
Abstract
This article considers how minoritisation features in Domestic Homicide Reviews (DHRs) in England and Wales and identifies critical learning in relation to addressing minoritisation. Five themes were identified: i) the invisibility of race, culture and ethnicity; ii) perceptions and experiences of services; iii) use of stereotypes and the culturalisation of domestic violence and abuse (DVA); iv) lack of interpreters; and v) DHR recommendations. Our analysis illustrates that statutory sector services should strengthen their responses to Black and minoritised victims by ensuring proper recording of cultural background is used to inform practice; engage professionally trained interpreters with an awareness of DVA; resist framing DVA as endemic to minoritised cultures; and enhance trust and confidence in public services within minoritised communities. The best examples of DHRs challenged service narratives and usually sought expertise from a specialist Black/minoritised DVA service or community organisation (frequently minoritised women's rights organisations).
Keywords
Introduction
Domestic homicide is a gendered global phenomenon. In 2017, 87,000 women were killed worldwide; 30,000 were killed by intimate ex/partners and 20,000 by family members (UNODC, 2018: 10). Women represented 82% of all intimate partner homicides in 2017 globally (UNODC, 2018: 19). In England and Wales, 114 domestic homicides were recorded between April 2020 and March 2021, similar to the average for the past five years (ONS, 2022a). Of these, 59% (n = 67) were intimate partner homicides, mostly involving female victims (n = 57, 85%), with the remaining 41% (n = 47) representing adult family homicides, mostly involving male victims (n = 29, 62%) (ONS, 2022b). Overall, women represented 66% (n = 75) of domestic homicide victims for that year, and men were principal suspects in 88% (n = 100) of cases (ONS, 2022b).
The Crime Survey for England and Wales (ONS, 2021) estimated that 5.5% of adults aged 16 to 74 years (2.3 million) had experienced domestic violence and abuse (DVA) between April 2019 and March 2020, of which 1.6 million (70%) were women. Those in the White and Mixed ethnic groups were significantly more likely to be victims than those in the Asian or Black ethnic groups, although some categories had small numbers so caution is required (ONS, 2020).
Domestic Homicide Reviews (DHRs) are a statutory requirement in England and Wales under section 9 of the Domestic Violence, Crime and Victims Act (2004), instituted in 2011. They are commissioned by Community Safety Partnerships in England, and Public Service Boards in Wales, following a domestic homicide where a person aged 16 or over dies from violence, abuse or neglect by a relative, intimate partner or member of the same household (Home Office, 2016). An independent chair is appointed to lead a multi-agency panel to identify lessons learned and make recommendations to strengthen responses to DVA with the aim of preventing escalation to domestic homicides in the future (see Haines-Delmont et al., 2022 for a detailed explanation of England & Wales DHR processes). Agencies (e.g. health services, criminal justice agencies, victim services, social care, education) are required to produce an Individual Management Review report which provide details of their contact with the victim, perpetrator, and any children. These are analysed by the DHR panel and recommendations made in an Overview Report (the DHR) which is quality assured by the Home Office prior to publication. Similar review systems include Safeguarding Adults Reviews, and Mental Health Homicide Reviews – concerning homicides committed by mental health patients (see Robinson et al., 2019).
Existing England and Wales DHR studies are often small scale (e.g. Benbow et al., 2019; Robinson et al., 2019; Sharp-Jeffs and Kelly, 2016), none of which specifically focus on minoritisation. Benbow et al. (2019) report that demographic information, particularly ethnicity, was often redacted within DHRs in the interests of anonymity, making it difficult to identify them. However, we located 95 DHRs relating to minoritised homicide cases which took place between 2011–2017, representing the first study of its kind in England and Wales.
This paper focusses on DHRs where either the victim or perpetrator were from a Black or minoritised background. This included White British victims (born in the UK in interracial relationships) and White Europeans (e.g. Eastern Europeans) originating from outside of the UK. Black and minoritised victims in relationships with White British perpetrators are also included. The rationale is that these victim groups illuminate the racialised dynamics that perpetrators frequently benefit from and that service responses often bolster – e.g. victim fears that minoritised perpetrators may experience racism if victims disclose DVA; the erroneous assumption that DVA is tolerated in minoritized communities; perpetrators generating fear where the victim's immigration status is dependent on him. These dynamics work to strengthen the perpetrator's power within the abusive relationship. Case-level variables offer key contextual information about the victim-perpetrator relationship.
The aims of the study are to:
Analyse contextual case-level and victim characteristics of this sample. Explore how issues of race, ethnicity and culture are discussed in DHRs and service narratives. Recommend changes to develop policy and practice regarding i) DHR processes and ii) service responses.
Terminology and implications
Minoritisation refers to a socio-historical process based on unequal power relations whereby groups and communities come to be positioned as minorities (Burman and Chantler, 2005). It recognises the active processes of othering, unequal access to resources, power, cultural capital and discourses (Burman et al., 2004; Gunaratnum, 2003). Our data reveals significant similarities across minoritised groups which are important to ensure that learning from DHRs have the widest applicability. Hence, our analysis focuses both on visible minorities and White minorities. Different processes of minoritisation affect first, second, third generation and more recently arrived migrants and people of different ethnicities. We argue later that there is a slippage in minoritisation processes between migrants and minoritised victims through the creation of the ‘hostile environment’.
Gender-Based violence (GBV) is used internationally, referring to harmful acts which disproportionately affect women and girls. The United Nations (UN) defines GBV as based on deep rooted gender inequalities, bolstered by laws, institutions and communities (UN, 1993). The UN High Commission for Refugees (UNHCR) makes explicit that GBV is a serious violation of human rights. Forced marriage and female genital mutilation (FGM) are frequently specified in understandings of GBV as ‘harmful cultural practices’ (Longman and Bradley, 2016). Whilst the recognition of diverse forms of GBV is welcomed, their construction as ‘harmful cultural practices’ requires further interrogation as it works to ‘other’ minoritised women. Such categorisation suggests that mainstream GBV is neither a cultural practice nor harmful, which is problematic (Chantler and Gangoli, 2011; Gill and Walker, 2020). Socio-cultural norms are inherent aspects of reinforcing GBV and many policies advocated internationally to prevent GBV focus on changing cultural and social norms (WHO, 2009). It is widely accepted that women and girls are killed by intimate partners/family members due to discrimination, misogyny and unequal gendered power relations (UNODC, 2018).
DVA is the most common type of GBV but has a narrower definition as it often eschews the explicit human rights violation and gendered dimensions of GBV and does not mention specific abuses more prevalent in minoritised communities. Nevertheless, both terms will be utilised according to the terminology used in the literature cited. England and Wales’ definition of DVA is: ‘an incident or pattern of incidents of controlling, coercive or threatening behaviour, violence or abuse between those aged 16 or over who are, or have been, intimate partners or family members regardless of gender or sexuality’ (Home Office, 2016: 12). This definition is reflected in the Domestic Abuse Act 2021 and its breadth allows for abuses including adult family abuse, forced marriage, FGM and honour-based abuse. The most extreme consequence of DVA is domestic homicide.
The term victim-survivor is used regarding recommendations for future service developments as these refer to lessons identified from a domestic homicide to strengthen responses to existing or future DVA victim-survivors.
Background
Combatting GBV internationally is addressed by a range of policies using social, public health and criminal justice responses (UNODC, 2018), including the Istanbul Convention in Europe (Council of Europe, 2014). The Istanbul Convention is a European human rights treaty which establishes a comprehensive approach to GBV. It's aims are to prevent GBV, protect victims and prosecute perpetrators. The UK has declined to ratify the Istanbul Convention as it is reluctant to commit to protecting migrant women experiencing GBV (EVAW, 2021).
In the year ending 31 March 2017, DVA was estimated to have cost over £66 billion in England and Wales. The largest cost is the physical and emotional harms (fear, anxiety and depression) incurred by victims (£47 billion). The estimated cost to the economy is £14 billion arising from lost output due to time off work and reduced productivity due to DVA. Costs to the public purse include health services (£2.3 billion); police (£1.3 billion); housing costs and victim services (£550 million) (Oliver et al., 2019).
There is limited UK or international literature regarding minoritisation and domestic homicide. Vatnar et al. (2017) argue that socioeconomic factors are central to domestic homicide, demonstrated in studies comparing domestic homicide between minoritised and White communities in Norway. They found that factors such as higher rates of unemployment in minoritised communities, racism and related social disadvantage may be more important than ethnicity or culture. Similar findings are reported in the US (Centerwall, 1995). An analysis of 84 London-based DHRs (Montique, 2019) indicates the need to develop intersectionality within DHR processes. Regarding minoritised victims, it highlights immigration status as a barrier to support and the need for agencies to liaise with minoritised specialists when supporting DVA victims.
DHR recommendations focus on improving DVA responses for victim-survivors, so next we summarise the literature relating to DVA and minoritisation. Femi-Ajao et al. (2020) found four barriers preventing DVA disclosure to services for Black and minoritised victims in the UK: immigration status, particularly ‘No Recourse to Public Funds’, community influences, lack of interpreters, and unsupportive attitudes from staff within mainstream services. These interconnected barriers are reflected in the under-reporting of DVA for minoritised women (Sundari, 2008; Femi-Ajao et al., 2020) and can prevent victims from seeking support or restrict their ability to leave an abusive environment (Begum et al., 2020; Burman et al., 2004; Dudley, 2017; Sundari 2008). Spousal migrants to the UK are often unaware of their rights and can be manipulated by their perpetrators into believing that they could be deported or separated from their children should they seek support (Begum et al., 2020; DAC, 2021; Harrar, 2021). However, deportation is a possible outcome and insecure status engenders fear of services (Chantler et al. 2003; Dudley, 2017; Sundari, 2008).
A lack of understanding of culture and community influences has meant that some professionals make assumptions about the levels of abuse that are acceptable within these diasporas, deciding not to intervene to respect multiculturalism and fears of being labelled culturally insensitive or racist (Begum et al., 2020; Burman et al., 2004; Chantler et al., 2021; Wiper, 2012). Chantler et al. (2001) have termed this ‘race anxiety’, resulting in a loss of protection for DVA victim-survivors. Services may also be reluctant to engage with communities, limiting opportunities to inform migrant victims about their rights in the UK (Harrar, 2021; Siddiqui, 2018). Further, incomplete records on the ethnicity of individuals affected by DVA and homicide in the UK, makes it difficult to ascertain the prevalence of DVA in minoritised communities (Begum et al., 2020; Chantler et al., 2020; Dudley, 2017; Rowlands and Cook, 2022; Wiper, 2012).
Phoenix's (1987) characterisation of ‘normalised absence/pathologized presence’ is highly pertinent to our analyses. Normalised absence refers to how minoritised people are normally invisible in research, but when present, are frequently constructed through a pathologizing frame. This twinning of normalised absence and pathologized presence is conceptually very helpful in our analysis. Our focus on minoritisation is important because the primary function of DHRs is to prevent future domestic homicides and to strengthen responses to DVA. Policy makers, practitioners, DHR panels and review authors need to be cognisant of how minoritisation may play into service responses, in analysing antecedents to domestic homicide and recommendations made, thus disrupting their normalised absence. However, the spotlight on ethnicity risks feeding stereotypes of ‘barbaric others’ (Razack, 2004) and passive victims (pathologized presence). Yet not speaking about issues of race, culture and ethnicity means that related specificities may be overlooked in generic writings on domestic homicide (normalised absence).
Method
Publicly available DHRs from local Community Safety Partnership websites in England and Wales were collected in collaboration with the King's College London (n = 302). This paper analysed a sub-sample of these DHRs (n = 95, 31%) purposively selected due to either the victim or perpetrator being from a Black or minoritised background. The 95 DHRs relate to homicides that occurred between 2011 and 2017 across 23 Police Forces. Ethical approval was not required due to the public availability and anonymisation of DHRs.
Utilising existing literature and our previous work, templates were refined to systematically extract quantitative and qualitative data from DHRs. Quantitative variables were extracted and coded into Excel capturing information on: victim and perpetrator characteristics; relationship characteristics and history; ethnicity; immigration status; risk factors; and agency responses and contact. A thematic document analysis (Gross, 2018) was undertaken using a qualitative template capturing key components related to minoritisation (use of interpreters, organisational culture, service response) and the information presented within the report such as equalities information, panel expertise, and recommendations. Our qualitative template included extraction for criticisms and recommendations that DHRs made – all providing insight into service effectiveness. However, researchers also read DHRs critically and identified patterns where the information presented did not generate appropriate recommendations or where DHR panels/authors were unaware that they were replicating stereotypes. NVivo20 was used to organise, classify and analyse this data. Interpretative coding was completed manually alongside automated coding to check researcher interpretation. Information, classifications, and trends were cross-examined which enabled the research team to conceptualise, examine relationships and interrogate the data.
Findings
Case-level characteristics
The sample comprised mostly intimate partner homicide cases (81%, n = 77); the remainder were adult family homicide (18%, n = 17), most commonly sons killing their mothers, and one case involving the murder of a housemate. Intimate partner homicide victims were most commonly female (95%, n = 73), largely killed by male partners (49%, n = 38) or ex-partners (45%, n = 35). Most victims and perpetrators had been in their relationships for over five years (55%, n = 42) with the largest category representing relationships of over 10 years (36%, n = 28). Only 12% of intimate partner homicide cases (n = 9) involved couples who had been together for less than a year. Nearly half (46%, n = 35) of intimate partner homicides involved couples who had separated. Of these, the majority (66%, n = 23) had separated within 12 months prior to the homicide, most commonly between one and six months (29%, n = 10). Most victims and perpetrators (64%, n = 61) were living together at the time of the homicide. Just over a third (34%, n = 21) also lived with other adults, usually other family. Most cases (85%, n = 81) contained evidence of prior DVA in the victim-perpetrator relationship, with nearly all (99%, n = 80) involving the use of DVA by the perpetrator towards the victim.
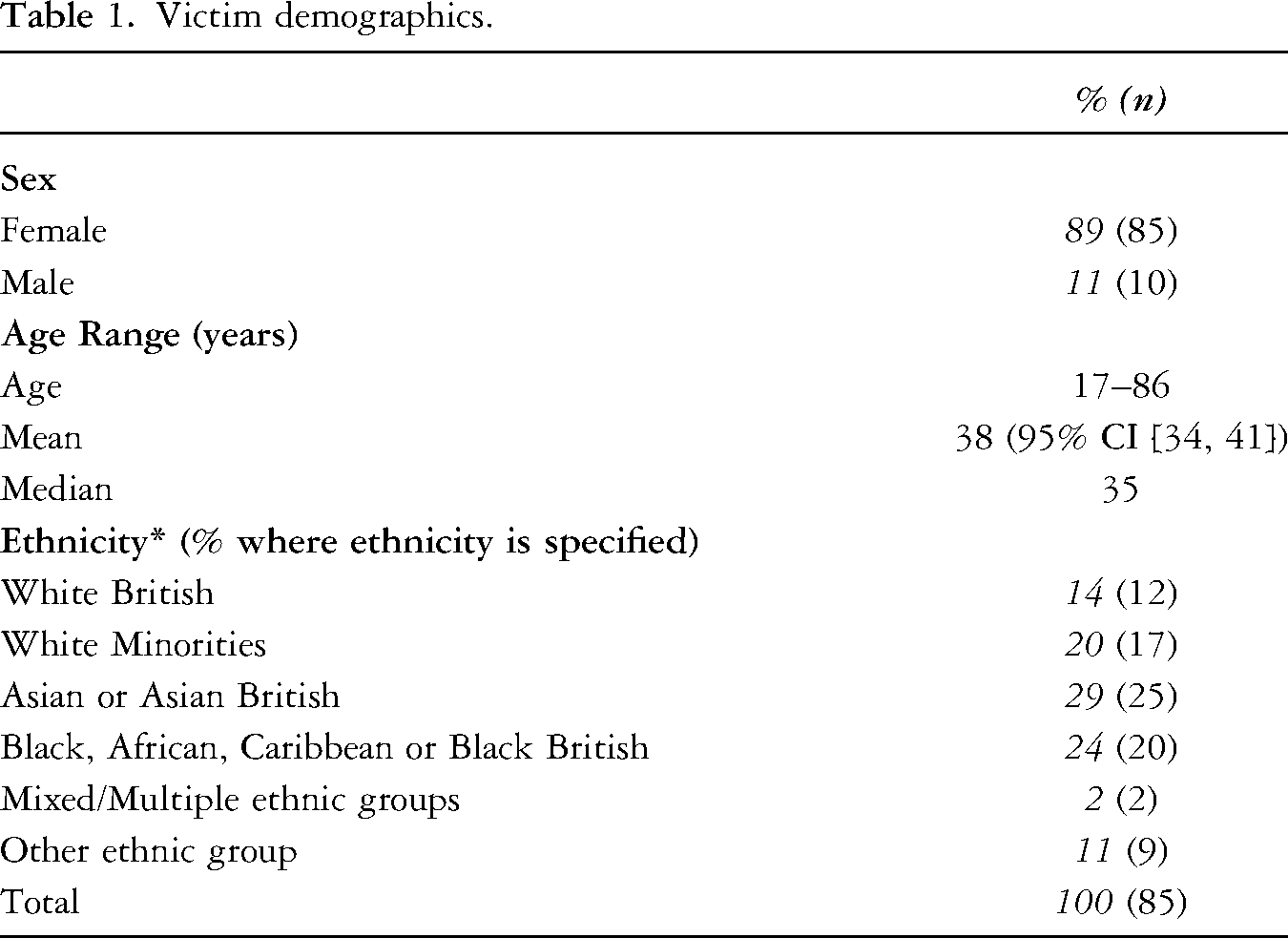
Victim demographics
Most victims were female (89%, n = 85) and aged 17 to 86 years. Victim ethnicity data was provided in 85 (89%) of the 95 DHRs. The most common ethnicity categories for minoritised victims were ‘Asian or Asian British’ (29%, n = 25) followed by ‘Black, African, Caribbean, or Black British’ (24%, n = 20). White minorities from Eastern Europe, Southern Europe and Ireland formed the third largest group (20%, n = 17). Lastly, there were 12 White British victims (14%), killed by a perpetrator from a minoritised background (see Table 1). Over half of victims (54%, n = 51) had migrated to the UK. Of these, 73% (n = 37) had done so at least five years prior to the homicide, with nearly half (47%, n = 24) having lived in the UK for over 10 years.
Victim demographics.
Five inter-linked themes were identified from our qualitative analysis.
Invisibility of race and culture
Most commonly, issues of racism, ethnicity and culture were eschewed, reflecting a normalised absence. For example, DHR213 notes that the victim was from [African country] but does not detail her ethnicity, aside from a single opaque reference to perceptions of ‘Afro Caribbean women’ (DHR213: 77). This occlusion was seen in other DHRs where there was only one sentence stating the victim's ethnicity with no further mention of how their social locations might have impacted on engagement with and responses of services.
DHR good practice is where DHRs challenged the Individual Management Reviews produced by services: Several agencies had no details of ethnicity, nationality or religion as these were not recorded at the point of the referral. It is a core principle of good practice to ensure agencies know the background of those using their services; otherwise they have no information to consider in what way they might need to adapt and improve access (DHR234: 68).
Perceptions and experiences of services
Perceptions of services were inconsistently reported. Where reported, these frequently illustrated fear and mistrust of services, exemplified by: ‘There is a recognised distrust of authorities and much of this is a cultural issue. This also has a profound effect on the use of services, as many will avoid engagement with statutory agencies’ (DHR189: 19). Sometimes fears were based on negative experiences with agencies in countries of origin, but nearly half of the sample who had migrated had lived in the UK for over ten years. Lack of awareness and understanding of UK laws, culture, available support, and deliberate misinformation by perpetrators also influenced perceptions of services. Insufficient knowledge was partly due to isolation but also attributable to limited service promotion or missed opportunities by professionals.
In over one third of DHRs, perceptions of services influenced help-seeking prior to the homicide. For example, DHR099 discusses a White British woman killed by her Black British ex-partner. The DHR states: ‘We have not identified any equality or diversity issues in this case in respect of the family of Ms FC. They are white British residents and there are no diversity, disability or sexual orientation concerns.’ (DHR099: 46). However, the DHR mentions that the victim was concerned about seeking help as: ‘She was worried about what might happen to him as a black man if he was found to be harassing a white woman’ (DHR099: 28). Fears of institutional racism appear to have been overlooked in the DHR and the opportunity to enhance perceptions of police/minoritised community relations was not identified or recommended.
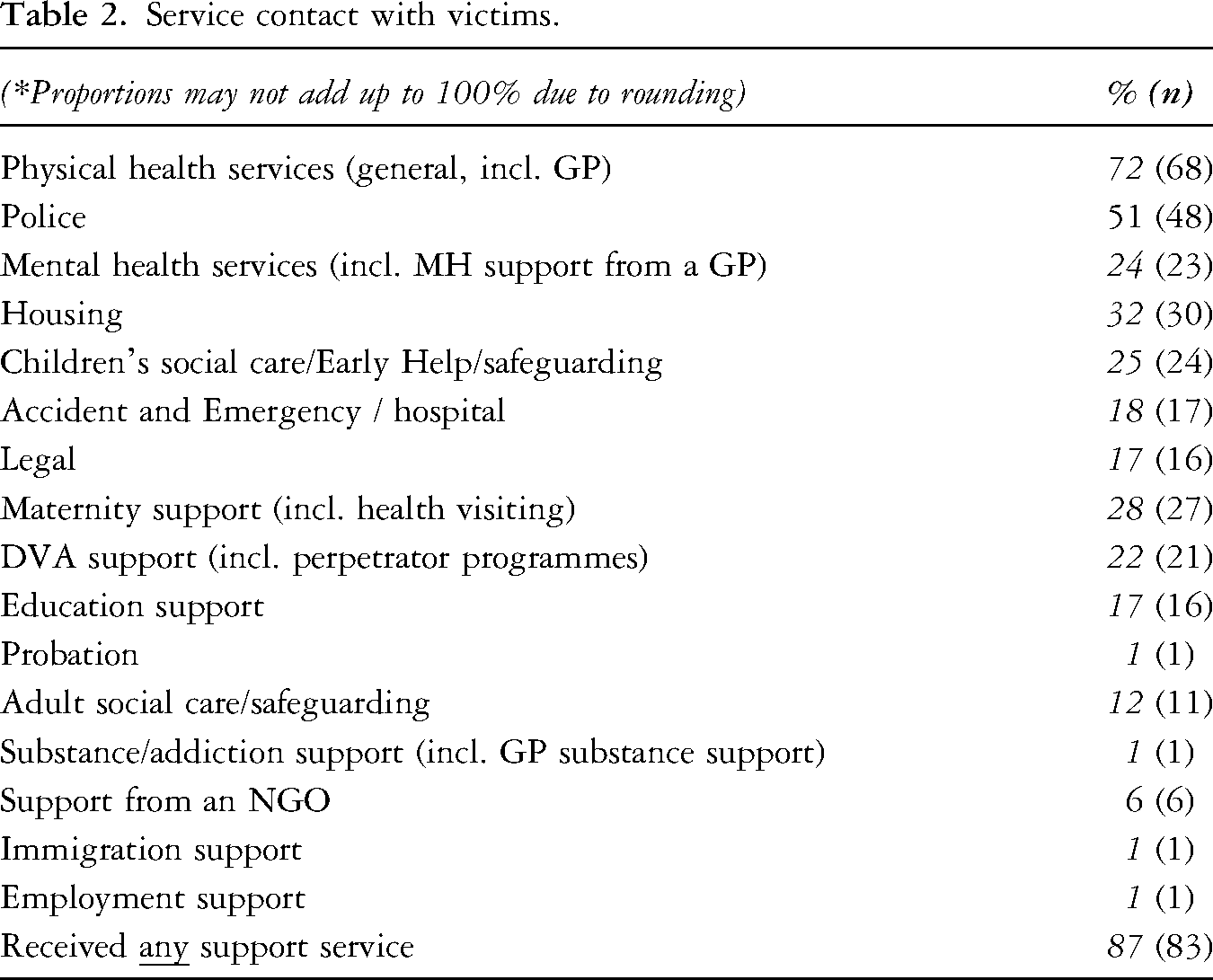
Perceptions of services is key, given that most victims (87%, n = 83) had some form of agency contact (see Table 2). Statutory agencies were often aware of the DVA (57%, n = 54), most frequently the police (47%, n = 45), health (39%, n = 37) and children's services (25%, n = 24). Assessments were carried out in over half (53%, n = 50) of the DHRs, relating to either DVA in the victim-perpetrator relationship, or the risk of harm posed by the perpetrator (to the victim or partners more broadly). Where assessments had been completed, only eight cases (16%) had a ‘High’ risk rating.
Service contact with victims.
DHRs reported that victims had prior negative help-seeking experiences and inadequate responses to victimisation. DHR210 counted over 800 agency contacts in the nine years before the homicide and several hundred throughout the victim's childhood. Opportunities to intervene and offer support were missed throughout. The victim and her family were subject to racist abuse and harassment, including their home being burned down. The DHR panel acknowledged that these experiences and professional responses influenced perception and experiences of services.
Good practice examples were few and included discussion of specific health conditions and ethnicity e.g. diabetes, thalassemia or the cultural significance of infertility. Other positive practice examples included victim-focused interpreting (see below).
Stereotypes and the culturalisation of DVA
Common stereotypes within DHRs illustrate the uncritical acceptance of the normalisation and culturalisation of DVA in minoritised communities. Several tropes were utilised by a range of services which hampered effective intervention. For example, DHR156 makes no mention of the victim's cultural background as she was a successful businesswoman. Similarly, women who appeared ‘strong’, intelligent or cheerful were not recognised as victims (DHR213, DHR206, DHR203) even when requesting help. Minoritised women who were perceived as ‘westernised’ were expected by agencies to disclose abuse as they were constructed as agentic and unencumbered by supposed cultural norms preventing disclosure (DHR152).
The cultural dimensions surrounding shame, honour and gender can complicate help-seeking. Families were aware of DVA in under half (46%, n = 44) of cases, with friends in under a third (32%, n = 30). In DHR030, the victim's sister ‘was very clear that no woman in her culture would disclose DVA to a man, whether a GP, or a member of the family…[or] via an interpreter who was male’ (DHR030: 20). She further discusses shame for abused women, replicated in other DHRs: ‘in my culture it is not acceptable for a woman to report violence’ (DHR60: 25) or that such matters are ‘private’: ‘culturally it is unacceptable to talk about problems outside of the family’ (DHR62: 21). Whilst cultural factors influence help-seeking, another DHR concludes ‘It is equally important that culture does not become the only rationale for the difficulties that face victims when disclosing and talking about domestic abuse…’ (DHR291: 33).
Where DHRs mention issues of ‘race’ and culture, several typify an uncritical acceptance of supposed cultural norms related to DVA. DHR041 concerns an African-Caribbean couple where some agencies displayed an acceptance of normalised violence within these communities: …[ service] recorded in their files a statement from [victim] that in [Caribbean country], domestic violence was very common and something she almost expected. However, it was not recorded if or how this was challenged (DHR041: p40). There seems to be some indication in professionals’ notes…[that], domestic violence was tolerated in the family…it remains unclear why this was not explored or challenged by a variety of professionals (DHR073: 25, Executive Summary). [DVA] is seen as an acceptable part of Iranian Kurdish culture. It is a male dominated society… If the occasion arises where a woman does complain it is seen that she brings shame upon the family.
Interpreters and communication
Where required, professional interpreters were used inconsistently or not at all, both within and between services, regardless of organisational policy. Whilst possibly a pragmatic solution in diverse or remote areas, telephone interpreting services were often viewed as unsuitable by professionals. For example, in DHR135 the GP felt that it interfered with the doctor-patient relationship despite noting that the perpetrator constantly spoke over the GP. In DHR120, evidence indicated that interpreters prevented open discussion about sensitive issues and that intended emphasis might have been lost.
DHR082 records 20 face-to-face NHS contacts with the victim and perpetrator, but interpreters were used on only four occasions. In DHR135, the only contact between the victim and the police occurred when the perpetrator claimed he had been abused. Police issued a harassment warning to the victim, using her son as interpreter. Simultaneously, interviews with the perpetrator (the alleged DVA victim) were conducted using a professional interpreter.
Friends and relatives (even children and victims’ in-laws) were used to interpret for victims, by police, housing and medical professionals. A shortage of interpreting services or professionals’ naivety also led to perpetrators interpreting for their victims, including during mental health and gynaecological appointments despite noted relationship difficulties. This was due to perpetrator resistance to external support or a lack of guidance and/or poor professional judgement. For example, in DHR114 the perpetrator interpreted for his mother-in-law (the victim) despite not speaking the same language. Where victims’ views were not obtained directly, vulnerabilities went unrecognised, and victims’ voices were absent from risk assessments. Occasionally, the victim was asked to interpret for the perpetrator (e.g. DHR149), which overlooks the relationship dynamics potentially resulting in poor risk assessment. DHR148 clearly states that an inability to communicate was a significant factor in accessing support prior to the homicide. A shortage of female interpreters was evident. In DHR063 the victim was required to give detailed explanations of a serious sexual assault to a male GP, a male police officer and subsequently examined by a male forensic medical examiner without interpreter assistance. It is unsurprising that she chose not to support further action or seek further help.
A small number of DHRs highlight good practice and the benefits to accessibility where staff or interpreters spoke the same language as the victim. For example, DHR088 notes that appropriate services were used, including the deployment of a Polish speaking Police Community Support Officer. In DHR125, despite protests from the perpetrator, police used an interpreter, and a social worker who spoke their language was assigned to the victim.
DHR recommendations
Over 1648 recommendations were made across the 95 DHRs. This is an underestimate as some recommendations were not publicly available, individual agency recommendations were not detailed, relevant actions were already underway linked to a previous DHR in the same local authority, or they had been completed prior to publication and therefore excluded. Some DHRs identified equalities issues but failed to include adequate connecting recommendations. Recommendations were targeted towards several organisations, primarily physical health services and the criminal justice sector. Commonly, recommendations referred to developing DVA organisational policy, multi-agency working, risk assessment and training. Importantly, for this sample, 53% of DHRs (n = 50) had recommendations specifically related to minoritisation, although in some cases, issues of ethnicity/culture were appendages to the primary focus of recommendations e.g. DVA training or assessment. Additionally, generic recommendations such as ‘improved record keeping or recording systems’, often contained a further element such as ensuring databases reflect diverse needs. Likewise, enhanced ‘risk assessment’ features the importance of identifying risks such as forced marriage or honour-based violence.
Broader, often vague, recommendations encompassed ‘cultural sensitivity’ or ‘cultural awareness’. More specific training recommendations advocated for recognition concerning the role of race, religion, culture and ethnicity regarding barriers to help-seeking; dispelling assumptions about cultural acceptance of DVA; immigration issues ‘No Recourse to Public Funds’; honour-based violence; and the use of interpreters. It was rare to find monitoring and audit of training implementation and attendance (c.f. DHR032).
Recommendations for awareness-raising activities encompassed multi-lingual advertising, and information campaigns aimed at minoritised DVA victims, their families and wider networks including workplaces; education establishments; health services; community and faith venues; and online spaces. Community engagement events (including women-only consultations) to build trust and confidence in services were suggested to increase DVA knowledge via community-based training and develop appropriate interventions and referral pathways. DHR158 called such activities a ‘community empowerment approach’. Explanations of safeguarding, legal rights, health systems, and reporting processes were also suggested. DHR131 suggested that improving such knowledge could occur at the earliest opportunity – on UK entry.
Recommendations regarding independent professional interpreters were not made in all applicable DHRs. Recommendations included identifying and documenting preferred language, English language proficiency and using female interpreters for DVA victims. Equipping professionals to use trained interpreters with an understanding of DVA also featured. DHR244 made a national recommendation to develop DVA helplines in a range of languages to facilitate DVA disclosure and service access. Recommendations to address gaps in DVA specialist provision were rare but more likely to be made in London boroughs. For example, two boroughs recommended that the Community Safety Partnership work with other commissioning bodies to ensure sufficient specialist provision (DHR145, DHR209). Scoping exercises into the availability of, and clarity about, routes to specialist DVA provision were endorsed. Elsewhere, an absence of similar recommendations might reflect the DVA service landscape which has seen major cuts especially in specialist Minoritised DVA provision (Barter et al., 2018).
Some recommendations for the Home Office or UK Border Agency focused on immigration. This included awareness-raising activities for newly-arrived migrants noted earlier but also endorsed reviews of criteria, thresholds and associated guidance around foreign nationals, uncertain immigration status and illegal immigrants (e.g. DHR157, DHR111). Suggestions were made for improved risk assessments and increased police checks as well as exit checks. Some of these recommendations are problematic as they are likely to silence victims further, especially where both partners are migrants. Others appeared unrealistic: ‘Home Office consider advising that each Community Safety Partnership consider inviting the Immigration Service as associate members to local boards’ (DHR218: 21).
Good DHR practice involved exploration of key issues with matching recommendations, often connected to panel expertise. Some DHRs were particularly thorough and endorsed an interconnected, holistic suite of recommendations, placing responsibility onto services to ensure adequate provision for minoritised communities. For example, DHR234 made several pertinent recommendations including: quality assurance; promotion of anti-racist, culturally sensitive responses; addressing barriers and gaps in services; and improvement of referral information to shape service delivery. Such a comprehensive approach was rare within DHRs, indicating there is much to learn.
Discussion
The twinning of normalised absence/pathologized presence is evident across the findings. Discussion of minoritisation is largely absent, evidenced in the overlooking of, misattribution and minimal attention paid to minoritisation in Individual Management Reviews and in the DHRs themselves. The lack of recording of victims or perpetrators’ cultural/ethnic heritage means that services fail to consider whether or how services may need to adapt. This portrays an indifference or a lack of understanding of how social positioning impacts both victims’ help-seeking and service responses. The DVA literature is unequivocal that there are additional and intersecting barriers for DVA victim-survivors from minoritised communities. These include insecure immigration status, community pressures, language issues and unhelpful staff attitudes (DAC, 2021; Femi-Ajao et al., 2020; Montique, 2019; Sundari, 2008). Professional reluctance to intervene in ‘cultural matters’ for fear of being labelled culturally insensitive also features in the literature (Chantler et al., 2021).
Pathologized presence is most evident in the culturalisation of DVA in minoritised communities. There is wide disparity in the extent to which the DHR panels challenge the narratives provided by agencies. In some reports, missed opportunities regarding equality matters are downplayed or the narrative provided is accepted at face value. DHR good practice challenges such Individual Management Reviews and makes holistic recommendations to respond appropriately to minoritised DVA victims.
Whilst cultural barriers such as shame/honour and a lack of knowledge of service entitlement impeded minoritised victims help-seeking, their structural locations are a key factor – exemplified by the culturalisation of DVA. The construction of DVA as normalised within minoritised communities in DHRs (regardless of whether South Asian, African-Caribbean, Middle-Eastern or Eastern European) suggests that DVA in majority communities (in this case, White British) is assumed to be an individual act of transgression rather than a cultural issue (Chantler and Gangoli, 2011). This portrayal minimises the misogyny, patriarchy and sex discrimination, that are part of the structural arrangements of White British society and recognised globally as both a cause and consequence of DVA (UNODC, 2019).
Further, the culturalisation of DVA in minoritised communities works to embolden DVA perpetrators as they know that services will not act due to such constructions. This unholy alliance between perpetrators and services has serious and detrimental impacts for victims, potentially culminating in domestic homicide. This construction also works to ‘other’ minoritised communities and fuels racist stereotypes. Services need to turn the spotlight onto themselves to understand how organisational cultures of DVA normalisation and stereotypes impact on risk assessment and appropriate intervention (Burman et al., 2004; Montique, 2019).
Additionally, the inappropriate use of interpreters reported in DHRs is problematic and has been repeatedly highlighted (Chand, 2005; Chantler et al., 2020; Montique, 2019; Sawrikar, 2015). Pollock (2021) argues that service users prefer informal interpreters who may have greater knowledge of an individual's life and context. She suggests that individuals should be empowered to choose who provides language support to redress power imbalances between service users and professionals. Pollock (2021) proposes a move towards engagement and training with willing relatives and friends.
Despite their theoretical suitability it might be inappropriate for friends or relatives to provide interpreting support in DVA contexts (unless this is the victim's choice) owing to safeguarding risks. Some DHRs show that perpetrators, children, in-laws and friends are used by statutory services to interpret. This ignores power imbalances inherent in DVA and places either the child and/or the victim at greater risk, with professionals only likely to be told what the perpetrator wants, thus further silencing the victim's voice and impeding accurate risk assessments. Overcoming language and communication difficulties is critical in facilitating professional relationships as well as ensuring that victims are informed of their options and rights. Whilst some DHRs recognised this and made appropriate recommendations for professional interpreters with an understanding of DVA, others failed to identify the significance of making such recommendations.
A key factor in minoritised victims’ engagement with services rests on trust. Some DHRs illustrate that the lack of trust and fear of mainstream services is an impediment to help-seeking. Importantly, the wider socio-political environment is crucial. Griffiths and Yeo (2021) provide a detailed analysis of the UK's ‘hostile environment’ to migrants and discusses ‘deputising immigration control’ or what Yuval-Davis et al. (2019) term ‘everyday bordering’. These concepts refer to the myriad ways in which third parties including local authorities, health services, police, landlords, banks and employers are mandated to check immigration status to ascertain rights to goods and services, often exceeding what is required by law and legitimising institutional discrimination. Such ‘bordering’ exacerbates existing fears potentially deterring help-seeking. Whilst the intention of such policies is to deter ‘illegal’ migrants from entering and remaining in the UK, the Windrush scandal has demonstrated the ‘spillage’ of the hostile environment from unsettled to minoritised people generally, causing fear, uncertainty, and a distrust of the nation-state (Griffiths and Yeo, 2021).
Further, the hostile environment creates suspicion within the wider community and potentially impacts on service providers’ attitudes. This is particularly visible for DVA victims with ‘No Recourse to Public Funds’, although our sample only had a few victims in this situation. Importantly, these victims mostly did not contact services for many of the reasons already discussed. Perpetrators’ manipulation of victims’ immigration status together with ‘deputising’ makes help-seeking almost impossible. The Domestic Abuse Commissioner's Office (DAC, 2021) has introduced the term, ‘immigration abuse’ to reflect perpetrator manipulation of insecure status. This term also applies to the nation-state for creating immigration rules which permit such manipulation to occur. DAC (2021) argues for a firewall between public services and the UK Border Agency to encourage help-seeking and remove deportation fears. DHR recommendations regarding immigration should therefore be avoided given the wider ramifications of the hostile environment.
The current DHR requirements regarding equality (based on the Equality Act 2010) appear to generate a tick-box, tokenistic approach rather than a deeper engagement with potentially inequitable and high-risk service provision. In some DHRs this is justified due to a lack of resources to respond to minoritised victims. This requires challenging as it removes freedom from GBV as a universal human right during austerity and assumes that during economic hardship the needs of minoritised victims can be overlooked. However, as taxpayers at local and national levels, this rationale is difficult to uphold. It implies that while minoritised status does not bar them from paying taxes, it does bar them from services.
Key to this are the funding cuts to statutory sector services and the DVA specialist sector (Barter et al., 2018), but the minoritised DVA sector has been particularly impacted (APPG, 2015; Hall et al., 2017). In turn, there is growing pressure to secure ‘by and for’ services (Imkaan, 2018; 2020) defined as ‘specialist services that are designed and delivered by and for the users and communities they aim to serve’ (NAVCA, 2012). ‘By and for’ can suggest that only these organisations are able to provide appropriate support. Indeed, they have been at the forefront of championing, campaigning and supporting minoritised women on issues such as ‘No Recourse to Public Funds’, honour-based violence and FGM, with a crucial role in providing accessible and responsive support. Where ‘by and for’ expertise was sought on DHR panels, recommendations were often more robust and tangible. The decimation of this sector and its expertise is of serious concern. However, not all minoritised victims want to access ‘by and for’ services and so the wider DVA sector needs to be cognisant of minoritised women's needs and be equipped to respond appropriately. Some DHRs without ‘by and for’ expertise had gone to great lengths to understand the relevant issues demonstrating the possibilities for all agencies to engage with minoritisation. Further, our study illustrates that most victims and perpetrators were in contact with numerous statutory services, so the ability to respond adequately to minoritised victims extends beyond the specialist DVA sector.
Conclusion
Urgent action is required to better respond to Black and minoritised victims of DVA, both by DHR panels and statutory sector agencies.
DHR guidance (Home Office, 2016) directs panels to consider equality and diversity issues, but this is frequently treated in a cursory manner in Individual Management Reviews and DHRs. Positive DHR practice included the challenging of service narratives regarding minoritisation and made holistic recommendations to develop practice, especially noticeable where Black and minoritised specialist support was sought. DHR guidance makes clear that the panel requires relevant expertise (Home Office, 2016) and as illustrated, this should include the ‘by and for’ sector to generate meaningful dialogue and recommendations. DHR authors should take a much more proactive, questioning stance in understanding how issues of minoritisation, ‘No Recourse to Public Funds’, potential racism and culture feature in DHRs and be cognisant of the ripple effect of the ‘hostile environment’. Where DHRs are unquestioning about the normalisation of DVA in minoritised communities there is a danger of colluding with patriarchal systems in minoritised communities and making victims invisible. Recommendations relating to training for cultural sensitivity should be treated cautiously unless situated within a broader framework of minoritisation and racialisation. Training for Chairs should include an understanding of minoritisation and the Home Office DHR Quality Assurance process should be cognisant of this. The Equalities section in the DHR guidance needs strengthening to encourage a deeper engagement with minoritisation by panels.
Services should ensure that ethnicity/cultural data is routinely taken and used to identify how agencies have adapted service provision where required. Professionally trained female interpreters versed in DVA should be used, as not doing so curtails victims’ rights, increases risk, and deters future help-seeking. The normalisation of violence works to leave minoritised women experiencing DVA unprotected – services should address abuse and be prepared to challenge supposed ‘cultural’ norms. Analysis of DHR recommendations also indicates that public services need to build trust within minoritised communities to increase awareness of and responsiveness to DVA. Women-only spaces are important for informing victims about their rights and available services.
At a wider policy level, the continuing hostile environment is detrimental to minoritised women regardless of whether they are recently arrived or settled in the UK for generations. A change in policy direction to a ‘friendly’ environment would be helpful and may work to increase help-seeking by minoritised DVA victims, increase trust and acceptability of services. One very public way of doing so would be to ratify the Istanbul Convention.
Footnotes
Acknowledgements
The support of the Economic and Social Research Council (ESRC) is gratefully acknowledged. Grant Reference: ES/S005471/2.
Author's Note
Megan Ward is also affiliated at London School of Economics, UK.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Economic and Social Research Council, (grant number ES/S005471/2).
Author biographies
![]() .
.