
Abstract
Background
Severe obesity is increasing in prevalence globally, placing a significant burden on an individual's health and to public healthcare systems. Multidisciplinary and group-based interventions – which involve coordinated input from dietetics, psychology, physiotherapy and peer support – may improve health behaviours and weight outcomes in individuals living with severe obesity. At current, there is no assessment of the efficacy of group-based, multidisciplinary interventions, in severe obesity management.
Aims/Objectives
Thus, this study aims to evaluate the efficacy of an 8-week group-based multidisciplinary intervention, termed Be Well, on initial changes to dietary behaviours, weight and mood outcomes in patients living with severe obesity. The study was conducted at a hospital-based and publicly funded obesity service, based in New South Wales, Australia.
Method
127 were registered to attend Be Well. Of these, 98 attended the first session, and 77 proceeded to complete the intervention. Changes in dietary behaviours (i.e. reported discretionary and non-discretionary food intake), body mass index (BMI) and mood (i.e. scores on the DASS-21), from pre to post intervention, were evaluated.
Results
From pre to post intervention, patients had significant reductions in BMI, self-reported discretionary food intake, stress and depression scores. Patients reported feeling less isolated and having an improved understanding of health beyond weight, post the intervention.
Conclusion
Multidisciplinary group interventions are an effective first step for the treatment of severe obesity by tertiary services, with more work needed to understand barriers and facilitators of engagement.
Introduction
Obesity is a complex metabolic disease, commonly defined as a body mass index (BMI) of ≥ 30.0 kg/m2, and further classified according to degree – that is, mild (class 1; BMI of 30 to 35), moderate (class 2; BMI of 35 to 40) and severe (class 3; BMI ≥ 40). Based off this definition at least one-third of Australians have obesity, with prevalence increasing nationally (i.e. from 19% in 1995 to 31% in 2018 (AIHW, 2024)) and internationally (i.e. 4% in 1975 to over 18% in 2016 (NCD-RisC, 2016)). Obesity is associated with several physical health (e.g. type 2 diabetes, cardiovascular disease, obstructive sleep apnoea, and cancers) and mental health (e.g. depression, anxiety (Pi-Sunyer, 2009; Scully et al., 2021)) disorders. Relative to mild and moderate forms of obesity, individuals with severe and class 3 obesity are more likely to have obesity-related comorbidities and adverse health outcomes (Abdelaal et al., 2017; Andreyeva et al., 2004; Kyrou et al., 2000).
Weight loss and management interventions for obesity, especially when severe and complicated (i.e. accompanied by several adverse health conditions and outcomes), can be useful in the short term but vary in their long-term efficacy (Bischoff et al., 2017). In their meta-analysis, Anderson et al. (2001) reported that after 5 years, only 21% of individuals living with obesity maintained the weight they lost from a very low energy diet (based on 8/29 studies (Anderson et al., 2001)). One reason weight loss interventions have low long-term efficacy is that many rely on just one type of treatment (e.g. diet or exercise or surgery or psychotherapy etc.). As obesity is a multifactorial disease – that is, related to genetic, metabolic, economic and psychosocial factors – multidisciplinary interventions, which involve coordinated input from dietetics, psychology and physiotherapy, are required (Bischoff et al., 2017; Cannon et al., 2016). In line with this, a multicomponent intervention – which focussed on diet change, physical activity, group cognitive behavioural therapy and psychoeducation – was shown to have a greater effect on weight loss in individuals with obesity, relative to an intervention that only addressed a single behaviour (i.e. diet change (Donini et al., 2009)).
International guidelines strongly recommend the multidisciplinary approach to treatment of obesity, especially when severe and complicated (Sharaiha et al., 2023). Despite this, there are relatively few publicly or privately funded multidisciplinary obesity services in Australia, limiting evaluation of their efficacy (Atlantis et al., 2018; Chen et al., 2022; Lam et al., 2024). Further, there appears to be little evaluation of cost-effective multidisciplinary approaches to treatment of severe obesity, such as group-based multidisciplinary interventions. Group-based multidisciplinary interventions may be effective in severe obesity management, especially when operating in adjunct to individualised specialist appointments (Cannon et al., 2016). This is because they require fewer resources (i.e. have a lower staff to patient ratio), offer peer support, and involve coordinated input across dietetics, psychology and physiotherapy. Evaluating the efficacy of group-based multidisciplinary interventions for severe obesity in particular, is important because relative to other forms of obesity, severe obesity is responsible for the greatest economic burden in terms of healthcare cost and overall costs to society (Andreyeva et al., 2004).
To add needed evaluation of multidisciplinary treatment of obesity in Australia, this study aims to evaluate the initial dietary, weight and mood outcomes of individuals living with severe and complicated obesity, who attended an 8-week group multidisciplinary lifestyle intervention, termed Be Well. There are three ways Be Well differs from other interventions for obesity. First, Be Well is a relatively short intervention – that is, 8 weeks, with each session only 2 h in duration – making it feasible for online and in person delivery, and for individuals with work and carer commitments. Second, to better suit the needs of individuals living with severe obesity, Be Well focusses on holistic wellbeing outcomes, which are measured by self-report measures of diet quality, and mood (i.e. depression, anxiety and stress), alongside weight. Third, to promote adherence to lifestyle modifications promoted in Be Well (i.e. diet, exercise), Be Well uses cognitive behavioural components, such as behavioural activation (i.e. activity scheduling to improve mood and promote motivation), and cognitive strategies (e.g. realistic and achievable goal setting, and promotion of alternative behaviour during negative mood states to manage emotional eating; Castelnuovo et al., 2017).
Be Well was led by practitioners from the Family Metabolic Health Service's Adult Healthy Weight Clinic – that is, a multidisciplinary, publicly funded obesity service based in the Nepean Blue Mountains Local Health District (Williams et al., 2023). As the prevalence of obesity in the Nepean Blue Mountain region (i.e. 31.5%; HealthStats NSW, 2025)) is comparable to that of Australia, this region provides an ideal sample to examine the efficacy of multidisciplinary interventions for the treatment of severe obesity in Australia.
Method
Participants
Participants were eligible if they resided in the Nepean Blue Mountains Local Health District and were referred to the Adult Healthy Weight Clinic from February 2019 to December 2019. During this time, four Be Well interventions were evaluated (with ∼20 to a maximum 30 individuals per intervention). Sample size was based on effect sizes derived from past obesity intervention studies examining weight and mood improvements (i.e. Cohen's d = ∼0.3 to 1, which equated to approximately 90 participants, using Howell's formula; Anderson et al., 2001; Donini et al., 2009; Howell, 1992)
A total of 127 individuals (Male = 33, Female = 92, Prefer not to say/unknown = 2) were enrolled to attend one of the Be Well interventions between February and December 2019. All individuals were aged between 17 and 72 years (M = 43.3, SD = 14.4). Of the total sample, 98 (Male = 26, Female = 71, Prefer not to say/unknown = 1) attended at least one session of Be Well, who were aged between 17 and 72 years (M = 44.9, SD = 14.3, Median = 42, IQR = 34 to 56).
Materials and measures
Patient referral form
The following data was extracted from the referral form.
Basic demographic information
Gender (male, female, prefer not to say), Aboriginal or Torres Strait Islander status (yes, no) and geographical (postal-code) information.
General health information
Smoking status (yes, no, not answered), restricted mobility (yes, no), Number of medications (0, 1–2, 3–4, ≥ 5).
Presence of pre-specified chronic health conditions of interest
Presence of any of the following obesity-related conditions was recorded: Type 2 diabetes, obstructive sleep apnoea, hypertension, metabolic dysfunction associated fatty liver disease, asthma, gastro-oesophageal reflux disease, cardiovascular disease, other (specify).
Mental health conditions
Presence of any: Depression, anxiety, other (specify).
Types of medications
Use of – insulin, glucogen-like-peptide- 1 (GLP-1) agonist or phentermine, selective serotonin re-uptake inhibitors, anxiolytic/ hypnotics, antimanic drugs, opioids and analgesics, and other medications – was quantified.
Anthropometric measurements
Body weight (kg) and height (m) were collected at the first Be Well, post Be Well (8 weeks and 12 weeks) by the facilitating clinicians.
Socio-Economic Indexes for Areas Index (SEIFA) of household disadvantage (Australian Bureau of Statistics, 2019)
This is publicly available data in Australia, which ranks geographical areas according to their relative socio-economic disadvantage (i.e. most disadvantaged [1] to least [5]) using census data. A SEIFA disadvantage score was generated for each participant, based on their residential postal code.
The depression anxiety and stress scale (DASS-21)
The DASS-21 is a 21-item measure that assesses trait levels of depression, anxiety and stress (Lovibond and Lovibond, 2011). Participants were asked to rate how often, over the past week, they had experienced symptoms of depression (N = 7 items), anxiety (N = 7 items) and stress (N = 7 items), on a 4-point scale (0–3) – which were then totalled to respectively form Depression, Anxiety and Stress subscales. Depression, Anxiety and Stress subscale scores were then multiplied by two, and thus each ranged from 0 to 42 – with the total DASS score ranging from 0 to 126. This scale was only administered to two/four Be Well Group, due to later consideration of its utility in measuring self-reported depression, anxiety and stress.
Food recall survey
This is a bespoke survey, based off pre-existing lengthier nutrition surveys (ABS, 2024; New South Wales Health, Population Health Surveys, 2024), and was designed by senior dietitians at the Family Metabolic Health Service to measure intake of non-discretionary and discretionary foods.
Non-discretionary food recall. Participants were asked to specify the number of daily serves they have of: Fruit (from 0 to 5 + serves per day), vegetables (from 0 to 5 + serves per day), grains and cereals (from 0 to 8 + serves per day), dairy or dairy alternatives (from 0 to 5 + serves per day), and protein-based foods (from 0 to 6 + serves per day). Visual images of an Australian serving size for each were provided for guidance (see Stata | StataCorp LLC, n.d.). Scores on each of these variables were summed to get a ‘non-discretionary food intake score’.
Discretionary food recall. First, participants were asked to specify the number of times per day they consumed discretionary foods (from 0 to 6 + serves per day) – with visual images provided for examples of discretionary foods (see EatforHealth.gov, 2024). Second, participants were asked to rate how often they consumed each of the following foods – that is, fried potato/hot chips, fruit juice/cordial, sugar sweetened beverages/soft drinks, chips/crisps, sweet snacks/cakes/biscuits/muesli bars, ice-cream /chocolate /lollies /confectionary, alcoholic drinks and processed meats – using the response options, ‘never or < once per week [0]’, ‘1–2 times per week [1.5]’, ‘3–4 times per week [3.5]’, and ‘Daily [7]’. Scores on each of these variables were summed to get a ‘discretionary food intake score’.
Be Well evaluation form
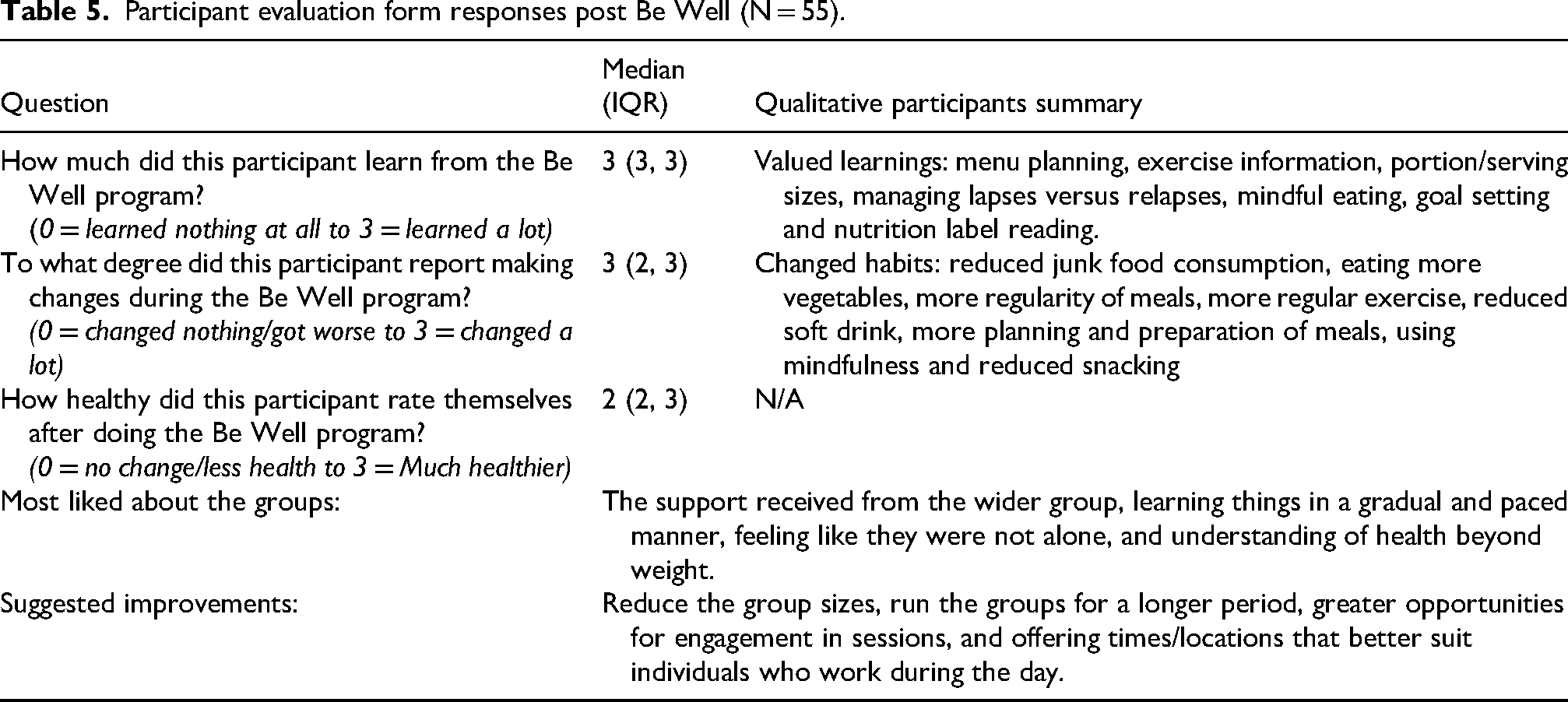
An evaluation survey comprised of three Likert questions, which asked respondents: (1) how much they learnt from the program (0 ‘nothing’ to 3 ‘a lot’); (2) the extent to which they made changes during the program (from 0 ‘changed nothing/got worse’ to 3 ‘changed a lot’); and (3) how much healthier they felt after Be Well (from 0 ‘not at all healthier/less healthier’ to 3 ‘much healthier’). Four free text questions which asked respondents; (1) what their valued learnings were; (2) what their changed habits were; (3) what they most like about the Be Well group intervention; and (4) suggested improvements.
Procedure
As Be Well forms a part of a clinical setting, content may have varied slightly week to week (e.g. depending on the questions patients asked). The typical procedure was as follows: First, Adult Healthy Weight Clinic patients came to the Be Well intervention, where four baseline assessments/checks were done: (1) body height and weight; (2) eligibility for an 8-week group intervention; (3) dietary intake (as measured via the Food Recall Survey) and (4) the DASS-21 (for two of the four Be Well Groups, due to later consideration of its utility in measuring self-reported depression, anxiety and stress; see section Participants).
Second, the Be Well intervention was delivered and comprised of two-hour weekly sessions, which ran for 8 weeks. All Be Well sessions were run in person at either the Adult Healthy Weight Clinic or a local neighbourhood community centre. Each session included a presentation, group discussion and related educational exercises. All sessions were run by a clinical psychologist and a dietitian, ensuring appropriate nutritional and physical activity information, and psychological strategies for behaviour change, and improved self-care.
Third, and at the last Be Well session (week 8), participants completed the DASS-21, Food Recall Survey and the Be Well Evaluation form, and had their height and weights measured again by a clinician. Finally, at one month post Be Well, participants who continued to attend the Adult Healthy Weight Clinic had their heights/weights remeasured at each clinic appointment.
Analyses
All analyses were then performed using STATA data analysis and statistical software version 18 (Stata, 2024). Data were non-normally distributed (i.e. standardised skewness and kurtosis values were ≥ 3, and QQ plots examination). As such, non-parametric tests were run. To reduce bias, data analyses were run by research members (SS, GM) not involved in Be Well administration. A visual summary of the recruitment and data analysis approach can be found in the flow diagram (see Supplemental Figure 1).
Prior to running the analyses, three preliminary steps were done. First, Likert question data was numerically coded and scored. Second, participants were grouped into one of two cohorts; (i) completers (those who attended ≥ 6 or more group sessions (N = 76/98 [77.6%]) and (ii) non-completers (those who attended < 6 group sessions (N = 22/98 [22.4%]). Third, and for 9 (11.5%) of completers, the last body weight measured was at week 6–7 (as opposed to week 8 (last Be Well)), and we used this weight as their final weight to reduce missing data.
There were five steps taken to analyse the following data. First, and to provide a description of the total cohort (N = 127), descriptive statistics were run on participant characteristics retrieved from their referral form. Second, and for each outcome variable of interest – that is, Food Recall Survey scores, BMI and DASS-21 – we examined if there were any differences in baseline scores between completers and non-completers via Mann-Whitney U-tests. This step was done to ensure that there were no systematic differences that could account for attrition rates.
Third, and for the completers only, the difference in BMI at the start of Be Well (baseline) relative to post Be Well (at 8 weeks and 12 weeks), were examined using Wilcoxon signed rank tests. Fourth, differences in dietary recall and DASS-21 scores (at baseline vs 8 weeks) were assessed via Wilcoxon signed rank tests. Fifth qualitative data was summarised.
Alpha levels were set for each outcome variable of interest separately. For food-recall responses, alpha was adjusted so that the family-wise error rate was set by food-type (discretionary, non-discretionary; i.e. 0.05/2). For BMI, significance was accepted at an alpha level of 0.05. For the DASS-21, the family wise error was set by subscale (depression, anxiety, stress; i.e. 0.05/3). As data are sensitive and can be used to identify patients, data is not made available. Only non-identifiable (e.g. aggregate scores) data for non-sensitive information will be made available on reasonable request.
Results
Descriptives of participants at referral
All characteristics of the total enrolled sample (N = 127) at referral are presented in Table 1. Three characteristics warrant commenting. First, approximately half the sample qualified as having polypharmacy (≥ 5 medication). Second, the majority of the cohort came from a region classified as moderately disadvantaged (56.7%). Third, the most prevalent chronic health conditions were obstructive sleep apnoea and type 2 diabetes present in approximately 40% of the sample.
Participant characteristics at referral (N = 127).
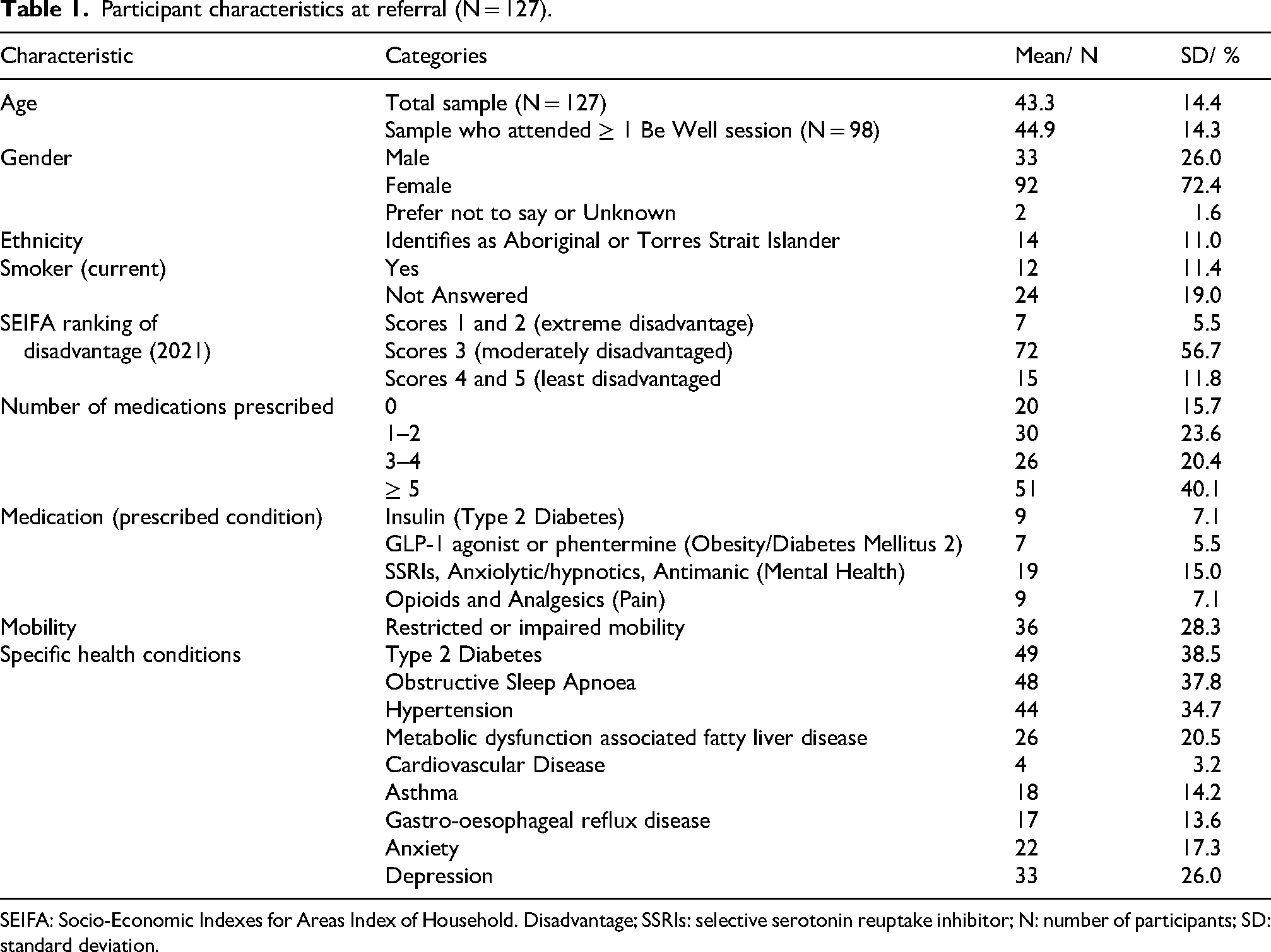
SEIFA: Socio-Economic Indexes for Areas Index of Household. Disadvantage; SSRIs: selective serotonin reuptake inhibitor; N: number of participants; SD: standard deviation.
Dietary recall results
Dietary recall responses (baseline: Completers vs non-completers)
Mann-Whitney U-tests were run to compare discretionary and non-discretionary food intake scores, in completers and non-completers. There was no statistically significant difference found between the baseline Food Recall scores of completers (N = 54) versus non-completers (N = 8), in terms of their discretionary (Z = −1.68, p = 0.09) food intake and non-discretionary food intake (Z = 0.95, p = 0.35).
Dietary recall responses in completers (baseline vs week 8)
Wilcoxon signed rank tests were run, to compare discretionary and non-discretionary food intake, from pre to post Be Well. There was a significant reduction in the number of discretionary foods consumed by individuals, from baseline to week 8 (Z = 4.91, p < 0.001, N = 46). Further, there was a significant increase in non-discretionary food intake overall, at the end of Be Well relative to baseline (Z = −2.97, p = 0.003).
Post-hoc pairwise Wilcoxon tests indicated that there were statistically significant reductions in consumption of takeaway foods, fried potatoes and chips, sugar sweetened beverages, crisps, sweet snacks, ice cream and confectionary and discretionary foods generally (all Z's > 2.79, p's < 0.0053; see Table 1). There was also a statistically significant increase in consumption of vegetables (Z = −4.98, p < 0.0001) from pre to post Be Well intervention (see Figure 1, and Table 2).
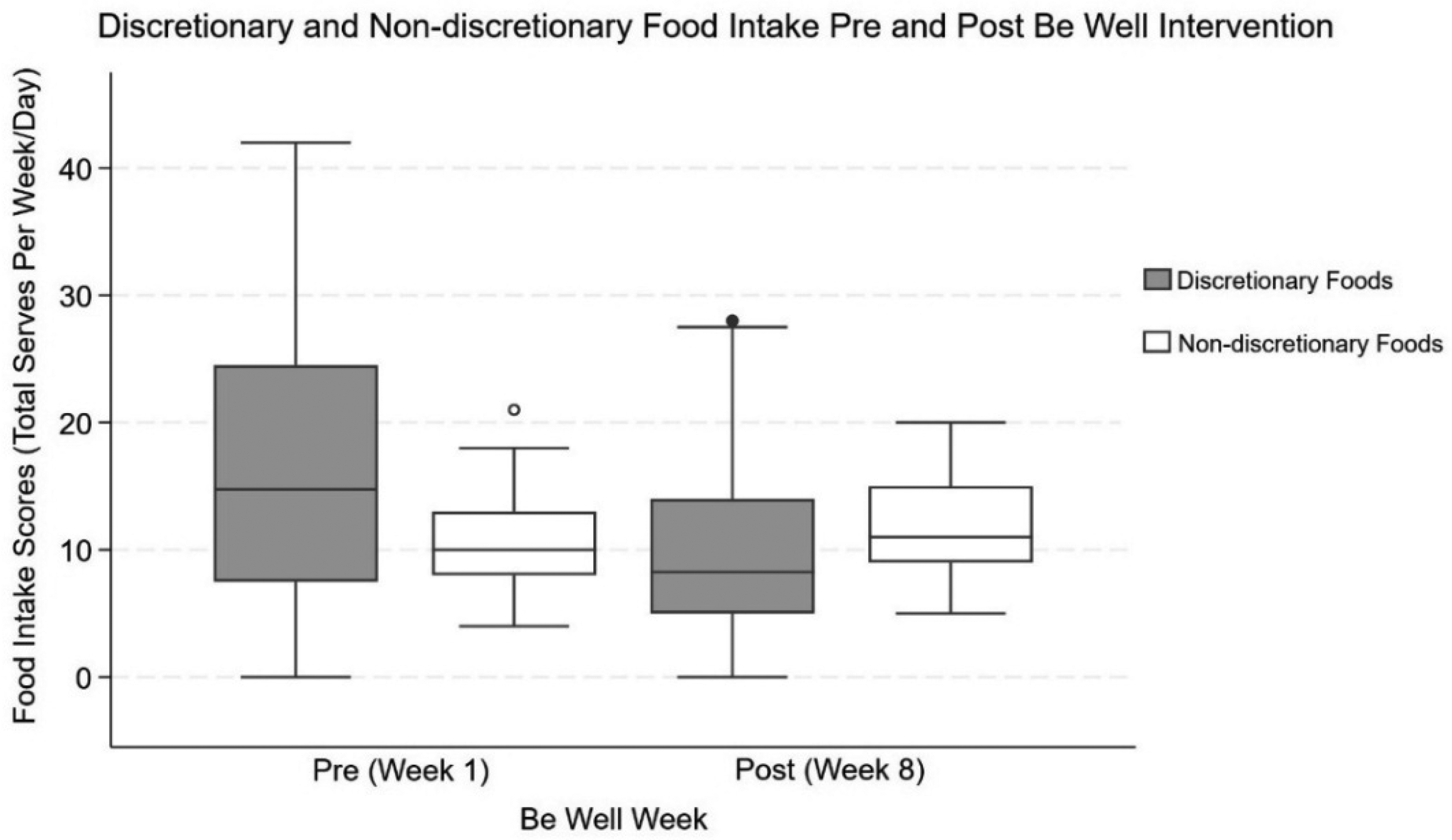
Discretionary and non-discretionary food intake, pre and post intervention. Higher scores, indicate greater consumption of non-discretionary foods per day, and discretionary foods per week.
Discretionary, non-discretionary and dietary behaviours descriptives.
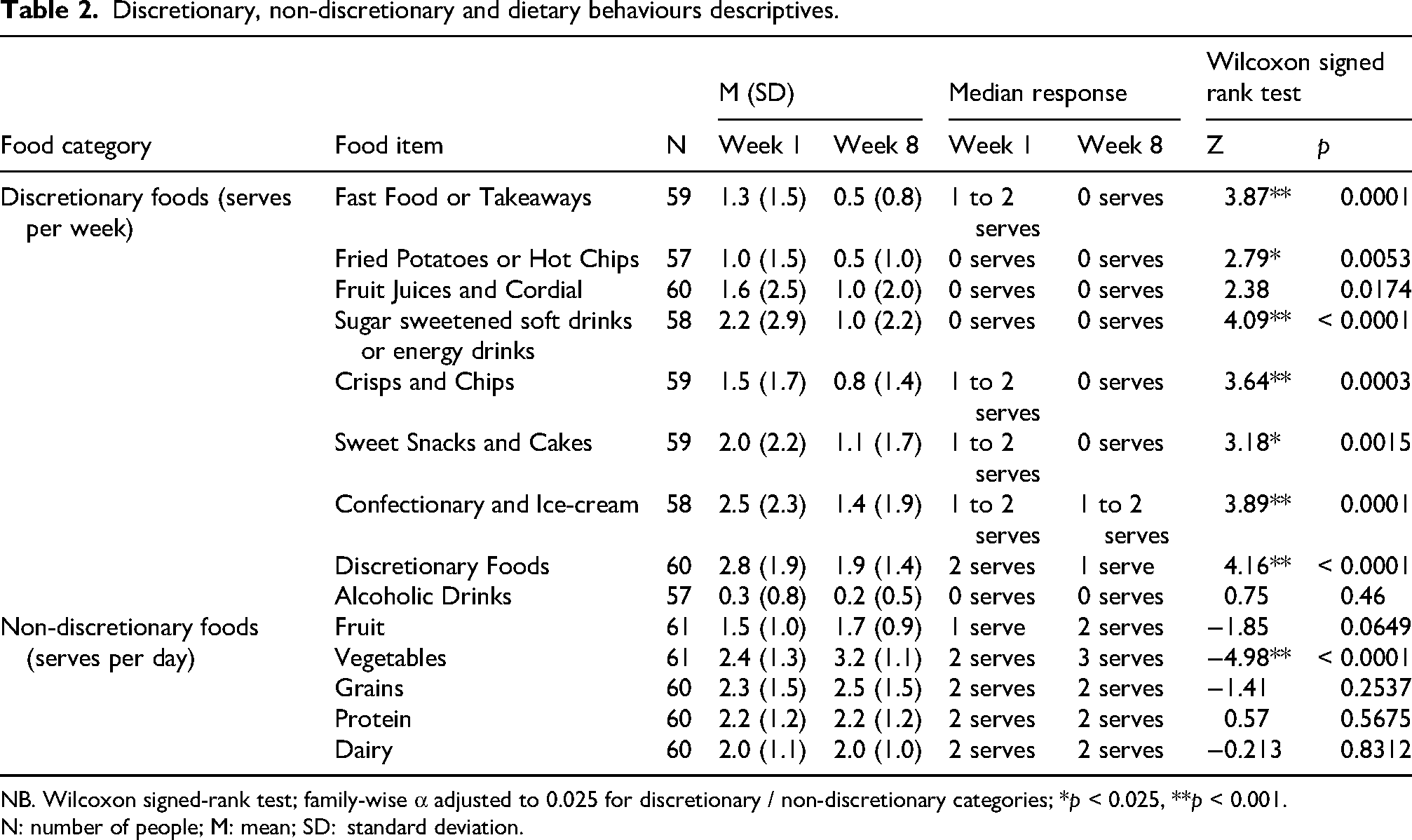
NB. Wilcoxon signed-rank test; family-wise α adjusted to 0.025 for discretionary / non-discretionary categories; *p < 0.025, **p < 0.001.
N: number of people; M: mean; SD: standard deviation.
Anthropometry (weight, BMI) results
Baseline (completers vs non-completers)
Mann-Whitney U-tests were conducted to compare completers and non-completers in their baseline weight. There was no significant difference in the baseline BMI of completers versus non-completers (Z = 0.58, p = 0.56), nor any significant difference in the weight between completers and non-completers (Z = −0.75, p = 0.45, see Table 3 for descriptives).
Baseline body weight descriptives for the total cohort, completers and non-completers.
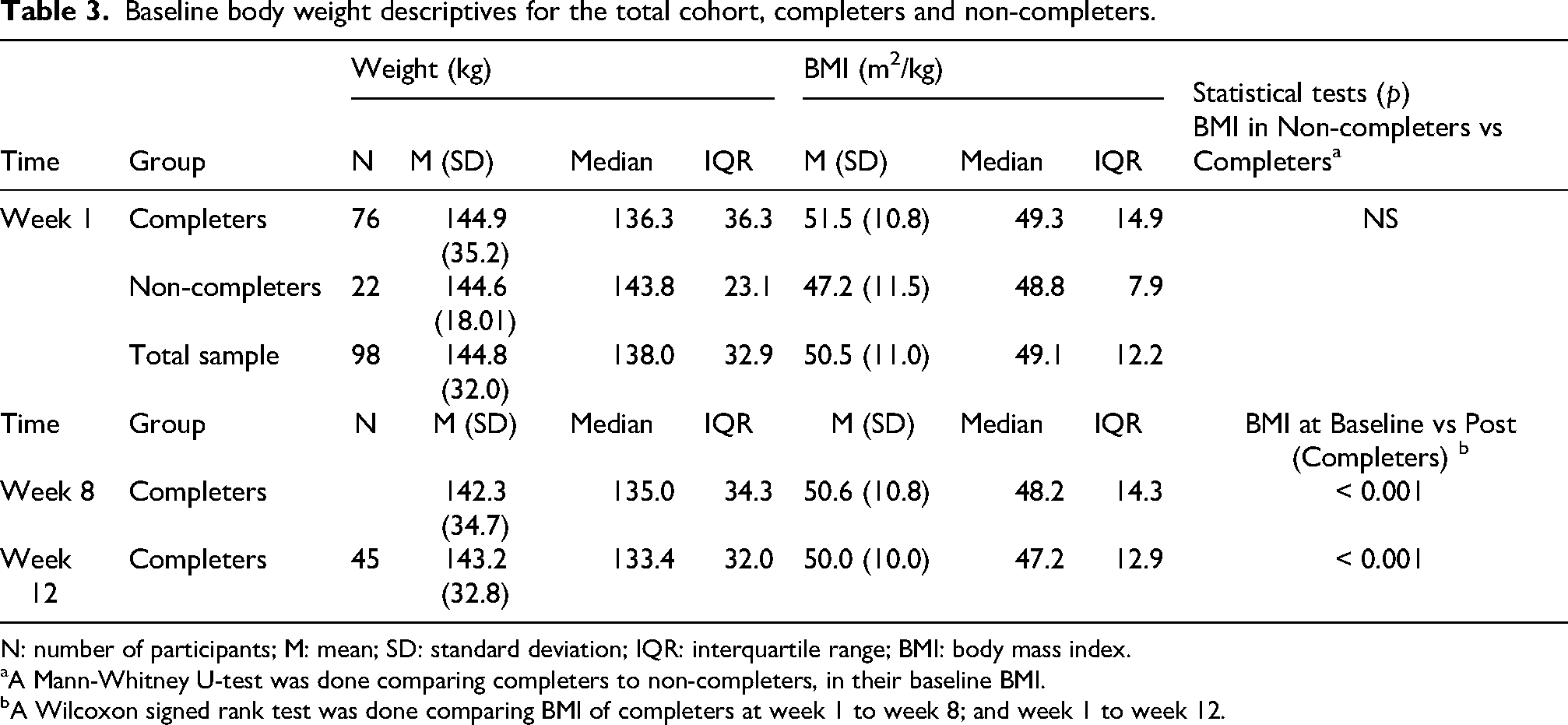
N: number of participants; M: mean; SD: standard deviation; IQR: interquartile range; BMI: body mass index.
A Mann-Whitney U-test was done comparing completers to non-completers, in their baseline BMI.
A Wilcoxon signed rank test was done comparing BMI of completers at week 1 to week 8; and week 1 to week 12.
Completers (baseline vs week 8 and week 12)
Wilcoxon signed rank tests were done to compare baseline BMI to BMI at 8 weeks and 12 weeks, in individuals who completed Be Well. BMI at 8 weeks was significantly lower than their BMI at week 1 (i.e. baseline; Z = 5.60, p < 0.001). Further, BMI at 12 weeks post intervention was significantly lower than BMI at week 1 (Z = 5.44, p < 0.001; see Table 3 for descriptives).
Results related to self-reported depression, anxiety and stress (DASS-21)
DASS-21 (completers vs non-completers)
The DASS-21 was completed at baseline by 36 participants (32 completers and 4 non-completers). A Mann-Whitney U-test was run to determine if there were any differences in baseline DASS-21 scores between completers and non-completers. No statistical difference was found between completers and non-completers in their total DASS-21 scores (Z = −0.48, p = 0.65). There were also no significant differences in baseline stress, anxiety and depression DASS-21 subscale scores between completers and non-completers (all Z's < −.53, p's > 0.62). At baseline (week 1), approximately one-third of the sample had severe or extremely severe levels of anxiety, stress, and depression. See Table 3 for descriptives.
DASS-21 completers (baseline vs week 8)
There were 14 completers who repeated the DASS-21 at 8 weeks post Be Well. Wilcoxon signed rank tests were done to compare baseline DASS-21 scores, to DASS-21 scores in week 8, in individuals who completed Be Well. There was significantly lower stress, and depression scores – that is, improvement in self-reported stress (Z = -2.85, p = 0.004), and depression scores (Z = 2.65, p = 0.008; family wise alpha set at 0.05/3) – from week 1 (baseline) to week 8 (post intervention) in these individuals (see Table 3). In terms of self-reported anxiety, while scores here tended to decrease, this decrease was not statistically significant (Z = 1.96, p = 0.051); see Table 4 for descriptives
DASS-21 results.
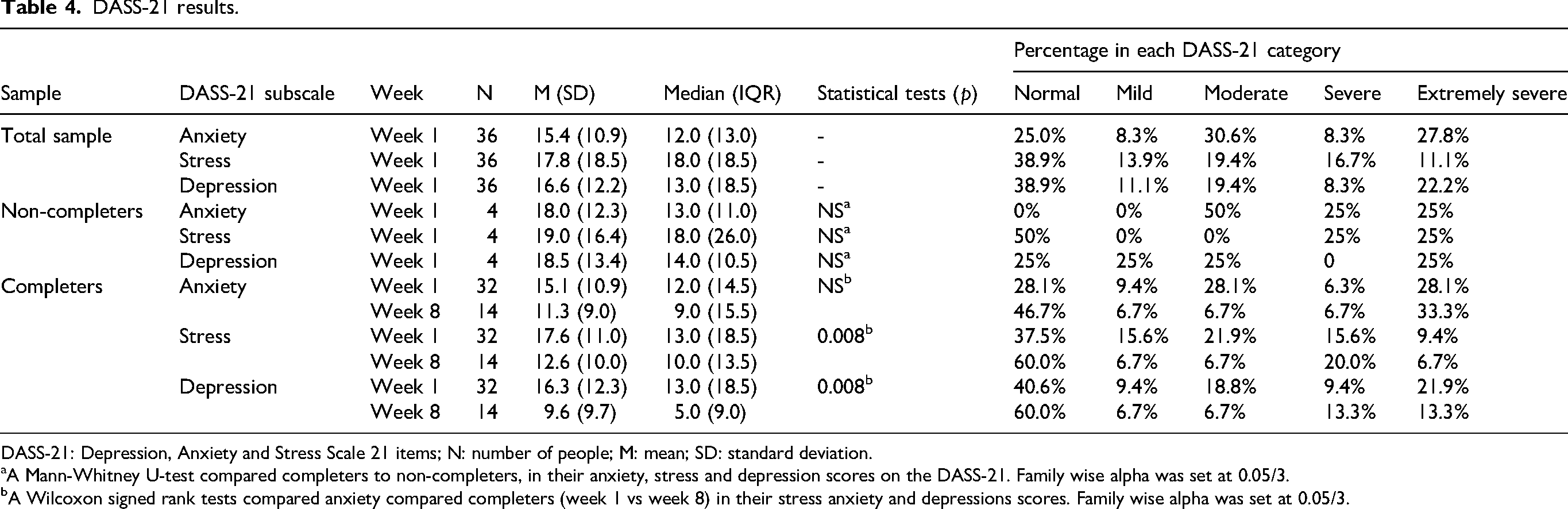
DASS-21: Depression, Anxiety and Stress Scale 21 items; N: number of people; M: mean; SD: standard deviation.
A Mann-Whitney U-test compared completers to non-completers, in their anxiety, stress and depression scores on the DASS-21. Family wise alpha was set at 0.05/3.
A Wilcoxon signed rank tests compared anxiety compared completers (week 1 vs week 8) in their stress anxiety and depressions scores. Family wise alpha was set at 0.05/3.
Be Well evaluation
There were 55 participants who completed an evaluation form post Be Well. This feedback is summarised in Table 5. Overall, the positive feedback can be summarised thematically into two themes – that is, ‘improved dietary self-efficacy’, and ‘social connectedness’. Feedback for suggested improvements can be summarised into the theme ‘enhancing program logistics’ (see Table 5).
Participant evaluation form responses post Be Well (N = 55).
Discussion
This is the first study to examine the efficacy of an 8-week publicly funded multidisciplinary group-based intervention, termed Be-Well, on dietary, mood and weight outcomes in individuals living with severe obesity. The individuals who were referred to the intervention had complicated and severe obesity, tended to reside in an area defined as moderately disadvantaged, and typically had several chronic health complications, as well as polypharmacy. To assess the effectiveness of the Be Well intervention in this cohort, we examined changes in self-reported dietary behaviours, mood and BMI, between pre and post intervention. The intervention led to significant improvements in dietary behaviours, improvements in mood and reductions in BMI – notable as the intervention was only 8 weeks, in a cohort with complex medical needs. These results provide support for the use of multidisciplinary group interventions as a first step for treatment of severe obesity.
The Be Well intervention used in this study was based off multidisciplinary approaches in obesity management (Anderson et al., 2001; Atlantis et al., 2018, 2019; Bischoff et al., 2017; Cannon et al., 2016; Chen et al., 2022; Donini et al., 2009; Lam et al., 2024; Sharaiha et al., 2023). As a consequence, the intervention used cognitive behavioural therapy strategies to promote adherence to lifestyle modifications – that is, behavioural activation to improve mood and motivation through exercise (e.g. activity planning, increasing incidental exercise), as well as sustainable dietary improvements (e.g. menu planning, label reading, improving nutritional literacy). In addition, cognitive strategies were used to manage health and facilitate adherence to exercise and dietary changes (e.g. goal setting, setting graded physical activity and strength based exercise goals, and promoting alternative healthy behaviours during negative mood states).
In line with Be Well's aim and multidisciplinary approaches, we observed statistically significant improvements in dietary patterns from pre to post intervention, in patients with severe obesity. There was almost a 50% mean reduction in consumption of discretionary foods and beverages – that is, foods/drinks that are high in saturated fat, sugar or salt, and low in fibre and micronutrients (Sui et al., 2017) – from pre to post intervention. Further, there was significant increase in daily serves of vegetables. These data suggest that, overall, individuals had an improved diet after attending Be Well. The reduction in discretionary food intake that occurred after an 8-week group intervention is important, given that diets comprised primarily of discretionary foods have deleterious effects on physical-, psychological- and cognitive-health (see Francis and Stevenson, 2013; Kopp, 2019; López-Taboada et al., 2020, for reviews).
Further, there were significant improvements in self-reported mood – that is, reductions in subjective depression and stress – in patients with severe obesity from their baseline to the end of the Be Well intervention. While a small sample, it is interesting to speculate why improvements in subjective depression and stress occurred over a short period. One reason may be that mood improvements were driven by other observed changes – for example, improved dietary behaviours, weight – and/or behavioural activation, which are associated with reductions in depression (Crawford and Henry, 2003; Swainson et al., 2023). Another, potential explanation for improvements in self-reported mood is that they were facilitated by an greater sense of social connectedness and health literacy (as based of qualitative feedback).
Finally, we observed statistically significant reductions in BMI and weight, at 8 weeks, and sustained up to 12 weeks post baseline. In line with this, Atlantis et al. (2019) found that patients with severe obesity who attended a 12-month service from a multidisciplinary team in Australia, had sustainable improvements in BMI, and in measures of physical endurance/strength (Atlantis et al., 2019). In line with Atlantis et al. (2019) – who reported a 1.7 (kg/m2) average BMI change in patients with severe obesity attending a multidisciplinary Australian obesity clinic – we found a 1.5 (kg/m2) average BMI change, from baseline to post Be Well (12 weeks) in the Be Well completers. This indicates that the efficacy of Be Well – a group-based intervention – may be comparable to multidisciplinary and individualised treatment of severe obesity offered at specialist clinics. Further, long-term (e.g. ∼12 month) attendance at our multidisciplinary service, which begins with Be Well, led to reductions in emergency department presentations and acute hospital admissions in individuals with severe Class 3 obesity (Williams et al., 2023). Similar results have been reported for individuals with Class 2 and Class 1 obesity (Chen et al., 2022; Donini et al., 2009).
As noted above, one difference between our study and past intervention studies examining multidisciplinary treatment efficacy for severe obesity in Australia (Atlantis et al., 2019; Chen et al., 2022) pertains to the group-based nature of Be Well. There are several benefits of using a group intervention as the first stage for treatment of severe obesity. First, group interventions are more cost-effective than individual appointments, due to the lower clinician to patient ratio, and, because disengagement from group therapy would be less costly than non-attendance to individual appointments. The use of cost-saving strategies for severe obesity treatment is particularly important, as severe obesity places significant economic burden on society and disproportionately effects individuals from lower socioeconomic backgrounds (Anekwe et al., 2020). Second, more people are given treatment in a group intervention – which is particularly important as, in Australia, patients with severe obesity are waiting > 2 years, and there are more than 300 patients on waitlists for tertiary obesity services (Atlantis et al., 2018). Finally, as per feedback from patients, group interventions serve as an important stigma reducing measure – that is, patients begin to feel less isolated and more supported by others living with similar health complications.
There are few limitations of the current study which are now considered in relation to their impact on the interpretation of the study's results. The first limitation of the current study is that there was a 39% attrition rate from the initial registered sample. The attrition rate was, however, only 21% if individuals had attended a single Be Well session. Thus, some level of attrition came from barriers to attending the obesity clinic overall, rather than the group intervention per se. Indeed, a 21% attrition rate is relatively low, especially when considering studies report a range of 30–81% attrition in weight management programs for obesity – and that this rate tends to be higher as the severity of obesity increases (Leung et al., 2017). This suggests the current study sample was – at least relative to other studies – a more generalisable cohort of individuals living with complicated and severe obesity. Relatedly, another limitation was that an incomplete attrition bias analysis was conducted. While we examined if the non-completers differed at baseline to completers, more extensive analyses – examining demographic, medical and psychosocial differences between completers and non-completers – is warranted in future studies, to ascertain if completers have clinically different needs, and profiles to non-completers.
The third limitation is the small sample size used to the effect of Be Well on self-reported depression, anxiety and stress. As the DASS-21 was only administered on a small subset of the cohort, results pertaining to improvements in mood post Be Well should be interpreted with caution and require replication with a larger sample size to determine their reliability. Notably, the reason for the low response rate for the DASS-21 was primarily because it was only administered to two of the four Be Well groups, rather than a participant selection bias introduced from the measure itself.
A fourth limitation was that a non-standardised and self-report dietary survey was used to measure food intake. While the scale was based off extant guidelines, future studies validating the food intake scale used in the current study against existing – longer form and validated food frequency surveys, and food diaries (ABS, 2024; New South Wales Health, Population Health Surveys, 2024) – are warranted to ascertain the scale's psychometric properties. Fifth, a relatively short follow-up period (12 weeks) was used to measure weight changes making it difficult to ascertain longer term changes, due to Be Well. Twelve weeks was the last follow-up point for weight, because after this time, patients receive individualised treatment for obesity management (i.e. individual appointments with endocrinologists, diabetes educators, dietitians, physiotherapists and psychologists). Thus, it would be difficult to ascertain if weight maintenance post 12 weeks was due to Be Well and/ or the individualised treatment.
Finally, it remains unclear how much the changes to diet, mood and health, were due to the intervention per se, as opposed to time, or simply being in contact with a health service – as there was no control group. Of note, recent unpublished data indicates that ∼31% patients attending the FMHS, report gaining 5–10 kg in the 6 months prior to attending (December, 2024) – despite being in contact with the FMHS during this time. This suggests that the health and weight changes are unlikely due to contact with the service or time itself. Nevertheless, future studies using waitlist control groups are warranted, to reveal the unique effects of group-based multidisciplinary interventions in severe obesity management.
Based off the current findings, several future studies are recommended to address the extant study's limitations and to extend implications. First, attrition from group-based multidisciplinary services should be investigated using mixed designs. This would further the understanding of the demographic, biological (medical profile), psychological (mental health related, cognitions, expectations etc) and social (socioeconomic status, financial security, life stressors) predictors of attrition from multidisciplinary severe obesity management. Second, future studies are required to determine the psychometric properties of the food intake survey used in this study, by validating it against extant and lengthier, food-frequency scales and diaries (ABS, 2024; New South Wales Health, Population Health Surveys, 2024). As it is a relatively short measure of discretionary and non-discretionary food intake, if validated, the food intake survey could allow for efficient collection of diet quality in clinical settings. Third, studies comparing group-based interventions – such as Be Well – to control (waitlist control) and individualised multidisciplinary treatment, are warranted to understand the clinical and economic efficacy of group-based interventions in severe obesity.
Taken together, we present the findings from the first study to evaluate the effectiveness of the Be Well intervention – that is, a lifestyle and behavioural group intervention – which acts as a first step in the team's multidisciplinary treatment of severe obesity at the Family Metabolic Health Service. As such, the data come from a real-world specialist obesity service in Australia and provide promising evidence for the use of a group-intervention as an initial and resource-efficient means to improve health behaviours and weight outcomes, in individuals living with severe obesity. Future directions include scaling up Be Well in resource limited settings through virtual adaption – for example, developing self-paced modules from the content in Be Well, which could be delivered to multidisciplinary obesity services and outpatient diabetes services to promote lifestyle modifications in severe obesity. Future research is also needed to better understand barriers to engagement with multidisciplinary specialist obesity services and the predictors of treatment efficacy.
Supplemental Material
sj-docx-1-nah-10.1177_02601060261420684 - Supplemental material for Multidisciplinary and group-based interventions as the first step for improving dietary and health behaviours in severe obesity
Supplemental material, sj-docx-1-nah-10.1177_02601060261420684 for Multidisciplinary and group-based interventions as the first step for improving dietary and health behaviours in severe obesity by Supreet Saluja, Gabrielle Maston Suthern, Sophia Kwan, Sally Badorrek, Emma Walker, Rebecca Teng Jing Yap, Divia Mohandas, India Grace Shepherd, Rosalynn Wen and Kathryn Williams in Nutrition and Health
Supplemental Material
sj-docx-2-nah-10.1177_02601060261420684 - Supplemental material for Multidisciplinary and group-based interventions as the first step for improving dietary and health behaviours in severe obesity
Supplemental material, sj-docx-2-nah-10.1177_02601060261420684 for Multidisciplinary and group-based interventions as the first step for improving dietary and health behaviours in severe obesity by Supreet Saluja, Gabrielle Maston Suthern, Sophia Kwan, Sally Badorrek, Emma Walker, Rebecca Teng Jing Yap, Divia Mohandas, India Grace Shepherd, Rosalynn Wen and Kathryn Williams in Nutrition and Health
Supplemental Material
sj-docx-3-nah-10.1177_02601060261420684 - Supplemental material for Multidisciplinary and group-based interventions as the first step for improving dietary and health behaviours in severe obesity
Supplemental material, sj-docx-3-nah-10.1177_02601060261420684 for Multidisciplinary and group-based interventions as the first step for improving dietary and health behaviours in severe obesity by Supreet Saluja, Gabrielle Maston Suthern, Sophia Kwan, Sally Badorrek, Emma Walker, Rebecca Teng Jing Yap, Divia Mohandas, India Grace Shepherd, Rosalynn Wen and Kathryn Williams in Nutrition and Health
Supplemental Material
sj-docx-4-nah-10.1177_02601060261420684 - Supplemental material for Multidisciplinary and group-based interventions as the first step for improving dietary and health behaviours in severe obesity
Supplemental material, sj-docx-4-nah-10.1177_02601060261420684 for Multidisciplinary and group-based interventions as the first step for improving dietary and health behaviours in severe obesity by Supreet Saluja, Gabrielle Maston Suthern, Sophia Kwan, Sally Badorrek, Emma Walker, Rebecca Teng Jing Yap, Divia Mohandas, India Grace Shepherd, Rosalynn Wen and Kathryn Williams in Nutrition and Health
Supplemental Material
sj-docx-5-nah-10.1177_02601060261420684 - Supplemental material for Multidisciplinary and group-based interventions as the first step for improving dietary and health behaviours in severe obesity
Supplemental material, sj-docx-5-nah-10.1177_02601060261420684 for Multidisciplinary and group-based interventions as the first step for improving dietary and health behaviours in severe obesity by Supreet Saluja, Gabrielle Maston Suthern, Sophia Kwan, Sally Badorrek, Emma Walker, Rebecca Teng Jing Yap, Divia Mohandas, India Grace Shepherd, Rosalynn Wen and Kathryn Williams in Nutrition and Health
Footnotes
Acknowledgements
We would like to thank staff who assisted in running the intervention and to all patients for their time and valuable contributions.
Ethical considerations and consent to participate
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Nepean Blue Mountains Local Health District Ethical Committee (dated 09/09/2022: 2020/ETH02108). A waiver of consent was obtained from all patients, to analyse de-identified data.
Consent for publication
A waiver of consent was obtained from all patients, to analyse de-identified data and for publication of deidentified data.
Author contributions
Author KW had oversight of the project, formulated the research questions, and assisted in original and revised manuscript write up, proofing and supervision. Authors SS and GMS analysed data, formulated the research questions and wrote the MS. Authors SK, and SB, assisted in designing the study, execution and revision of the MS. Authors EW, RY, DM, IS and RW assisted in execution of the study and proofing the MS.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
As data are sensitive and can be used to identify patients, data is not made available. Only non-identifiable data for non-sensitive information will be made available on reasonable request.
Supplemental material
Supplemental material for this article is available online.