
Abstract
We examine how first-person plural and second-person singular pronouns used in coronavirus disease 2019 (COVID-19) communications impact people's likelihood to follow stay-at-home recommendations. A 2 (first-person plural [“we”] vs. second-person singular [“you”]) by continuous trait self-control between-subjects experiment (N = 223) was used to examine individuals’ adherence to stay-at-home recommendations. Results suggest that “you”-based appeals may be more broadly effective in garnering stay-at-home adherence, whereas low self-control individuals are less responsive to “we” appeals. Implications for research and practice are discussed.
During the coronavirus disease 2019 (COVID-19) pandemic, the welfare of society relies on each individual's voluntary engagement in non-pharmaceutical interventions (NPIs), including mask-wearing, physical distancing, and self-quarantining. Carrying out these behaviors can be strenuous because individuals need to overcome the temptation of immediate comfort (e.g., not wearing a mask on a hot summer's day) and must change habitual behaviors (De Ridder et al., 2012; Ramkissoon, 2020); these are particularly difficult when persistence is also required (Harvey et al., 2021). Communications from health authorities are important determinants of people's likelihood to engage in effortful health-related behaviors—from getting a vaccination (e.g., Gilkey et al., 2016) to quitting smoking (Grandpre et al., 2003). During the COVID-19 pandemic, governments and health organizations have worked particularly hard to encourage individuals to engage in NPI behaviors in an effort to curb the spread of the virus.
Prior research suggests that pronoun usage, particularly that of the first-person plural “we” and the second-person singular “you,” plays a critical role in promoting perceived group cohesiveness and interdependence (e.g., Chen & Loftus, 2019; Sendén et al., 2014). According to Scheibman’s (2004) theories on “clusivity” (i.e., inclusivity and exclusivity), the pronoun “we” can be strategically used to suggest the inclusion of the speaker and all other people involved in the event, thus evoking a sense of commonality and involvement. This suggests that in the context of the COVID-19 pandemic, the use of the plural first-person pronoun “we” should be more effective in eliciting behaviors that benefit the group. Governments and health authorities often communicate the importance of collective action by using phrases in public health messages such as “we’re all in this together,” perhaps due to beliefs that individuals are more likely to carry out these actions when they experience a strong sense of responsibility for collective welfare (De Cremer & Van Lange, 2001).
However, whether individuals partake in a particular action largely depends on the resources, such as self-control, which are available to them (Muraven & Slessareva, 2003; also refer Tu et al., 2021). Therefore, in the current research, we explore the effect of identity framing (as communicated by using different pronouns in health appeals), further exploring individual differences in self-control as a boundary condition on people's willingness to engage in NPIs (e.g., staying-at-home). We first review relevant literature on personal pronouns and self-control and then outline our hypotheses.
“We” Versus “You” Pronouns
Pronouns are frequently used to communicate or construct identities and relationships (e.g., Cruz et al., 2017; Galdiolo et al., 2016). As Cramer (2010) explains, “through the differential use of pronouns, speakers create, recreate, and make visible specific identities in real time” (p. 620). In particular, we tend to use the first-person plural “we” (vs. the second-person singular “you”) to communicate or build relationships, and it has consequential effects on relationship quality and cooperative behavior (e.g., Cruz et al., 2017; Sela et al., 2012).
In general, the use of “we” suggests close relationships or a collective identity, while the use of “you” reflects separateness or an individual identity. In communications where the relationship between the speaker and the audience has been established, prior research suggests a beneficial effect of using “we” as opposed to “you.” For example, in romantic relationships, the use of “we” (vs. “you”) in daily conversations is positively associated with relationship quality (e.g., Galdiolo et al., 2016; Rohrbaugh et al., 2012). Additionally, greater use of “we” in couple communication is associated with more positive treatment outcomes (Hallgren & McCrady, 2016; Rohrbaugh et al., 2012). Beyond romantic relationships, the instrumental role of “we” in promoting greater psychological closeness has also been found in relationships that involve asymmetric power or status (e.g., Gordon & Luke, 2016; Planken, 2005). For example, professional negotiators seemed to use “we” strategically to promote a sense of solidarity (Planken, 2005).
Although existing evidence convergently suggests a superior role of the single-person plural “we” over the second-person singular “you” in promoting perceived interdependence and group cohesion, a few different streams of research suggest that the use of “you” could be beneficial in other situations. First, the effectiveness of pronoun usage seems to depend on relationship distance. For example, in marketing communications, psychological relationship distance between the source of information and the message recipient is a critical moderator for the “we”/“you” effect (Cruz et al., 2017; Sela et al., 2012). Sela et al. (2012) found that using the pronoun “we” led to more positive attitudes toward the brand than using “you and the brand” among existing customers (close relationships). The reversed effect was true among prospective customers (distant relationships).
Contrarily, messages that speak directly to consumers by including a second-person singular “you” can prompt self-referencing (Martin et al., 2004), eliciting deeper information processing and consumer involvement. By analyzing brand posts on Facebook, Cruz et al. (2017) found that the use of “you” in brand messaging resulted in more consumer “likes,” “shares,” and “comments.” Meanwhile, in studies of political discourse, researchers found that “we” was frequently employed by politicians to deflect individual responsibility (e.g., Kranert, 2017). As such, the use of the first-person plural “we” might imply or activate diffusion of responsibility.
From the health authorities’ perspective, it is sensible to use “we” in health communications to promote NPI adherence because collective actions are required to slow the spread of COVID-19. However, prior research suggests that the use of “we” may counterintuitively discourage cooperation in certain situations. We propose that given the large scale of individuals involved in the context of COVID-19, this circumstance reflects the latter line of research in which people involved in the communications are more likely to perceive a distant relationship between themselves and the health organization. To rearticulate, an average citizen is likely to perceive the World Health Organization (WHO) or the Centre for Disease Control and Prevention (CDC) as far away from them, and hence, the use of “we” is likely to result in diminished persuasion. Further, we theorize that using “we” in health communications could lead people to construe the goal of flattening the curve as a collective matter and responsibility, thus diluting the role of the individual. This is important because grasping the full scope of the cooperative effort required to limit the spread of COVID-19 could lead individuals to feel that they possess a limited ability to make a difference (i.e., diminished self-efficacy; Bandura & Cervone, 1983), or lead them to perceive a diminished sense of responsibility for contributing (Messick & McClelland, 1983). Thus, in this context, the “we” pronoun may discourage NPI adherence.
Additionally, research in cognitive psychology has consistently demonstrated a link between the use of “you” and self-referencing. Compared to other personal pronouns (e.g., “I” and “he”), “you” is more likely to mentally simulate or embody described actions in narratives (for a review, refer to Glenberg, 2007), resulting in stronger information retention over time (Ditman et al., 2010). As such, using the pronoun “you” is likely to promote a sense that the message speaks directly to the recipient. This, in turn, could motivate self-referencing (Martin et al., 2004) and enhance individual involvement. Furthermore, when “you” is used (e.g., “you can get through this”), this enhanced self-referencing is likely to promote a mental simulation of the action, encoding it from the actor's perspective. Taking these reasons together, we expect individual-focused appeals (i.e., the use of “you”) will be more effective than collective-focused appeals (i.e., the use of “we”) in promoting NPI adherence.
Trait Self-Control as a Boundary Condition
Although we propose that the use of “we” in health messages may counterintuitively discourage NPI adherence, we do not expect this to occur among all individuals. Rather, we suggest that some people are better at overcoming this “free-riding” temptation and will exhibit high NPI adherence regardless of which pronouns are used in health messages. Specifically, engaging in NPIs represents a self-control dilemma in the sense that individuals need to exert effort to resist the temptations of carrying out habitual behaviors (De Ridder et al., 2012), and instead adapt to the pandemic by developing new habits and routines. As such, we focus on the role of trait self-control, which reflects an individual's predisposition to resist temptation (Tangney et al., 2004), as a boundary condition to our proposition.
Prior research in self-control suggests that some people naturally have more self-control resources than others. Those with higher (vs. lower) self-control are better at managing and monitoring their emotions and behaviors and hence are more likely to achieve success in various domains (e.g., Redden & Haws, 2013; Tangney et al., 2004). Recent research found that the trait self-control positively predicted whether individuals developed new, adaptive habits during self-quarantine (Kokkoris & Stavrova, 2021). Thus, people with high dispositional self-control, in general, should show a higher level of NPI adherence than those with low dispositional self-control.
Additionally, prior research shows that people with high dispositional self-control are less influenced by their environment than those with low dispositional self-control, as they might have already adopted various strategies that support goal achievement (De Ridder et al., 2012; Redden & Haws, 2013). For example, Redden and Haws (2013) found that participants with higher trait self-control paid more attention and were satiated faster when eating unhealthy (vs. healthy) food, whereas participants with lower trait self-control did not show such detection of a “self-control trap” and consumed more unhealthy food. Taken together, we expect that low self-control individuals will show lower NPI adherence when presented with a health appeal using “we” compared to a health appeal using “you,” whereas high self-control individuals will demonstrate higher levels of NPI adherence regardless of the pronoun usage in health messages. This means that low self-control will serve as a boundary condition and dampen the efficacy of “we” pronoun usage. In the next section, we present a study designed to test our hypotheses and show the results from this study.
Method
Participants
Two hundred and twenty-three American participants (Mage = 40.37, SDage = 13.04, range = 18–78; 50% female) completed the study through an online panel (Amazon's MTturk) in exchange for pay ($0.50USD) between May 5, 2020, and May 8, 2020. At this time, more than 1.2 million COVID-19 cases were reported in the USA. While recruiting, we excluded participants from states where strict curfews had been imposed at that time; these included New York State, California, Oregon, Illinois, Wisconsin, and Washington State. A post hoc power analysis based on the observed outcomes of this study shows that a sample size of 223 participants has a power of .95 to detect a two-tailed small-to-medium effect size (r = .20).
Design
Participants were randomly distributed across a 2 (pronoun type: “we” vs. “you”) by continuous (trait self-control) between-subjects design. Our focal-dependent variable was participants’ likelihood to stay-at-home (vs. go out) in two different scenarios.
Materials and Procedure
Participants first read a description about COVID-19 (see Appendix A for details). They were then randomly assigned into one of the two pronoun conditions. In the “we” (vs. “you”) condition, participants viewed a message ostensibly from the WHO saying, “stay home, we can get through this together (you can get through this).” We chose the WHO as the source of information because it is a world-level organization with high levels of credibility (Bell et al., 2020). As the WHO is a world-level organization, it is also more likely that an average person will perceive a distant relationship with it. Participants were then presented with two scenarios (see Appendix A for details) in which they were asked to make a trade-off between “go to a friend's party” versus “stay-at-home” on a 9-point Likert scale (1 = stay at home, 9 = go to the party); and “stick to my normal routine” versus “stay-at-home” on a 9-point Likert scale (1 = stay at home, 9 = stick to my routine). Next, participants completed the 13-item general trait self-control scale (Tangney et al., 2004; α = .88) on a 7-point scale (1 = strongly disagree, 7 = strongly agree) after several unrelated filler tasks. Sample items of this self-control scale include “I am good at resisting temptation” and “I do certain things that are bad for me, if they are fun” (reverse coded). Then, participants reported their level of trust in the WHO (“How much do you trust the World Health Organization (WHO)?”) on a 7-point Likert scale (1 = distrust a great deal; 7 = trust a great deal). Prior research found that trust toward the message source had a significant impact on people's intention to follow the recommended health behavior (e.g., Almutairi et al., 2020; Oksanen et al., 2020). Hence, participants’ trust toward the WHO was measured and included in our analysis as a covariate. Finally, participants answered demographic questions that measured their gender, age, and ethnicity and were debriefed.
Results
Descriptive statistics can be found in Table 1. The dataset including the variables reported here is available in the OSF repository; retrieved from https:/osf.io/d5qxf/. We first assessed the validity of combining our two stay-at-home adherence measures using a Pearson correlation (2-tailed), which yielded a substantial and positive correlation (r = .65, p < .01) indicating 42% overlapping variance. We next conducted a 2 (condition: “we” vs. “you”; between subjects; coded as “−1” vs. “1”) by continuous (self-control) by 2 (scenarios: skip party vs. change routine; within-subjects) analysis of covariance to evaluate whether an interaction effect—which would provide evidence of a differential effect of the dependent variable by the condition—was present. As we intended to use existing attitudes toward the message source, the WHO, we included this measure as a covariate in our theory testing; our manipulation had no significant impact on the trust in WHO (p = .48). Importantly, neither pronoun usage (F[1, 218] = 0.07, p = .79) nor self-control (F[1, 218] = 0.01, p = .91) interacted with the scenario condition, and the three-way interaction (F[1, 218] = 0.32, p = .57) was not significant either. Thus, we aggregated these two scenarios into an index of stay-at-home adherence (α = .79), where a higher value indicates a greater stay-at-home likelihood.
Means, Standard Deviations, and Intercorrelations of Dependent Variables Across Experimental Conditions.
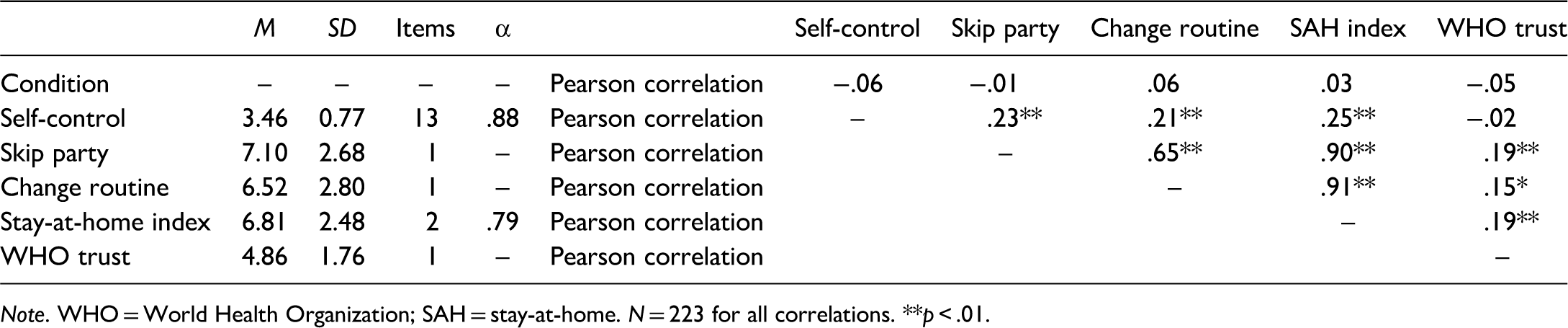
Note. WHO = World Health Organization; SAH = stay-at-home. N = 223 for all correlations. **p < .01.
We next turned our attention to theory testing (see Table 2). In particular, we used Hayes’ (2017) PROCESS macro model 1 version 3.5 (bootstrap replications: 5,000) to assess the moderating effect of self-control (W) on the relationship between pronoun type (X; “we” vs. “you; coded as “−1” vs. “1”) and stay-at-home likelihood (Y). Trust toward the WHO was entered into the model as a covariate. The overall model was significant (R2 = .12, F[4, 218] = 7.52, p < .001). As predicted, the results specifically revealed a significant main effect of pronoun type, where the “you” pronoun performed better (M = 6.88; SD = 2.33) than the “we” pronoun (M = 6.74; SD = 2.64; t[218] = 2.47, p = .01; CI: 0.3796 to 3.2740), and revealed a significant main effect of self-control (t[218] = .78, p < .01; CI: 0.3673 to 1.1828), where higher self-control was associated with greater stay-at-home likelihood. Importantly, this effect was qualified by a significant interaction (R2change = .02; F[1, 218] = 5.55, p = .02).
Regression Coefficients for Aggregate Stay-at-Home Likelihood.
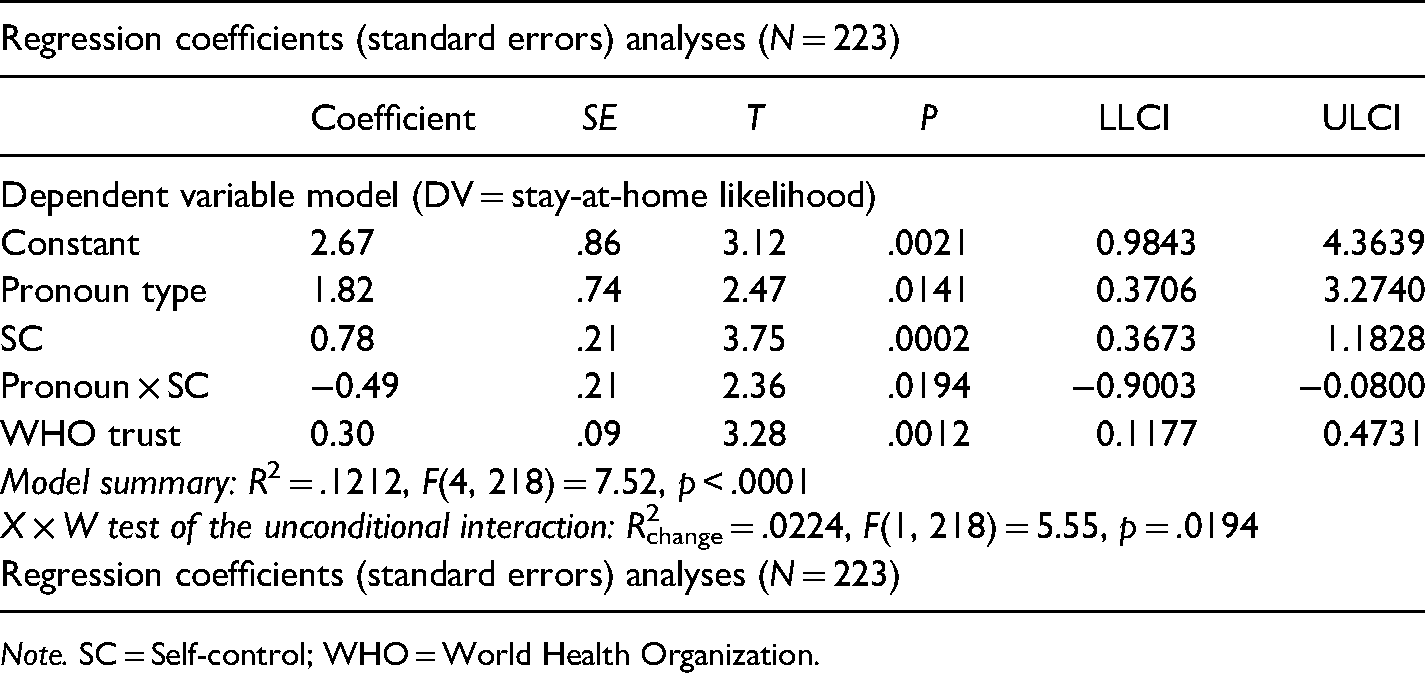
Note. SC = Self-control; WHO = World Health Organization.
We next interpreted the conditional effects of pronoun type on stay-at-home-likelihood at the 16th, 50th, and 86th percentiles in accordance with the recommendations of Hayes (2017). As predicted, when self-control was low (16th percentile), the effect of pronoun type on stay-at-home was significant (effect = .50, SE = .22, t = 2.24, p = .03; CI: 0.0609–0.9444). However, this effect did not emerge when self-control was moderate (50th percentile; effect = 0.16, SE = .16, t = 1.03, p = .30; CI: −0.1491 to 0.4756) or high (86th percentile; effect = −.29, SE = .24, t = −1.22, p = .22; CI: −0.7564 to 0.1779), in accordance with our predictions. Interpreting the Johnson–Neyman region of significance, values of self-control below 2.96 yielded a significant effect of pronoun type on stay-at-home, with 31.84% of the sample falling within that region (see Figure 1).
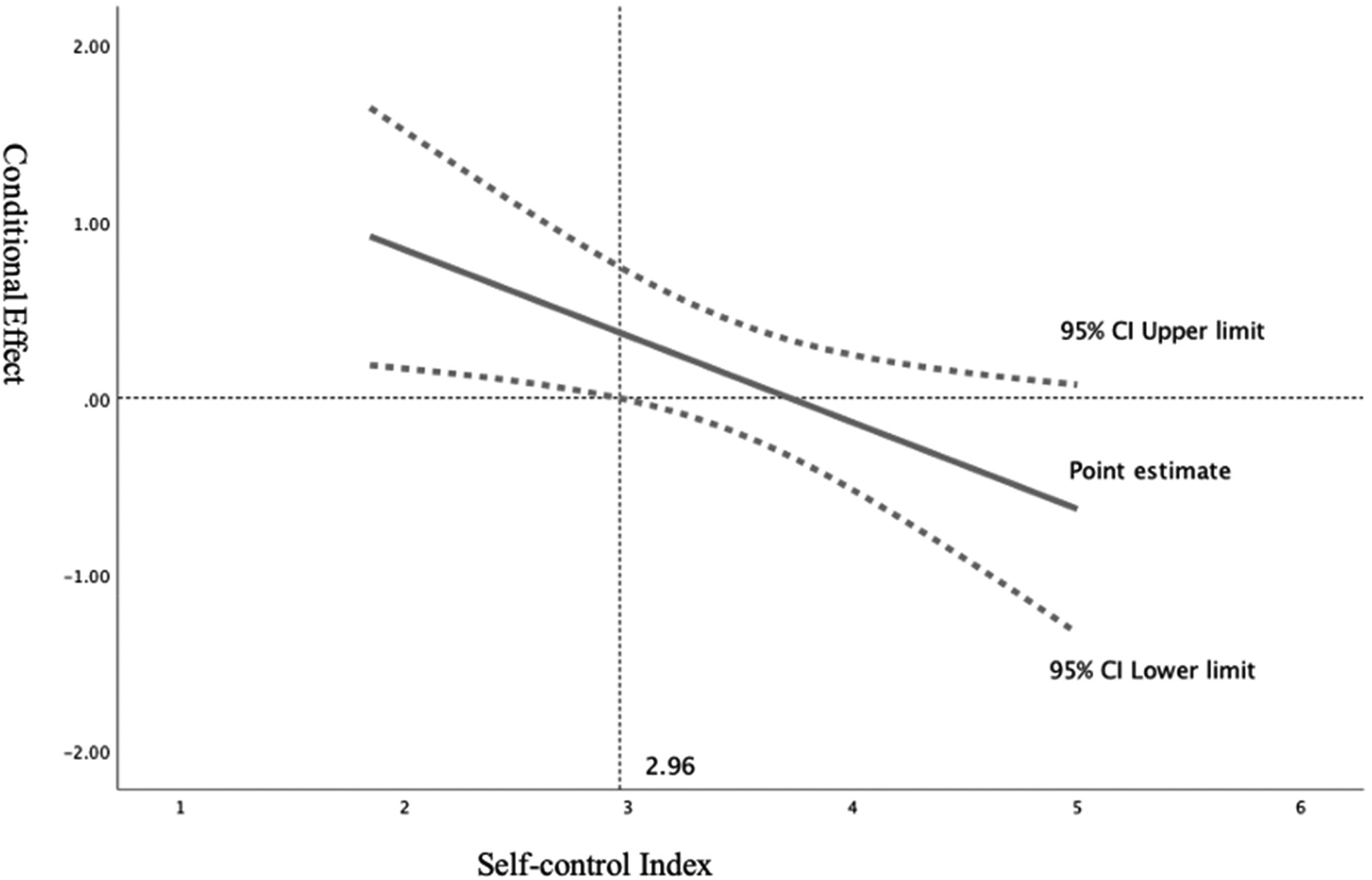
Johnson–Neyman plot of the conditional effect of pronoun type as a function of self-control.
Discussion
Taken together, we find that pronoun type significantly influences NPI adherence intentions and that this effect is moderated by an individual's trait self-control. In particular, those high on self-control intended to adhere more to stay-at-home guidance regardless of pronoun usage, whereas low self-control individuals were less (vs. more) inclined to adhere to the NPI when a “we” (vs. “you”) pronoun was applied. These findings have important implications for governments, health organizations, and NGOs communicating to the public during the ongoing pandemic situation, as well as in other public health communication situations. In particular, “you” messages may be preferable overall for garnering NPI adherence.
Moreover, certain groups are more likely to face self-control dilemmas than others in daily life (De Ridder et al., 2012) and hence are more likely to experience self-control resource depletion (Muraven & Baumeister, 2000) and less likely to adhere to health communications. For example, compared to the elderly, younger people are more likely to experience impulses (e.g., De Ridder et al., 2012) and temptations (Andrews et al., 2020) and hence are more likely to experience self-control resource shortages (i.e., low self-control) in daily life. As such, health messages using “you,” rather than “we,” might be particularly useful in promoting young people's NPI adherence.
Our research is limited in several ways. In particular, our sampling procedure holds limitations in terms of generalizability and data quality. Specifically, while Amazon's MTurk provides access to a large and diverse participant pool, these respondents can have limited attention and are, in some cases, non-naïve (Aguinis et al., 2021; Smith et al., 2016). We suggest that such a sample was appropriate given the speed with which we sought to collect data in an ever-changing pandemic situation, and we implemented attention checks into our data cleaning to mitigate some concerns. Nonetheless, convergent evidence should be sought in future research.
Additionally, our theory provides several opportunities for future research to investigate the mechanism and other boundary conditions of these pronoun effects. For example, we propose that a distant relationship is a necessary precondition for the heightened performance of the “you” (vs. “we”) pronoun among low self-control individuals (e.g., because “we” used by an organization with whom one does not have a relationship could generate resentment), which future research should directly assess. Second, prior research suggests several possible mechanisms for this effect. For example, the use of “we” may shift one's focus from the self to the large scale of people involved (Pennebaker et al., 2003; Simmons et al., 2005). As a result, this might decrease perceived self-efficacy—the subjective feelings of one's actions are effective in achieving the desired goal (Bandura & Cervone, 1983)—and diminish personal responsibility (Messick & McClelland, 1983). Future research should directly assess these propositions.
Conclusions
Our study provides preliminary, but promising, evidence to suggest that self-control moderates the effect of pronoun type in health communications on individuals’ NPI adherence. Specifically, high self-control consumers were generally responsive to all message conditions, whereas low self-control individuals demonstrated heightened (vs. diminished) willingness to adhere to stay-at-home when “you” (vs. “we”) pronouns were used. We hope this research will seed future studies to validate and extend our findings and prove fruitful to health communicators in the COVID-19 pandemic and beyond.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the University of Lethbridge.