
Abstract
People on probation face particular health inequalities and are categorised as an ‘inclusion health’ population group within public health policy in Wales. The health of this group is thought to be worse than the general population and a factor in whether people reoffend. This article is based on mixed-methods exploratory research which included a survey covering 34 community-based services who work with people on probation across Wales. Survey respondents indicated service availability and waiting lists, and mistrust of professionals are key barriers to accessing healthcare. The most identified health needs were mental health and substance misuse related. There is an opportunity to increase the focus on healthcare for people on probation through inclusion health approaches.
Introduction
People on probation as an ‘inclusion health’ group
Evidence suggests that the health of those subject to probation or prison sentences is worse than the health of the general population (Brooker et al., 2020; Cumming, 2020; Skinner and Farrington, 2023; Williams et al., 2023) and mortality rates of those with offending histories are higher than the general population (Piquero et al., 2014; Skinner and Farrington, 2023). Research studies principally consider mental health concerns within this group and rarely examine poor physical health outcomes (Skinner and Farrington, 2023). For example, communicable diseases, which include tuberculosis, viral hepatitis and sexually transmitted infections (WHO, 2023), are one of the most common specific health needs of people who have offended (Royal College of Nursing, 2009). As a result, people on probation are increasingly subject to ‘inclusion health’ approaches by public health agencies which work to ‘prevent and redress health and social inequities among the most vulnerable and excluded populations’ (Luchenski et al., 2018: 266). Practitioners are encouraged to know and respond to health and wellbeing issues of inclusion health groups (PHE, 2021). Despite this, the health of people on community probation supervision remains overlooked within research and policy responses (Lloyd, 2013; Skinner and Farrington 2023; Williams et al., 2023). People on probation therefore ‘often face a double disadvantage of both health inequality and difficulty of access to health services’ (Lloyd, 2013: 4). Indeed, Brooker et al. (2008) have suggested there is a lack of sufficient services for community-based offenders whose needs are greater than the general population.
It has been argued that research to develop understandings and provisions regarding the health needs of people on probation has wider humanistic and economic benefits (Skinner and Farrington, 2023). Notably, mental and physical health are suggested factors which contribute to offending (Jackson and Vaughn, 2018; Skinner and Farrington, 2023; Social Exclusion Unit, 2002) and people with offending histories believe there is ‘a strong association’ between their health and their involvement in offending behaviour (Lees et al., 2013). Furthermore, inclusion health groups face stigma (PHE, 2021), particularly those who are prison-experienced (Schnittker and John, 2007). The term ‘offender’ is accepted as an ‘unhelpful label’ but remains in use within certain contexts (HMPPS, 2021: 4). Therefore, there is an opportunity to move from ‘offender health’ to ‘inclusion health’ research for people on probation, as well as greater opportunities to use public health thinking within criminological research (Skinner and Farrington, 2023). Indeed, this mixed-methods study explores health needs and provision for people on probation in Wales (also drawing from literature in England) from an inclusion health perspective. This builds upon recent inclusion health studies in South Wales (Irwin and Whitear 2020; Jones, 2022; Williams et al., 2023) and adds to the developing picture of Welsh public health and justice research and data (see Ford et al., 2019; Jones, 2020; Perrett et al., 2020).
The ‘jagged edge’: Challenges in exploring health and justice in Wales
Around 14,000 people are supervised by probation in Wales with under a third of these within custody (MoJ, 2023a). The service is organised into six delivery units which closely align with the seven health board areas in Wales. 1 It has been recognised that ‘making sense of the health and justice landscape can be challenging due to the complexity of, and interdependencies between, the health and justice systems’ (HMPPS, 2019: 7). This is a particular issue for Wales given that responsibility for health is devolved to the Welsh Government, whilst justice powers are reserved to the UK Government. HMPPS in Wales has responsibility for commissioning services, for example, in relation to Alcohol and Drug Treatment Requirements, whilst Welsh health boards provide health care within the Welsh prisons, as well as the community (HMPPS, 2019). Whilst there are efforts to create health and justice strategies (HMPPS, 2019, 2022a), examining the issues for Wales, including obtaining relevant data can be problematic, given the lack of understanding of Wales’ justice system as a distinct entity (Jones and Wyn Jones, 2022). This ‘jagged edge’ of justice within the current devolution settlement was recognised with the Commission for Justice in Wales which stated, ‘if criminal justice is to be effective…it must be closely integrated with services…for example, health, drug and alcohol misuse’ (Welsh Government, 2019: 135). To progress Welsh criminological understandings, there have been efforts to unpick prison and probation data in Wales (see Jones 2018, 2020, 2023; Jones and Wyn Jones, 2022). Most significantly, Wales has the highest incarceration rate in Western Europe and a higher proportion of community sentences compared to England (Jones and Wyn Jones, 2022). Coupled with this, Wales has specific health challenges, including longer waiting lists; indeed ‘a person in Wales is more likely to die each year than a person of the same age in England’ (Dayan and Flinders, 2022). Given these critical factors, there is a need to pay specific attention to health and justice matters in Wales. Indeed, it has been suggested that when researching community safety more broadly, it is ‘seriously flawed’ to accept that Wales reflects the position in England (Edwards and Hughes, 2009).
What is known about the health of people on probation?
Mental health
Mental health is a well-known issue for people on probation, yet often goes untreated. In a study by Georgiadis et al. (2016), 58% of men involved in offending had at least one common mental health problem, with only 26% reporting receiving treatment. Depression, for example, has been identified as a significant problem for people on probation who reside at approved premises (Hatfield et al., 2004). Furthermore, estimates have suggested that ‘30–50% of a probation caseload and 60–70% of a prison population may meet the criteria for one or more personality disorders’ (HMPPS and NHS England, 2020). Despite many people on probation suffering from one or more mental illnesses or mental illness combined with a substance misuse problem, it can be left undiagnosed or untreated (Brooker et al., 2020: 2). Indeed, only 2% of Community Orders and Suspended Sentence Orders in England and Wales have Mental Health Treatment requirements and there is evidence that such requirements are ‘underused’ in Wales (Welsh Government, 2019: 221). Little is known about the mental health needs of people on probation in Wales, although 62% of people on probation in Wales are assessed as having ‘thinking and behaviour needs’ (HMPPS, 2022a). Mental health issues in prison are better documented, most notably within prison inspection reports. For example, 65% of prisoners arriving at HMP Cardiff said they had a mental health problem (HMIP, 2019). Official reports indicate self-harm and suicide are a particular issue across the prison population (MoJ, 2023b) but there is little examination of suicide amongst people with offending histories based in the community (Skinner and Farrington, 2023).
Substance misuse
There is a higher prevalence of substance misuse by people on probation compared to the general population (Brooker et al., 2008; Mair and May, 1997; Sirdifield et al., 2019, 2020). People who inject drugs are at higher risk of blood-borne viruses such as Hepatitis C (Crowley et al., 2019) (see ‘communicable diseases’). Health issues relating to alcohol dependency are also well-documented; for example, a study by Goodall et al. (2016) to inform policy on violence prevention and alcohol monitoring in Scotland found blackouts and loss of memory were common harms. Furthermore, it is thought that around 75–85% of all UK prisoners have a dual diagnosis of a mental health problem with alcohol or drug misuse (The Bradley Report, 2009). Hatfield et al. (2004) found people on probation with mental health needs also have a more significant drug problem. Mental illness combined with substance misuse has been related to early conflict with the law (Jolliffe et al., 2017). However, drug use can reduce with time; in a longitudinal study of males involved in the criminal justice system in London, found at 18 years, 32% were drug users, compared with 19% at 32 years (Piquero et al., 2014).
In Wales, 26% of people on probation have an identified alcohol misuse need and 37% have a drug misuse need (HMPPS, 2022a). A similar picture exists within Welsh prisons, with 38% of prisoners arriving at HMP Cardiff reporting a drug or alcohol problem (HMIP, 2019). Fitzpatrick and Thorne (2011) suggest there is a greater need for alcohol interventions for people on probation compared to drug treatment, given the scale of the alcohol use. Notably, 4% of Community Orders in England and Wales have a drug or alcohol treatment requirement (MoJ, 2023a). Such requirements have increased since the introduction of alcohol abstinence and monitoring following a successful pilot in Wales (MoJ, 2022). However, a systematic literature review of community supervision and substance misuse found that much of the evidence is dated and new research is needed to better understand profile of needs and effective interventions (Sirdifield et al., 2020).
Physical health
Research suggests that ‘offending may be associated with poor physical health and an increased risk of premature mortality’ (Skinner and Farrington, 2023: 2). There is limited understanding (and no known government published data) on the physical health needs of people on probation, and the health of prisoners is often used as a proxy to understand health needs of this population group. For example, 20% of prisoners arriving at HMP Cardiff describe a physical health problem and 44% have a disability (HMIP, 2019). Furthermore, ageing prisoners have complex health problems which suggest that their physical health status is ten years older than the general population (Hayes et al., 2012). Chronic disease is a particular issue; a third of deaths by natural causes in prison are due to cardiovascular disease (Williams et al., 2022). Historically, 49% of people on probation reportedly ‘currently had or expected to have certain long-term health problems or disabilities’ (Mair and May 1997: 17). Hatfield et al. (2004) found 19% of people on probation in their study had one or more physical health problems identified, combined with high rates of mental health disorder. More recently, 46% of people on probation within a Welsh study reported long-term illnesses (Williams et al., 2023). Communicable diseases are also one of the most common specific health needs of people who have offended (Royal College of Nursing, 2009). Injecting drugs accounts for 80% of Hepatitis C infections and there is a heightened risk for prison leavers (Crowley et al., 2019).
Wider determinants of health
Factors such as employment, finance and relationships are connected to health and offending (Link et al., 2019: 563). Williams et al. (2023) found the employment rate amongst people on probation (31%) was less than half that of the general population in Wales (74%). Pact (2023) suggests families play an important role in supporting the health needs of those involved in the criminal justice system. Indeed, 6 in 10 people on probation in Wales have a need to address relationship issues (HMPPS, 2022a). In addition, poor neighbourhood quality (including lack of access to green spaces and fear of crime) has been associated with poor health (Dunstan et al., 2013). Williams et al. (2023) suggested that people on probation live in the most deprived areas and less likely to have access to an outdoor area or garden at home than the general population in Wales. Notably, four in ten prison leavers in Wales are assessed as having an accommodation need (HMPPS, 2022a).
Moreover, examining health determinants is particularly relevant for Black, Asian and minority ethnic people on probation, who continue to be over-represented within the criminal justice system in Wales (Jones, 2023). Factors such as socio-economic status, living arrangements and occupation, as well as a prevalence of underlying health conditions, were notably linked to a higher risk of mortality of COVID-19 amongst ethnically diverse groups (Ayoubkhani et al., 2021; Platt and Warwick, 2020).
Barriers to accessing healthcare
Many barriers to accessing healthcare exist for people on probation. A study of 16 probation areas in England and Wales found that main barrier for health and justice was ‘poor communication’, ‘little joint working, understanding and education between primary care and probation’ (Parkes et al., 2012). Indeed, Rennie et al. (2009) observed that the primary focus of criminal justice is not healthcare, and there is a resultant gap in staff training and lack of information sharing, including partnership working. This is a particular issue for mental health, both within the community and pre-release from custody. Patel et al. (2018) reviewed mental health care provision within prison inspection reports identified key challenges around ‘process’ and ‘staffing’ issues, as well as concerns around ‘range’ and ‘quality of service’. Additional concerns included delays accessing services and lack of specialist training. Furthermore, prison leavers who inject drugs are particularly marginalised and have been described as ‘underserved by traditional health services’, ‘despite high rates of physical and psychiatric morbidity’ (Crowley et al., 2019: 6). Notably, links have been drawn between poor access to health care on release from prison and the increased transmission of disease, and even increased risk of death (see discussion in Eshareturi et al., 2014).
Methodology
This study formed part of a wider mixed-methods research project to understand the population demographics, health needs and service provision across Wales that serve inclusion health populations, including those involved with the criminal justice system (Rabaiotti, 2023). The methodology draws from community-led service mapping (Oxfam, 2021) and steps to mapping health service provision (Price et al., 2019). The research design included desktop research, submission of Freedom of Information (FOI) requests to HM Prison and Probation Service (HMPPS) and a survey. Data was subject to a thematic analysis using six-phase approach from coding to defining themes (Braun and Clarke, 2006). The research received ethical approval and was conducted in line with Swansea University's research integrity policy.
Desktop review of services
A service mapping exercise was carried out initially using the Dewis Cymru directory to identify relevant services across Wales (Data Cymru, 2023). Keywords including, ‘offenders’, ‘prisoners’, ‘probation’ gave access to over 80 results. A further search was carried out via the ‘Clinks directory of voluntary sector justice services’ which gave access to over 200 potential results for services in Wales (Clinks, 2023). The findings were cross-referenced to avoid duplications, and whether they met the criteria, namely services working with people on probation in Wales. This was supported by Google searches including health board websites and updated following the survey responses and response from a FOI request to HMPPS about commissioned services in Wales. The final number of services mapped who work with the population group was 140.
Survey approach
A survey was designed to gather information to develop an understanding of the service provision across Wales that serves inclusion health populations, as well as a better understanding of their service users and their needs. The survey was accessible online during May 2023 and included a mixture of closed and open-ended questions to gather quantitative and qualitative data. Informed consent was given, and all questions were optional. Respondents identified the agency they worked for but no personal or identifiable data was gathered. Qualitative responses were manually analysed using MS Excel, by coding and grouping comments into sub-themes and themes which had been informed by the literature review (Braun and Clarke, 2006).
Survey sample
The survey was aimed at professionals working with people in probation in Wales beyond statutory probation provision. It was distributed to email addresses identified via the service mapping exercise, plus health and justice contacts. Fifty-one surveys were completed. However, several were submitted from the same organisations, albeit they may represent different teams, services, or locations. Therefore, when accounting for potential duplications in services, there was a sample of 34 separate services, which equates to a 24% response rate.
Unique identifiers were assigned to the 51 respondents based on their service status. The majority (61%) represented the voluntary or not-for-profit sector (Vol 1–Vol 31), with a quarter providing a statutory service (Stat 1–Stat 13). Three respondents represented the private sector and four respondents selected ‘other’ (combined as Oth 1–Oth 7).
When asked to describe the core aspects of provision, most (39%) described general support (including work to ‘reduce reoffending’), a quarter provided a mental health or well-being service and a lesser amount (22%) provided housing or employment and training service. Only 4 (8%) respondents provide physical health-related support.
The survey was representative of all local authorities in Wales with most services covering multiple areas, in particular the South Wales area. Most (29) respondents covered Swansea (57% of respondents). The lowest representation was Gwynedd with only 16 out of the 51 (31%) respondents covering the area.
Limitations
The survey sample was not reflective of all services working with the population group in Wales and respondents did not answer every question. The survey relied on key informants and health needs disclosed to them and whilst they have relevant expertise, they may not accurately represent the population group or their interests (Lokot, 2021). Nevertheless, the findings serve to highlight an issue which policy needs to address, as well as providing a starting point for further research.
Findings
The findings are presented in four thematic sections. The first shares the mapping of a wide range of services which support people on probation in Wales, some of which support healthcare needs. The second, third and fourth sections draw from the data provided by key informants in the survey. This includes the health offer from service providers, common health needs identified and perceived barriers to accessing healthcare.
Beyond statutory provision: Services supporting people on probation in Wales
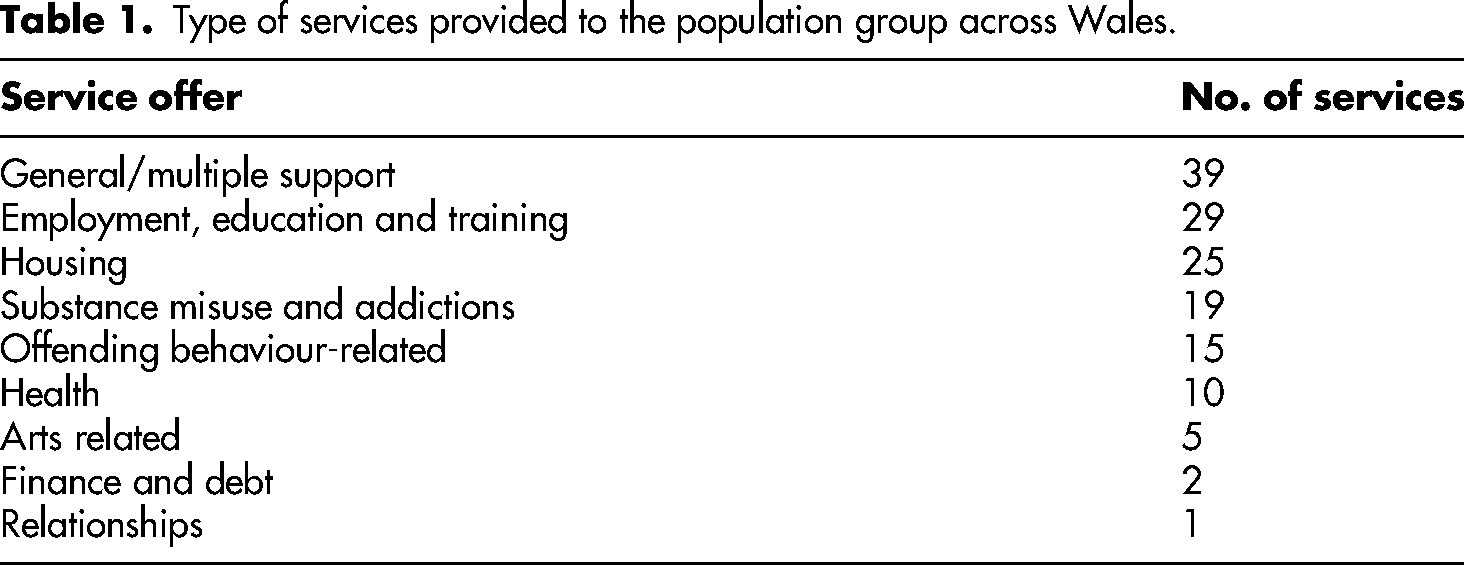
Through the desktop research, 140 services for adults were mapped across Wales, mainly consisting of voluntary organisations, that provide needs-related services to people on probation, prison leavers, and those in conflict with the criminal justice system. Almost half of the services were available on an all-Wales basis. 41% were South Wales only, 16% were North Wales only and 7% in the Dyfed and Powys area. A large proportion (28%) of services provide multi-natured support. In terms of specialist support, the main provision was employment and training, and housing support (see Table 1). Fourteen percent of services provided substance misuse and addiction support and 7% of services referred to health-related support.
Type of services provided to the population group across Wales.
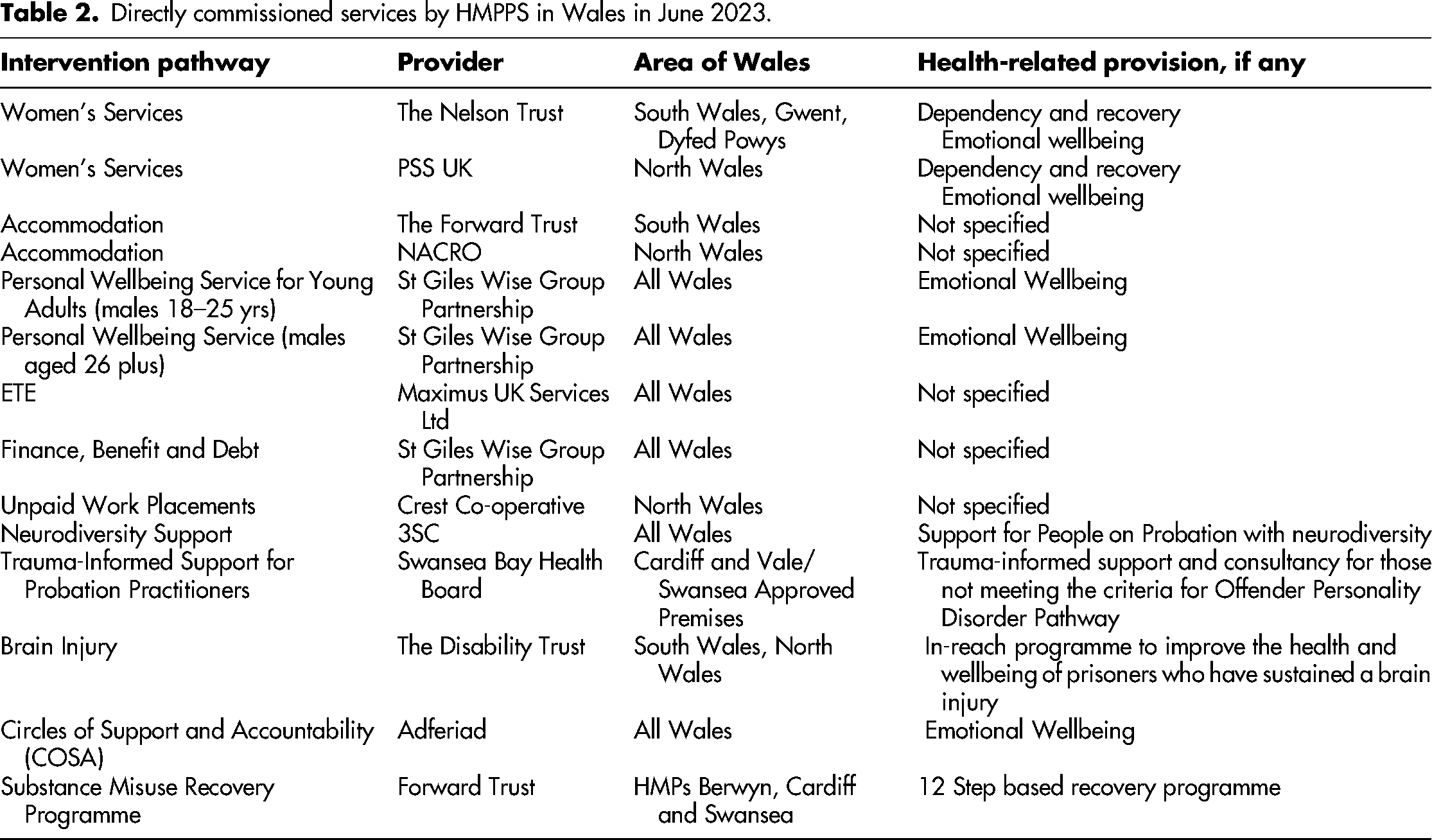
Over twenty of these services are known to be commissioned or co-commissioned rehabilitative services for people on probation in Wales by HMPPS in Wales. Information provided in a FOI response indicated that 9 of the 14 commissioned services are related to health (mental health and emotional well-being) and substance misuse. This includes a new all-Wales neurodiversity support service, well-being support for women and young adults and support for those with brain injury in HMP Swansea and HMP Cardiff (see Table 2). Of the co-commissioned services, 5 of the 9 services are substance misuse services which cover regions of Wales (North Wales, South Wales, Dyfed, Powys and Gwent). It is understood there are other services, ‘internally commissioned’, that do not feature within the FOI Request. For example, the Wales Offender Personality Disorder Pathway is a jointly commissioned service between NHS Wales and HMPPS to improve the psychological health and well-being of people on probation and reduce their risk of re-offending (HMPPS 2022b).
Directly commissioned services by HMPPS in Wales in June 2023.
Service eligibility, referral criteria and access
Survey respondents were asked to describe the eligibility criteria of their service. A manual analysis of 48 qualitative responses coded and grouped the description of service provision. The highest response was person on probation, prison leaver or person involved in criminal justice system (46%), followed by need-related (25%), age (23%) offence or risk-related (19%). Respondents indicated that agencies have multiple referral routes. The highest response was statutory referral (71%), followed by self-referral (47%) and non-statutory referral (41%). Respondents indicated that services are accessed in various ways. The highest response was in-person at the service provider premises (90% of providers use this location), followed by in-person at community hub or similar (80%) and the third highest response was remote (telephone) (78%). Responses indicated that agencies provide responsive or regular contact. The highest response was depending on individual need (67%), followed by daily (65%) and weekly contact (59%). Only 8% of respondents suggested that services engage once or twice each year.
Assessing and signposting: Healthcare ‘support’ for people on probation
Identifying and accessing health-related needs
Most respondents (86%) indicated that their service identifies and/or assesses health needs or issues. Four (8%) respondents indicated that their service does not do this and three (6%) were unsure. A total of 46 qualitative comments provided explanation as to how their service identifies and/or assesses health needs or issues. Most respondents (61%) described the use of initial screening or health needs assessment: Everyone has an initial assessment and from there is signposted to services either internally or externally or both. (Vol 15) Physical health: generally self-identified by the service user or notified via prison health. Mental health: [the same], also personality disorder screenings and referrals, liaison with community and forensic mental health services. (Stat 10) [We] have a number of health and wellbeing champions who are trained to identify any health issues and signpost where applicable. (Vol 23)
Thirty percent of respondents mentioned a formal assessment process. As Vol 8 said: The clinical nurses monitor, assess and evaluate health needs and sometimes our resilience staff are a pre-curser to any rising health concerns.
A quarter of respondents described the implementation of arrangements, including taking a ‘partnership’ approach: We deliver an enhanced GP service on a weekly basis for those who specify a need. We work alongside our partners at [the health board] and have a funded vehicle to remove barriers to accessing health services for those who struggle to gain access, we will also attend with the individual if they choose. (Vol 2) Our [service users] are often involved with other statutory services…organisations will share information about health needs as part of the referral and as part of ongoing joint working. (Vol 22)
There was also an emphasis on a patient-centred approach (22% of comments). As Vol 7 said: [There is a] continual process of needs assessment as support is delivered to ensure it's tailored and appropriate… including referrals to other agencies.
A few comments from participants based in statutory services suggested improvements were needed to identify and assess health needs. For example, Stat 3 said their risk assessment ‘does not capture enough health data’ and Stat 4 explained that they ‘can refer for assessments on a number of health issues but [they are] not directly responsible’.
Provision of health-related services or clinics
Less than half of respondents provided health-related services or clinics either directly or through a partnership or commissioned service. Respondents were able to provide qualitative comments to describe the type of health-related services or clinics provided. Twelve comments were received. Most of the respondents (72%) described a mental health-related service with less than half offering counselling or similar. Six (27%) respondents referred to drug treatment or prescribing clinics. A range of services were offered, with one respondent explaining that they provide: Access to counselling for those experiencing lower-level poor mental health as a result of what's happened to them and the impact it's had. We also offer advocacy where needed to speed up referrals to health services. (Vol 7)
The prevalence of mental health as a key issue: Service providers’ understandings of health needs
Respondents were asked about common presenting physical, mental health and wider related needs and provided detailed qualitative comments, as well as limited responses suggesting their service users had ‘all, most’ or ‘common forms’ of physical and mental health issues. Mental health issues were featured as a key need within both physical health and mental health comments.
Common physical health needs
Forty-one responses described common physical health needs identified or reported by service users. The most common responses (39% comments) were mental health-related physical needs and substance misuse-related conditions or injuries. Seventeen percent of comments described respiratory conditions and 15% of comments described communicable diseases and mobility issues. A smaller proportion of comments covered a wide range of physical ailments, including but not limited to, eating and sleeping concerns, pain issues, heart conditions, sexual health, dental health and diabetes.
Common mental health needs
When asked to consider common mental health needs identified or reported by service users, 48 responses were categorised. The most common response was depression (75% of all comments), followed by stress and anxiety (52%). Post-traumatic stress disorder (PTSD) featured highly (27%), followed by self-harm/suicidal thoughts (23%) and neurodiversity or learning difficulties (23%). Other notable categories include psychosis, schizophrenia and bipolar (21%) and personality disorder (19%).
Wider related needs
Considering the wider needs of the population group, respondents were asked to select as many as applied from a range of 13 needs. All survey respondents (51) answered this question. Each selected an average of eight needs. Looking at the top five needs, most respondents selected mental health (86% of respondents in comparison to only 51% selecting physical health), followed by financial issues (78%), substance misuse (74%), social isolation (74%) and accommodation (73%). Employment (67%), lack of basic needs (65%) and relationship issues (71%) also featured highly. The lowest response was lack of digital access (41%).
Nineteen further comments were received in relation to the wider needs of the service users. Forty-two percent of these comments talked about responding to individual needs and being inclusive to improve access to health and justice. One respondent wrote ‘some of our most vulnerable patients are unable to access the help that they need at the time that they need it’ (Stat 7). A third referenced the multiple and varied needs of this service user group. Stat 3 commented ‘people in criminal justice system have a wide and varied level of need’ and Stat 4 stated ‘we could be here all day’ listing needs.
Inequal healthcare: Barriers faced by people on probation
A quarter of comments around wider needs of service users related to lack of services, lack of integration and lack of staff understanding of service user group. Similar responses were received when asking specifically about barriers to accessing healthcare.
Service accessibility
Respondents were asked to select the three main barriers to accessing health services for their service user group from 19 options. Forty-eight respondents answered. According to half of the respondents, the highest barrier to accessing health is ‘service waiting lists’. As Stat 5 said: Accessing good health service provision has steadily become more difficult over the past ten years. People on probation face health inequalities. Provision for mental health in Wales is the worst it's been for years. Engagement from health isn’t great, due to the demands on them. (Stat 3) Many clients are struggling to gain GP appointments due to having to call at 8am in morning; many experience anxiety and this creates a barrier to support. (Vol 31)
Thirty-three percent of respondents selected ‘not registered with a GP’ and ‘lack of information about services’. Vol 9 explained: We do find that they are less likely to access services due to the lack of knowledge to what is available locally to them.
The lack of understanding of professionals
Thirty-eight percent considered ‘mistrust of professionals’ was a barrier for people on probation in accessing healthcare. Respondents acknowledged this group face judgement or even discrimination: [they] fear they will be judged if they access local services and have been convicted of a crime that could mean they are recognised and possibly judged because of this. (Vol 9) Unfortunately, I have observed that some of the individuals that we support have been discriminated against because of their issues with substance misuse and offending. (Oth 4) Many health provisions do not always seem to come from a trauma informed/psychologically informed approach. (Vol 18) Health service provision is unable to assist as solution involves knowledge of criminal justice system which is simply not covered by government. (Vol 17)
However, findings suggested that those working with people on probation have a lack of health understanding. For example, 22 (43%) of respondents were unsure whether their service has a policy or process on communicable diseases. Vol 3 said ‘this is something I have not come across’. Whilst 10 comments reflected a developing understanding of communicable diseases, with specific reference to a bloodborne virus testing pilot between Public Health Wales and probation. One respondent commented: Although we have supported males with some communicable diseases, we don’t mention this, as it is about the client and not the disease, it's about the client being respected and treated with the respect they deserve. (Oth 3)
Discussion
‘Engagement isn’t great’: Challenges in health and justice research and practice in Wales
This study builds on an emerging body of Wales inclusion health and justice research and data (Irwin and Whitear 2020; Jones, 2020, 2022; Perrett et al., 2020; Williams et al., 2023). Whilst people on probation have a universal right to health treatment, the low levels of interactions between this group and primary care suggest there need to be supportive strategies between health and justice agencies (HMPPS, 2019). Until these are properly implemented, we may continue to see, for example, disproportionate access of emergency departments and inpatient stays for people on probation in Wales (see Williams et al., 2023). A particular challenge exists given the non-devolved position of justice and the interactions with devolved agencies which support health and wider needs (Jones and Wyn Jones, 2022; Welsh Government 2019). This results in a complex policy landscape which extends to practice where criminal justice practitioners lack healthcare knowledge, whilst the system faces continual high demand, with one respondent acknowledging ‘engagement from health isn’t great’. It has been suggested that ‘there is an inherent conflict in focussing on health in the criminal justice system, as healthcare delivery is not its main purpose’ (Rennie et al., 2009: 6). This leaves people on probation, especially those with substance misuse issues, with high rates of poor physical and mental health as particularly marginalised and ‘underserved by traditional health services’ (Crowley et al., 2019: 6). This is despite people with offending histories concerned that there is ‘a strong association’ between their health and their involvement in offending behaviour (Lees et al., 2013).
Positively, there are indications that desistance-based approaches to health needs can improve the life quality for prison leavers (Link et al., 2019) and wider offending populations (Brooker et al., 2023). Furthermore, the Covid 19 pandemic has highlighted the need to do more to improve healthcare for this population group as well as their families and community (Pact, 2023). Indeed, there have been developments in health and justice partnership working in Wales including employing three dedicated coordinators to strengthen treatment pathways (HMPPS 2022a). Whilst it remains too early to understand the benefit of the health and justice partnership coordinator role, other examples of collaboration between health and police in Wales, such as trauma-informed approaches training, have reported a positive impact (Barton et al., 2020).
‘We could be here all day’: Health needs of people on probation and wider determinants of health
The health of those subject to probation or prison sentences is thought to be worse than the general population (Brooker et al., 2020; Cumming, 2020; Williams et al., 2023) and a factor in whether people go on to reoffend (Social Exclusion Unit, 2002; Skinner and Farrington, 2023). Much of the research in this area is focussed on mental health issues and prisoner health (Skinner and Farrington, 2023; Williams et al., 2023). The latter remains an important area of research, not least because Wales has the highest imprisonment rate in Western Europe (Jones, 2018). Concerns have been raised about a rapid rise in natural deaths in prison, which is not simply about the ageing population but broader intersectional matters affecting ethnically diverse groups, as well as prison healthcare challenges (Shaw et al., 2020). Notably, Black Asian and minority ethnic groups continue to be overrepresented in the criminal justice system (Jones, 2023) and experience disadvantage in accessing healthcare (Shaw et al., 2020). Therefore, whilst this research responds to ‘inclusion health’, concepts of intersectionality and health equity can be useful in health research (Kelly et al., 2022) as well as considering wider determinants of health. Survey respondents acknowledged the multiple social needs of people on probation, with one commenting that ‘we could be here all day’ in listing needs. Wider determinants of health such as unemployment and accommodation are key known needs (HMPPS, 2022a) and survey respondents also considered financial challenges and social isolation were particular issues. Such factors are closely related to poor health and justice outcomes (Link et al., 2019).
However, there is a lack of research and understanding of health issues for those under community supervision (Skinner and Farrington, 2023). Williams et al. (2023: 5) also recognised gaps within the research and found within their study that ‘people on probation have significantly poorer self-reported health than that of the general population and a significantly higher prevalence of mental health conditions’. Building on their work in Wales, this study involved a survey of key informants who identified common health needs as mental health and substance misuse related. In addition, depression, stress and anxiety were the most commonly cited mental health concerns. Whilst there are limitations with using key informants to gather such information, respondent views were consistent with the literature concerning people on probation (Brooker et al., 2008; Brooker et al., 2020; Hatfield et al., 2004). Findings indicated overlaps in health needs, including dual diagnosis and mental health were a reoccurring theme throughout the research. However, it is possible that the scale of physical health issues did not emerge, given, for example, the lack of formal assessment by service providers and other barriers to reporting such issues.
Service provision for this group: A gap in broad health-related support
HMPPS in Wales commission and co-commission services of which the majority support mental health, emotional well-being and substance misuse. Whilst it is a strength that HMPPS are commissioning health-related services, many of these are targeted to certain cohorts and are limited in their attention to physical health. A broader set of services for adults were mapped (140 in total), primarily consisting of voluntary sector organisations, that provide needs-related services to people on probation. The services are geographically well-distributed and primarily relate to general support, employment and housing and to a lesser extent substance misuse and health. When also considering the commissioned services, there is a gap in providing health-related dedicated support for the population group. This may be particularly important given ‘people on probation have significantly greater use of GP services and hospital inpatient stays than the general population and utilise emergency departments often’ (Williams et al., 2023: 5). Indeed, there is no requirement for probation to have health-based workers although this is the case within youth offending teams (Brooker et al., 2023).
However, the survey respondent group (51 in total) did contain a significant proportion of organisations supporting health of people on probation. 86% of respondents indicated that their service identifies and/or assesses health needs or issues and 41% provide health-related services or clinics either directly or through a partnership/commissioned service. Collaborative examples include bloodborne virus testing, enhanced GP services and neurodiversity support. It is suggested integrated approaches can provide a more holistic response for supporting health needs of people on probation (Annison et al., 2019), such as benefits of integrated screening initiatives (Story et al., 2020). There is more to do to understand service provisions around health support, as well as developing health literacy and reducing barriers to encourage service access (Williams et al., 2022).
‘They fear they will be judged’: Barriers to healthcare
Inclusion health principles recognise that there are inequalities for certain population groups, such as people on probation, in accessing to health care. Barriers are reflective of systemic problems, particularly for prisoner leavers due to process issues, and service access, range and quality (Patel et al., 2018). Difficulties around communication and information sharing continue within the community (Parkes et al., 2012). The survey identified the key barriers to accessing health as service waiting lists, absence of services or service availability and mistrust of professionals. Whilst service pressures are unsurprising, the findings present two areas for further exploration. Firstly, it is unclear what particular health services are lacking for people on probation and whether the current services both statutory and non-statutory are meeting their needs in terms of supporting (or supporting access to) healthcare. For example, communicable diseases are known to be prevalent in this group yet only a quarter of respondents said their service has a policy or process to detect or support the management of communicable diseases. Secondly, the acknowledgement by over a third of respondents that ‘mistrust’ acts as a barrier is significant. This is compounded for ethnically diverse people in conflict with the law (Shaw et al., 2020). As one voluntary sector respondent said people on probation are ‘less likely to access services due to…fear they will be judged’ and another had observed individuals being ‘discriminated against because of their issues with substance misuse and offending’. Inclusion health groups face stigma (PHE, 2021), particularly those who are prison-experienced (Schnittker and John, 2007). Stigma and fear have been found to be barriers in accessing health checks in prison settings (Williams et al., 2022). When considering inclusion health populations, reducing barriers of stigma, such as improved staff training is important (Luchenski et al., 2018).
Concluding remarks
There are strong humanistic and economic arguments for developing an understanding of the health of people on probation to inform specialist interventions (Skinner and Farrington, 2023). Health inequalities exist for this population group because of complex multiple and overlapping factors, including mental health issues, substance misuse, offending behaviour and wider social needs. This is exacerbated by challenges accessing healthcare. Whilst there are efforts to put in place probation health strategies, these are said to be ‘hampered by differences in relation to the mandate for health provision, how health needs are assessed and how healthcare is commissioned and provided’ (Brooker et al., 2023: 275). Based on the findings within this exploratory article, there is an opportunity to increase the focus on healthcare for people on probation through inclusion health approaches.
Footnotes
Acknowledgements
The author would like to thank Jade Logan for her assistance with data collection in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Public Health Wales,