
Abstract
This article makes the case for the consideration of a humanitarian borderscape. The article analyses the recent humanitarian responses to irregular migration in the Mediterranean, Aegean and Greece and argues that processes of im/mobility produce specific times, spaces and types of care. The argument transcends recent discussions on the shrinking and/or expanding of humanitarian spaces, suggesting instead that a focus on the specific setting of the border and the dynamics of mobility are more useful to understanding humanitarian responses to mobility and immobility. In addition, the article contributes to the emerging literature on borderscapes by offering an interpretive analysis of the creation of a particular humanitarian borderscape made up of specific features and activities, which are undertaken by a multiplicity of actors in multiple places. Building on a consideration of this multiplicity, the article focuses specifically on the work of Médecins Sans Frontières.
MSF is not sans frontières; we're full of frontières, borders permeate everything we do and it's even worse in this migration crisis—MSF Humanitarian Affairs Coordinator, Athens, Greece.
Introduction
In the spring of 2015, the medical humanitarian movement Médecins Sans Frontières (MSF) installed water taps in a field next to a railway line on the Greek-FYROM border in an effort to provide clean water for migrants forced to sleep out in the open. In September 2015, in the same field, MSF erected the first tents of what became the transit space of Idomeni. The railway line at Idomeni had become a de facto border crossing for migrants denied passage at the official border crossing point on European highway E75, 1.5 km further east. Since early 2015, the border area around the railway line and Idomeni had seen migrant journeys interrupted on the way north to other parts of Europe. This interruption was the cause of various forms of suffering as journeys were delayed by border closures violently enforced by the FYROM police.
Throughout the autumn of 2015 and into 2016 the border and the transit space at Idomeni repeatedly opened and closed. Then in May 2016, the Greek authorities cleared the space. Idomeni offers us a microcosm of the politics and violence of im/mobility that have become intimately entwined with humanitarian attempts to offer some relief (see Jones et al., 2017; Pallister-Wilkins, 2017). Idomeni, however, is just one site in a large network of dispersed transit spaces, holding places and migration corridors that have been produced by borderworkers and humanitarian responders over the last decade and more, as migrants continue to confront and challenge Europe's exclusive border regime that sees them concomitantly in need of care (see Albahari, 2015).
As migrants encountered border restrictions on their journeys, humanitarian actors found that their efforts to provide assistance were not only conditioned by mobility and immobility but were repeatedly curtailed and challenged. This resulted in humanitarian agencies continuously re-orienting and relocating their activities in response to mobility, and as they try to find the time and space to offer care. Thus humanitarians struggle to provide what little humanitarian relief they can in often transient, makeshift conditions. It is this transience that has led me to mobilise the borderscapes approach. This approach, with its sensitivity to the multiplicity of practices that produce borders across time and space helps me make sense of actions that challenge traditional, usually fixed, (humanitarian) care giving. However, I argue that the humanitarian borderscape is a specific borderscape with particular features relating to im/mobility and the times, spaces and types of care.
Using borderscapes helps me to explore recent humanitarian interventions through a focus on what they tell us about ‘spaces of humanitarianism’ that are concerned not only with where humanitarian action takes place, but also humanitarianism as a field of action or possibility, and the shrinking or expanding of humanitarian space (Sandvik, 2016). Here, I cautiously build on the borderscapes literature to argue for borders as highly contingent and fluid entities working to condition, and being conditioned by, im/mobility. Such an approach enables me to account for the where and the how of humanitarian borderwork in Europe while considering the highly ambiguous nature of much of this action. Therefore, the decision to engage with the work on borderscapes is empirically driven by observations from the field. However, I use borderscapes cautiously, fully aware of the lack of a clear conceptualisation of exactly what a borderscape is, and the tendencies in borderscapes literature for both over-generalisation and over-specification (Tallis, 2017).
Instead, I argue for the humanitarian borderscape as a particular type of borderscape made up of an array of features and activities (Ingold, 1993; Tallis, 2017) relating to humanitarian practice. These features and activities while observable in the humanitarian borderscapes I studied, are also present in other sites, and continue to animate humanitarian practice elsewhere. Thus, while the humanitarian borderscape is a specific type of borderscape, it is not over-specified, as it is made up of socio-political processes, concerns and practices around im/mobility, risks and governance that can be uncovered elsewhere. In using borderscapes, this article offers an empirical analysis to compliment, yet build on, earlier theoretical work on borderscapes while expanding recent work on the humanitarian border.
The recent academic work on the humanitarian border has reflected the growing presence of humanitarian concerns in border control and border spaces. At the beginning of this decade, Walters drew our attention to the ‘reinvention of the border as a space of humanitarian government’ (2011: 138) emerging because ‘border crossing has become [for some]… a matter of life and death’ (2011: 139). Building on this and focusing on the policing of the US and the EU borders respectively, Williams (2015) and I (2015a) have shown the ways humanitarian logics concerned with those at risk have become intertwined with border policing practices more traditionally focused on migrants as a risk, resulting in complementary practices of care and control that expand possibilities for and types of practices at the border. Others have focused on the presence of humanitarian logics in technocratic migration management efforts (Andrijasevic and Walters, 2010) and counter-smuggling campaigns (see Garelli and Tazzioli, 2017; McNevin et al., 2016), while the growth of SAR efforts—in the Mediterranean especially—have led to an increasing focus on the work of both state (see Cuttitta, 2017; Little and Vaughan-Williams, 2016; Tazzioli, 2016) and non-state actors (see Stierl, 2016, 2017). Garelli and Tazzioli have shown how the enactment of categories of vulnerability and ethics of protection in migration control has come to produce particular types of border spaces in Italy (2017). Meanwhile, I have termed the work of non-state actors and the use of categories of vulnerability in border practices as ‘humanitarian borderwork’ (Jones et al., 2017). Humanitarian borderwork, I argue, ‘re-orients border practices around the provisions for particular forms of life and introduces explicitly humanitarian actors into the borderwork assemblage’ (Jones et al., 2017: 6).
It is on this body of work that my argument rests. However, I aim to advance the discussion beyond one concerned with the presence of complementary logics of care and control, or the inclusion of non-state actors, into borderwork (see Pallister-Wilkins, 2016, 2017). Cuttitta (2017) has recently argued that humanitarian borderwork follows the delocalisation of the border, while İşleyen (2017) has drawn our attention to the dynamics and productive role of mobility in governing transit migration. I want to focus specifically on what this delocalisation means for the work of humanitarian actors at the borders of Europe, while questioning what such work means for humanitarian practice and ongoing debates about humanitarianism (Scott-Smith, 2016), and the borderscape framework itself (Tallis, 2017).
Although not wanting to downplay the diversity of actors involved in humanitarian borderwork, the article focuses mainly on the work of MSF in this humanitarian borderscape. This is done for reasons of parsimony and coherence, but also because alongside the host of local actors engaged in humanitarian actions in a variety of locations, my fieldwork has consistently focused on MSF's actions, across a range of sites. My research with MSF began in the spring of 2015 with a series of interviews and conversations with members of the Operational Centres of Amsterdam and Brussels as well as MSF Greece. I visited Sicily in September 2015 and Greece multiple times between September 2015 and May 2016, and I continue my research engagement with MSF practitioners up until the present day in Athens and in the Operational Centres of Amsterdam and Brussels. I have formally interviewed over 30 MSF practitioners—in the field, in local headquarters and in the Operational Centres—and have had informal discussions with many more. These interviews have been semi-structured in nature and I employ an interpretive approach to analysis. But more than this, I am guided by the emerging focus on practice in critical security studies (Côté-Boucher et al., 2014) that argues for research to pay close attention not only to what security professionals 1 say but also what they do. As such, my fieldwork employs participant observation focused on the sites and humanitarian practices of humanitarian borderwork undertaken by MSF'ers in the field, as well as at their desks and in meetings. Further, I have had practitioners critically reflect on their own practice by running a workshop that was designed to explore the practices and socio-politics of MSF's work in European border spaces, and included medics, operational managers and advocacy specialists. 2
This article proceeds as follows. Firstly, the potential and limits of a borderscapes approach will be discussed, along with some of the current attempts to produce a borderscapes framework that is useful for comparative analyses of the rich variety of borderscapes that critical border studies engage with and render visible. Secondly, and building on my argument that the humanitarian borderscape is a specific type of borderscape made up of a specific array of features and activities, I discuss the particular aspects of humanitarianism and its practice that relate to these features and activities. Here, particular attention is paid to the humanitarian space as both a field of action as well as a particular time, space and type of intervention. Having laid out the foundations for the consideration of the humanitarian borderscape as one type of borderscape, I will then discuss how this particular borderscape came into being through features and activities relating to two interrelated themes growing from my fieldwork: im/mobility; and times, spaces and types of care.
Borderscapes
Within the field of critical border studies there has been an ongoing conversation about how to ‘de-centre the border’ and to account for and reveal the ways in which borders are in a ‘constant state of becoming’. This conversation has also argued for the border to become the starting point of investigation and not the taken-for-granted subject (Parker and Vaughan-Williams, 2012). Building on this, the concept of the borderscape has emerged, alluding not only to the productive and dynamic nature of borders as social practices of spatial differentiation, something often referred to as bordering (Paasi, 1998) or borderwork (Rumford, 2008), but also to the ‘dislocation, relocation and multiplication of borders and their functions and practices through borders’ distribution and proliferation in a variety of social and political arenas’ (Brambilla, 2015: 15). As a result it is argued that border studies needs ‘retooling in the face of the diffusion and complexification of borders’ (Brambilla, 2015: 16).
Building on Appadurai's work on scapes (1996) that used such a concept to present the interconnected yet fractured and contested nature of the world under globalisation, the work on borderscapes by Rajaram and Grundy-Warr in their edited volume sought to consider the border as ‘mobile perspectival, and relational’ as well as the border as a zone ‘where the multiplicity and chaos of the universal and the discomfits and possibilities of the body intrude’ (2007: x). For Rajaram and Grundy-Warr, simply thinking of the border as a space of inclusion and exclusion occludes the role that society plays in ameliorating and affecting space (2007: xxviii).
Here, the borderscape approach enables both a reflection of the ‘spatial and conceptual complexity of the border as fluid and shifting, biopolitical, discursive and socially produced’ (Perera, 2007) and ‘shifting, displaced, negotiated, visible and invisible’ in location (Brambilla, 2015: 19). ‘Kaleidoscopic’ in their variability, borders are constantly doing and undoing, and tracing and retracing, and the ‘gaze’ of the borderscape enables ‘variations of borders in space and time, and in different settings criss-crossed by negotiations between a variety of different actors, not only the state’ to be grasped (Brambilla, 2015: 25). As Parker and Vaughan-Williams have argued, ‘borders also travel’ like the migrants they aim to control (2012: 730).
That said, for all the calls for and talk of retooling our understanding of borders, borderscapes remains under-conceptualised. As I have briefly outlined, much of the work on borderscapes states the potential of using the approach in accounting for the diversity and constructed nature of borders. It appears as if it can be all things to all borders and by extension border scholars. Agier celebrates the instability of borders that takes centre stage in the borderscape idea as enabling at least recognition of the relational aspects of the border. However, Agier suggests that Appadurai's stretching of the scapes metaphor looses the ability for reference. As a result, Agier calls for a return to ‘the question of the drawing of borders’ (2016: 44). But how do we answer questions about the drawing of borders?
This loss of reference identified by Agier, Tallis 3 argues, leads to two problems: over-generalisation, and over-specification (Tallis, 2017). In the over-generalised borderscape, borders are heterogeneous entities that appear everywhere and are a central part of political life, leading to a loss of distinctiveness. Tallis suggests that this results in borders becoming hard to ‘specify or disentangle from the wider socio-political field or for over-generalised analyses that often become instrumentalised to make wider critical points about oppressive governance that can lack nuance and subjectivity’ (2017: 4). Alongside this, Tallis argues that over-specification comes with its own set of problems. Based as these studies are on anthropological and ethnographic studies of the border, they are thick with descriptions of specific border sites and practices but raise problems for border studies, which is inherently multi-disciplinary in nature (2017: 5). This over-specification stands in the way of the development of comparative frameworks and greater conceptual development and encumbers attempts at theory building that go beyond border studies and into wider socio-political research (Tallis, 2017: 5).
Helpfully, while highlighting the limits of the borderscape approach, Tallis also suggests a way to move beyond what may at first appear to be an impasse, with border and other critical post-structuralist influenced scholars—myself included—not wishing to return to the idea of fixed knowledge about the border. On the other hand, I am keen not to fall back into borderscapes being all things to all borders, and want to be able to account for the geographical, historical, political and social contingency of the humanitarian borderscape, while guarding against over-specification.
Here, Tallis suggests it is useful to return to earlier work on landscape (2017: 8). Ingold conceptualises landscape as being made up of ‘an array of related features’ and ‘an array of related activities’ (1993). Ingold's ‘related arrays of features and activities’ here allow for a consideration of plurality while importantly calling attention to how such pluralities are formed and interact. It also speaks to how these related features and activities might be present in wider socio-political processes beyond the border in a similar vein to Nail's work on assemblages (2017). Meanwhile focusing on both the array and the idea of related features and activities it becomes possible to identify and map specific types of borderscape, highlighting similarities and differences in the process, enabling us to analyse what kind of borderscape is being studied and where it can be found.
Therefore, in trying to make sense of the wide variety of practices across times and spaces that I encountered in my fieldwork, and focusing on what is relational about the features and activities, I argue for a humanitarian borderscape. This humanitarian borderscape is made up of particular humanitarian-related features and activities that are both particular to the borderscape in question but can also be found in wider socio-political processes concerning humanitarianism and wider practices of biopolitical security. It is to a discussion of these that I now turn.
Humanitarian features and activities
A discussion of humanitarian practice at or in response to borders requires an understanding of how humanitarianism in the present relates to and works with space. Spatial analyses of humanitarian action have been mainly concerned with three areas: one, the role of territorialised humanitarian action in the space of refugee camps (Agier, 2011) or the medical clinic (Brauman, 2012; Redfield, 2013); two, the de-territorialising and re-territorialising nature of humanitarianism (Debrix, 1998); and three, the shrinking or expansion of humanitarian space as a field of action (Sandvik, 2016). The array of related humanitarian features and activities enacted over the previous two years and earlier in response to migrants' arrivals in Europe challenge much of what we know in all of these areas and calls for a reassessment of humanitarianism's relationship with space as a result.
Practitioner-led analyses of the territorialisation of humanitarianism in refugee camps have sought to critique and move beyond the camp as the default modus operandi for displaced populations (Chkam, 2016). This recognises that, increasingly, displaced people in today's world are not resident in camp settings, and that the camp itself is routinely considered by humanitarians to be a problematic site of governance for problematic/risky populations (Agier, 2011). Meanwhile, within medical humanitarianism, clinics, triage centres or hospitals remain the key sites for the provision of care to static, at risk, populations (Redfield, 2013). The territorialised model of governance encompassed by the refugee camp and the clinic is challenged by the actions and desires of migrants when movement is the principle agent and mobility equates to a life with what is thought to be a secure future. As such, within the context of migrants in Europe, the logic of the refugee camp or the clinic as a tool of humanitarian government where and when it occurs is linked both to territorialising of care and the de- and re-territorialising nature of mobile populations. It is to this ambiguous nature of humanitarian space today, which I now want to turn.
Humanitarianism engages with the theoretically borderless world of a universal ethics—while at the same time producing hierarchical relationships of power (Debrix, 1998; Deleuze and Guattari, 2004). Humanitarianism appeals to the universality of humanity and with it supposedly transcends the international state system. At the same time, through enacting sovereign practices that govern life, humanitarianism works with and through space, and constitutes space, in particular ways. Put simply, while universal in its ethical approach and appeal to human life, humanitarianism is performed somewhere and through something and is thus also particular, made up of a particular array of features and activities. In addition, these features and activities produce new boundaries or consolidate existing ones in the shape of categorisations of life, such as those considered in need of assistance, e.g. Syrian refugees, and those considered to be economic migrants, e.g. Moroccans (Fassin, 2012; Jones, 2009).
Recent work engaging with the space or spaces of humanitarianism has been principally focused on fields of intervention concerning the preservation of life, the provision of relief and questions concerning the contracting or expanding nature of these fields (Sandvik, 2016). This argument builds on the specific conceptualisation made famous by MSF's Rony Brauman of the espace humanitaire as a space where humanitarians driven by particular rationalities concerned with universal humanity, a relief of suffering and respect for human dignity act independently of state politics (Hubert and Brassard-Boudreau, 2010). This independent action itself differs and sets its own boundaries of intervention depending on the practitioners involved and the particular ‘crisis’ concerned (Brauman, 2012, see also Weizman, 2011).
In addressing these boundaries of intervention, debates have tended to argue for a contraction of the possibilities for action and thus a shrinking of the espace humanitaire—that is, the possibility for action (Collinson and Elhawary, 2012). This argument considers the increasingly insecure settings in which humanitarian actors operate (Tennant et al., 2010), the heightened levels of risk faced by personnel on the ground, the concomitant colonisation of the espace humanitaire by states, their militaries and their foreign policy aims (Derderian et al., 2013), subsequent problems with humanitarian access, and the shrinking of an independent operational capability. As Sandvik argues, ‘the notion of the shrinking humanitarian space is both a normative claim about the proper role of humanitarian actors and a set of claims about the nature of threats to the humanitarian space’ (2015: 4). Within this framework of normative claims and perceived and actualised threats, there are those that argue for the expanding of humanitarian space based on a retreat of social welfare and a return of private philanthropy (Fassin, 2012), an increase in humanitarian aid budgets, or the growing possibilities offered by information technology (Sandvik, 2016).
However, within the context of humanitarian action in Europe's borderlands, arguments over the shrinking and/or expanding of humanitarian space fail to account for the fluid nature of the field in terms of access, independence, the proliferation of actors and the types of emergency being addressed. As such, the field of intervention appears markedly different, structured as it is by the forces of mobility and immobility relating to European border policies and practices, and the continuation of territorialised borders of exclusion for migrants (see Scott-Smith, 2016); supporting Weizman's argument that politics needs to be considered in discussions about the humanitarian space (2011: 58–61). One cannot account for the presence of humanitarian actors in SAR missions, on the one hand, and the simultaneous reliance of these actors on state-produced information and legal permission—that makes such missions possible using the rubric of shrinking or expanding space—on the other. At one and the same time, SAR missions seem to expand the field of interventions, generating new times and spaces of intervention, while challenging the independence of humanitarian action. As Brauman himself makes clear, the humanitarian ‘field is defined not by a particular set of techniques but by the setting in which such action takes place’ (2012: 7).
Therefore, the space of action impacts and structures the form of humanitarian practice being undertaken. But others have argued that this is not a one-way process and that humanitarian practice or techniques, to use Brauman's terminology, also work to structure space in particular ways. Here it is useful to return to Debrix's (1998) earlier work on humanitarianism that is both de-territorialising, as it is universal, and re-territorialising, as it happens somewhere and through particular practices that employ particular ideas and categories of life that order the world in particular ways. Alongside this are arguments around humanitarianism as a form of liberal government, where humanitarian rationalities enable a concomitant expansion of the moral field of action, broadly concerned with care coupled with a subsequent rationalisation of population governance (see Lester and Dussart, 2013; Reid-Henry, 2014).
These arguments around the genealogy of liberal government point to the limits of the espace humanitaire as a space of action independent of broader socio-political processes concerned with the security of populations (Foucault, 2009). In Debrix's work on MSF, he argues that as humanitarian actors, MSF have the ability to both challenge the international order of territorialised and sovereign states and at the same time consolidate it by everyday practices of reterritorialisation through processes of triage or ordering that enact hierarchies of humanitarian victimhood, or what Fassin calls a ‘politics of life’ (2012). These processes of categorising humanitarian victims that enact processes of inclusion and exclusion can be understood as a form of bordering (Jones, 2009). But more than this I argue, building on the work of Reid-Henry (2014), that humanitarian techniques also reproduce particular logics of risk management, rationalisation efficiency and efficacy we have come to recognise as belonging to the modern liberal state.
Thus, in discussing humanitarian practice in the present, and thinking about such practice in relation to the border, an array of features and activities emerge. These coalesce around ‘settings’ and ‘techniques’ as Brauman would call them or what Ingold might term ‘features and activities’ (Ingold, 1993). In the following section I discuss these settings and techniques, features and activities, how they relate to each other and how they come to construct a particular humanitarian borderscape through the role of im/mobility in structuring times, spaces and types of care.
The making of a Humanitarian borderscape
The emergent and ephemeral humanitarian borderscape is structured and conditioned by the im/mobility of migrants as they are channelled through ‘corridors’ and ‘narrow bands’ structured by border controls and transport infrastructures (see Figure 1). The structural conditions that limit migrants’ agency have been likened to a ‘chain of complicity’ that ‘undermines people's ability to seek refuge’ (Whittall, 2016). This chain takes the form of corridors, narrow bands, ‘gauntlets’ (Whittall, 2016) or ‘obstacle courses’ (MSF, 2015) that work to structure the places and spaces of humanitarian assistance, likened by one MSF specialist in migration and displacement to ‘humanitarianism in a queue’ (interview with author, 12 May 2016) and leading to uneven and spatially disaggregated forms of intervention that, as the same migration and displacement specialist says, ‘respond in limited ways to need’.
Migratory routes, February 2016, ©MSF.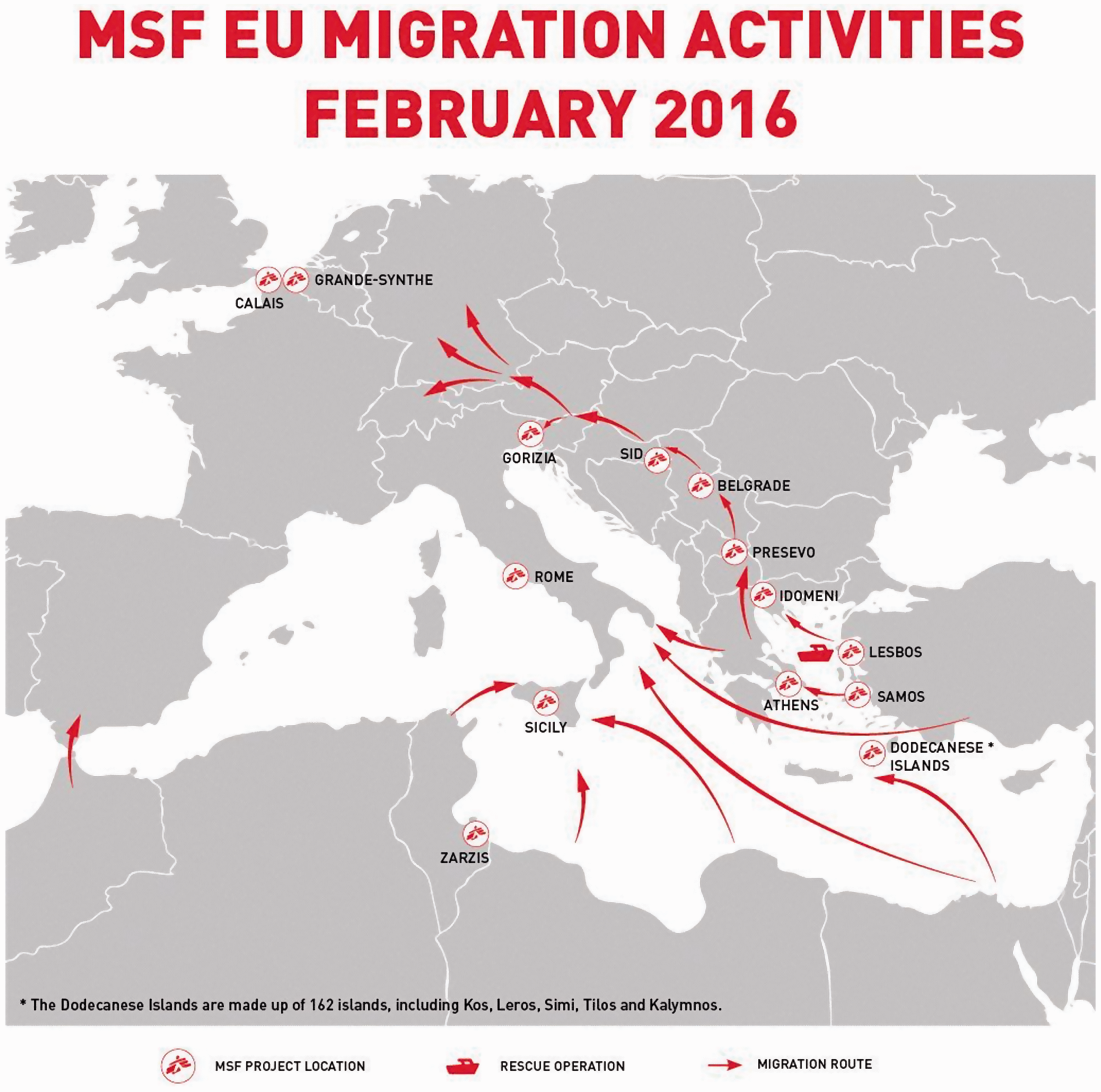
Humanitarian practices exist at multiple sites and scales that correspond to the corridors and narrow bands along which migrants travel—at sea, on boats, at ports, train and bus stations, transit service stations at the sides of roads and in border waiting areas—and thus the geography of humanitarian borderwork is intimately linked to processes of im/mobility that come to structure humanitarian assistance at various times, in various ways and in various spaces, so that MSF can claim to be present in offering assistance ‘all the way along the chain’ or the ‘queue’. Such geography challenges the spatial and temporal traditions of humanitarian intervention in refugee camps (Hyndman, 2000), medical clinics and hospitals (Brauman, 2012), while at the same time speaking to the role of mobility in many of MSF's missions elsewhere (see Healy and Tiller, 2016; Ponthieu and Incerti, 2016; Redfield, 2013).
Here, the uneven geographies of Europe's borders, from the Mediterranean Sea to the European motorway network, render humanitarian assistance spatio-temporally possible while concomitantly limiting it. In offering a more detailed discussion of how a humanitarian borderscape comes to be produced through the relationship between im/mobility and its structuring of times, spaces and types of care, the following discussion focuses on and is built around a number of key and illustrative fieldwork sites.
Im/mobility, transit and humanitarian intervention on Lesvos
To illustrate the way im/mobility impacts times, spaces and types of care and is thus a feature of the humanitarian borderscape it is useful to begin by mapping the times and spaces of intervention on the island of Lesvos. The intervention mapped below (see Figure 2) is only that performed by MSF and should be understood as happening within an environment that sees a multiplicity of other humanitarian actors concomitantly offering assistance. What is described is a composite picture of those times and spaces in which MSF practitioners were present offering assistance; it should neither be understood as comprehensive nor read as encompassing every migrant's journey.
Mobility, transit and sites of humanitarian intervention on Lesvos, ©Polly Pallister-Wilkins.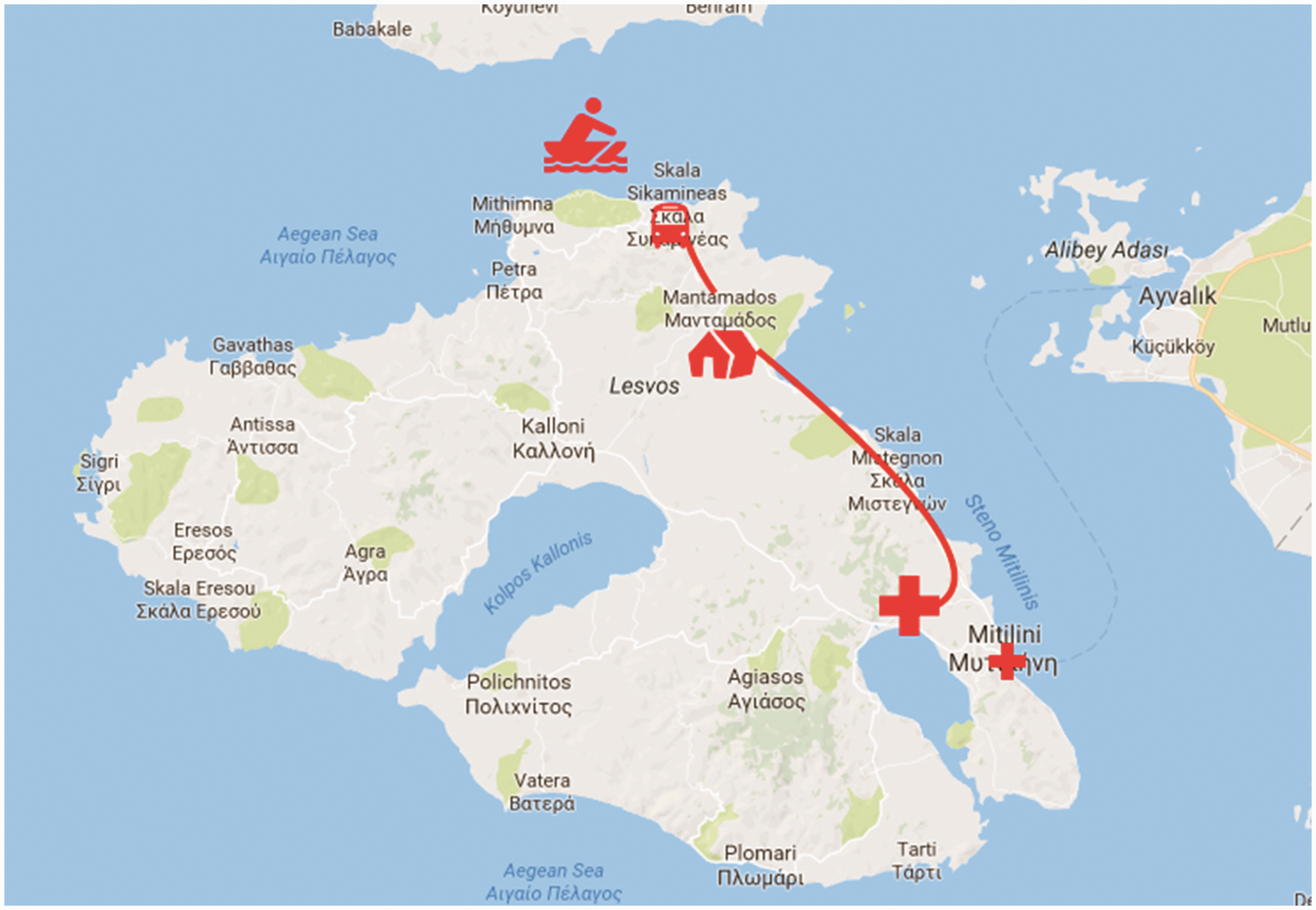
In December 2015, migrants arriving in Lesvos would have first encountered MSF at sea (see Figure 3) as they engaged in what can best be described as pre-emptive SAR missions. Here, MSF along with partners from Greenpeace worked from a rigid-hull inflatable boat to monitor and guide the rubber dinghies and other small vessels making the 10–12 km crossing from Turkey to safe places of disembarkation on the beaches.
4
Similar to MSF SAR operations a Norwegian SAR team help push a migrant dinghy with a failed motor to the Lesvos shore, October 2015, ©Polly Pallister-Wilkins.
Migrants would then encounter MSF again when they took one of the MSF-contracted buses from the village of Skala Sikamineas on the north-east shore.
5
After a 20 km drive they could wait, sleep, get warm, pick up blankets, receive information or use the Wi-Fi network at the MSF-run transit point at Manatamados, from where they caught another bus to the Moria ‘hotspot’ to register with the Greek police and Frontex. At Moria, people may have received basic medical triage from MSF medical practitioners working inside the hotspot (see Figure 4). At certain times, the authorities on the island accommodated predominantly families, understood as more vulnerable, or Syrians, believed to be more deserving as ‘genuine refugees’, at Kara Tepe, where MSF also provided cultural mediators and medical services using one of its mobile clinics. Before the implementation of the EU-Turkey Statement on 22 March 2016, people at Moria or Kara Tepe, once registered, were ‘free’ to carry on their journeys to mainland Greece and beyond.
MSF Clinic, Moria Hotspot, November 2015, ©Polly Pallister-Wilkins.
Im/mobility worked to structure times, spaces and types of care on Lesvos in other ways. Needs emerged and disappeared as mobility fluctuated and was impacted not only by the numbers of mobile people that could cause bottlenecks but also by external factors such as a delayed shipment of rubber dinghies to Turkey from a factory in China (interview with a member of the Koninklijk Marechaussee on secondment with Frontex, Moria hotspot, 23 November 2015) or the weather conditions. Boat arrivals in Lesvos were and continue to be greatly impacted by weather conditions, especially wind direction, which had knock-on effects all the way along the ‘queue’, from the shore to the hotspot. When I first visited Moria in October 2015 the preceding days had seen the largest number of arrivals on the island that year. Every day in late October, thousands of people were landing on the northern beaches in favourable weather conditions and before new border obstacles and closures were put in their way. The day before my first visit to Moria the weather turned, with torrential rain and strong winds that continued on the day of my first visit to Moria. By the time, I arrived at the hotspot in the mid-afternoon, I met people who I had seen arrive on the beaches four days earlier standing knee-deep in mud or worse, waiting to register with the authorities before they could gain access to the inside of the hotspot and avail themselves of what humanitarian assistance was available. At this moment, MSF and other humanitarian practitioners were overburdened by the numbers of people, the weather and the poor infrastructural conditions of the hotspot itself, with the public health specialist I was shadowing saying it was the worse conditions they had ever worked in (conversation with author, 24 October 2015).
On my next visit, a month later, there had been no arrivals on the island for the previous few days as heavy winds from the south made the crossing from Turkey almost impossible. The hotspot was empty but for unaccompanied minors being kept in ‘protective custody’. Making the most of the quiet, MSF took the opportunity to strengthen their infrastructure within the hotspot, replacing their triage tents (see Figure 4) with portacabins that would later be abandoned, after MSF withdrew following the EU-Turkey statement. This underlined that much of MSF's work on Lesvos was ‘only intended as temporary measures’ (MSF Greece spokesperson, conversation with author, 30 November 2015).
All of these encounters then are tempered and structured by a combination of im/mobility, transport infrastructures and the limits of humanitarian triage itself (Redfield, 2013). Here what MSF calls the ‘limitation of means’ (MSF, 1999) in terms of time, space and resources worked to limit the provision of care. Triage, here, renders visible the ‘limitation of means and the making of choices’ (MSF, 1999) within humanitarianism, which operates theoretically on universal ideals of relieving suffering and upholding human dignity, but in practice focuses on those in need, and thus is itself hierarchical and uneven as well as a producer of new categories of life built around vulnerability and need (see Pallister-Wilkins, 2017). Meanwhile on Lesvos and elsewhere, the possibility for intervention to provide care and medical assistance was structured by the desires of migrants to keep moving. In many instances, those needing further medical attention would refuse or forego treatment in order to carry on their journeys. This was stated bluntly as ‘movement is life!’ by an MSF public health specialist (conversation with author, 24 October 2015) with movement here being productive of the humanitarian borderwork that seeks to protect such life. The transit point at Mantamados is a case in point.
The limited care of Mantamados
Scaling down further and looking at one site in the humanitarian borderscape helps to further uncover the relationship between im/mobility and its structuring of times, spaces and types of care. Mantamados was constructed by MSF in the autumn of 2015 as a transit point on the journey from the north shore of Lesvos to the hotspot of Moria. Built to both regulate the movement of migrants from the arrival beaches to the registration point and as a site for migrants to briefly rest, change their clothes or sleep if they arrived late in the evening, it was also a place in which migrants, arriving after the last buses had left Skala Sikamineas, could reach on foot to sleep and catch a bus the next morning.
The role of transportation itself in producing Mantamados is illuminating for thinking about the role of im/mobility in the humanitarian borderscape (see Figure 5). Designed specifically to act as both a place through which people moved and a place to regulate that movement, it also acted as a transport hub, from which MSF-contracted buses moved migrants from the beaches to the hotspot. Even the provision of a bus service itself is something of a departure for a medical humanitarian organisation more used to providing assistance in clinics and hospitals. If they provide transportation at all, it is most usually in the form of ambulances transporting patients to and from their homes or camps to clinics and hospitals (Redfield, 2013). Mobility, or the desire for mobility on the part of migrants, and the risks of that mobility—the roads migrants would have to walk on if no transportation was offered were dangerous—spurred MSF into offering the buses. Here, then, the buses themselves were a form of care: a way of pre-emptively managing the risks of a dangerous walk, transposing the logics of public health and an ethos of ‘do no harm’ onto the provision of transportation.
One of the signs dotted along the road to Mantamados, November 2015, ©Polly Pallister-Wilkins.
Mantamados was intimately shaped as a space of transit through this relationship to transportation and the fostering and governing of mobility. As a staging post on the journey between the northern shore and registration in Moria, Mantamados acted as a sort of mobile triage point in a similar way to an emergency room or doctor's surgery regulates the admission of patients to a hospital. The will of migrants to keep going, and the desire by MSF to respect and foster such ‘vital mobility’ (Redfield, 2013) and to keep the queue moving, was reflected in the transit space itself and the type of assistance it offered. Care requires and takes time. Even the quickest triage which seeks to filter and sort patients according to need to maximise efficiency requires time as well as space.
MSF medical practitioners also highlighted the ethical considerations for the provision of care. Doctors have an obligation to treat patients after diagnosis. If you provide the means of and perform the act of diagnosis then you are ethically obligated to treat. Treatment here does not just mean the initial phase of prescribing a medicine or tending a wound, but also entails follow-up. Doctors and other medical staff should follow up on treatment with their patients to ascertain whether a particular intervention is working or has perhaps caused further complication. This is why medical treatment traditionally requires forms of stasis where patients can be monitored, tests performed, treatment administered and referrals made if necessary. 6 Such ethical considerations were in tension, as we have seen, with the desires of migrants themselves who wanted to keep moving, to register, to leave the island and to continue their journeys.
This intimate relationship between im/mobility and the times, spaces and types of care was rendered into material form in the information provided in Mantamados itself (see Figure 6). These signs provided in Arabic and Dari as well as English made clear that the space was only to be used for limited periods of time and was for all intents and purposes nothing more than a bus stop. Migrants were instructed that the transit centre exists to provide ‘transportation to the registration camp [Moria]’ and that ‘there are medical consultations in the registration camp where you can get medical care.’ This at first appears a striking thing for a medical humanitarian organisation to say: ‘you cannot get medical attention here’ seems counter-intuitive to the aims of MSF. However, when we consider Mantamados and its purpose in light of mobility and the medical ethics around treatment discussed then the active denial of treatment becomes clearer. When considerations of limited resources and their most effective use are taken into account, only providing medical attention in the ‘registration camp’ in Moria becomes operationally understandable. In addition, Moria is located much closer to the hospital in Mytilene where any patients needing referrals for serious conditions could more easily and quickly be admitted. Meanwhile, the instruction to ‘take with you the blanket you are given. You will need it as the weather is getting colder and winter is coming’ shows attempts at a very limited form of what we could term ‘bare care’, in which the very basics such as warmth in the form of blankets are provided remotely and on the move as migrants continue their journeys.
Sign at Mantamados making clear the purpose of the transit space, November 2015, ©Polly Pallister-Wilkins.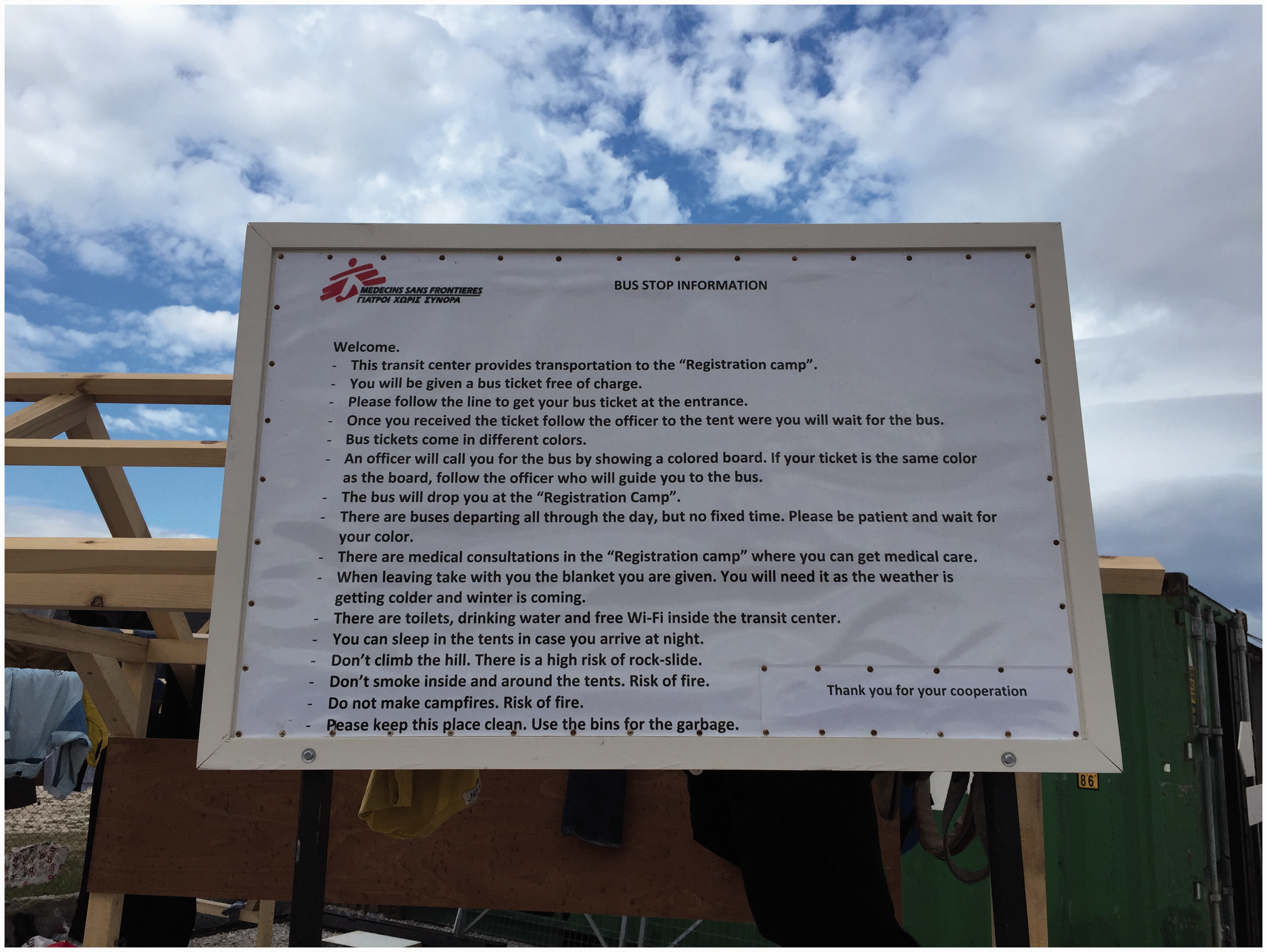
Im/mobility and the times and spaces of care in Idomeni and Polykastro
The border as a space is not fixed but fluid and shifting (see Figure 7). As Perera has discussed, the borderscape is produced through (amongst other things) the mobility of migrant bodies and attempts to organise, control and terminate their movements (2007: 206). Here, the spatially disaggregated and multi-scalar nature of the border is coterminous with spatio-temporally limited practices in the types of borderwork performed and border spaces produced.
Shifting spaces of care at Idomeni and Polykastro, ©Polly Pallister-Wilkins.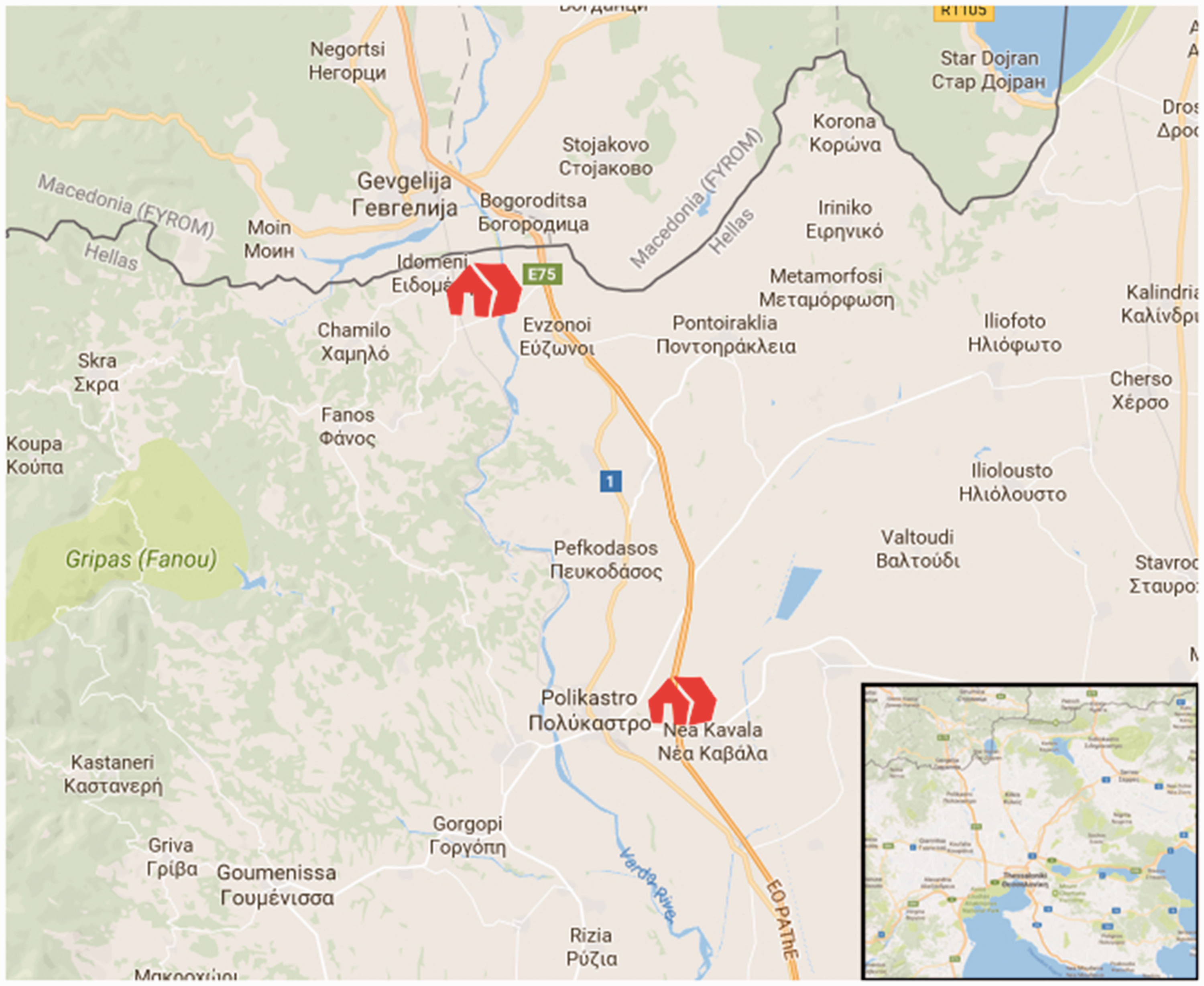
During my field research many of the spaces produced through humanitarian borderwork underwent considerable changes of use over the 6–12 months of my visits. As humanitarian intervention responded to changes in the mobilities of migrants and border closures, spaces took on different roles, moved or were reanimated and reinvented. This has been described as ‘adaptation’ according to one specialist (discussion with author, 14 November 2016). This adaptation comes about in response to migrants’ im/mobility, which determines not only when and where humanitarian assistance is provided but also creates the need for such assistance in the first instance. Idomeni is an illustrative site in the humanitarian borderscape in this regard.
‘Everything changes, all the time, every day. We have gone from nothing to a huge transit camp, to the camp now being closed again,’ was how the director of field operations for Idomeni described it to me early one January morning in 2016 sitting in MSF's office in Polykastro, 20 km south of the Greek-FYROM border. At this time Idomeni was closed (see Figure 8) by MSF while discussions were ongoing about allowing the Greek police use of the space to carry out what one MSF Humanitarian Affairs advisor in Athens called ‘border triage’ (interview with author, 14 January 2016). Rather than allow the Greek police to use the space for ‘border triage’, or border policing, MSF made the decision to close Idomeni during December 2015 and January 2016. In this instance, MSF's ‘ethic of refusal’ and humanitarian principles of neutrality and non-collusion with state authorities in their humanitarian space structured their actions even while the decision to close the space caused divisions between different national associations. In turn this upholding of humanitarian principles reconfigured borderwork and the borderscape itself according to humanitarian principles.
An empty Idomeni, January 2016, ©Polly Pallister-Wilkins.
Instead of arriving in Idomeni, migrants coming on buses from the ferries in Athens would be directed off the E75 highway by the police at the northbound EKO service station at Polykastro. Here, migrants' movement towards the FYROM border at Idomeni would be regulated by the Greek police, which turned the service station at Polykastro into a site of interruption, transit and humanitarian borderwork, as MSF attempted to respond to the needs of people made to wait (see Figure 9). Thus Polykastro underlines the temporally limited nature of humanitarian borderwork that responds to people's mobility and changes in European border control in a back-and-forth between migrant agency and a state's often violent attempts at control.
EKO service station, E75, Polykastro, January 2016, ©Polly Pallister-Wilkins.
The humanitarian interventions at Idomeni and Polykastro speak to François Debrix's argument around the new geographies that international medical assistance creates through interventions in time and space. According to Debrix, MSF with its tradition of ingérence—roughly meaning interference or a right to intervene—both upsets state-based spatial arrangements concerned with territorial control and the protection of the population, and consolidates other forms of sovereignty and government (1998). For Debrix (1998), MSF's work through their power over life and death and engagement in governmental practices constitutes and orders space in particular ways performing new territorial strategies and engaging in a politics of ordering around humanitarian categories of need or what Fassin has called a ‘politics of life’ (2012).
I argue that MSF's humanitarian borderwork both destabilises and restabilises border spaces in clear, concrete ways related to the im/mobility of migrants, the opening and closing of borders, the shifting of border controls away from the border and the categorisations of vulnerability that are performed as part of care giving. At Idomeni and Polykastro, MSF's borderwork was structured through the opening and closing of the border, yet created new types of border spaces concerned with the provision of care in addition to control. As a transit space that existed extra-legally without the permission of the local municipality or the national Greek government, Idomeni clearly unsettled traditional territorial and governmental arrangements, while also providing MSF with a space and a way of performing its own politics of life based not on categorising migrants according to their citizenship or right to move across the border but instead according to their vulnerability (MSF, 2016b). Both Idomeni and Polykastro as spaces exist through their relationship to the border and the ways in which it impacts on migrant im/mobility, causing interruption and at times harm (MSF, 2016c). Thus, the violence of the border is recognised and alleviated but remains, structuring MSF's practices on the ground.
The search and rescue ship as a fleeting time and mobile space of care
The violence of Europe's borders to those migrants excluded from the privileges of visa-free travel is most stark in the Mediterranean Sea, where at the time of writing, 14,318 people are known to have died since 2014. 7 In response to this danger to life, MSF began SAR operations in May 2015. Initially providing medical assistance on-board the MOAS' (Migrant Offshore Aid Station) boat the MY Phoenix, soon MSF was running boats of its own: the Bourbon Argos, the Dignity I and lately the Prudence, while also—after the co-operation with MOAS collapsed—joining forces with SOS Méditerranée on their boat the Aquarius. These SAR vessels are joined by those of other organisations, and each one is a floating, mobile space of humanitarian rescue and care. However, like elsewhere in the humanitarian borderscape, this care is tempered by the conditions of im/mobility that make up the Mediterranean border space.
Humanitarianism at sea works to ‘assist people who have not yet arrived in Europe, people EU States are not keen on receiving in the first place’ (Deleuze G and Guattari F (2004): 22–40), and unlike the transit spaces discussed, or the bus services that performed care or pre-emptive risk management through the provision of transportation, SAR efforts produce a mobile humanitarianism that cannot easily be fixed in time or space. SAR occurs where rescue is needed; it is not restricted by transport infrastructures such as road networks. As such it is the risk to life caused by the Mediterranean's violent and exclusive border that structures the time, space and type of care, in this case rescue. But in addition, the types of care that can be offered are conditioned by the setting and by the particular risks faced and harm experienced by rescued migrants. Similar to the limited nature of care offered in transit spaces, the medical facilities available on the SAR ships are limited, but unlike the transit spaces, are limited not only by migrants’ desires to keep moving or because of an ethical hesitation to diagnose and treat without adequate chance to follow up, but also by the very conditions of being a boat at sea.
These are not hospital ships, but first and foremost rescue vessels designed to save and accommodate as many lives as possible (see Figure 10). The mere act of rescue in this instance becomes to some extent a medical humanitarian act (interview with author 29 April 2015) in a stark illustration of the ways humanitarianism can and is about intervening in life and death. That being said the initial decision by the Operational Centre Amsterdam to undertake SAR was taken after what one of the architects called ‘intense internal discussion’ (conversation with author, 29 April 2015; for a full account and reflection see del Valle, 2004), while disagreements and questions emerged over whether there was a distinct medical humanitarian need for engaging in SAR. Other discussions concerned the ‘legality’ of those being rescued (interview with author, 29 April 2015; discussions with author, 30 May and 12 September 2015; for more see Pallister-Wilkins, 2015b) or how the organisation could offset accusations of being a pull factor and engaging in smuggling (discussions with author, 30 May 2015). These debates continue and MSF has to constantly defend itself against both criticism that it is colluding with smugglers (see Wintour, 2017) and fears of co-optation into broader efforts at border control (MSF, 2017a).
Medical round on the Prudence, ©MSF_Sea.
The limits placed on the types of care provided by SAR operations underline the problems faced by those trying to provide medical care in mobile conditions. Many of the conditions practitioners encounter are complex: some are long-running medical conditions, others are exacerbated or caused by the journeys migrants have taken (discussions with author, 14 November 2016, 4 and 20 May 2017), and others by the risks of the dangerous sea crossing itself. Psychosocial trauma is a key issue faced by the MSF'ers on the SAR boats. In addressing the acute and complex psychosocial needs of migrants, practitioners face similar hurdles to those medical professionals in land-based operations, namely a need for time, safe spaces and the ability to carry out long-term continuity of care. One practitioner commented: Sometimes our patients don't need intensive medical intervention and we can't provide it on the ship in the brief time that we have with them, sometimes the best that we can do is just to hold someone's hand and to make that human connection, to let them know that in that moment they are safe. (interview with author, 20 May 2017)
Here, affective care comes to stand in for the ability to provide more comprehensive long-term assistance. ‘The best that we can do is ensure that upon disembarkation people are referred to get the help they need. This may be from our MSF teams in Italy or from the Italian health service’ (interview with author, 20 May 2017). It is very clear therefore that the humanitarian borderscape under these delocalised (see Cuttitta, 2017) conditions has very particular (limited) features and shapes and is sculpted by specific activities relating to the act of rescue at sea.
Conclusion
In this article, I have tried to make sense of the humanitarian actions undertaken in Europe's border spaces in response to migrant im/mobility and the risks they face. I have argued that the humanitarian borderscape is a specific type of borderscape structured through the relationship between im/mobility and the times, spaces and types of care. The argument is focused on what the border does to humanitarian practice and not only what humanitarian practice does to borderwork and as such is different from previous work on the humanitarian border. The article has shown how humanitarian practice, like the border itself, is influenced by the settings and the types of work or practices carried out, and as such is always in a state of becoming. Attempts to conceptualise humanitarian practice as it responds to migrant im/mobilities within fixed and linear processes—from violent borders to humanitarian borders—are thus inadequate in portraying humanitarian work at the border.
Any discussion of these features and activities, of im/mobility and the times, spaces and types of care that make up the humanitarian borderscape, cannot avoid also addressing the exclusive and violent nature of the border in structuring the field of action or the espace humanitaire. It might seem banal to stress that humanitarian action that works to construct a humanitarian borderscape is dependent on those very structures for conditioning the scene, but such a claim speaks to the wider social processes underpinning and also growing from the humanitarian borderscape. Such a discussion points to one of the key tensions for humanitarian practice both within its work in the borderscape, as unpacked in this article, but also beyond, namely what type of politics to promote when working with mobility (see Scott-Smith, 2016: 2).
In thinking about this politics in relation to mobility I have shown how mobility unsettles and restructures humanitarian practice. Mobility is a setting, while intervening to reduce the harm faced by mobile populations is a stated aim of those humanitarians responding to the suffering produced by violent borders (Brauman, 2012). Mobility, or perhaps I should say immobility, is thus a wider socio-political process with particular affects addressed by humanitarian action in limited and highly prescribed ways. As Scott-Smith argues: the key issue in contemporary humanitarianism… is not that humanitarian solutions are insufficient. It is that humanitarian problems are insufficient. Framing an issue as a distinctly humanitarian one necessarily limits the responses available. Seeing inescapably political issues as humanitarian ones, in other words, can seriously curtail the possibilities for reducing suffering, and nowhere is this more evident than in the recent migration crisis. (2016: 3)
Humanitarian practice, as I have shown, is intimately shaped by the features of im/mobility, responding with specific activities best described as limited attempts at care provision. However, mobility remains in tension with humanitarian practice, especially of the medical kind, which requires fixed spaces and sufficient time for effective, adequate and ethically sound treatment to be carried out. Humanitarian practice continues to confront the ‘problems’ migrant mobility engenders in Europe and elsewhere (MSF, 2017b), while mobility structures the humanitarian space and the deeper politics go unaddressed. Yet these themes of im/mobility and their relation to specific times, spaces and types of activities are not unique to the humanitarian borderscape. The specificities of im/mobility, as well the times, spaces and types of care engendered, produce a particular type of borderscape, as I have shown. However, scholars may wish to focus on the specific role of im/mobility and its inter-relation to particular times, spaces and practices in other border settings, or use the approach of Tallis (2017) more generally to uncover their own related features and activities.
Footnotes
Acknowledgements
This article has been presented at a range of conferences and workshops over the previous two years including at ISA, Atlanta and AAG, San Francisco in 2016; the Re-Mapping Europe workshop held at the University of Amsterdam in 2016 and at the European Workshops in International Studies, Cardiff 2017. The article is stronger as a result of the comments and suggestions of colleagues at these events as well as the insightful suggestions of the three peer reviewers. Thanks must also go to those who participated in the Humanitarian Mobilities: a conversation between researchers and practitioners workshop that I organised in Amsterdam on 4 May 2017 with the support of ACCESS EUROPE. I wish to thank the hospitality of the Transcapes research team in Athens, Ilias Papagiannopoulos-Miaoulis in Athens and Thessaloniki, and Philippa and Eric Kempson in Lesvos. Finally, I am indebted to the numerous members of MSF who have repeatedly indulged me, been candid with their thoughts and experiences and abundantly generous with their time.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.