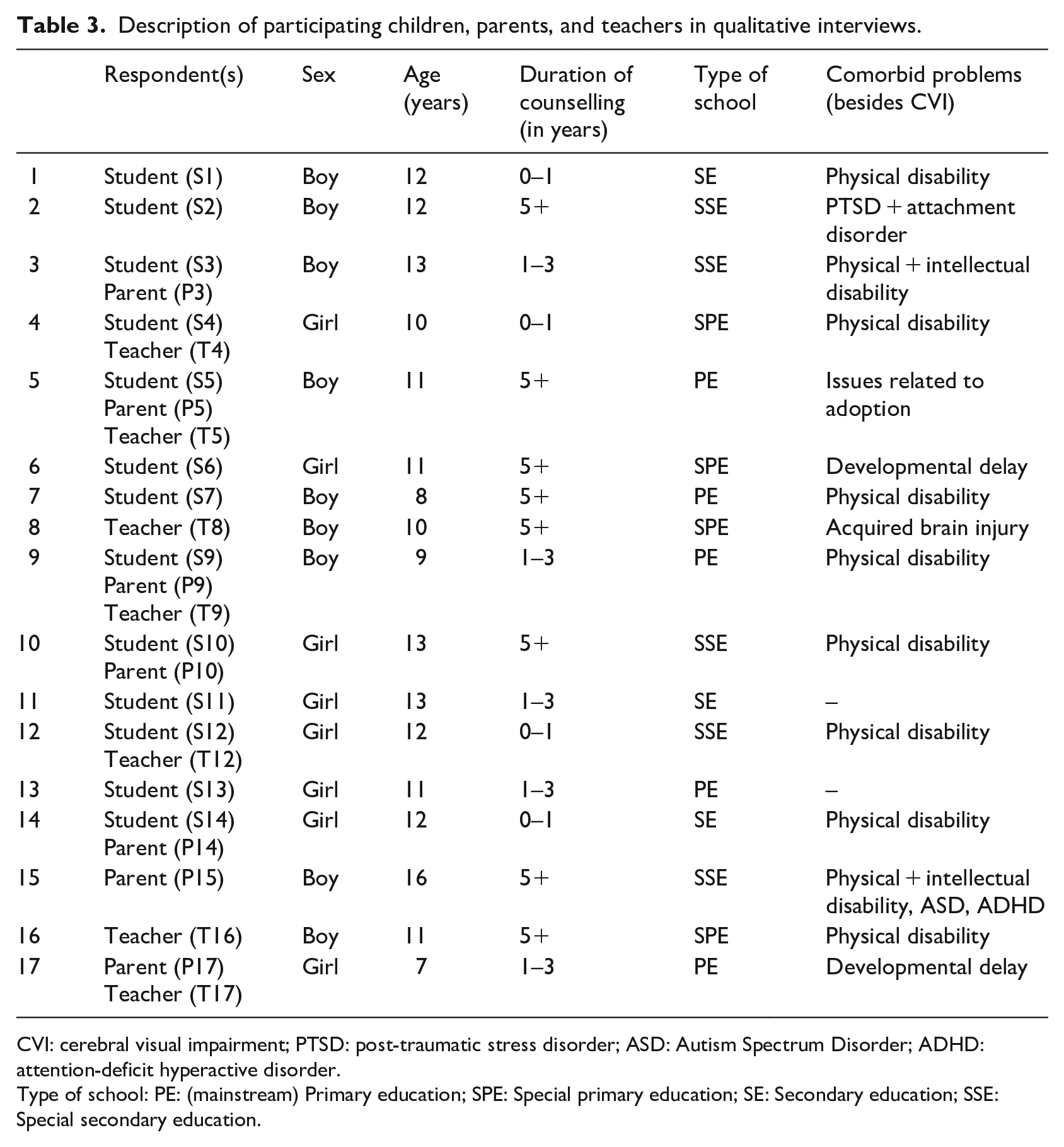
CVI: cerebral visual impairment; PTSD: post-traumatic stress disorder; ASD: Autism Spectrum Disorder; ADHD: attention-deficit hyperactive disorder.
Type of school: PE: (mainstream) Primary education; SPE: Special primary education; SE: Secondary education; SSE: Special secondary education.
‘What did you (/your child/student) like about the psycho-educational programme “My CVI”?’
Most children enjoyed participating in the programme (S2, S7, S9, S14; P3, P9, P10, P15, P17; T4, T5, T8, T9, T12): ‘I wanted to make all the lessons at once after finishing the first lesson!’ (S2) and ‘He liked that he was allowed to participate in “My CVI” at fixed times; in these moments he could take a moment to think about his CVI’ (T9). Children liked that the information was given by other children with CVI (S2, S5, S6, S10, S13), which resulted in recognition that there are also other children with comparable problems (S2, S3, S9, S10; P3, P5, P15; T4).
Most children, and their parents and teachers, said they found the information in the psycho-educational programme clear and informative (S3, S4, S6, S7, S10, S11, S13, S14; P3, P10, P15; T5, T8, T9, T12, T16). Some topics and videos were more relatable than others, although this also differed between respondents. The most relatable videos were about:
Difficulties in recognizing someone else (S1, S3, S4, S6, S11, S13, S14; P3, P17; T17);
Finding something (S4, S5, S6, S9, S13; P5, P15, P17);
Navigating through traffic (S1, S3, S5, S11, S12; P3, P14, P15);
Playing ball games (S3, S11, S13, S14; P10, P14, P15);
Difficulties with seeing on a crowded surface, for example, a heavily printed table cloth (S3, S5, S12; P3, P10; T12);
Difficulties in crowded places (S6, S13; P3, P10, P14, P17).
For parents and teachers it was sometimes difficult to get a clear picture of the programme the child followed, because they didn’t share much about it. Some parents replied they would have liked to participate in the psycho-educational programme together with their child (P3, P5). While the programme was originally developed to be completed at school, some children participated in the programme at home, partly because of the lockdown caused by COVID-19. The parents of these children (P10, P17) responded that they appreciated the opportunity to participate with their child together in the psycho-educational programme, which may also have increased understanding in the child: ‘I really liked [participating in the program] at home. (. . .). I recognized certain aspects in [child], while she didn’t. Then we talked about it and I explained what I recognized, and then she recognized it too’ (P10).
‘What have you (/your child/student) learned from following the psycho-educational programme “My CVI”?’
Of the 13 students, 12 responded that they now know more about CVI: ‘I have learned CVI can be different between different children’ (S1). Parents (P3, P5, P10, P17) and teachers (T5, T8, T12, T16, T17) agreed. Parents (P3, P10, P15) also said their child recognized many things in the psycho-educational programme. This recognition contributed to awareness (S14; P5, P10, P17; T4, T5), and children also started to ask questions ‘Will I have this my whole life?’, ‘Can I drive a car later?’ (P9). This recognition could be confronting and therefore not always appreciated (S14, P14). Children (S4, S6, S10) also replied they learned new ways to deal with their CVI: ‘I learned there are many tools which can help me deal with my CVI’ (S4), which was corroborated by teachers: T8 (tools for reading), T12 (tools on the computer), as well as parents (P3, P17).
Psychosocial effects of participation in ‘My CVI’
Participating in the psycho-educational programme ‘My CVI’ had some small psychosocial effects. Most parents and teachers reported the mood of the child had not changed after participating in the psycho-educational programme (P10, P15, P17; T5, T12, T17). The teacher who did report change in the mood of the student after participating in ‘My CVI’ stated ‘He could be very sad about [his CVI], he now accepts it more as a part of him. He mentions it more often and allows it to be’ (T9).
Most parents and teachers did not observe a change in how the child was able to cope with difficult situations in class (P5, P9, P10, P15, P17; T5, T8, T12, T16, T17). This could also be related to the fact that some children were already able to tell what bothers them and ask for help if necessary (T12, T16), or do not encounter difficult situations (T5, T8). One parent replied their child was able to stand up for himself better after completing the psycho-educational programme: ‘And he is able to say that [the fact that the software on his computer for his visual impairment no longer worked after an update] clearly. His confidence has grown in that he dares to say so’ (P3). All teachers responded that the position of the child had not changed in the group after participating in ‘My CVI’.
‘How do you (/your child/student) explain to others what you can and cannot do?’
Most children, parents, and teachers (S1, S3, S4, S7, S9, S11, S13, S14; P5, P9, P15, P17; T3, T5, T9, T16, T17) replied the way the child explained their impairment to others had not changed much after participating in the programme. Five students (S2, S5, S6, S10, S12), two parents (P3, P10), and two teachers (T5, T8) said the child explained their impairment a little bit different: ‘Before (. . .) I just said “I have CVI”. I now also explain what I find difficult, like ball games (S10)’. ‘(. . .) We had a class discussion about what [name student] has. That was great! It was in a very positive way that he just briefly explained what [CVI] was’ (T5).
‘What can be improved about the psycho-educational programme “My CVI”?’
Most suggestions for improvement were regarding the quiz questions after each videoclip; children had to keep answering the questions until they had all four of them correct, which was sometimes frustrating (S2, S11, S14; P5, P17; T8, T16, T17). Some technical difficulties were reported too: some clips did not play (S13; T12), or the child had to start in a previous section (S4). Some children were very enthusiastic about the programme and requested more video clips (S9, S11), with one concrete suggestion to add a video clip on playing sports (S6).
For (developmentally) younger children the programme may have been too difficult, which may have limited validity of their responses in selecting video clips for their personalized playlist and therefore the potential benefits of participation: one child had comorbid problems (physical and intellectual disability, ADHD, ASD; P15), another child was quite young and also had a delayed development (P17).
The timing of when to offer the programme seems important; when children already know a lot about their impairment, they are less motivated to participate in the programme (P9). However, at certain life milestones, for example, transitioning to secondary education, information regarding one’s impairment and tools on how to explain it to others may fit a window of opportunity (S5).
Discussion
This study looked into the effect of participating in the psycho-educational programme ‘My CVI’ for increasing children’s knowledge of their CVI and associated effects on their self-esteem, coping and well-being. The main result of the quantitative analyses was that participating in the programme resulted in increased knowledge of CVI. In addition, teachers reported a better social and academic self-concept in children after participation in the programme (only on observed data) and children reported less feelings of social exclusion. No effects of participation were found on self-reported self-esteem, coping or other measures for well-being. Against hypotheses, an increase in knowledge of CVI was not associated with changes in psychosocial functioning. Qualitative data revealed children enjoyed participating in the psycho-educational programme; they learned they were not the only one with CVI, and gained more knowledge and practical tools on how to deal with their visual impairment.
Both objectively and subjectively determined, participation in the psycho-educational programme was associated with an increase in knowledge of CVI. This effect of participation in an educational computerized programme has been found before for children with other impairments (Stinson et al., 2008). The use of a computerized form of psycho-education appeals to children and fits with their experiences in the current digital age (de Freitas & Liarokapis, 2011). Besides an increase in knowledge, participation was also associated with benefits on social measures: an increased social and academic self-concept and decreased feelings of social exclusion. This effect was not achieved through increased knowledge of CVI but likely a direct effect of participation in ‘My CVI’. In ‘My CVI’, participating children are told by other children with CVI what they encounter with their CVI and how they deal with it. This will likely have contributed to the feeling of participating children they are not alone in their impairment, which was corroborated with the qualitative statements. This is a positive effect, as has previously been shown that children with visual impairments generally experience lower self-esteem than their good-sighted peers (Augestad, 2017), and more often encounter social exclusion, such as bullying (Pinquart, 2017).
For more skill-based outcomes, such as coping with difficult situations, increased knowledge of CVI may result in better functioning in the longer run, because these skills require time to practice and develop. Increasing knowledge of a child’s impairment, may – in time – also have effects on their well-being. The time frame in the current study may have been too short to study this in more detail. In addition, it is feasible that knowledge learned in the psycho-educational programme may not be generalized to daily life. Active parental or teacher support, as suggested in the interviews, may be a crucial step to guide children in applying their gained knowledge of a daily basis, which could be a suggestion for further implementation.
Limitations
Despite considerable efforts, the final sample is modest in size, and diverse in age and comorbid problems. While these comorbid problems are representative for the population of children with CVI, it limits the possibility for subanalyses. Interview data suggest that the psycho-educational programme may be more effective for slightly older children and children with not too severe other impairments. The period in which our study took place, with several educational lockdowns due to the COVID-19 pandemic, was not representative for a normal school year. Because of these lockdowns data collection was more difficult, which is why we extended our period of data collection. Some children could therefore not finish the follow-up assessment within the same school year, which is why we were not able to collect the perspective of their teachers at follow-up. In addition, teachers, as well as parents and therefore children, have been under greater stress than under normal circumstances, which may have limited their time and possibilities to invest in the psycho-educational programme. Children missed several periods of face-to-face contact in schools. This limited their opportunities to practice their newly taught skills and the uncertainty in this period may have negatively affected their well-being. Because of these circumstances it is possible that the effects of ‘My CVI’ could be larger in a more normal situation.
Clinical implications
The qualitative interviews showed that participating children should not be (developmentally) too young to benefit from participation. The wish to be more involved with the participation of the child in the programme was expressed by some parents and teachers. The effect of the programme could be enhanced by the possibility to discuss the applicability of certain video clips and situations between parent/teacher and child, and increase generalization to daily life situations. It may be best suitable to offer the programme in the beginning of treatment for CVI, when children do not yet have much information about CVI. The programme could also be offered a second time a few years later when circumstances and needs of children have changed, for example, when starting secondary education. Based on the suggestions of participants in the qualitative interviews, adaptations to the psycho-educational programme have been made. These changes were content-related and technical: (1) the quiz questions were changed so that the correct answers are now shown after two attempts; (2) in the manual for implementation, we added the suggestion to involve parents and/or teachers for developmentally younger children. Technical adaptations were (1) all clips now play correctly, (2) participants did not have to start in a previous section, and (3) adding the possibility to repeat a lesson (to provide more opportunities for parental involvement). Next, the programme will continue to be offered through care organizations for children with CVI, both nationally and internationally.
Implications for further research
The main research question which is still unanswered is whether increased knowledge about CVI may result in effects on coping and well-being over a longer period of time. In the current study a follow-up period of 3 months was applied. Effects on these skill-based outcomes and well-being may take more time to emerge. Next, qualitative interviews suggested that the timing of when to offer the programme seems important. It would be worthwhile to further investigate this hypothesis. Finally, we recommend to investigate the added benefit of active parental or teacher support, both on children’s understanding of their CVI, and on parents’ and teachers’ understanding and their support of their children/students.
Conclusion
Knowledge of one’s impairment facilitates psychosocial functioning (Shilubane & Mazibuko, 2020). Currently very few psycho-educational programmes for CVI exist, despite the complexity of this visual impairment. ‘My CVI’ seems a promising programme for educating young people on their CVI and assist them in explaining their impairment and needs to others.
Supplemental Material
sj-docx-1-jvi-10.1177_02646196221139779 – Supplemental material for A mixed-methods study into the effect of a psycho-educational programme for children with cerebral visual impairment (CVI)
Supplemental material, sj-docx-1-jvi-10.1177_02646196221139779 for A mixed-methods study into the effect of a psycho-educational programme for children with cerebral visual impairment (CVI) by Mathilde M Overbeek, Mariska Stokla-Wulfse, Pieternel Lievense, Yvonne Kruithof, Florine Pilon and Sabina Kef in The British Journal of Visual Impairment
Footnotes
Acknowledgements
The authors would like to thank the five CVI heroes, the young persons who shared their experiences with CVI in the videoclips in the psycho-educational program: Chris, Evie, Jasper, Natasha, and Yu-Chan. We are also grateful to the five master students who helped collect the data. And, last but not least, we would like to thank all parents, children, and teachers for their willingness to participate in this study.
Author contributions
Conceptualization: Mathilde M. Overbeek (MMO), Mariska Stokla-Wulfse (MSW), Pieternel Lievense (PL), Yvonne Kruithof (YK), Florine Pilon (FP), Sabina Kef (SK); Methodology and Formal analysis: MMO; Data curation: PL, MMO; Writing – initial draft: MMO; Writing – review & editing: MMO, MSW, PL, YK, FP, SK; Project administration: MSW; Funding acquisition: MSW, PL, YK, FP
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Programmaraad, which was part of the Expertise budget of the Ministry of Health, Well-being and Sports (VWS), Project No. VJ2018-04.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.