
Abstract
The acquisition of surgical skills is an essential component of veterinary training. The use of live animals or cadavers for early surgical skills development is limited by ethical, logistical and financial constraints, highlighting the need for accessible and animal welfare-oriented training alternatives. The objective of this study was to evaluate the effectiveness of a low-cost, balloon-based simulator for teaching basic surgical knot techniques to undergraduate veterinary students with no prior surgical experience. A cohort of 20 students practised slip knots, Miller’s knots and transfixation knots, using a low-fidelity balloon simulator under a structured training protocol. Performance was assessed by using standardised rubrics, i.e. execution time and a binary success/failure classification based on air leakage. From the 13th repetition onward, all students successfully executed slip knots and Miller’s knots, while competency in the transfixation knot was achieved by the 14th repetition. Execution time decreased significantly from the 11th repetition for all three techniques, indicating progressive improvement in technical efficiency. It was evident that the balloon-based simulator facilitated the acquisition of basic surgical knot-tying skills, and represents an accessible, ethical and effective tool for early-stage surgical training in veterinary education.
Introduction
The development of clinical competencies is essential in the training of veterinary students. Among clinical competencies, practical skills play a central role because they integrate technical execution with professional attitudes, such as responsibility, clinical decision-making, situational awareness and patient safety within real or simulated clinical contexts. 1 In clinical practice, surgery is one of the most critical areas, as it requires the mastery of basic principles such as instrument handling, delicate tissue manipulation, time and motion control, and specific skills including cutting, haemostasis and suturing. Surgical performance does not depend solely on technical proficiency. Non-technical skills — including situational awareness, decision-making, communication, teamwork and leadership — are also key determinants for ensuring safe and effective clinical practice.1,2 This complexity highlights the need for comprehensive preclinical training that integrates knowledge, technical ability and transversal competency, right from the very early stages of the taught course.
In response to the ethical, logistical and economic constraints associated with the use of live animals or cadavers, and to increase student enrolment, many veterinary teaching institutions have incorporated simulation laboratories. These environments provide a safe, controlled setting that is centred on students and supported by immediate feedback, thereby enhancing both technical and non-technical skills. 1 Globally, veterinary accreditation bodies require graduates to be competent in basic surgical procedures, although they do not specify the teaching methodologies. Traditionally, cadavers have been used for practicing various skills; however, this approach has several limitations, including tissue rigidity, autolysis and the absence of blood flow. In this study, the term “preclinical” refers to the training phase prior to the independent performance of procedures. This phase is conducted in a simulated or supervised setting and does not involve live animals. In surgical training, students must first acquire fundamental psychomotor skills before progressing to procedures involving live animals. 3
International Three Rs education initiatives, such as those promoted by the Norwegian Consensus Platform for the Replacement, Reduction and Refinement of Animal Experiments (Norecopa), strongly advocate early surgical skills training using low-fidelity, homemade and synthetic simulators. These initiatives emphasise structured training protocols and competency-based progression, supporting ethical, accessible and pedagogically sound alternatives to animal use in preclinical education. 4 Vascular ligatures are essential for achieving haemostasis, and their performance depends on secure, efficient surgical knots. Although multiple knot types exist, only a few are routinely used in clinical practice. Early mastery of surgical ligature techniques, under supervision and through deliberate practice, is crucial for ensuring safe and effective performance in subsequent clinical training. 5 A practical and low-cost educational simulator represents an alternative to the use of animal cadavers or live animals during the early stages of surgical skills training. 3 In this scenario, near-peer teaching (NPT) has also gained importance. In this approach, advanced students instruct less-experienced peers, thereby promoting empathy, collaborative learning and a supportive environment. Recent studies have demonstrated its effectiveness through objective evaluation methods. 6 From an educational perspective, this training strategy is consistent with established surgical education models, including mastery learning, competency-based medical education (CBME) and objective structured assessment of technical skills (OSATS). These frameworks emphasise repeated practice, predefined performance benchmarks and objective assessment, to ensure that learners achieve competence before progressing to more complex or higher-risk training environments.7–10
This study evaluated the effectiveness of a low-cost balloon-based simulator for teaching three vascular ligature techniques — the transfixation knot, the Miller’s knot and the slip knot — to undergraduate veterinary students with no prior surgical experience. In addition to undergraduate veterinary education, the psychomotor skills addressed in this study are directly transferable to laboratory animal science training. Secure vascular ligatures, knot integrity and controlled tissue handling are core competencies for laboratory animal professionals involved in experimental surgery, necropsy procedures and the refinement of invasive techniques. Consequently, the proposed simulator may also contribute to early-stage skill acquisition in laboratory animal training programmes, aligning with international Three Rs education strategies aimed at reducing animal use during initial competency development.
Materials and methods
Simulator
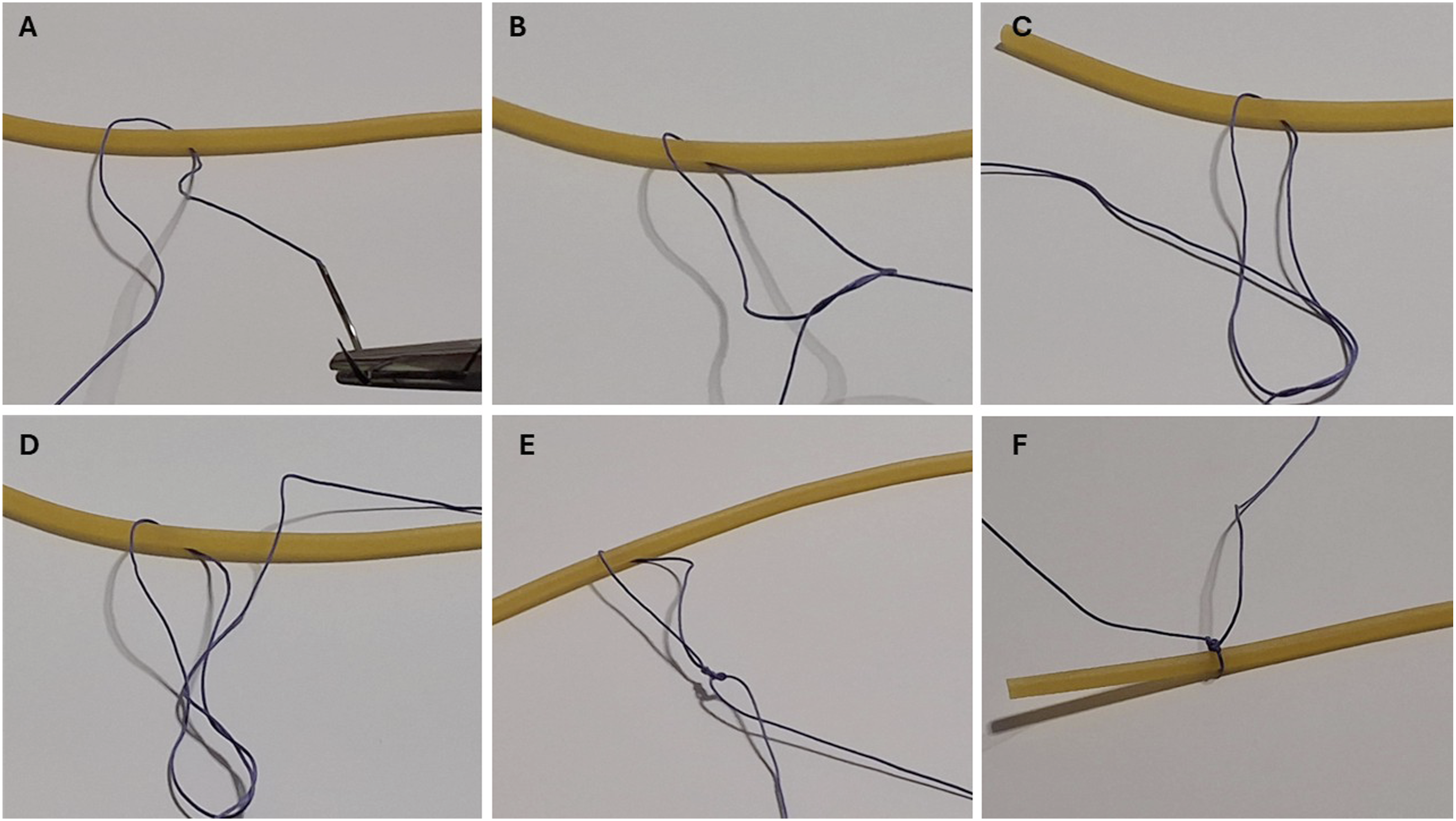
Latex modelling balloons, commonly used for balloon twisting activities, were inflated to approximately 75% of their capacity (approximately 4 cm in diameter). These models were used to practise three vascular ligature techniques: the transfixation knot, the Miller’s knot and the slip knot (Figures 1–3, respectively). Each student performed 15 repetitions of each technique. Stepwise execution of the Miller’s knot, using the low-fidelity balloon-based simulator. A hollow, latex tube was used as a tubular structure to simulate a vascular pedicle and to demonstrate the steps of the knot. (a) The ligature is passed beneath the balloon, leaving both suture ends accessible. (b) The first loop is created around the structure. (c) The loop is gently tightened to maintain positioning. (d) A second circumferential loop is formed, characteristic of the Miller’s knot, increasing friction and resistance to slippage. (e) Controlled counter-traction is applied to secure the knot. (f) Final configuration of a compact and stable Miller’s ligature. This sequence illustrates the standardised technique practised and evaluated during the training sessions. Stepwise execution of the transfixation knot, using the balloon-based simulator. A hollow, latex tube was used as a tubular structure to simulate a vascular pedicle and to demonstrate the steps of the knot. (a) The needle and suture are passed transversely through the tubular structure to establish the transfixing point. (b) The suture is pulled to initiate circumferential encirclement. (c) The first loop remains stabilised by the transfixing bite. (d) The suture ends are crossed to begin knot formation. (e) Controlled tightening is performed with surgical instruments. (f) Final secured ligature. This technique was evaluated for knot integrity, air leakage and execution time as part of the structured repetition protocol. Stepwise execution of the slip knot, using the balloon-based simulator. A hollow, latex tube was used as a tubular structure to simulate a vascular pedicle and to demonstrate the steps of the knot. (a) The suture is placed around the tubular structure. (b) Initial formation of the sliding loop configuration. (c) Creation of the main loop enabling knot mobility. (d) Completion of the sliding loop by passing the free end through the turn. (e) Progressive sliding of the knot toward the tubular structure under controlled tension. (f) Final tightening of the slip knot, compressing the balloon surface. This technique was assessed for mechanical integrity and leakage by using the standardised criteria.

Participants
Twenty undergraduate veterinary students from the Universidad Autónoma Metropolitana, Unidad Xochimilco (Mexico City), who were enrolled in the Surgical Techniques and Therapeutics module, participated in the study. All participants had no prior surgical experience. As part of their regular academic activities, all students received standardised theoretical and practical instruction in surgical knot-tying techniques, prior to the training sessions.
Procedure
Each student performed 15 repetitions of each ligature technique per session, resulting in 300 observations per technique per session, and a total of 600 observations per technique across both sessions. For the leakage test, multiple consecutive ligatures were applied along an air-inflated balloon, forming a series of segmented sections resembling a ‘sausage’ configuration (Figure 4). Once completed, each ligature was sectioned between knots to assess air leakage. If the balloon lost air, then the ligature was classified as ‘incorrect’; if no leakage occurred, it was classified as ‘correct’. For each repetition, three parameters were evaluated: knot integrity, the presence or absence of air leakage, and the execution time (in seconds). The execution time was recorded manually with a digital stopwatch from the initiation of the first movement to the final cut of the suture material. The balloon-based simulator and the leakage test procedure for the objective assessment of knot security. (a) Air-filled latex balloons, inflated to approximately 75% capacity. (b) Ligature application in progress. (c) Completed ligature applied circumferentially. (d) Ligatures are placed sequentially along the balloon to create segmented sections for leakage testing. After sectioning between knots, air leakage was evaluated. Loss of air indicated knot failure (classified as ‘incorrect’), whereas absence of leakage indicated adequate mechanical security (classified as ‘correct’). This binary outcome measure constituted the primary objective assessment of ligature effectiveness.
Participants were undergraduate veterinary students enrolled in the Surgical Techniques and Therapeutics module within the same academic year. The training sessions were conducted in small groups and facilitated by faculty members and graduate students. Each session lasted approximately 60 minutes. Independent practice between sessions was neither restricted nor monitored, and students were not surveyed about additional practice undertaken outside the scheduled sessions.
Data analysis
Faculty members, assisted by graduate students, classified each ligature as ‘correct’ or ‘incorrect’. Data were organised in Excel™ and analysed with descriptive statistics. To compare the two sessions, a paired Wilcoxon test was performed at the p < 0.05 significance level by using the PAST software (v4.09). 11 Participants were considered to have reached the learning curve plateau when no significant differences (p > 0.05), in terms of the correct/incorrect classification or the execution time, were observed between consecutive attempts. Although the simulator does not accurately replicate the anatomy or consistency of a blood vessel (low fidelity), it proved helpful for evaluating the mechanical effectiveness of the ligatures, as air rapidly escapes when a knot is not adequately secured. This characteristic allows for high-sensitivity error detection, promoting the development of technical precision and manual control during training.
Results
Performance in the execution of the three surgical knots by the veterinary students, according to a correct/incorrect binary classification.

The 20 participants repeated each attempt 15 times, resulting in 300 repetitions per attempt, per knot. The performance is expressed as the number and proportion of correct executions per attempt, with the 95% confidence intervals (95% CI) indicated. The standard error (SE) and 95% confidence intervals were calculated using binomial distribution.
Comparison of the execution times of the three surgical knots among the veterinary students.

The 20 participants repeated each attempt 15 times. Thus, in total, there were 300 repetitions per attempt, per knot. The mean was calculated by summing the 300 time measurements per attempt and dividing by the total number of observations. The standard deviation was calculated to show how spread out the individual time measurements were around the mean value. Participants were considered to have reached the learning curve plateau when no significant differences (p > 0.05) in the time taken were observed between consecutive attempts (see also Figure 5).

Example learning curves based on the execution time over 15 consecutive repetitions for the three knots. The bars represent the mean execution time (seconds) ± standard deviation for each repetition (n = 20 students per session). Linear trend lines and corresponding coefficients of determination (R2) illustrate the progressive reduction in execution time, reflecting improvements in technical proficiency during structured, deliberate practice with the low-fidelity simulator.
Discussion
The traditional ‘mentor–apprentice’ model of surgical training has been a cornerstone of veterinary surgical education for decades. However, its effectiveness depends on the instructor’s pedagogical skills and the student’s individual learning pace — factors that may introduce variability in outcomes. 12 In contrast, surgical simulators help shorten the time taken to reach the learning curve plateau, provide a safe environment for practising and enhance the retention of technical skills.1,3 Within the spectrum of simulation-based education, the balloon-based model evaluated in this study represents a very low-fidelity bench simulator, primarily intended for early-stage psychomotor skill acquisition. Low-fidelity models are particularly effective during initial training phases, where the educational focus is on fundamental knot mechanics, hand–eye coordination and error recognition, rather than anatomical realism. 13
In this study, structured exercise repetition using a balloon-based model led to progressive improvement in performance across three surgical knot types. Students reached technical competency by attempts 13 and 14, with no significant differences in subsequent repetitions (p < 0.001). This pattern aligns with the principles of deliberate practice, which combine intentional repetition, immediate feedback and objective evaluation, and has been shown to be effective in developing surgical skills.3,14 Although the simulator is low-fidelity and does not accurately reproduce the texture or mechanical properties of biological tissues, its potential for detecting failures in knot security via air leakage makes it a functional, highly sensitive tool. This characteristic enables early and precise error detection, thereby promoting the development of manual control and technical accuracy in the early stages of surgical training. 9
Commercial surgical simulators, including silicone vessel models, synthetic tissue platforms and integrated surgical skills boards, offer greater tissue compliance, friction and anatomical context than do balloon-based models. Box trainers, box-contained training models, and laparoscopic simulators further support the development of bimanual dexterity, instrument ergonomics and spatial awareness, often incorporating validated assessment frameworks such as the objective structured assessment of technical skills (OSATS) or automated motion tracking.8,14,15 More recently, virtual reality and augmented reality simulators have demonstrated improved transfer of procedural skills to clinical performance, particularly when embedded within structured curricula and proficiency-based progression models. Meta-analyses in human surgical education have consistently shown that simulation-based training with deliberate practice leads to superior operative performance and lower error rates than do traditional apprenticeship-based approaches.8,15
Despite these advances, the balloon-based simulator offers several distinct advantages. Its ultra-low cost and ease of fabrication enable broad accessibility, particularly in low-resource educational settings. The model provides immediate binary feedback (i.e. success/failure) through air leakage, allowing high-sensitivity detection of knot failure without integrated sensors. Its scalability supports distributed and repeated practice, a cornerstone of mastery learning approaches. Importantly, the simulator represents a clear replacement strategy within the Three Rs framework, by eliminating the need for animal cadavers or live tissue during early skills training.8,9
Several limitations must be acknowledged. Balloons do not replicate the mechanical properties of biological tissues, such as elasticity, resistance and friction, which may limit skill transfer to real surgical environments, particularly for transfixation ligatures. The model lacks anatomical and procedural context, isolating knot mechanics from spatial constraints and instrument ergonomics encountered in clinical settings. Additionally, unlike higher-fidelity simulators, it does not incorporate automated objective metrics, and the present study did not assess transfer validity to biological tissues or clinical performance.13,16
More recently, virtual reality and augmented reality simulators have demonstrated improved transfer of procedural skills to clinical performance, particularly when embedded within structured curricula and proficiency-based progression models. Meta-analyses in human surgical education have consistently shown that simulation-based training with deliberate practice leads to superior operative performance and lower error rates than traditional apprenticeship-based approaches. The observation that slip knots and Miller’s knots were mastered earlier than the transfixation knot is consistent with previous studies attributing this difference to the greater technical complexity of the latter.10,12 Likewise, the progressive decrease in execution time supports the effectiveness of an approach based on deliberate practice and error management, which fosters deep, transferable and sustainable learning. 10
Several limitations of the study design must be acknowledged. Independent practice by students between training sessions was not controlled, and this may have influenced individual learning curve profiles. The study did not include a control group trained with alternative simulators or traditional methods, and it did not evaluate the long-term retention of skills. Furthermore, the transfer of skills acquired by using the balloon-based simulator to biological tissue or clinical performance was not assessed, and this should be addressed in future studies. 13 An additional relevant component was the incorporation of near-peer teaching (NPT), in which graduate students served as facilitators. This strategy has demonstrated benefits in the acquisition of surgical skills by promoting empathy, communication and collaboration among students with different levels of experience. 6
Conclusions
The literature indicates that, without continued practice, even basic surgical skills may deteriorate significantly after several months, regardless of initial competence. 14 Therefore, incorporating low-cost models, such as the one used in this study, into periodic reinforcement sessions may help maintain students’ psychomotor skills and confidence throughout their training.
For Three Rs-oriented educational programmes, the balloon-based simulator may be conceptualised as part of a tiered surgical training curriculum. In this framework, low-cost bench models serve as an entry point for psychomotor skill acquisition, followed by progression to synthetic tissue models, box-contained training models, or virtual reality simulators for procedural integration and, ultimately, to limited, ethically justified animal-based training when necessary. This staged progression supports both educational effectiveness and the systematic reduction and refinement of animal use.4,8,17
The balloon-based simulator offers a practical, accessible approach to early acquisition of surgical knot-tying skills in veterinary education. Its simplicity and low cost support its use as an introductory training tool before progressing to higher-fidelity simulators or supervised clinical practice.3,10,18 This simplicity and low cost, coupled with its ease of fabrication and broad applicability, make it a valuable tool for institutions with limited resources, without compromising the quality or depth of the educational process.
Footnotes
Acknowledgements
We extend our gratitude to the students enrolled in the Surgical Techniques and Therapeutics module, who voluntarily and enthusiastically participated in the training using this simple simulator.
ORCID iDs
Ethical considerations
This study did not involve procedures with live animals or the handling of biological samples. Student participation was voluntary and conducted as part of their regular academic activities.
Consent to participate
All participants were informed of the training objectives and agreed to participate without compromising their integrity. No identifiable personal data were collected; only the last four digits of each student’s university identification number were recorded for the purpose of pairing observations in the statistical analysis using the Wilcoxon test.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.