
Abstract
Background:
Depressive and anxiety disorders are prevalent, impactful conditions that are rising globally. Antidepressants showed limited efficacy and side effects, highlighting the need for alternatives. Intermittent fasting (IF) has emerged as a potential nutritional strategy to improve mood-related symptoms (MRSs).
Aim:
To evaluate differences in anxiety and depression between adults practising IF and those following a regular eating pattern (REP), exploring variations within IF groups, comparing early IF (EIF; morning/afternoon feeding), late IF (LIF; afternoon/evening feeding) and REP groups, and between sexes.
Methods:
A cross-sectional study (May 2024–May 2025) employed an anonymous 41-question online survey distributed globally, including the Hospital Anxiety and Depression Scale (HADS) questionnaire to assess anxiety and depression. Data from 302 healthy participants aged 18–65 (88 male, 214 female) were analysed using IBM SPSS Statistics. A two-way ANOVA examined the effects of sex and eating patterns on anxiety and depression.
Results:
Participants included 214/302 (70.9%) in the REP and 88/302 (29.1%) in the IF group, with 22/302 (7.2%) in the EIF and 66/302 (21.9%) in the LIF group. Females reported significantly higher mean anxiety than males (p = 0.047). The IF group reported significantly lower anxiety (p = 0.031) and depression (p = 0.022) than the REP group.
Conclusion:
Our findings suggest an association between IF and reduced anxiety and depression. Further research is needed to elucidate the IF-MRSs relationship, explore sex-specific approaches and optimal dietary strategies to improve MRSs.
Introduction
Depressive and anxiety disorders are the most prevalent and disabling mood-related symptoms (MRSs), with increasing prevalence worldwide (World Health Organization [WHO], 2017). Women experience mental health problems three times more often than men, with anxiety twice as common (Mental Health Foundation, 2025) and depression 50% more prevalent (WHO, 2017). Anxiety affects 4.4% of the global population and is characterised by excessive fear and worry, substantially increasing the risk of depression, substance misuse and suicidal behaviour (WHO, 2025a). Depression is characterised by persistent sadness, diminished interest or pleasure, feelings of guilt or low self-worth, disturbances in sleep and appetite, fatigue and impaired concentration, and may lead to suicide, accounting for nearly 800,000 deaths annually (WHO, 2017). Despite this burden, only one in four individuals with anxiety (WHO, 2025a) and one in three with depression (WHO, 2025b) receive treatment. In the UK, one in four adults and one in 10 children are affected by mental illness (National Health Service [NHS], 2025), with an estimated annual economic cost of £117.9 billion (NHS, 2022).
Antidepressants, often combined with psychotherapy, are the gold standard for treating MRSs (Berthelot et al., 2021; Murta et al., 2023), yet they are only effective in half of patients and can cause severe side effects (Howland, 2008; Rush et al., 2006). Therefore, alternative treatments are needed, with growing interest in nutritional strategies (Marx et al., 2021; Sarris et al., 2020). This is relevant as the pathophysiology of MRSs is linked to genetics, environmental factors (Pettersson et al., 2019; Shadrina et al., 2018) and their interaction (Amare et al., 2017; Gutiérrez-Rojas et al., 2020). Obesity often accompanies MRSs and influences its course (Grigolon et al., 2021; Silva et al., 2020); thus, weight loss might improve outcomes (Fabricatore et al., 2011). The Mediterranean Diet shows consistent protective effects on MRSs (Bayes et al., 2022; Jacka et al., 2017; Parletta et al., 2019; Sánchez-Villegas et al., 2013), and emerging evidence also supports carbohydrate-restricted and ketogenic diets (Dietch et al., 2023). Among novel approaches, intermittent fasting (IF), alternating fasting with ad libitum feeding, has gained prominence over the past 20 years (Murta et al., 2023), partly because caloric restriction is difficult to sustain, while IF might show greater acceptance and adherence (O’Connor et al., 2021).
Preclinical evidence shows changes in gene regulation following a 16-h fasting window (Kim et al., 2018) and suggests that IF may benefit MRSs by reducing insulin resistance and improving body composition (Elesawy et al., 2021; Smith et al., 2019), enhancing serotonergic transmission (Li et al., 2014), increasing neurotrophic factor production (Li et al., 2014; Smith et al., 2019), regulating circadian rhythms (Choi et al., 1998; Dias et al., 2021; Guerrero-Vargas et al., 2021; Shim and Tanaka, 2000) and positively modifying the gut microbiota (Soares et al., 2021), which in turn modulates the microbiota–gut–brain axis (Cignarella et al., 2018; Prada and Diaz-Gomez, 2020). Furthermore, fasting may counter ageing, a risk factor for cognitive decline and mental illness (Longo and Mattson, 2014). In humans, IF has been associated with reduced anxiety and depression, with some studies reporting sex-specific effects, while others suggest that early IF (EIF; morning/afternoon feeding) is potentially the most effective IF pattern for mental health, possibly due to circadian rhythm alignment (Berthelot et al., 2021; Fernández-Rodríguez et al., 2022; Murta et al., 2023). Currently, specific timing guidelines remain undefined (Xie, He et al., 2022). Table 1 shows the most common patterns.
Main types of intermittent fasting patterns.

Note: Adapted from ‘Intermittent Fasting as a Potential Therapeutic Instrument for Major Depression Disorder: A Systematic Review of Clinical and Preclinical Studies’ by L. Murta, D. Seixas, L. Harada, R. F. Damiano, and M. Zanetti, 2023, International Journal of Molecular Sciences, 24(21), 15551, p. 3 (10.3390/ijms242115551).
This research is significant because identifying differences in anxiety and depression across eating patterns, including potential gender variations, could inform future longitudinal and interventional studies aimed at clarifying causal relationships between specific meal timing patterns and reductions in anxiety and depression, as well as determining whether distinct approaches are warranted for males and females. Therefore, this study aimed to assess whether significant differences exist in anxiety and depression between adults practising IF and those following a regular eating pattern (REP). Additionally, the study aimed to explore potential differences within the IF population by comparing EIF, late IF (LIF; afternoon/evening feeding) and REP groups, as well as between sexes.
Methods
Study design and sample
This cross-sectional study used a voluntary, anonymous, quantitative online questionnaire (JISC, 2024), distributed globally via email, social networks (LinkedIn, WhatsApp, Telegram, Facebook, Instagram), online forums (Reddit, r/SampleSize, r/SurveyExchange) and word-of-mouth from May 2024 to May 2025. A sample size of 377 was suggested by the Raosoft calculator (Raosoft Incorporated, 2004) for a 95% confidence level and 5% margin of error. Of 324 completed surveys, 22 were excluded after screening for inclusion/exclusion criteria (Table 2), missing data or response incongruities, leaving 302 participants (88 male, 214 female) for analysis. Among 105 participants reporting IF, 17 were reassigned to the REP group due to mismatched patterns, resulting in a final cohort of 214 in the REP group and 88 in the IF groups (22 EIF, 66 LIF). Due to the low numbers of participants assigned to the EIF group analysis of comparisons between the EIF and LIF groups was considered exploratory. Figure 1 presents the selection process. Ethical approval was granted by St Mary's University, Twickenham, London (UK), Research Ethics Sub-Committee.
Inclusion and exclusion criteria of the study.

Note: Inclusion and exclusion criteria were derived from relevant literature (Alnasser and Almutairi, 2022; Bailey et al., 2023; Fava et al., 2015; Kessler et al., 2018; Nugraha et al., 2020; Riat et al., 2021; Shalabi et al., 2023).
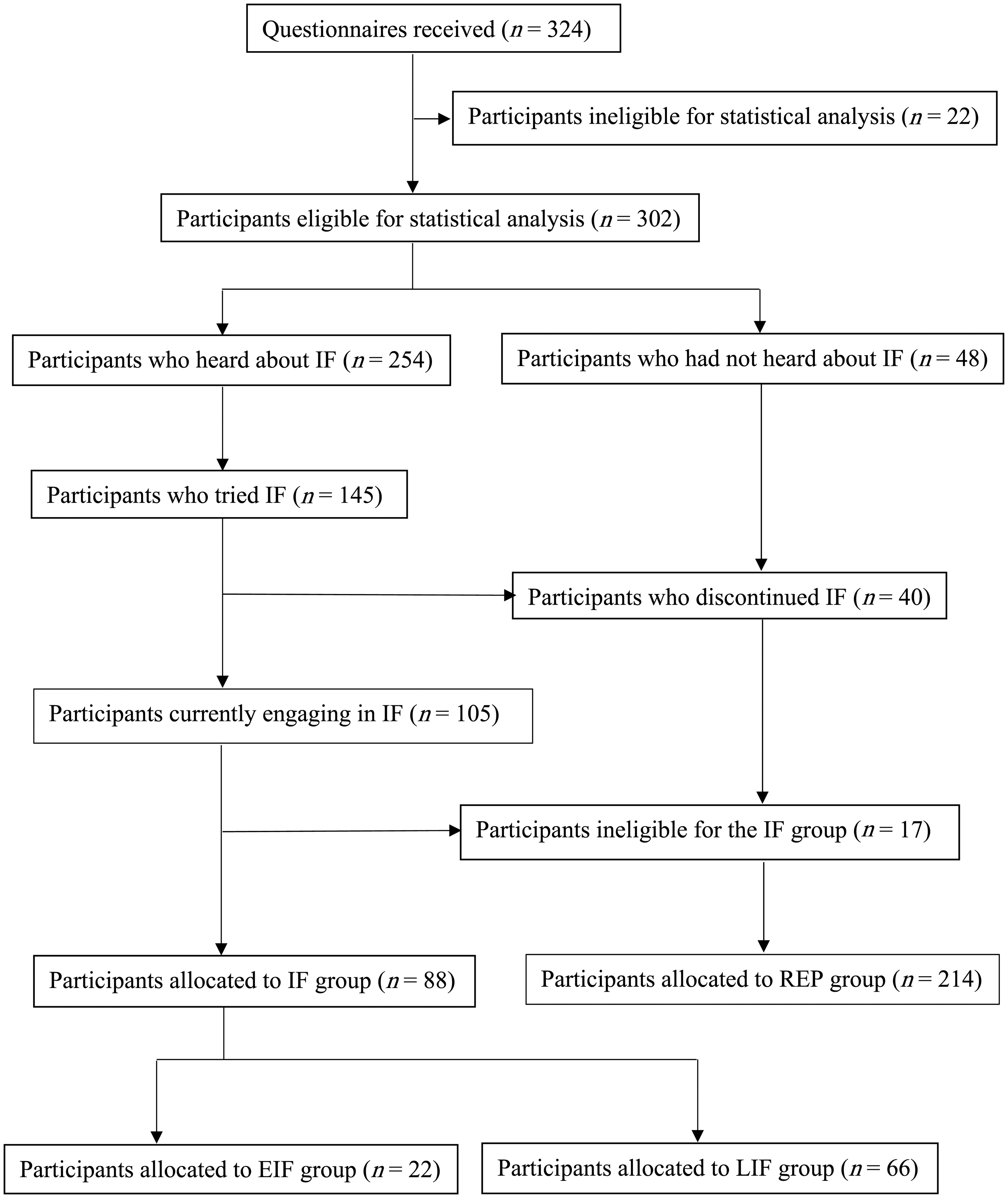
Participant selection flow chart.
Intermittent fasting pattern assessed
Intermittent fasting in the present study was defined as a fasting window of ≥16 h at least 5 days per week, consistent with the definition of time-restricted eating (TRE) presented in Table 1. This reflects the commonly reported 16-h fast among IF followers (Alnasser and Almutairi, 2022; Welton et al., 2020), while the 5-day threshold ensured high adherence (Bjerre et al., 2022; Steger et al., 2023). Participants self-allocated to IF groups based on habitual meal timing, with EIF eating from morning to afternoon and LIF from late morning, noon, or afternoon to evening or night. The REP group had eating windows exceeding 8 h at least 3 days per week.
Questionnaire
The English questionnaire comprised four sections with 41 questions and took approximately 10 min to complete. It drew on relevant literature and was partially adapted from prior surveys assessing experiences and outcomes in voluntary IF populations, comparing responses across multiple parameters. Alhussain et al. (2021) allocated 1242 Muslim Saudi adults outside Ramadan to alternate-day fasting twice weekly or a non-fasting control group. Alnasser and Almutairi (2022) surveyed 514 Muslim Saudi adults practising various voluntary IF regimens, most commonly 8-h TRE. Shalabi et al. (2023) examined voluntary IF practices among 147 Muslim Saudi adults, while Bailey et al. (2023) classified 690 US adults as current or former followers of 12-h TRE. Our participants received an introductory paragraph outlining the study's aim and inclusion/exclusion criteria, provided informed consent with confidentiality and withdrawal assurances, and were given MRSs support resources. Section 1 collected sociodemographic data, including sex, age, ethnicity, country of residence, education, occupation and income (Gov.uk, 2021, 2024a, 2024b; Office for National Statistics, 2021). Section 2 collected self-reported anthropometrics data (height, weight) for Body Mass Index (BMI) calculation and assessed Physical Activity Level (PAL) (Department of Health, 1991; Scientific Advisory Committee on Nutrition [SACN], 2012). Section 3 addressed IF practices, including awareness, sources of information, frequency, reasons for discontinuation (Conlon et al., 2011; Goldhamer et al., 2001; Harvie et al., 2011; Pi-Sunyer, 1993; Redman et al., 2009; Shaheen et al., 2018; Wang and Wu, 2022; Welton et al., 2020), duration, intentions to continue, motivations (Donnelly et al., 2018; Ezzati et al., 2023; He et al., 2023; Li et al., 2023; Rovira-Llopis et al., 2023; Wei et al., 2022; Xie, He et al., 2022; Xie, Sun et al., 2022), practised IF patterns (Adafer et al., 2020; Lü et al., 2023; Steger et al., 2023; Svendsen and Forslund, 2024), hydration, diet, weight loss, physical symptoms, health status changes due to IF and app usage for fasting hours. Section 4 included the 14-item Hospital Anxiety and Depression Scale (HADS) questionnaire (Zigmond and Snaith, 1983).
Statistical analyses
Data were analysed using IBM SPSS Statistics Version 29.0.1.1-244. Categorical variables were reported as counts and percentages; continuous variables as means ± standard deviations. Differences among the three eating patterns were assessed using chi-square tests for categorical variables and one-way ANOVA for continuous variables, with pairwise comparisons in both cases. A two-way ANOVA examined the effects of sex and eating patterns (first REP versus IF, then REP versus EIF versus LIF) on HADS anxiety (HADS-A) and depression (HADS-D) scores. Significant interactions were followed by simple main effects analyses; non-significant interactions were assessed for main effects. Residual analysis tested the assumptions of the two-way ANOVA. Outliers were identified via boxplot inspection, and results were reported with and without them. Normality was assessed with Shapiro–Wilk tests, and homogeneity of variances was evaluated with Levene's tests. Post hoc tests used Bonferroni correction. The significance level was set at p < 0.05, with 95% confidence intervals. The manuscript adhered to the Strengthening the Reporting of Observational Studies in Epidemiology-Nutritional Epidemiology (STROBE-nutreporting) guidelines (Lachat et al., 2016).
Results
Participant characteristics
No significant differences were observed across groups regarding sex, ethnicity, residence, education, profession, income, PAL, height, weight or BMI (p > 0.05). Age differed significantly between groups (F = 3.747, p = 0.025), with LIF participants being significantly older than REP (p = 0.019). Table 3 shows participants’ anthropometrics and PAL; sociodemographics are in the supplementary material.
Participants’ self-reported anthropometric data and PAL.
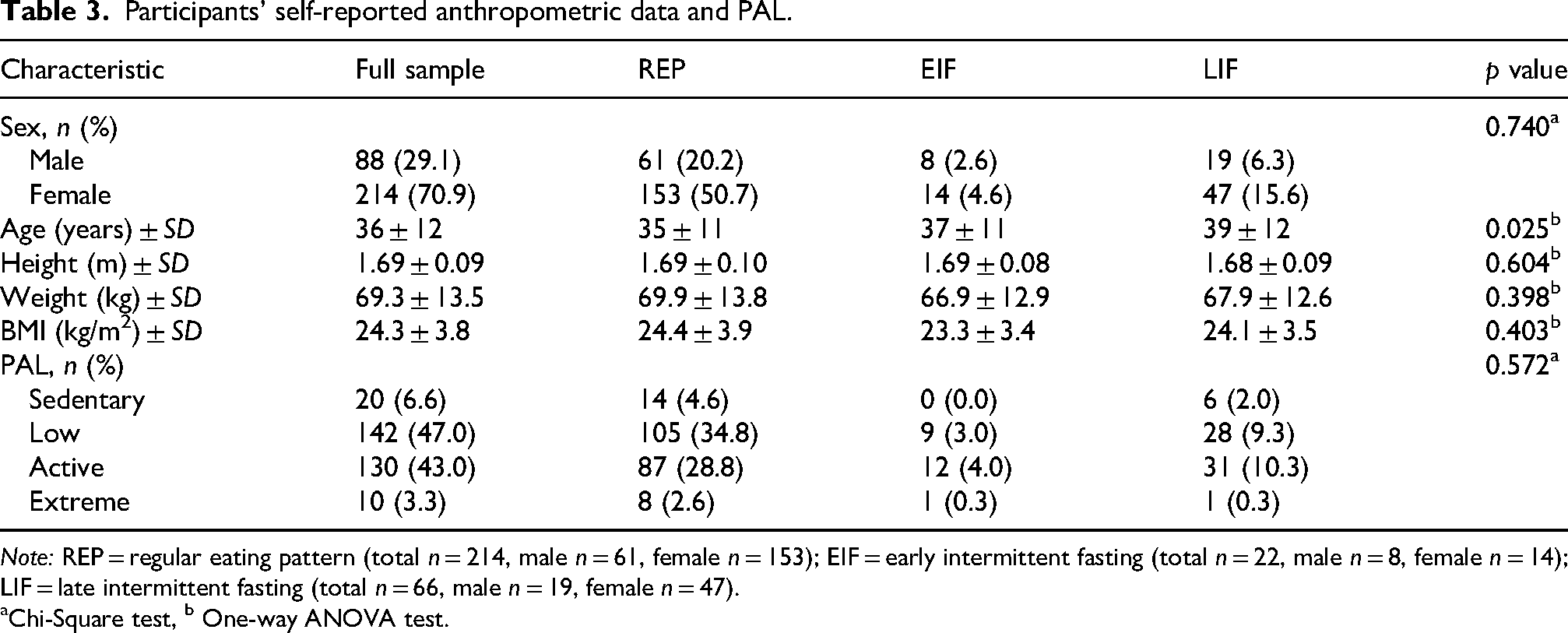
Note: REP = regular eating pattern (total n = 214, male n = 61, female n = 153); EIF = early intermittent fasting (total n = 22, male n = 8, female n = 14); LIF = late intermittent fasting (total n = 66, male n = 19, female n = 47).
Chi-Square test, b One-way ANOVA test.
Participant experiences with intermittent fasting
Among participants, 84% (254/302) had heard of IF; of these, 57% (145/254) had attempted it, with 61% (88/145) engaging multiple times and 17% (25/145) trying it once. Primary information sources were friends and family (39%) and social networks (31%), while healthcare professionals accounted for 9%. Reasons for practising IF included weight loss (43%), improving cognitive/emotional health (27%), decreasing inflammation (27%), reducing chronic disease risk (25%) and enhancing gut microbiota (24%). A 16-h fasting window was the most common, reported by 78% (69/88) of the IF group. While fasting, 94% reported hydrating, and 89% did not use an app to track hours. During the eating window, 67% consumed the same quantity of food, 23% less and 10% more. Sixteen percent reported no specific diet, with high-protein being the most common pattern (14%). Negative IF effects included hunger (33%), energy shortages (19%) and headaches (15%). In contrast, 19% of participants reported no adverse effects. Health outcomes included no change for 52%, improved health for 43% and worsened health for 5%. Weight changes among participants varied, with 26% losing less than 2.2 kg, 18% losing 2.2–4.9 kg, 9% losing 5–9.9 kg, 37% experiencing no change and 4% gaining weight. Reasons for discontinuing IF included loss of interest (26%), decreased energy (13%) and adverse cognitive/emotional effects (11%). Length of IF experience varied, with 12% having practised for 3–6 months, 18% for 7–12 months, 36% for 1–5 years and 12% for over 5 years. Regarding plans to continue IF, 39% intend lifelong adherence, 50% are unsure and 10% will stop after achieving specific goals.
Participants’ HADS-A scores
Assessing anxiety across REP and IF groups did not reveal a significant interaction effect between sex and eating patterns (F = 0.358, p = 0.550). Females had significantly higher mean HADS-A (8.1 ± 4.5) than males (6.8 ± 4.1, p = 0.047). The IF group had significantly lower mean HADS-A (6.7 ± 4.7) than the REP group (8.2 ± 4.2, p = 0.031). Mean HADS-A scores are represented in Figure 2. Results remained consistent after excluding four outliers, although sex differences were no longer significant (p = 0.061). When comparing REP, EIF and LIF groups, no significant interaction was observed between sex and eating patterns (F = 0.593, p = 0.553), and no main effects of sex (F = 2.930, p = 0.088), or eating patterns (F = 2.733, p = 0.067) were found. Results remained consistent after excluding four outliers.
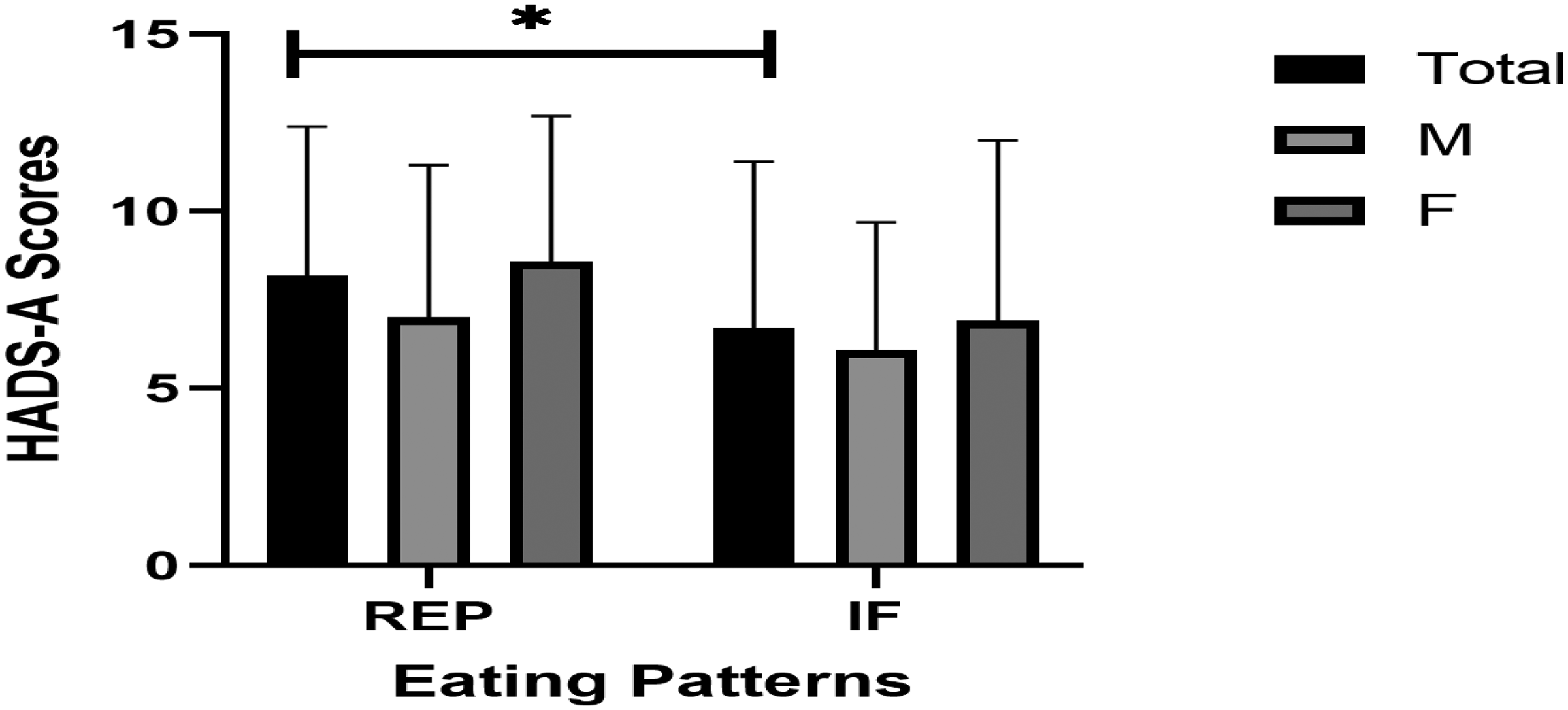
Mean HADS-A scores by group. Note: REP = regular eating pattern (total n = 214, male n = 61, female n = 153); IF = intermittent fasting (total n = 88, male n = 27, female n = 61). M = male, F = female. Error bars represent + SD.
Participants’ HADS-D scores
Assessing depression across REP and IF, there was no significant interaction effect between sex and eating patterns (F = 0.148, p = 0.700). The IF group had significantly lower mean HADS-D (3.3 ± 3.3) than the REP group (4.4 ± 3.5, p = 0.022). Mean HADS-D scores are represented in Figure 3. Results remained consistent after excluding four outliers and two extreme outliers. When comparing REP, EIF and LIF groups, no significant interaction effect between sex and eating patterns was observed (F = 0.060, p = 0.941). There was a significant main effect of eating patterns (F = 3.235, p = 0.041). However, Bonferroni-adjusted pairwise comparisons were not significant (p > 0.05). After removing four outliers and two extreme outliers, the EIF group had significantly lower mean HADS-D than the REP group (p = 0.047).

Mean HADS-D scores by groups. Note: REP = regular eating pattern (total n = 214, male n = 61, female n = 153); IF = intermittent fasting (total n = 88, male n = 27, female n = 61). M = male, F = female. Error bars represent + SD.
Discussion
This study aimed to assess differences in anxiety and depression between adults practising IF and those following REP, and within the IF population exploratory analysis was carried out to compare EIF, LIF and REP groups, as well as between sexes. Males reported significantly lower anxiety than females, and the IF group reported significantly lower anxiety and depression than the REP group.
Participant characteristics
Females accounted for 71% of participants, reflecting lower male response rates in surveys (Dillman et al., 2002; Singer et al., 2000). LIF, but not EIF, participants were significantly older than REP. Previous research has reported that current IF followers were older compared with former followers (Bailey et al., 2023), suggesting that younger individuals may exhibit lower adherence due to social influences on eating behaviour (Martin et al., 2018), heightened hunger cues (Johnson et al., 2020) and reduced health-related concerns (Gooding et al., 2016). Conversely, other evidence observed a young IF follower sample, suggesting greater health and weight consciousness among this group (Shalabi et al., 2023). There was no significant difference in BMI between the IF and REP groups; previous findings have been mixed reporting no difference (Bailey et al., 2023), higher (Alhussain et al., 2021) or lower (Alnasser and Almutairi, 2022) BMI values among IF followers.
Anxiety and depression
Anxiety and depression scores were significantly lower in the IF group than in the REP group, aligning with a recent systematic review and meta-analysis of 14 intervention studies, which found that IF moderately reduces depressive symptoms; however, no significant reduction in anxiety was observed (Fernández-Rodríguez et al., 2022). Alternate-day fasting interventions have reported promising results: two RCTs, one in multiple sclerosis patients (Fitzgerald et al., 2018) and one in obese prediabetic subjects (Tay et al., 2020), reported reductions in depression, while a non-RCT in healthy subjects found decreases in anxiety and depression lasting up to six months (Kessler et al., 2018). However, when combined with caloric restriction, alternate-day fasting yielded mixed results: an RCT in healthy older men reported improved mood but no change in depression compared with controls (Hussin et al., 2013); an RCT in overweight/obese subjects found mood improvements with both fasting plus caloric restriction and caloric restriction alone (Bowen et al., 2018); and an RCT in healthy overweight/obese women observed no between-group differences relative to caloric restriction (Teong et al., 2021). Notably, improvements in depression following calorie restriction without fasting have been reported (Fitzgerald et al., 2018; Martin et al., 2016; Prehn et al., 2017). Short-term caloric restriction may exert antidepressant effects (Zhang et al., 2015) via orexin activation, enhanced CREB phosphorylation and neurotrophic effects associated with endorphin release and ketone production (Fusco et al., 2012; Lutter et al., 2008; Molina et al., 1995), although, over time, it is challenging to maintain (O’Connor et al., 2021) and can trigger depression (Li et al., 2018). It remains unclear whether IF offers benefits beyond caloric restriction or whether specific IF patterns are superior (Berthelot et al., 2021).
Previous research suggested that the response to IF on MRSs is stronger in males than in females (Nugraha et al., 2020). No differences were observed in the present study, although females exhibited significantly higher anxiety levels than males, confirming a greater predisposition to anxiety (Mental Health Foundation, 2025). The study by Nugraha et al. (2020) was carried out on Ramadan fasting (RF), assessing MRSs before, during and after a religious fasting period, whereas the present study compared voluntary fasting with non-fasting individuals. Ramadan studies have also shown heterogeneous results. A systematic review and meta-analysis of 11 studies, five of which examined RF, reported moderately lower anxiety and mildly lower depression in fasting groups, with Ramadan itself associated with improved MRSs (Berthelot et al., 2021). However, some studies have reported worsening MRSs in response to RF (Gueldich et al., 2019; Roky et al., 2000), and the only study involving patients with Major Depressive Disorder found no change (Jahrami et al., 2021). A recent systematic review of RF by Ahmed et al. (2025) found reductions of 72.7% in depression and 66.6% in anxiety symptoms, with no gender differences. MRSs improvements were attributed not solely to fasting per se, but to a constellation of interconnected lifestyle changes during Ramadan (Ahmed et al., 2025), including spiritual and social engagement (Berthelot et al., 2021), tobacco abstinence (Secades-Villa et al., 2017) and sleep reduction (Ioannou et al., 2021). Biologically, Ramadan has been associated with reduced inflammation, oxidative stress and cortisol levels, alongside enhanced neurogenesis and neurotransmitter regulation, including increased serotonin, dopamine and gamma-aminobutyric acid (GABA) (Sulaiman et al., 2023). Conversely, poorer MRSs during Ramadan have been associated with individual and cultural differences (Berthelot et al., 2021; Heun, 2018) and late-night food consumption (Al-Rawi et al., 2020), which may disrupt circadian rhythms (Qasrawi et al., 2017). In mammals, the circadian system follows an approximately 24-h rhythm and regulates hormonal secretion, metabolism, digestion, feeding behaviour and the sleep–wake cycle (Fishbein et al., 2021; Flanagan et al., 2021; Murta et al., 2023), with strong evidence for a bidirectional association with MRSs (Walker et al., 2020). Daytime fasting with nocturnal feeding, as observed in RF, may exert an anti-physiological effect on the circadian system (Murta et al., 2023), and the failure of many RF studies has been attributed to incongruity with circadian regulation, which partially reverses normal circadian patterns and disrupts biological clocks (Qasrawi et al., 2017).
Previous research has suggested that TRE based IF, as measured in the present study, may represent the most effective eating pattern for supporting mental health, potentially through circadian rhythm alignment (Panda, 2016), with EIF showing greater synchrony with human physiological rhythms (Cioffi et al., 2018), as key metabolic circadian rhythms, including insulin sensitivity and the thermic effect of food, peak in the morning (Poggiogalle et al., 2018). Consistent with this, two RCTs, one in healthy obese individuals (Jamshed et al., 2022) and another in patients with type 2 diabetes (Kahleova et al., 2015), reported significant reductions in depressive symptoms following EIF combined with caloric restriction, compared with caloric restriction alone. In the present study, however, no significant differences in anxiety or depression were observed between individuals practising EIF and those practising LIF. These findings should be interpreted cautiously due to the small number of EIF participants. Nonetheless, in line with previous evidence, fasting timing warrants further investigation in studies with larger samples. Age has also been suggested as a factor that may moderate the impact of IF on MRSs. A retrospective cohort study reported reduced mental distress in participants over 70 with an eating window of ≤8 h, although there was no effect in the overall sample (Currenti et al., 2021).
Participant experiences with intermittent fasting
With 84% of participants aware of IF, these findings underscore its growing prominence. Many followers had practised it for years and intended to continue, while loss of interest was the main reason for discontinuation, suggesting IF is a well-tolerated, simple and sustainable lifestyle choice (Bjerre et al., 2022; O’Connor et al., 2021), and supporting evidence of high satisfaction with the practice (Shalabi et al., 2023). LIF was the predominant pattern, aligning with reports that dinner is the most frequently consumed meal (Bailey et al., 2023), and the 16-h fasting window was most common, consistent with previous findings (Alnasser and Almutairi, 2022; Welton et al., 2020). Upon breaking the fast, our participants followed diverse dietary patterns, while 16% followed none, consistent with previous findings (Alnasser and Almutairi, 2022), suggesting reliance on the inherent benefits of IF (Wilhelmi de Toledo et al., 2020; Zouhal et al., 2020). Weight reduction was the main motivator for practising IF, aligning with previous findings (Alhussain et al., 2021; Alnasser and Almutairi, 2022; Bailey et al., 2023; Shalabi et al., 2023) and supported by evidence of its effectiveness (Wilhelmi de Toledo et al., 2020; Zouhal et al., 2020). Notably, 27% reported following IF to improve MRSs, contextualising our study. Significant weight loss was reported following IF, consistent with previous studies (Alnasser and Almutairi, 2022; Shalabi et al., 2023). A 5% reduction in body weight is clinically meaningful, lowering disease risk (Williamson et al., 2015) and indicating programme efficacy (Perry et al., 2011), supporting IF as a viable alternative to caloric restriction for metabolic health (Antoni et al., 2018; Gill and Panda, 2015; Kesztyus et al., 2019; Lin et al., 2023; O’Connor et al., 2021; Wilkinson et al., 2020; Xie, Sun et al., 2022), primarily via an unintentional reduction of 350–500 kcal/day (Gabel et al., 2021).
Heterogeneity in findings likely reflects differences in study design, sample characteristics, MRSs assessment, type of IF investigated and study duration (Berthelot et al., 2021; Fernández-Rodríguez et al., 2022; Murta et al., 2023). Only one study specifically examined Major Depressive Disorder, and none assessed diet quality (Murta et al., 2023). Furthermore, MRSs were often ancillary, and participants generally had healthy baseline anxiety and depression, as also observed in the present study, where scores up to 7 on HADS-A and HADS-D were classified as ‘Normal’, limiting observable effects and suggesting that IF could be more effective in psychiatric populations, pending clinical confirmation (Berthelot et al., 2021). Intervention duration appears crucial, with studies over 12 weeks showing greater MRSs reductions, suggesting physiological adaptation requires time (Murta et al., 2023). In the present study, participants’ extended IF experience may explain their lower anxiety and depression scores versus the REP group.
Strengths and limitations
This study is the first cross-sectional analysis to examine different eating patterns, sexes and MRSs, specifically focusing on 8-h TRE practised at least 5 days per week. Moreover, a reasonable number of long-term IF followers provided valuable insights. However, these strengths also highlight certain limitations. Recruitment was global; therefore, cultural or religious fasting practices that may influence participation, such as reliance on RF, might have reduced the inclination to engage in other forms of IF. Dependence on a self-reported questionnaire may have introduced recall bias and, among IF followers, favourable bias (Alnasser and Almutairi, 2022; Bailey et al., 2023; Shalabi et al., 2023), while the online format may have caused selection bias by excluding participants without digital access or English proficiency. Seventeen participants reporting IF were reclassified into the REP group due to mismatched IF patterns, potentially affecting results, as different fasting protocols may differentially influence MRSs. Misclassification bias is also possible within the REP group, as individuals who naturally skip meals but are unaware of IF could have been incorrectly categorised. The moderate and uneven sample size, 88/302 in the IF group and only 22 in the EIF subgroup, limited the statistical power, so these results can only be considered exploratory. Finally, the cross-sectional design precluded causal inference.
Future research should clarify associations and causality between IF and MRSs, include larger and more balanced samples, and evaluate whether IF exerts benefits beyond caloric restriction. Longitudinal studies and RCTs exceeding 12 weeks, incorporating follow-up and involving registered dietitians and nutritionists, are warranted to assess feasibility across diverse populations, including older adults, obese individuals, diabetics and those diagnosed with Major Depressive Disorder, and incorporate Ramadan cohorts to disentangle physiological from contextual effects (Bailey et al., 2023; Berthelot et al., 2021; Lee et al., 2020; Murta et al., 2023). Further investigations should determine which IF patterns yield the most pronounced benefits, whether sex-specific adaptations are required, and whether dietary composition during the eating window confers additional mental health advantages (Murta et al., 2023).
Conclusions
Our findings suggest an association between IF and reduced anxiety and depression. Further research is warranted to clarify the relationship and causality between IF and MRSs, evaluate its feasibility in vulnerable populations, and explore sex-specific adaptations and optimal dietary strategies for integration with IF.
Supplemental Material
sj-docx-1-nah-10.1177_02601060261450010 - Supplemental material for Timing matters? Assessing the relationship between a regular eating pattern compared to intermittent fasting (early versus late) and mental health outcomes: A cross-sectional study
Supplemental material, sj-docx-1-nah-10.1177_02601060261450010 for Timing matters? Assessing the relationship between a regular eating pattern compared to intermittent fasting (early versus late) and mental health outcomes: A cross-sectional study by Alfio Giuffrida, Lottie Burnett-Armstrong, Emily West and Alexandra King in Nutrition and Health
Supplemental Material
sj-docx-2-nah-10.1177_02601060261450010 - Supplemental material for Timing matters? Assessing the relationship between a regular eating pattern compared to intermittent fasting (early versus late) and mental health outcomes: A cross-sectional study
Supplemental material, sj-docx-2-nah-10.1177_02601060261450010 for Timing matters? Assessing the relationship between a regular eating pattern compared to intermittent fasting (early versus late) and mental health outcomes: A cross-sectional study by Alfio Giuffrida, Lottie Burnett-Armstrong, Emily West and Alexandra King in Nutrition and Health
Footnotes
Acknowledgements
We extend our gratitude to all participants for their time and involvement, which was essential to the success of this research.
Ethical approval
Ethical approval for this study was granted by the Research Ethics Sub-committee at St Mary's University, Twickenham, London (UK) (SMU_ETHICS_2023-24_570 and SMU_ETHICS_2024-25_895). An online consent form for participation in the study was provided on the survey website.
Consent for publication
All authors approved the submission and consented to the publication of the manuscript.
Authors’ contributions
AG: conceptualisation, designing the study, data collection, data analysis and writing the manuscript – preparation, review and editing. LBA and EW: data collection and writing the article – review. AK: formulating the research question, designing the study and writing the article – review and editing. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Availability of data and materials
Data can be obtained from the corresponding author upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.