
Abstract
Discharge to Assess (D2A) models of care have been developed to expedite the process of discharging hospital patients as soon as they are medically fit to leave, thereby improving the efficiency and effectiveness of the healthcare system. This article focuses on the implementation of a D2A model in Kent, England, which formed a case study for a European research programme of improvements in integrated care for older people. It uses the Critical Systems Heuristics framework to examine the implementation process and focuses in particular on why this improvement project proved to be so difficult to implement and why the anticipated outcomes were so elusive. The analysis highlights the value in using critical systems thinking to better evaluate integrated care initiatives, in particular by identifying more explicitly different stakeholder perspectives and power relationships within the system and its decision environment.
Keywords
Introduction
Delayed discharges of older inpatients occur in most countries and have significant associated costs for healthcare systems and for patients (Landeiro et al., 2019; Rojas-García et al., 2018). Transfers of care from hospitals can be complicated and frustrating, especially for patients with both health and social care needs (CQC, 2019; NAO, 2016; Oliver, 2016). The coordination and timing of assessments and decisions about post-discharge care can cause serious delays (Werner et al., 2019). In the UK, a Discharge to Assess (D2A) model was developed whereby patients who are clinically optimised and do not require an acute hospital bed, but may still require care services, are provided with short term, funded support to be discharged to their own home (where appropriate) or another community setting (NHSE et al., 2016).
Its fundamental principle is to conduct full health and social care assessments after, rather than before discharge. Core components comprise: comprehensive assessments of continuing health and social care needs, conducted when patients reach home; a single point of access to coordinate discharge; built-in links with primary care; a community reablement and rehabilitation service; and increased opportunities for multi-disciplinary communication and decision making (Monitor, 2015). Reablement services generally focus on optimising independent functioning by helping people accommodate their illness or disability (SCIE, 2013). Local examples of D2A have been found to reduce delays, increase the number of patients discharged on (or the day after) their day of admission, and avert significant long-term care costs (DHSC, 2020).
Background
Hospital discharge in England involves the safe and timely transfer of patients between settings and services based on different organisational principles; it requires coordination between different branches of the NHS, local authorities, private providers and the voluntary sector. Consequently, discharge requires structural, financial and professional boundaries to be spanned (Gilburt, 2016). For example, the NHS in England is organisationally fragmented between and within hospital, primary care, community health and regulatory bodies, but is accountable to Parliament and the Secretary of State for Health and Social Care. It has a powerful national identity and strong public allegiance. By contrast, adult social care (ASC) is the responsibility of 151 elected local authorities accountable both to their electors and to central government. It enjoys considerably less status than the NHS and is often perceived to be its unequal partner (Wistow, 2001).
Structural, cultural and status differentials, all directly influenced by funding issues, have consistently presented challenges to collaborative working (Erens et al., 2016). The NHS is 99% tax funded with the remaining 1% from user charges. ASC is funded both by taxation (national and local) and by substantial, means-tested charges. A very large volume of unpaid, informal care is provided by families and friends (Lu et al., 2021). Funding allocations have consistently favoured acute hospitals over primary care and community health. Likewise, the NHS has consistently secured more resources than ASC (Luchinskaya et al., 2017); local authority spending on ASC has fallen significantly since 2009/10, despite a growing older population. Whilst these cuts enabled some financial protection of the NHS, decision-makers failed to appreciate the dynamic interrelationships between social care provision and the use of NHS services; the availability of ASC has been demonstrated to be an important determinant of the use of NHS services (Crawford et al., 2018).
The boundaries between a ‘free’ NHS and means-tested social care are not fixed and are currently determined with reference to policy on Continuing Health Care, which defines eligibility for long term care in narrow, predominantly medical terms (DH, 2018). From the mid-1970s, the NHS began to withdraw funding from continuing care by exploiting a loophole in social security regulations, and transferring its responsibilities to means-tested independent sector providers, without prior Parliamentary approval or public debate (House of Commons, 1995; Wistow, 1995).
A discharge case study: Swale Home First
The Swale Home First D2A service in Kent, England, was a case study in the SUSTAIN integrated care improvement programme, a European Horizon 2020 project (2015–2019) designed to support the continuing improvement of integrated services for older people (De Bruin et al., 2018). Swale had already started to identify and address social care-related barriers to hospital discharge and joined SUSTAIN to make further improvements in care integration. The local project was initiated through two stakeholder workshops led by a steering group of representatives from:
hospital (discharge planners), social care (discharge planners and reablement service providers), primary/community care (rapid response service providers), the Clinical Commissioning Group (commissioners of healthcare services), the Local Authority (commissioners/providers of adult social care), third sector organisations (AgeUK), and Healthwatch (an independent champion for people using services).
SUSTAIN researchers supported the steering group to design and implement an improvement plan from autumn 2016 to spring 2018, and to evaluate its process and outcomes.
The plan’s overall aim was to shift hospital-based activities into home settings by:
Identifying older patients whose discharge might be safely expedited through more efficient transfer processes. Providing a comprehensive, ‘context-specific’ assessment of health and social care needs on those patients’ return home. Ensuring the immediate delivery of coordinated, person-centred ‘wraparound’ support to enable them to recuperate, regain and maintain their independence at home.
The planned improvements and implementation requirements are shown in Figure 1.
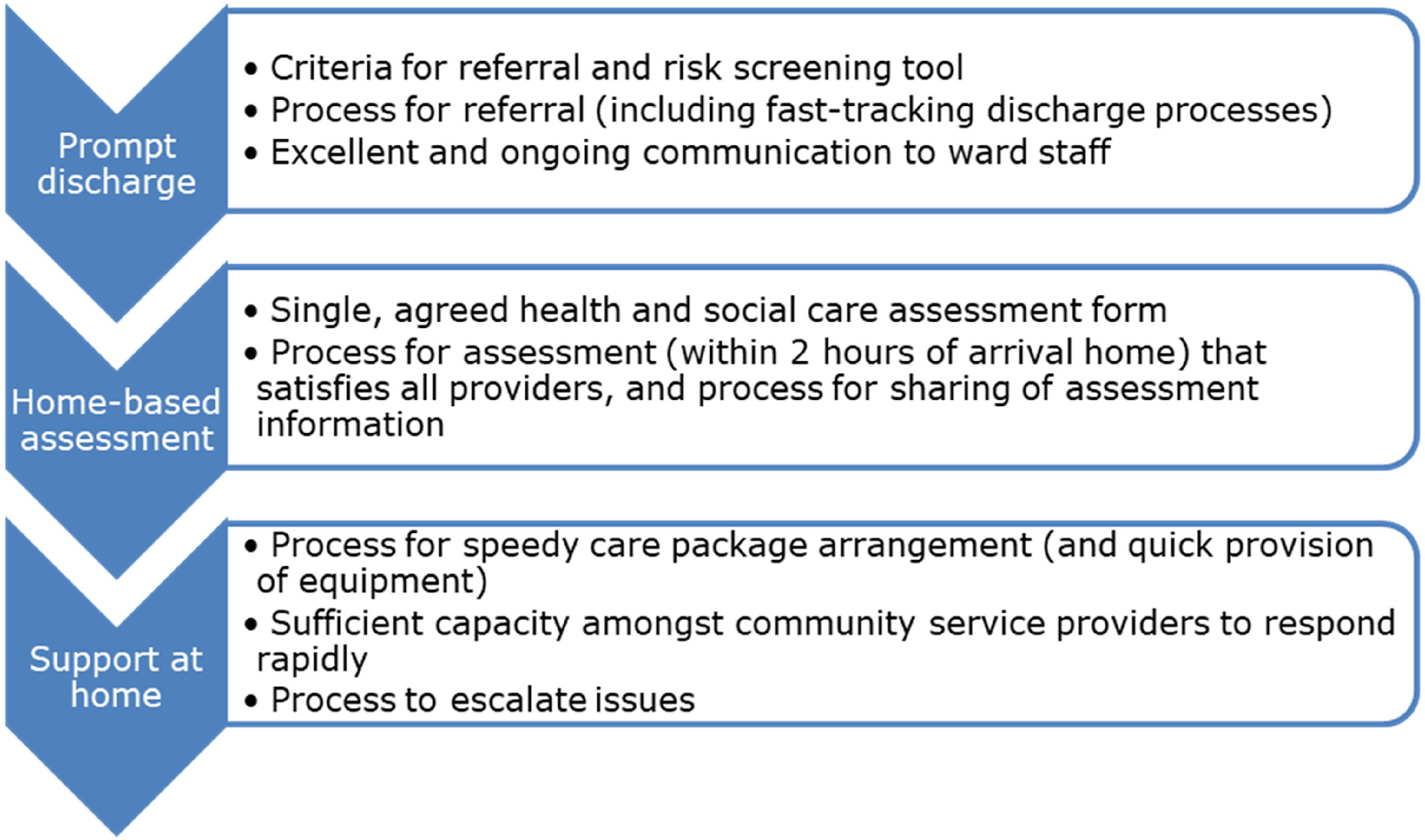
Planned improvements and requirements for implementation.
Similar D2A models had been successfully implemented elsewhere, including within the same hospital, for patients returning home to Swale’s neighbouring district. Yet, the SUSTAIN evaluation of Swale Home First produced unexpected results, reporting potential reductions in efficiency and reported user experiences but few compensating gains. The evaluators initially sought to understand how the improvement project worked (or didn’t) in practice through the implementation science methodology briefly summarised in the next section. But to more fully understand the intricacies of implementation and causes of the outcomes observed, we further analysed the evaluation’s findings using the Critical Systems Heuristics framework (Ulrich and Reynolds, 2010) to take a ‘a deeper dive into the “black box” of complexities that integrated care initiatives represent’ (Goodwin, 2019: 1).
Methods
To monitor the improvement plan’s development and implementation, SUSTAIN researchers adopted a case study design (Yin, 2009), embedded within an implementation science approach (Glasgow et al., 2012). The latter helped ensure that the improvement plan was evidence-based; the evaluation used practical measures for rapid feedback and was based on a partnership approach highlighting local contextual factors. The case study design enabled a detailed and intensive examination of the project’s operation, using a set of qualitative and quantitative data collection tools to gather data from different sources (see Billings et al., 2018, 2020). The lead author here was a participant observer in the steering group which met fifteen times; she conducted eleven interviews with service users (four as dyad interviews with carers), ten with professionals and managers, and kept detailed field notes throughout. An analytical process that triangulated multiple data sources enabled an initial explanatory model to be built about the implementation of the plan (see Billings et al., 2020). Ethics approval for this project was granted by the Health Research Authority Social Care Research Ethics Committee (ref 16/IEC08/0045).
For this article, the authors conducted a retrospective systemic analysis of all the data available using the Critical Systems Heuristics (CSH) framework, developed to support reflective professional practice (Ulrich, 2000). A core methodological underpinning of CSH is that of ‘boundary judgements’: those prior (implicit) judgements that underpin all problem definitions, proposals for improvement and evaluations of outcomes. In CSH terms, these judgements define the boundaries of the system (Ulrich and Reynolds, 2010). In using CSH, the authors sought to understand the interrelationships between elements of our system of interest by surfacing stakeholders’ different perspectives and exploring power relations within it (Reynolds and Holwell, 2010).
The CSH framework identifies four dimensions of potential conflict that relate to
measures of success; the decision environment in which the system of interest is operating; the types of expertise drawn in; and the underpinning rationale and political space in which it operates.
It prompts questions for each dimension concerning:
stakeholders; what’s at stake; and stakeholding concerns.
Table 1 presents the twelve questions produced by this framework and used here.
The twelve CSH questions guiding analysis (numbered according to the order in which they were addressed adapted from Reynolds, 2007).
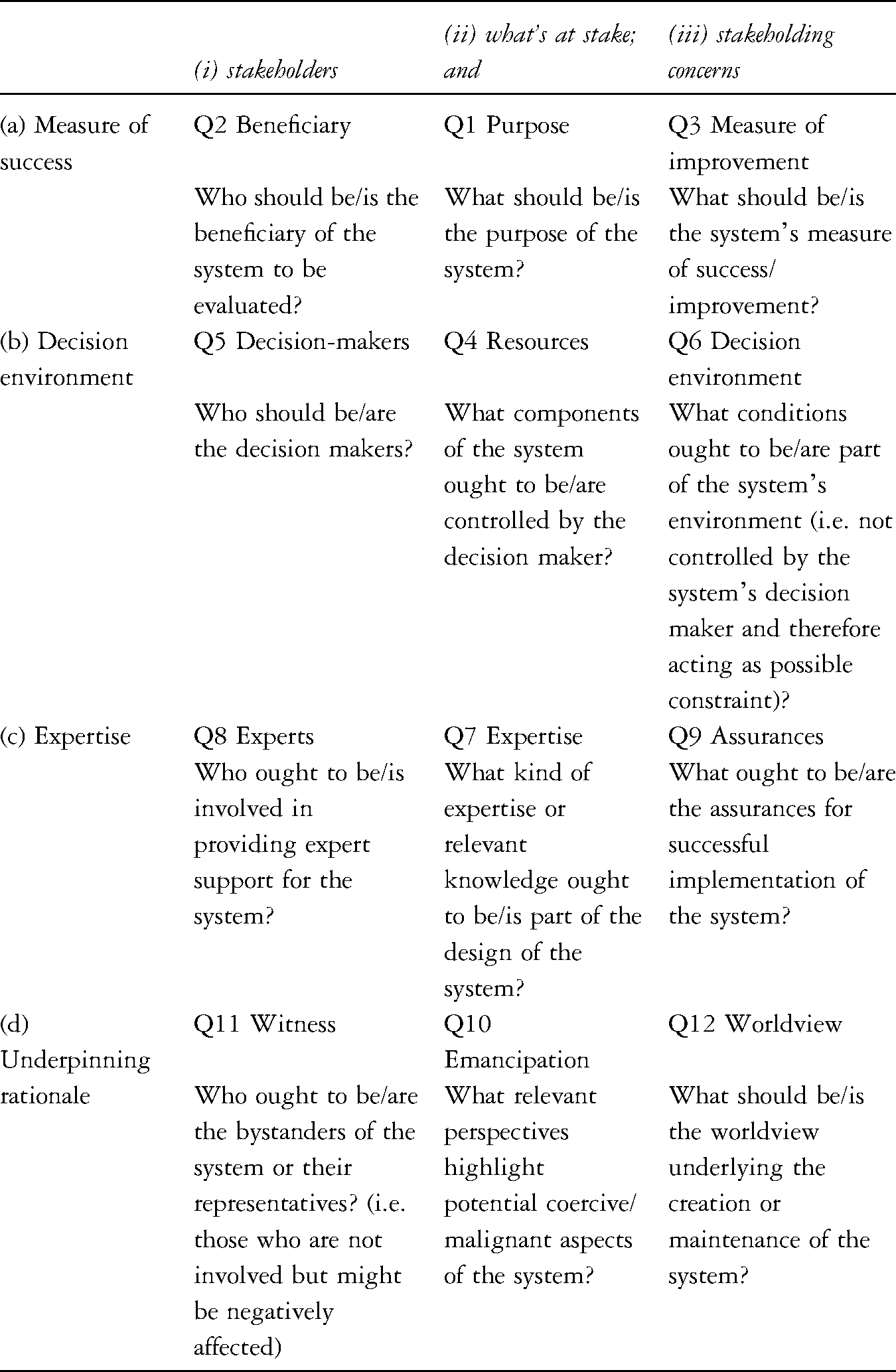
According to CSH, by examining these dimensions of potential conflict, we can make explicit:
the values and motivations built into people’s views of situations and efforts to ‘improve’ them; the power structures influencing what is considered a ‘problem’ and what may be done about it; the knowledge base defining what counts as relevant ‘information’, including experience and skills; the moral basis on which we expect ‘third parties’ (i.e. stakeholders not involved but in some way concerned) to accept the consequences of what is done, or not done.
Findings
The findings of the initial analysis are published elsewhere (Billings et al., 2018). They highlighted some successful aspects of the improvement project, facilitated by the persistence, commitment and willingness of steering group members to pursue improvements despite their many challenges. The steering group met frequently, shared information, identified problems and sought to develop potential solutions. Interviews with professionals described how the community health and social care teams, for example, were developing interpersonal trust and improving knowledge of each other’s services.
However, the evaluation found that the planned improvements (see Figure 1) were largely unrealised, and some negative outcomes emerged. Discharge was sometimes delayed by confusion amongst staff about the suitability or otherwise of particular patients for the service and by the continuation of multiple assessments within the hospital. Service users sometimes felt unaware of what was happening or why. They often arrived home too late or too tired to have an appropriate assessment. The transition from hospital to home could still be disjointed, with discharged patients waiting at home alone for assessments and services that did not materialise. Support available post-discharge was limited and largely consisted of social care reablement support. Providers of care in home settings were still poorly coordinated, often working in separate teams from multiple different locations and unable to offer sufficient wraparound support. Overall, the data did not demonstrate that D2A provided the anticipated benefits.
The evaluation highlighted some familiar implementation barriers, including aspects of leadership, organisational culture, information technology, professional involvement and resource availability. However, the disappointing nature of the results demanded further explanation. The monitoring and evaluation activities embedded within the improvement process provided an opportunity to explain how and why these findings emerged in the particular context of this case study. The subsequent analysis, employing CSH, is described below.
Measures of success
Q1 and Q2: Purpose and beneficiary
Initial stakeholder interviews surfaced multiple purposes for the improvement project, driven by concerns related to patient outcomes, person-centredness, care co-ordination, delayed discharges and the cost of care placements, e.g.: I had a feeling that people were just being parked in the community hospitals and the outcomes for them were extremely poor … I was concerned that we were just picking them up and putting them into permanent placements … I was becoming quite concerned about the cost … but more importantly about the poor outcomes for people themselves, older people (#9, Social Care Manager).
Interviewee 9 also discussed ‘winter pressures money’: part of the Government investment in adult social care to help reduce pressures on the NHS (Forder et al., 2018). This placed additional pressure on freeing up beds to improve patient flow in hospitals. Other stakeholders talked about the purpose behind incorporating an enhanced ‘wraparound’ service into the improvement plan, ‘so that we can really start discharging more complex patients back to their own home safely’ (#2, Healthcare Provider).
Multiple, co-existing purposes therefore include to:
improve health and social care outcomes for older people; improve decision-making and co-ordination for older people being discharged from hospital; reduce the number of new social care placements in care homes (and their associated costs); free up beds in hospitals; reduce delayed transfers of care; improve the flow of patients from the acute hospital.
These purposes revealed different emphases on securing benefits for service users on the one hand, and for the NHS and the wider health and social care system on the other. The interviews and project plans highlighted some potential conflicts between different perspectives. In practice, two quite different purposes were at play:
To improve the transfer of patients with health and social care needs from hospital to home, by implementing a D2A service, in order to reduce pressures on acute services and admissions to care homes. To improve the provision of person-centred, coordinated care for older people as they transfer from hospital to home, by implementing a D2A service, in order to maximise the health, wellbeing and independence of older people.
The first perspective privileged demand management by earlier discharge supported by timely and effective transfer processes. Benefits were conceptualised from the perspective of those involved in planning and providing services. This was close to how we observed the D2A model working in practice. The second focused on the quality of care provided throughout transfer (from the service-user perspective), and the longer-term goal of maximising health and wellbeing at home. This was more consistent with the evidence-based principles for D2A models in national guidelines (NHSE et al., 2016), with their emphasis on meeting people’s needs holistically rather than transferring resource pressures across organisational boundaries.
Although improved health outcomes might emerge from implementing D2A, they were not inevitable. The study showed that inter-dependencies between improved service efficiencies and user experiences were poorly understood and inadequately explored. As implementation challenges mounted, an interviewee noted ‘so many changes to what the focus has been’ (#5, Social Care Manager). The intended beneficiaries (originally more complex discharges requiring additional health service support in the patient’s home) implicitly became a narrower group of patients who could be discharged expeditiously while also requiring very little or no ongoing home care, as these interviewees suggest: Primarily … it’s to enable them to be discharged more quickly through the hospital process, so to avoid any delays on the hospital side (#5, Social Care Manager);
So we’re reducing bed days, bed days is one of our drivers, so we’re reducing cost, but the benefit for the patient is getting them home (#20, Healthcare Commissioner).
The discharge of more complex users through the D2A service was dismissed as ‘something that couldn’t be done because of insufficient capacity within health services’ (Steering Group meeting notes, August 2016). As implementation evolved, the dilution of the D2A model’s overall purpose was a fundamental limitation on the system’s delivery of improved user outcomes.
Q3: Measure of improvement
The two system purposes imply different success measures. Inclusion in the study required acceptance of SUSTAIN’s improvement measures associated with person-centredness, safety, efficiency and prevention (de Bruin et al., 2018). However, throughout implementation, the study observed strong pulls towards practice in which speed of discharge and sign-off was the overarching measure of success. This measure did not preclude perceived benefits to service users: based on the numbers of clients that leave our [reablement] service very, very quickly within the first week … I would say a good 50% of [Home First users] are actually getting an improved service, they’re getting home quicker (#5, Social Care Manager).
The number of referrals to Swale Home First was reported daily to senior management. However, it was largely assumed that (a) these referrals were appropriate and would be accepted, (b) discharge through Home First would be quicker and more efficient than otherwise, and (c) discharge through Home First would be a positive experience for patients and service providers.
The key factor that diluted the model’s focus was its failure to establish a holistic ‘wraparound’ service for newly discharged service users with ongoing health and social care needs due to gaps in community health services, non-availability of investment to boost capacity, and weak relationships with the voluntary sector. Simultaneously, a higher-level strategy group was pushing the project to get on and implement something to reduce discharge delays as soon as possible. These factors combined as implementation progressed to narrow down improvement measures to ‘delayed discharge’ targets at the expense of patient-centred measures.
The decision environment
Q4: Resources
Despite the challenges, the steering group remained committed to its improvement plan. Members improved communication and collaboration between those involved in service delivery, and introduced a new assessment form which reduced duplications in service-user assessments – all of which helped to improve efficiency. However, they were unable to control a number of important conditions of success, such as capacity amongst community staff to provide care and support to people after early discharge, and the trust of ward staff that patient needs could be met safely and effectively at home. The steering group formally recorded: ‘it is not possible to take implementation forward without some input of resources. … the conclusion that this cannot go forward without some resource needs to be escalated.’ (Meeting notes, November 2016). However, the funders’ representatives were unable to fill resource gaps due to its overall financial deficit; the phrase ‘there is no money’ became a repeated mantra.
Commitment to the goal of improving integration between health and social care was crucial. However, while members of the steering group freely contributed their knowledge, time, expertise and experience, they were unable to secure tangible resources. Shortages of community staff and lack of investment from NHS partners were issues that simmered throughout, as this research note illustrates: ‘There was a clear sense of injustice aired here, with the feeling that social care had done all the offering up of resources, where health had done none’ (Steering Group, November 2016). Meanwhile, acute hospital staff blamed a lack of capacity in the ‘enablement at home’ service: ‘the ward’s being told there’s no capacity, just not to refer into [Home First]’ (#17, Acute Hospital professional). Some central government support later filtered through to social care, specifically for reducing delayed discharges. It bolstered the project’s capacity, but the spending conditions reinforced reducing delayed discharges as the system’s principal purpose.
Q5: Decision-makers
Representatives from most of the key organisations (except AgeUK) consistently attended the steering group. However, staff turnover, exacerbated by the re-contracting of community health services, meant individual attendances lacked continuity. Most attendees were low- and middle-level managers, though more senior local authority representatives sometimes attended. Hospital staff were rather marginal since no-one represented its senior management and apologies were frequently given. Whilst a Healthwatch representative in principle provided patient representation, there were no direct user/carer or advocacy voices to provide independent challenge.
Early in the project, the steering group attempted to identify a single NHS leader, since it was felt that ‘similar models across the country are health-led’ (Meeting notes, Nov 2016). Social care representatives felt strongly that local NHS partners needed to ‘step up’ and take the lead because ‘we cannot be … responsible for health’ (Meeting notes, Nov 2016). Health representatives’ claimed workload pressures stopped them accepting the lead role. Consequently, responsibility was shared through a ‘triangle model’ consisting of a social care manager, community health services manager and NHS commissioning manager. Thus, the project lacked a single advocate with the authority to resolve conflict and ensure the improvement plan’s delivery.
Q6: Decision environment
The project was facilitated by a theoretically supportive policy environment, as this local authority manager explained: We couldn’t be in a better position policy-wise. It’s completely written in our business plan … It’s taken from national directives … so there’s no problem with policy and we’ve got a lot of support to bring about that change in terms of the strategic direction that we’re going in. (#9, Social Care Manager)
However, implementation was hindered by the many staff vacancies and long-standing recruitment difficulties, together with the lack of funding. Wanting a single point of leadership, the steering group lacked authority to shift resources across and between health and social care organisations to fund the best mix of services. Organisations like AgeUK were unable to boost capacity due to historical under investment in voluntary and community resources. As one manager emphasised: ‘if you ask for the voluntary sector to be involved in anything then you’ve got to finance it’ (#16, Social Care Manager).
The types of expertise drawn on
Q7: Expertise
The steering group’s considerable expertise and knowledge about their organisations’ internal systems and norms meant improvement proposals were realistic and grounded. Information sharing gave them ‘more of an understanding of each other’s roles and remits and constraints and how they can work together’ (#20, Healthcare Commissioner). The group discussed how the improvement project might work in theory (from a higher management perspective) and how it might/did work in practice, with senior practitioners ‘feeding back up’ information about ‘the intricate little problems and issues that we’ve had’ (#1, Healthcare Provider).
However, the group’s operational focus meant it lacked the knowledge and authority to successfully navigate or modify key implementation constraints. These capability gaps resulted in frustration: ‘Whilst the atmosphere [in the steering group] was cordial, there seemed a little bit of desperation that things aren’t moving forward, that the situation isn’t changing’ (Reflective notes, May 2017). The third sector was a noticeable gap in the group’s expertise, however, and its potential to enhance informal or social support was not considered. Moreover, group members’ contributions tended to be restricted to their particular experiences, and thus largely to focus on parts of the process rather than the whole. As participants commented: The leadership has been down to the people running the service and that sometimes causes difficulties because we only ever see our own pressures … at times I think possibly we’ve lacked the helicopter view of what would streamline the process (#5, Social Care Manager).
No-one can see the whole picture … our health and social care systems are complicated and they’re very fragmented now, we’ve got too many organisations involved … and it’s very hard for anyone to have a real overview (#19, AgeUK).
Some managers were, however, able to draw on theory-informed knowledge and use ‘evidence of other models or other pilots … evidence of how they were working’ (#20, Healthcare Commissioner).
Q8: Experts
General practitioners (GPs) were missing from the steering group, despite their role as co-ordinators of care at home. Their perspective might have been invaluable in providing greater assurance that assessment and support were available when patients reached home. The absence of lay voices in the group risked decisions being made on untested assumptions about what older service users might want or need. For example, a not uncommon assumption was: ‘For the client I think they get what they want in the sense of they want to be at home, so they get home a lot quicker'(#5, Social Care Manager). The fact that the same source also reported some had ‘returned to hospital unfortunately’, did not lead them to question their previous statement’s validity. We discuss the marginal influence of user and carer voices in The underpinning rationale and political space in which it operates below.
The research team (particularly the first author) contributed directly to the group’s expertise in a number of ways. Early on, their organisational skills helped to plan and organise meetings. Later, they contributed interpersonal skills in dealing with negotiations within and between steering group meetings. They also contributed evaluation expertise, especially about accessing user and carer voices. The resulting data highlighted the gaps that would have existed if lay perspectives had not been recorded, including the potential for unintended consequences.
Q9: Assurances
Assurances of success were based on the assumption that all older service-users without ongoing acute care needs were better off at home. However, this understanding was coloured by a medical/functional viewpoint, rather than a holistic viewpoint that considers the person’s need for social comfort, emotional support and building of confidence in their ability to manage on their own. Even when evidence emerged to the contrary (see The underpinning rationale and political space in which it operates), the assumption went unquestioned.
The improvement project was intended to enable holistic support for recently discharged people, partly through enhanced community health service provision. However, the lack of resources within those services led instead to a heavy reliance on social care reablement services for at-home support. The steering group discussed this situation at length but were unable to give assurances that health care needs would be met within the Home First service. In several meetings, a number of risks were discussed, including the risk that social care staff would be left facing complex difficulties without adequate resources. The lack of GP involvement meant there was little assurance that primary healthcare needs would be met in an efficient and co-ordinated way, and the lack of third-sector involvement similarly provided little assurance that they could support social and emotional needs.
The underpinning rationale and political space in which it operates
Q10: Emancipation
The evaluation found that users often did not experience a well-co-ordinated service; as one interviewee put it: ‘It all seemed as if the right hand doesn’t know what the left hand’s doing’ (User 8). Responsibility for co-ordination of care at home arguably shifted more onto the user since they received very few ‘pop-in’ visits; if they wanted support, they had to know who to contact and be proactive in organising it themselves. It was unclear whether they understood these implications of the D2A model, or had the necessary resources to undertake such tasks.
The efficiency of the service depended on reduced inputs from hospital-based staff such as occupational therapists (OTs). However, the evaluation found that some hospital staff, due to concerns about risk and safety, were reluctant to reduce their input: ‘Before they are discharged, most Home First patients are still being seen by an OT or physio, they’ve had their equipment provided, and have a care package in place’ (Meeting minutes, July 2017).
Whilst patients in general were keen to get home, the evaluation found older people sometimes felt ‘pushed’ out of hospital before they were fully prepared, despite the professional desire to maintain input described above, as these quotes illustrate: there were so many people waiting to come in, they wanted, the way I look at it, wanted to get rid of us to put more in the bed (User 11);
I just thought it was such a short time. To me, it seems like quite a serious operation, and it seemed like I was just being pushed out, basically (User 2).
Once home, the emphasis on self-care and reablement could be empowering, but could sometimes create difficulties, particularly when patients had just returned from hospital. Users without spouses living with them sometimes felt scared, weak and vulnerable: I was fragile coming home from hospital and especially being on my own here. I just needed someone to hold my hand (User 8);
I was frightened of falling (User 11).
Q11: Witnesses
All eleven service users we interviewed had family members and/or friends who ‘stepped up’ their provision of informal care. One carer (in his 80's) explained: I had a message that she was going to be discharged. I phoned my son because I realised I needed help … went up to the discharge desk and asked the sister ‘was there any medication and notes for discharge?’ And so they looked, and well, they couldn’t find them … after two and a half hours of sitting in there … we did get her home (Carer 4).
This carer went on to explain that no-one had assessed his capacity to cope emotionally – a consistent finding amongst carers. A service user who did not have family members to turn to explained that ‘If it hadn’t been for … my cleaner, I wouldn’t have survived’ (User 8). She explained that her cleaner helped her to wash, get dressed, prepare food and do shopping.
Interview and survey data suggested that users sometimes didn’t know where to look for more support, and were unaware of who was responsible for co-ordinating care. Although GPs were never spoken of within steering group discussions, and were not interviewed as part of the evaluation, service users and carers said GPs were often the first person they called if they had concerns.
Q12: Worldview
The moral basis of the improvement programme was to improve person-centred care and to improve efficiency. Person-centred integrated care might have been advocated as helping move away from an ethos that is medically-dominated, disease-oriented and often fragmented, towards one that is relationship-focused, collaborative and holistic (see, for example, the expanded chronic care model Barr et al., 2003). However, in the drive to reduce the burden on over-stretched hospital services by reducing lengths of stays and reducing service costs, the dominant worldview in the system was one that, in effect if not intent, minimised social, emotional and relational aspects of service user (and even informal carer) wellbeing. Data from user interviews, as illustrated below, suggested that there sometimes appeared to be a lack of compassion amongst staff working to ‘enable’ self-care, and users were sometimes missing the ‘softer’ aspects of a care visit: There’s one [carer] who come and said to me ‘I’m not doing anything today, I’m going to watch you.’ … Christ, bloody mad, I was. I was upstairs, trying to get a stocking off. ‘I’m not going to help you’, she said … Cruel, it was. (User 1)
And she was really bullying, you know; ‘Come on! Come on!’ It was like I haven’t got all day. (User 3)
User 6, who asked for help putting food on a plate the day after coming home from hospital because she was ‘wobbly’ and using a stick was told ‘no, you have to do that yourself’. Every time someone came I said ‘I don’t need an enablement team, I want care, I need care, my legs are like jelly, it takes me forever to go from my bedroom to the bathroom and I need help’. No, no help was ever offered, none whatsoever. (User 8)
Discussion
This article presented a systemic analysis of findings from the evaluation of Swale Home First, using the CSH framework, to understand why achievements were less positive than expected, especially given adoption of a national good practice model (D2A) and an improvement plan co-produced within the SUSTAIN programme. The CSH framework provided a set of conceptual lenses which enabled the authors to model the case study as a system organised around a particular purpose. The structured analysis generated by the framework enabled the team to identify more explicitly different stakeholder perspectives and power relationships within the system and its decision environment.
Values and motivations
The analysis found that different stakeholders tended to emphasise one of two motivations for improvement: (1) improving the transfer of older patients to reduce pressures on acute services/care homes; or (2) improving person-centred, coordinated care during and following transfer to maximise the health, wellbeing and independence of older people. These two purposes are not necessarily mutually exclusive and, in combination, might ease bed pressures through fewer preventable admissions and re-admissions (NHSE et al., 2016). We have shown, however, that Swale’s dominant values and motivations were strongly associated with freeing up acute beds through more rapid discharges. This association was related to a national political goal, backed by earmarked funds, to reduce delayed discharges (Forder et al., 2018). The person-centred dimension of the D2A model received much less attention in national implementation requirements, as did the supply of resources to ensure that independent living was a sustainable option post-discharge. This reflects the lower status of care compared with cure. Thus, local understandings of the model’s purpose were both partial and reinforced by national performance measures and implementation requirements based on similarly partial approaches. Moreover, it emerged that the focus on delayed transfers alone actually intensified some of the problems previously identified.
Power structures
The steering group operated in a decision environment which was, in a number of respects, incompatible with the model’s full implementation. For example, it lacked command over the resources necessary for such implementation, most notably funding for the expansion of community-based services to support earlier discharge and enable independent living. In addition, local staff recruitment and retention were hampered by a decreasing workforce supply (behind the national average), proximity to London, and recent commissioning changes affecting community health care providers. Implementation of the model did little to address the organisational fragmentation of care at the acute/community and health/social care interfaces, or to aid the spanning of the structural, financial and professional boundaries (Glendinning, 2003). Although the predominant framing of the improvement project was to reduce pressure on acute services, the acute sector representative in the steering group was not particularly senior, and did not regularly attend steering group meetings. The fact this didn’t matter reflects the enduring and largely unquestioned position of the acute sector in general (Harrison et al., 1992).
The steering group’s role was further limited by lacking mechanisms or authority to make decisions binding on its members and, thus, the organisational systems and routines of the individual partners continued to have primacy. These characteristics reveal that many factors shaping project outcomes lay outside the control of both the steering group and of its members individually. While the purpose of the group and the wider implementation team was to implement the D2A model, responsibility for many of the factors critical to achieving its full implementation lay outside that group and within its external environment. Moreover, the group to which it reported had little more control over those factors. Ultimately, the project had been tasked with specified ends but not the means to secure them. Problems the group could not improve by the resources and capacity available effectively lost visibility. The narrow boundary established around delayed transfers excluded the full range of improvements that might support improved health and wellbeing for patients discharged earlier to live independently at home.
Knowledge base
The steering group possessed valuable expertise and knowledge but it lacked authority in the decision environment, and also prioritised some forms of information and knowledge over others. Its knowledge base was dominated by those organising/delivering short-term support to people in the community (the Council’s ‘enablement at home’ service and Virgin Care’s rapid response service) and was therefore biased towards ‘quick recovery’. By marginalising the voices of the wider range of professionals, third sector providers, and lay people in the community who help to restore and maintain health and wellbeing, assurances of positive outcomes rested on much wishful thinking (Jones et al., 2021). Also, by focusing on operational- and local-level input rather than strategic-level input across a wider geographical footprint, the group were not able to get the ‘helicopter’ view required to more fully understand the interrelationships between the many different elements within the system (Cabinet Office, 2004).
Moral basis
The benefits for patients presented in the national D2A guidance were assumed and unquestioned. By not challenging them, they relegated to the background the voices of those people who didn’t want to feel ‘pushed’ out of hospital at the earliest opportunity, or who worried about coping, or who felt guilty about the burden they placed on their family. However, we know that the transition from hospital to home is often characterised by worry, emotional challenges and feelings of isolation (e.g. Bull, 1992; Cott, 2004; Ellis-Hill et al., 2009). Third parties (such as GPs, carers, friends) were expected to bear with the consequences of the improvement project on the basis that coming out of hospital quicker was self-evidently good for the patient and good for the hospital. Moreover, the lack of appreciation of interrelationships across the system meant that some consequences went unforeseen. For example, some staff in the hospital (such as OTs and discharge managers) did not trust that there was sufficient capacity in the community to quickly and appropriately assess a person’s support needs and put a plan in place. Trust is identified by many researchers as a key factor in successful inter-organisational relationships (Bloor, 2006). Asking staff not to perform tasks in hospital, but rather to refer patients to Home First, put them in a difficult position. Staff in primary care sometimes had to field the anxiety of patients and their carers following their return home, likely adding to their already stretched workload. The role of GPs in supporting patients overwhelmed by what feels like a sudden or abrupt discharge is noted elsewhere (e.g. Hesselink et al., 2012).
Our analysis exemplifies Churchman’s (1971) insight that the boundaries of analysis are crucial in determining how improvement is defined during an intervention, and hence what actions are taken. As Midgley et al. (1998) state: ‘something that appears to be an improvement given a narrowly defined boundary may not be seen as an improvement at all if the boundaries are pushed out’ (1998: 467). Ideally, boundaries should be established rationally, through dialogue by all those involved in and affected by the intervention (Ulrich, 1996). Midgley’s (1992) work has demonstrated the need to be aware of how some stakeholders and issues may become marginalised during interventions as ethical conflicts emerge. In our case study, an ethic of efficiency (patient throughput and flow) came into conflict with an ethic of person-centred care, which could only be dealt with by marginalising certain elements of the project. The need (due to environmental constraints and pressures) and tendency (due to ‘silo’ working and non-systems thinking) to make a narrow boundary judgement meant that certain elements, though pertinent, lay outside the system on which a light was cast; these elements were therefore cast into darkness. In a Foucauldian sense, power is expressed as the rise of some knowledges into positions of dominance and the subjugation of others. The mechanisms by which some knowledges and ethics maintain dominance while others remain suppressed are both dictated by and work to perpetuate existing power relationships, as is demonstrated by the medical definition underpinning Continuing Health Care.
Conclusion
This article demonstrates that CSH can provide a structure to surface and make transparent a fuller range of stakeholder interests and values, including those of older people, that previous implementation processes had ignored or marginalised. Similarly, the concept of boundary judgements helps to expose the power inherent in defining the purpose and scope of implementation. In this case, D2A came to be understood primarily as a tool for reducing discharge delays rather than one for facilitating discharge and providing individualised support outside hospital. In addition, by widening the system of interest beyond the improvement project and its steering group, the latter’s lack of power to improve outcomes came into sharp focus. Quite simply, they lacked command over the supply of resources necessary to improve system flow, without harming outcomes for some patients. While they largely understood the importance of appropriately tailored care, they lacked both the full range of resources needed and the authority to secure them.
For more than ten years, scholars have advocated a need for evaluation to engage with systems thinking and complexity science (e.g. Patton, 2011; Schmidt-Abbey et al., 2020; Westley et al., 2007; Williams and Imam, 2007). It is clear from this case study that problems faced in re-locating care for older people with complex needs are highly interdependent. This is widely understood in principle, and integrated care programmes (including SUSTAIN) would benefit from incorporating systems thinking and tools into intervention design, implementation and evaluation in order to better facilitate an understanding of the potential for improvement.
A strength of this study is its novel application of CSH to integrated care, highlighting the opportunities for critical systems thinking to better design and evaluate integrated care initiatives. In particular, this approach allows more developed models of analysis that challenge established assumptions and question embedded behaviours. Our case study confirms that such approaches can help ‘unpick the gap between the vision and rhetoric of integrated care initiatives and the reality of largely underwhelming health service outcomes’ (Lalani et al., 2020: 7). Its wider adoption would encourage reflexivity, and whilst improvement would not be guaranteed, it would support the exposure of more fundamental causes of limited outcomes and help focus attention on their mediation.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.