
Abstract
UK cannabis patients occupy a complex policy space in which prescribing has been lawful since 2018, but the drug remains otherwise illegal. This article draws on qualitative interviews from the first UK sociological study of cannabis patient experiences. The findings demonstrate that contradictory policies; a lack of training for professionals; and the legacy of prohibitionist constructions of cannabis result in a range of harms, including inequality and stigma. We employ the concepts of ‘stigma power’ and the ‘stigma machine’ to situate these experiences within the UK's contemporary neoliberal agendas and subsequent commitment to prohibition. Patients are not passive recipients of this stigma, employing what we term concealment, (re)construction and evangelism, to resist these processes. Like many of them, we call for comprehensive professional and public education about the legality of medical cannabis. We argue that to reduce stigma and inequality, this must be accompanied by critical reforms of drug policies.
Introduction
In 2018, the Misuse of Drugs (Amendments) Act legalised cannabis prescribing in the UK. This created a contradictory social and criminal justice policy environment, in which those who are prescribed cannabis occupy a liminal position - lawfully medicating in a context where it remains otherwise illegal. The law change has neither been widely publicised nor fully implemented in terms of making cannabis medicines available and affordable. These barriers mean that (legal) access to cannabis medicine is limited to those who can afford private healthcare, resulting in health inequalities. This article draws on data from the first UK sociological study of patients prescribed cannabis. The findings demonstrate that, despite their legal prescription, cannabis patients remain stigmatised, both directly and indirectly due to the ongoing criminalisation of the drug. This limits their freedom and their capacity to live independent, autonomous lives. We share the stories of patients feeling, experiencing and navigating this stigma in their everyday lives. Drawing on the concepts of ‘stigma power’ (Link and Phelan, 2014) and the ‘stigma machine’ (Tyler, 2020) we situate the stigmatisation of cannabis patients within a broader history and politics of cannabis use and control.
In countries where cannabis has been legalised, stigma is diminished (Baumbusch and Sloan Yip, 2022). Skliamis et al.'s (2022: 1483) pan-European study concluded that ‘punitive cannabis policy is associated with stigma, and liberal cannabis policy is associated with de-stigmatisation’. A Canadian study found the legacy of prohibition meant even when the drug is legalised, patients still must ‘navigate the uncertainties in attitudes and laws, flip the script on stigma, and create legitimacy for the therapeutic use of medical cannabis’ (Newhart and Dolphin, 2021: 295). UK research has demonstrated the stigma experienced by self-medicating cannabis users prior to legalised prescribing (Morris, 2018). Since the law change, only one study has surveyed cannabis patients (Troup et al., 2022). It found that the prohibitionist context perpetuated stigma for legally prescribed cannabis patients and identified the need for qualitative research to further explore this. Our research meets this need, by employing in-depth interviews to elicit patient experiences.
Law change: The legalisation of cannabis prescribing
Cannabis is criminalised in the UK as a class B controlled substance under the Misuse of Drugs Act 1971. In 2018, the Misuse of Drugs (Amendments) Act revised the Misuse of Drugs Regulations (2001), permitting medical cannabis (MHRA, 2020). Doctors on the General Medical Council's Specialist Register can prescribe unlicensed cannabis under the provision for ‘Specials’ under the Human Medicines Regulations 2012 (MHRA, 2020). Globally, cannabis is used to treat a wide range of conditions, including mental health (e.g., Post Traumatic Stress Disorder), pain (e.g., fibromyalgia), gastroenterological (e.g., Crohn's Disease), brain (e.g., epilepsy) and neurological/movement (e.g., Parkinson's Disease) disorders. However, UK NHS prescribing policy is restrictive, with NICE guidelines only allowing prescriptions for narrowly defined chemo-induced nausea and vomiting, spasticity, and severe treatment-resistant epilepsy (NICE, 2019). However, consultants can make a clinical decision to prescribe cannabis outside of these guidelines if they deem it suitable (NHS England, 2023), which was the case for many of the privately prescribed patients in our study. For more detail on the context of the UK law change, see Beckett Wilson and Metcalf McGrath (2023) and Bone and Potter (2021).
The 2018 legalisation of cannabis for medical purposes has gone largely under the radar and it sits uneasily alongside the UK's committed prohibitionist stance (see Hegemonic Prohibition section below). A freedom of information request in 2023 confirmed that less than five patients had obtained an NHS prescription for cannabis (Sinclair, 2023), leaving the majority reliant on private health care. Work by Beckett Wilson and Metcalf McGrath (2023) demonstrates that this creates a range of social harms and health inequalities. Some of the government's own membership have noted these harms and inequalities and are calling for change (see Julian Sturdy's request to the Secretary of State (Hansard, 2023), and note that Conservative MP Nickie Aiken is the Co-Chair of the All-Party Parliamentary Group for Medical Cannabis Under Prescription).
Stigma power
Link and Phelan's (2001) concept of ‘stigma power’ explains how the interests of stigmatisers are served through the exploitation, management, control, or exclusion of others (2014: 24). They suggest the powerful mobilise ‘stigma power’ to control by: ‘‘keeping people down’; ‘keeping people in’; and ‘keeping people away’’ (Link and Phelan, 2014: 25).
Tyler (2020) demonstrates that stigma power is ‘purposely crafted as a strategy of government’ (p.18) and that ‘state-led stigma campaigns and cultural stigma production cascade into our everyday interactions with each other’ (p.20). She calls on us to ‘ascertain where and by whom stigma is crafted’ (Tyler, 2020: 249) and to situate analyses of stigmatisation processes within their historical and political contexts. We draw on these theorisations of ‘stigma power’ to firstly show how cannabis patients experience stigma in different forms, and secondly to argue that, ultimately, stigma is a mechanism of power that is deliberately executed by the powerful in their own interests. The following section explores this exercise of state power in the history of UK cannabis control.
Cannabis constructions: Hegemonic prohibition and stigma
Understanding the historical social construction of cannabis helps to explain the context in which it is prescribed. Prohibition policy presents cannabis as a health hazard rather than a legitimate medicine, and stigmatises users of it as feckless yet risky populations: [C]urrent policies – of prohibition and criminalization of cannabis…contribute to sustaining the social classification of cannabis use as a deviant behavior [sic], as well as perceptions of cannabis users such as criminals, addicts and altogether ‘abusers’ (Ferraiolo, 2007, cited in Zolotov et al., 2018:5). Since the 1960's, the drug user has been recast as potentially posing a threat to the community – whether as a carrier of a metaphorical ‘socially infectious disease,’ as a carrier of a real contagious disease (HIV), or as a criminal predator’ (Seddon, 2009: 85). [Drug policy is based on] … fallacies [that] arbitrarily frame particular substances as ‘drugs’ and skew the risks of ‘drug use’ by focussing almost exclusively on specific types of use and users, and concentrating attention upon associated negative outcomes. This process allows certain substances to attain an unwarranted position of privilege whilst others are prohibited, creating a ‘drug apartheid’ – a deeply divisive system of segregation and punishment determined by the substance used (Taylor et al., 2016:2).
This policy and political environment contextualises the lack of NHS prescribing to date. The hegemony of the ‘drug apartheid’ inherent in the Misuse of Drugs Act 1971 prevents impartial consideration of scientific evidence on cannabis. Prohibition policy contradicts research evidence and the advice of the government's own Advisory Council on the Misuse of Drugs (Drake and Walters, 2015; Monaghan, 2014). Prohibition focuses on the potential harms of cannabis, whilst tight regulatory obstacles and lack of attention to the global evidence base, overlook the potential benefits of the drug. There is a contradiction here in that the law accepts it as safe for (private) medical prescribing but does not accept its safety in any other context. Even the law permitting prescribing is couched in terms of ‘misuse’: [F]orm and purpose limitations reflect the need to ensure that access is available to patients where medically appropriate, whilst minimising the risks of misuse, harm and diversion. This is in the context of the particular and unusual challenges arising from the very high levels of unlawful recreational use of cannabis (Misuse of Drugs Regulations 2018: 1, Section 3.2).
The harms of cannabis use are amplified by media and political narratives (Taylor, 2016), particularly when compared to the harms of alcohol, nicotine and some over the counter medications. Moreover, the cannabis harms are overshadowed by the harms of criminalising and policing it (Haden, 2006; Rolles et al., 2016), driving harmful methods of production (Beckett Wilson et al., 2017) and riskier strains (Nutt, 2019). Finally, the point that tight medical controls are needed due to ‘very high levels of unlawful recreational use of cannabis’ is undermined by the fact that cannabis use in the UK is still an activity of the small minority, with 7.4% of adults (16 to 59 years) and 16.2% of young people (16 to 24 years) reporting use (Office for National Statistics, 2022).
In summary, this critique demonstrates the government's commitment to prohibition and the ongoing construction of cannabis as a harmful drug. These discourses play an important role in controlling the populations who use cannabis and are fundamental to understanding the experiences of people prescribed it.
Methods
The study explored how people who are prescribed cannabis experience the intersections of social and criminal justice policy in their everyday lives. In other words, how people navigate the legal use of an otherwise criminalised drug. Semi-structured interviews were conducted with 24 prescribed patients, or their carers. People self-medicating without a prescription, or using cannabis for recreational reasons, were outside the scope of this study. Participants were recruited via a social media advert, which was posted and shared by several third-party medical cannabis organisations, including PLEA (patient-led advocates) and Project Twenty21 (research body). Some participants asked if they could refer other patients to the study, lending a ‘snowballing technique’ element to the recruitment process (Paton, 1990).
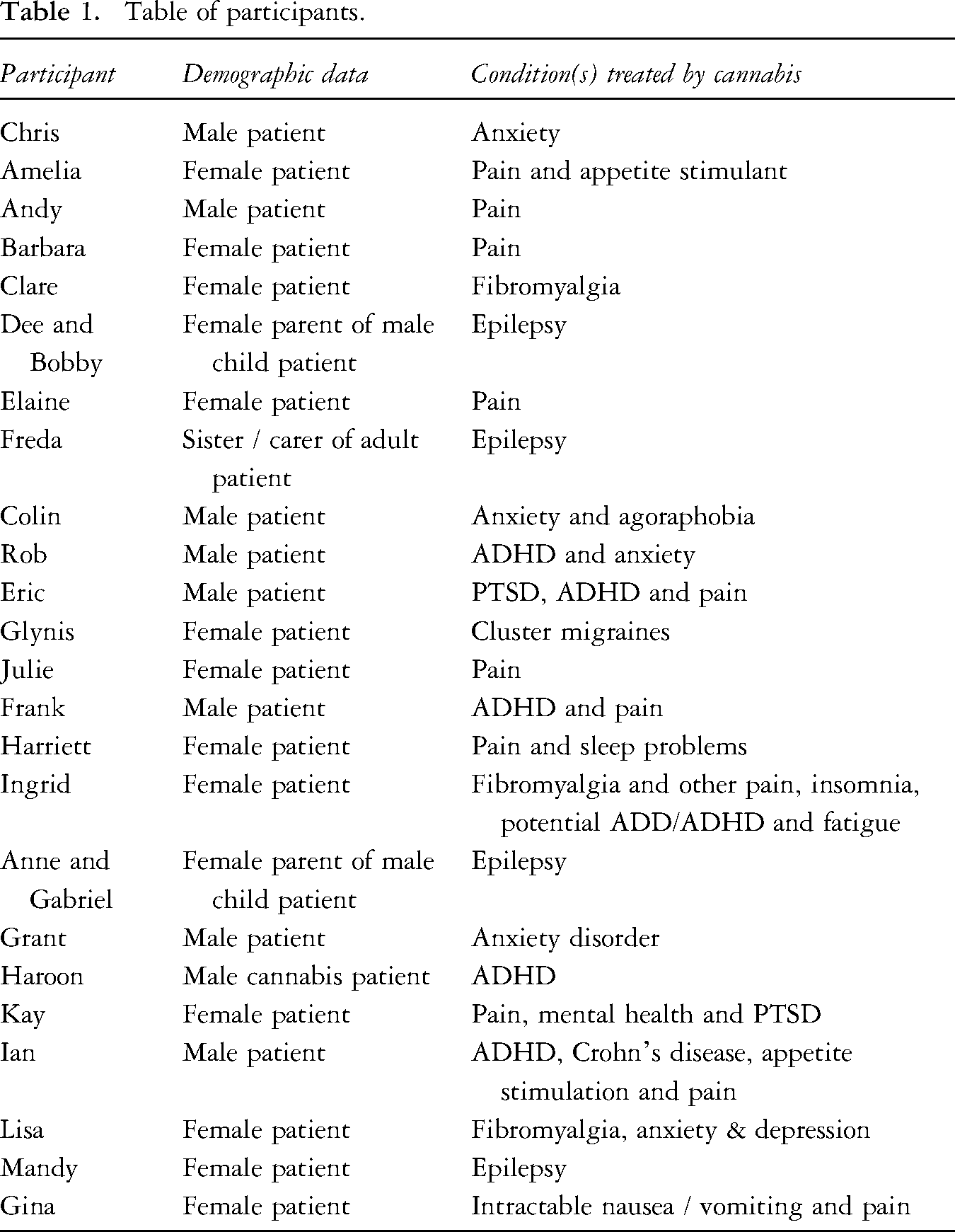
Patient profiles (pseudonyms and conditions) are included below. We did not collect detailed demographic information to protect patient anonymity, at the request of several participants. As a relatively small population, prescribed patients felt that the inclusion of granular detail in talking about their lives risked identification/exposure (Table 1).
Table of participants.
The British Society of Criminology’s (2015) ethical considerations underpinned this research. Knowing participants lived with a range of chronic health conditions and/or disabilities, accessibility was designed into the project. To this end, recruitment was through social media and interviews conducted virtually using Microsoft Teams conferencing software. This complied with health and safety guidelines in the aftermath of Covid and extended the study's geographical reach across the UK. It also meant patients could participate from the comfort of their homes and undertake interviews in short segments if needed. This strategy was approved by the University Research Ethics Committee.
With participants’ permission, interviews were recorded and transcribed. Reflexive thematic analysis was employed to analyse the data, which involved familiarisation with the transcripts and extensive development of semantic and latent codes (Braun and Clarke, 2021). Coding was inductive, to elicit participants’ ‘experiences, perspectives and meanings’ (Braun and Clarke, 2021: 56). Through iterative processes of data immersion and reflection, codes were refined into central themes of cannabis benefits and drawbacks; evidence, education and expertise; patient representation and communities; and stigma. The stigma data forms the basis of this article and was divided into stigmatising social interactions in healthcare; police and security services; work and home life; and resisting stigma. These themes act as headings in the Findings Section below.
Findings and discussion
Stigmatising social interactions
Gps, doctors and consultants
Having obtained a cannabis prescription (typically, given the context outlined above, from a private clinic) some patients were surprised to encounter NHS professionals who were unaware that cannabis prescribing was legal, or the processes for obtaining it on prescription. Some health professionals were curious and responsive to the patient explaining how they took their cannabis medication and its benefits (we discuss this, with examples, later). However, as with patients in other prohibitionist contexts (Satterland et al., 2015), some patients reported doctors who relayed enduring cannabis stereotypes and demonstrated negative attitudes. Ingrid's (patient) GP exposed a lack of understanding about the relative risks of cannabis when he suggested he would ‘rather be addicted to sleeping pills than … cannabis.’
Kay had been treated with Pregabalin for ten years for post-surgery spinal pain. She stopped taking it because it severely impacted her memory. She turned to illicit cannabis, then moved to a legal prescription when the law changed. However, she experienced pressure from her GP to replace the cannabis with anti-depressants. She explained the change cannabis had brought to her life: ‘All my life I’ve been carrying on swimming because it's the only safe physiotherapy and I’ve really tried, and I’ve kept going. I even went to university and got myself a master's degree. I was so knackered, but I never gave up and the cannabis enabled me to keep swimming and gave me a life’ (Kay, patient). ‘I’d still rather look like a lazy pot head fake than look like someone that I should look like with my condition, because I wouldn’t have lived this long. I’d never have survived without it, and I’d never have done the things that I’ve done. Not that I’ve done much but I kept going and I had a life whereas others didn’t have a life because they didn’t use the cannabis’ (Kay, patient, emphasis added).
Some patients noted that lack of training on cannabis medicine led some consultants to react badly to patients, leading to stigmatising treatment. One said: ‘You go and see this doctor, and he has just gotten it confused [with illicit cannabis]. Instead of going “OK, I don't know about this, I'll get back to you”, he got his back up. And so, we kind of had to almost appease him. In the end I said OK I'll go, because he was getting quite irritable. You don't want that when all I want is to get everything settled peacefully. So, we had to stop the conversation…It shocked us, what he was like. Then he said, “Oh yeah, but there's a lot of stigma around it, isn't it?” And my wife was like, “Yeah, I think we're experiencing that now!”. I just think it was because it was that particular drug… it was a bad reaction. My wife felt it. I felt it as a patient, and I don't think I should have. It was uncomfortable’ (Gina, patient). ‘[T]here's a language you need. It's like anything. Some people can just do business deals of millions of pounds over a beer or whatever it is, and some people struggle to job interview for Tesco. I don’t want to call it classist, but it is. You don’t want to call it moneyist [sic], but it is. Just like many other things in life, if you can’t afford it and you don’t have the way to get it, you’ll regret it. That's the American way - if you can’t afford insulin, die, simple as that. But it shouldn’t be like that in this country. It really is heart breaking …[O]bviously people who have got money are going to be in a very different situation to people who don’t. You may find that you’ve got … people saying, “Well it was easy” [to access cannabis], but you’ll find it's all white collar, earning £150,000 a year category. It's going to be very different to the unemployed’ (Julie, patient).
Police and security officers
Encounters with the police raised concerns for several participants. Amelia took precautions whenever she went into public spaces to protect herself legally: ‘If I’m not driving anywhere and I’m in an open space like a park, I would bring just what I need for that trip, and I would have it in the container that it's prescribed in, and I have on my phone the letter from the clinic … and you would just have to hope that if the police officer came over, they would accept that’ (Amelia, patient). [I]f I’m out and about, I’ve got a wheelchair, so it's fairly obvious that I’m a disabled person. I have a kind of visual cue for police that ‘Okay, this person isn’t pulling my arm’ (Amelia, patient). ‘He saw I'm in a wheelchair. Maybe he felt sorry for me. We went through…But I don't know if I’d gone to the next [security] guy over, whether I'd have had a bad reaction. You just don't know’ (Gina, patient).
As a Black woman, Lisa was acutely aware of the racist and political context of cannabis prohibition and made reference to the ‘war on drugs’. She spoke of trauma arising from a prior police caution for self-medicating with illicitly obtained cannabis. This made her initially hesitant to pursue a legal prescription, fearing records would make her a target for police attention: ‘[I thought to myself] “You’re setting yourself up to get raided. You’re handing over your details. It's an invitation for the police to come and harass you’ (Lisa, patient).
A reoccurring patient concern was whether prescribed cannabis could be used in public spaces, and potential reactions of other people who may instigate confrontations with representatives of the law. Patients prescribed cannabis flower felt this anxiety acutely, as the distinctive smell can attract attention. This resulted in some staying at home when medicating. Others planned ahead, to navigate medicating outside. ‘[I’m afraid people will smell the cannabis on me and try to steal it]. I’m pretty vulnerable with a walking stick. It's obvious I’m disabled. But I also feel vulnerable with … people smelling it and [calling the police]’ (Kay, patient). ‘[I’d been thinking that] it's probably inappropriate on a bus ride to pull out your vaporiser and annoy people. But actually, if [someone] was on a long train journey and had a seizure or a mental health crisis or any manner of complex disability that I have no right to know about… they’ve got a right to use the train in peace and quiet and symptom free. Sometimes people suddenly need to medicate for unknown reasons… it would be nice if we lived in a society where they could be free and comfortable to do that without harassment’ (Grant, patient).
Work and home life
Concerns around legal challenges extended into work and home life, with patients fearing confrontation from employers, landlords, friends, and family.
Patients provided insights into their daily decisions about whether to ‘come out’ as having a cannabis prescription. Decisions were taken in a range of contexts, with patients deliberating over the potential reactions of others. ‘I am interested whether my last employer would have allowed me to take my medication at work… So, let's say I took this medication, and it made me a little bit better to go back to work. Does that raise an alarm? But any other medication that you take, if it's making you better, you wouldn't be questioned. You wouldn't have questioned it because doctors know about it’ (Gina, patient). ‘If they knew about my medical cannabis, maybe the landlord wouldn’t accept me. And what would the neighbours think?’ (Mandy, patient)
Ex-soldier Eric was prescribed cannabis for PTSD and a spinal injury following active service. He hid his medication from his children, consuming his oil in a separate part of the house and vaping only after they were in bed. The improvement in his health was so great that he and his wife had to explain to their children what had changed. They said daddy had a new medication, but Eric did not feel able to reveal the full truth, for fear of stigmatisation: ‘I didn’t say it was called cannabis… I just said it's a flower, a plant. They don’t know how I do it, they just know that I’m not taking all of those tablets anymore and I’m using a flower. That's what they know, and they love it’ (Eric, patient). ‘[If somebody had seen it or smelt it or noticed what I was doing, their kids may have known my kids and then it would have been around school that my kid's father is a junkie or something… I didn’t want what I’m doing to stigmatise them [my children]’ (Eric, patient).
Resisting stigma
Patients did not passively accept stigma; they adopted a range of strategies for resisting. We term these strategies concealment, (re)construction and evangelism (outlined below). Resistance strategies were not specific to individual patients – the same person might deploy different strategies to negotiate different contexts and could switch strategy depending how they were feeling. Reid (2020) likens cannabis stigma to those faced by sexual minorities, observing that this comparison helps illuminate the lingering impact of stigma and trauma, even after legalisation. Taking this analogy further, just as ‘coming out’ as LGBT + is not a single ‘moment’ but regular and repeated decisions in different contexts with different people, we argue that ‘coming out’ as a medical cannabis patient is experienced as a series of daily situations and interactions. In this section, we highlight the strategies employed by participants to resist cannabis stigma and navigate repeated ‘moments,’ in which patients consider whether, how and when to discuss their cannabis medication.
Concealment
Participants employed a range of strategies to mitigate the stigma they experienced. The first strategy was concealment, where patients either hid the fact that they took cannabis or used their medication discreetly. Several reported feeling self-conscious of the smell created by vaping cannabis flower. Exercising discretion about when and where to use their medication was a reoccurring theme. Colin told us he used Google maps to locate discrete places to medicate, to avoid confrontation, whenever he left home. Others too described their daily anxieties about where to medicate. ‘I would feel anxious having gone for a walk [while using my medication] and [I would] keep it out of the way of people… [for example] if suddenly a family emerge out of nowhere with young kids’ (Grant, patient). ‘I made sure it was in a fairly secluded area of the park, that there wasn’t anyone around’ (Eric, patient).
(Re)construction
A second strategy employed to mitigate stigma was patients emphasising their identity as a ‘medical’ cannabis user who specifically avoided recreational or illicit use. Some perceived that a specific benefit of their prescription was how it distanced them from illicit users and marked them as different from the stereotypical ‘user’.
Patients also felt their prescription offered a degree of protection from criminalisation. Frank explained it was worth paying ‘premium’ prices at his private clinic (compared to street prices) for reduced anxiety about potential “harassment by the police”. Another patient recalled seeking illicitly purchased cannabis in desperation to alleviate her pain. After experiencing the relief it offered, she prioritised obtaining a prescription: ‘That was the first and pretty much last experience on the black market. I’m not a criminal and I don’t do these sorts of things. It was completely out of character for me. I thought “I must be able to do this legally”’ (Julie, patient). ‘Although the stigma is there, the fact that I now get it [on prescription], it's validated as a medicine. So, when you say, “I get it legally prescribed on prescription,” they cannot see you as a lazy pot-head druggie because I get it legally’ (Kay, patient). ‘As soon as you say, “cannabis prescription”, the bias goes … [people think] illegal cannabis [equals] bad, [but] prescription cannabis, oh, that's good for you, that's fine. It's a mindset and it needs changing because [cannabis] it's all the same. But it's the situation that we’re in, the government has brainwashed them quite successfully’ (Barbara, patient).
Evangelism
The final patient strategy to combat stigma was ‘cannabis evangelism’. Stories of improvements to health and quality of life, where conventional medicine had failed, abounded: ‘[Cannabis] is like a miracle, and I can’t explain it any other way. I didn’t have a life… and it gave me one’ (Mandy, patient) ‘I got into patient advocacy stuff… now, my whole thing is helping other people – especially people of colour – to navigate [the process for getting a prescription]’ (Lisa, patient). ‘I’m pretty open about it because I think that for any hope of ending the stigma, we kind of have to be, because it's just medicine’ (Amelia, patient). ‘…[A]t first there were a couple of carers who were a bit, “Oh, I’m not comfortable giving her cannabis.” After a good long chat with them, they got it. The same carers are now saying, “Freda, can you get my mum some oil?” Honestly! I’m converting the masses slowly but surely, we all are’ (Freda, patient carer).
Concluding thoughts
Cannabis stigma is multi-level and intersectional
Our findings demonstrate the stigmatisation that cannabis patients encounter. The context of UK historical and contemporary prohibition policy demonstrably produces stigma. Hegemonic prohibition undermines the status of cannabis as a legitimate medicine, whilst reinforcing its construction as an exclusively harmful drug, associated with deviant and criminal drug users. Consequently, cannabis patients encountered these discourses among professionals and in their everyday social interactions. Some had met healthcare professionals with mis-informed beliefs about the (il)legality of prescribing, or stigmatising attitudes towards the drug. Some had experienced interactions with the police that exposed a lack of training, which left officers reliant on prohibitionist beliefs and tropes about cannabis. Finally, participants told of stigmatising reactions to their cannabis prescription from the people around them, including family and friends. Choosing when and how to disclose their prescription was a stressful decision faced by patients on a regular basis. The (re)production of stigma from political discourse, through policy, and into the everyday, accords with other analyses (Link and Phelan, 2001; Reid, 2020 and Tyler, 2020).
Our evidence supports Tyler and Slater's (2018) point that racism and class struggle must be central to analyses of stigma as a form of power. Patient stories bear witness to Taylor et al.'s (2016) drug apartheid, in that cannabis stigma is experienced differently along racialised lines. Given the racism associated with historic prohibition policies, and evidence of disproportionate stop and searches of Black people under the Misuse of Drug Act 1971 (Shiner, 2015; Taylor et al., 2016) it is unsurprising that Black cannabis patients fear differential treatment and police harassment.
Socio-economic status is also integral to the experiences of cannabis patients, with health inequalities produced by the lack of NHS prescribing and consequent reliance on private medicine for legal access. This intersection of status and stigma is also underlined by participants who described the need to speak the ‘right language’ to gain recognition by doctors, or to represent themselves in a particular way to the police if challenged.
Cannabis stigma is similarly entangled with experiences of chronic illness and reduced capacity for work, feeding into stereotypes already imposed upon people with disabilities and those who claim benefits for example (Scambler, 2018). A further intersection arising in the data is that of parent / carer. In caring for disabled or chronically ill children, parents experience the stigma of disability and ‘go into battle’ to navigate institutions such as healthcare systems (Thomas, 2021). They are tasked with the hidden and, crucially, gendered work of coordinating care for their child (Østerud and Anvik, 2024), and concerns about potential responses to their child's cannabis medication, from doctors through to grandparents, serves as an additional burden. This fear of ‘courtesy stigma’ accords with Newhart and Dolphin’s (2021) study of cannabis stigma in the US. Adults who are a cannabis patient and a parent encounter negative stereotypes such the ‘bad mother’ discourse around substance-using mothers (Reid et al., 2008) and fears of additional judgements about their fitness to parent.
Resisting stigma through power struggles
Like Link and Phelan (2001: 378), we argue that stigmatised groups are not passive recipients of stigma but are engaging in ‘power struggles.’ Our participants employed strategies to resist and deflect stigmatising cannabis stereotypes and tropes. Most strongly believed that raising awareness about the benefits of medical cannabis held the key to combatting stigma. We heard many stories of cannabis patients educating, changing people's misinformed opinions, and challenging cannabis tropes, with their doctors, their friends and family and even the police. However, as Link and Phelan (2001: 378) highlight, ‘to the extent that power differences exist, resistance cannot fully overcome constraint’. To engender change, education about medical cannabis is certainly crucial, but must be accompanied by the dismantling of the criminalisation of social policy, and a commitment to provide equal access to cannabis medicine for those who need it.
Policy recommendations
Our participants’ experiences demonstrate the need for national programs of both professional and public education, to raise awareness of legal cannabis prescribing. This needs to be provided for all health professionals; not only potential prescribers, but all who meet with patients, to avoid stigmatising attitudes. Police officers, airport and security staff also need training, to protect the legal freedom of cannabis patients and avoid reputational damage in instances of unwarranted attention. Public facing organisations, venues and transport providers need to make provision for cannabis patients, both in terms of staff training and safe medicating spaces.
Stigma processes are rooted in power (Link and Phelan, 2001, 2014; Tyler, 2020). Paton (2018: 919) underlines the importance of ‘gazing up’ rather than ‘gazing down’ to look ‘at the stigmatisers … and not the stigmatised’. While training and education are undoubtedly needed, we cast our gaze upwards to the source of cannabis stigma, which is the social construction of the drug. Risk discourses and subsequent criminalising policies are produced by neoliberal governance; deployed to demonstrate to the public that they are being ‘protected’ from the threat of dangerous drugs and drug users, and to control specific sections of the population. To dismantle these discourses and genuinely reduce harm requires renewed efforts to challenge state authority and persuade the government to give due regard to the growing global evidence base against prohibition and in favour of cannabis prescribing.
Footnotes
Funding
This study received a small grant from Liverpool John Moores University for interview transcription and some research assistance.
Liverpool John Moores University,United Kingdom.