
Abstract
Background
Children under 36 months experience rapid growth, making proper nutrition crucial for their development and health. Early Childhood Development (ECD) centres play a key role in meeting these needs when parents are unavailable. Children spend 5–10 h daily in these centres, where they receive up to 70% of their nutritional needs.
Aim
This study aimed to develop an anthropometric profile of children under 36 months and assess food provisioning in ECD centres in Tutaleni Informal Settlement, Walvis Bay, Namibia.
Methodology
A cross-sectional, observational design with a quantitative approach was used. A census sampling strategy selected 110 children from 13 ECD centres. Demographic and anthropometric data were collected, cleaned, and analysed using Statistical Package for the Social Science (SPSS) version 27. WHO Anthro software version 3.2.2.1 was used to assess growth indices.
Summary
The study found that stunting affected 8.2% of children, predominantly boys and those aged 12–23 months. Wasting and overweight each had a prevalence of 5.5%, while underweight was 4.5%. None of the ECD centres provided meals; all children brought food from home, commonly yoghurt (100%), bread with jam (92.3%), pasta (92.3%), fruits, cooked rice (84.6%), and porridge (76.9%). Feeding mainly involved bottles (92.3%), with commercial formula used more frequently (76.9%) than expressed breastmilk (23.1%). These findings highlight ongoing malnutrition concerns in the ECD centres, stressing the need for targeted interventions, including caregiver and parental training on optimal feeding, to improve food environments and support healthy child development.
Keywords
Introduction
Childhood malnutrition is a significant public health issue with profound effects on child survival, growth, and development. According to the 2025 Joint Child Malnutrition Estimates by UNICEF, World Health Organization (WHO), and the World Bank Group, 23.2% of children under five were stunted, 6.6% were wasted, and 5.5% were overweight. Significantly, Africa bore a substantial share of this burden, with 43% of all children affected by stunting living on the continent. Additionally, more than 27% of children suffering from wasting and over 27% of those affected by overweight were also found in Africa (UNICEF, 2025). According to Johannes (2024), Namibia reported that 22.7% of children under five were stunted, 7.1% were wasted, and 13% were underweight (Johannes, 2024). However, limited data on Infant and Young Child Feeding practices hampers effective intervention efforts.
Malnutrition encompasses both undernutrition, including stunting, wasting, and micronutrient deficiencies, and overnutrition, which includes overweight and obesity (WHO, 2024). Its causes are multifaceted, involving inadequate dietary intake, infections, and suboptimal childcare practices (Katoch, 2022). The WHO and UNICEF recommend exclusive breastfeeding for the first 6 months, followed by complementary foods alongside breastfeeding until at least 24 months. Early introduction of complementary foods or replacing breastmilk with commercial milk formula (CMF) increases the risk of malnutrition and early death (MoHSS, 2021).
Infants and young children younger than 36 months are at a crucial stage for rapid physiological growth and development (WHO, 2024). At this stage, appropriate feeding plays a vital role in determining their normal growth, development, and overall health. When mothers return to work, Early Childhood Development (ECD) centres often assume responsibility for feeding children. These centres provide up to 70% of a child's daily nutritional intake, making food provisioning practices within ECD centres critical to child health (Harton and Myszkowska-Ryciak, 2018). ECD centres, however, often face challenges such as overcrowding and poor hygiene, increasing the risk of infections that can exacerbate undernutrition (Muniandy et al., 2020). Globally, daycare attendance has been linked to malnutrition due to inadequate feeding practices and insufficient caregiver knowledge (Muluye et al., 2020). Despite this, there is limited data on malnutrition including among children attending daycare in Namibia. This study aimed to address these gaps and provide data to inform targeted nutrition interventions in Namibian ECD centres.
Methodology
Study design
This study applied an observational, cross-sectional design to assess ECD centres and children under 36 months in Tutaleni Informal Settlement, Walvis Bay, from February to April 2024. Data were collected, analysed, and interpreted in relation to the study objectives and population context.
Study location
Namibia, located in Southern Africa, shares borders with Angola, Zambia, South Africa, Botswana, and the Atlantic Ocean. With a population of approximately 3 million, it is a middle-income country marked by significant inequality and poverty (Namibia Statistics Agency, 2023). Walvis Bay, the largest harbour town on the western coast, had a population of 102,704 in 2023 (Namibia Statistics Agency, 2023).
Study setting and target population
The study was conducted in Walvis Bay town, the fishing industry's hub, which employs around 16,000 residents (Haimbala and Ambi, 2020). Many working mothers leave their children at daycare centres for 5–10 h daily. In 2016, Namibia had 38,802 children aged 0–5, with 24.6% attending ECD centres (Ngololo Kamara et al., 2018, NSA, 2017). The Erongo region had the highest proportion (37.7%). By 2018, 2934 ECD centres were registered with the Ministry of Gender Equality and Child Welfare (Ngololo Kamara et al., 2018). In Tutaleni Informal Settlement, the classification of ECD centres is less strict, with daycare centres (for 0–3 years) and pre-primary schools (3–6 years) often combined. The area had a total of 24 daycare centres.
Sampling and sample size
All ECD centres in Tutaleni Informal Settlement were contacted to invite participation in the study. Using Raosoft for sample size calculation, with a 95% confidence level, 5% margin of error, and 50% response distribution (Aedh, 2022), a sample of 157 children was initially determined. However, a census sampling strategy was used, including all eligible ECD centres within the settlement. Ultimately, 110 children from 15 ECD centres participated in the study.
Inclusion and exclusion criteria
Inclusion criteria (Early Childhood Development centres)
All ECD centres, represented by the head or designated staff member (caretaker/teacher), that provided written consent to participate were included in the study. The designated representative must have worked at the ECD centre for more than 6 months to ensure sufficient familiarity with the children, centre routines, and operational practices, which was essential for providing reliable and contextually accurate information.
Inclusion criteria (children)
Children under 36 months in daycare institutions were included in the study. Eligibility was verified using health cards for children under five, and those without cards were assessed at a later appointment.
Exclusion criteria (Early Childhood Development centres)
ECD centres were excluded if the head of the centre did not provide written consent, if the centre had no children under the age of 36 months enrolled, or if the designated staff had worked there for less than 6 months. Parents were not involved in providing responses. They were only required to provide written consent for their children to be assessed.
Exclusion criteria (children)
Children whose mothers/caregivers did not provide written consent were excluded.
Research instruments
Anthropometric measurements are used to assess human body size and composition. These measurements are straightforward, safe, and non-invasive, offering valuable information about nutritional status. Common anthropometric measurements include weight, height, mid-upper arm circumference (MUAC), head circumference, and skinfold thickness (Gibson, 2024). In this study, quantitative data were collected using two tools: a validated anthropometric assessment protocol, and an ECD food provisioning questionnaire, adapted with permission from the South African National Dietary Intake Survey (2021). Questionnaires and consent forms were initially compiled in English and then professionally translated into Oshiwambo, Herero, Damara, and Afrikaans.
Training and standardization
The data collection team included the principal investigator (PI), a registered nutritionist with a Master of Public Health Nutrition degree, and three research assistants (RAs), comprising one registered nurse, one enrolled nurse, and one nutritionist. The PI, selected RAs based on their community ties, local language proficiency (Oshiwambo), and relevant experience. RAs received 2 days of training on ethical procedures, nutrition assessment techniques (weight, height, MUAC), and administering questionnaires. They were compensated following Stellenbosch University's guidelines from the Health Research Ethics Committee (HREC).
Pilot study
A pilot study was conducted to pretest the study instruments. The study evaluated the accuracy, content, wording, and language of the tools, and standardized procedures for measuring weight, height, and MUAC. Two ECD centres (10% of the sample) participated in the pilot study, conducted from February 6–12, 2024. Changes made to the tools included rephrasing questions and correcting spelling errors. Data from the pilot study were excluded from the main study.
Data collection procedure
Data collection commenced on 19 February 2024, following the completion of the pilot study and refinement of data collection tools. Two teams were formed for fieldwork. These teams initially worked together to standardize procedures and then operated independently at assigned sites. The PI made initial appointments with ECD centre heads and arranged for parental consent prior to child assessments. Both verbal and written information about the study was provided to parents and ECD caretakers in their preferred languages.
On the day of data collection, anthropometric measurements for children aged 6–36 months were taken. Simultaneously, interviewer-administered food provisioning questionnaires were conducted with ECD caretakers or heads in person, in a language of their choice. Children identified with malnutrition or other health concerns were assessed and referred (through contact with a parent) to the nearest clinics for further care using a standardized referral form. The PI provided a daily field debriefings and regular supervision. The field data collection lasted until the 25 April 2024.
Quality control measures
To ensure the quality and credibility of the study, several strategies were implemented. These included pretesting the data collection tools to identify and correct errors, ambiguities, and irrelevant questions, thereby ensuring their validity (Hossan et al., 2025). The ECD questionnaires, previously validated by the South African NDIS, were used to assess food provisioning practices. The study's reliability was enhanced by involving a diverse research team, including nutritionists, nurses, and medical professionals. To minimize potential inter-collector bias and maintain consistency in data collection, RAs were trained and standardized, anthropometric tools were calibrated, and multiple measurements were taken, with averages calculated. Additionally, the PI provided ongoing field supervision and technical support, with daily debriefing to address any issues.
Data analysis and presentation
Data management was overseen by an experienced statistician. Questionnaires and protocols were reviewed for completeness and accuracy. Cases with missing values (including unanswered items and incomplete responses) were appropriately coded and treated as missing data. A coding sheet and prepopulated Excel sheet were developed, and a database was created in a Statistical Package for the Social Science (SPSS) version 27 according to the coding sheet. Data were entered, cleaned, and analysed. Anthropometric data were analysed using WHO Anthro software version 3.2.2.1, with growth standards applied to determine the three indices, including: weight-for-height z-score (WHZ), height-for-age z-score (HAZ), and weight-for-age z-score (WAZ) based on age and sex (Gibson, 2024, Shrestha et al., 2022).
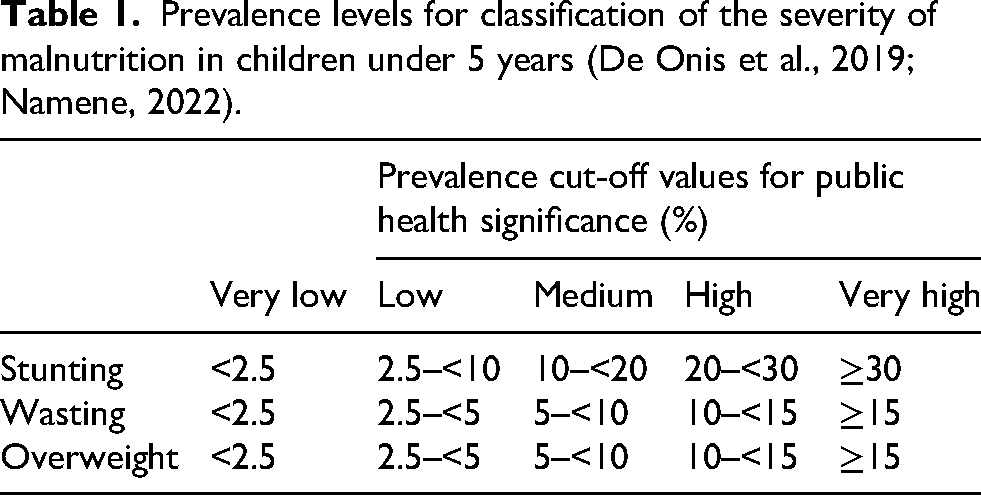
Malnutrition prevalence is classified according to WHO severity thresholds: low, medium, high, and very high for stunting, wasting, and overweight (Table 1) (Namene, 2022). Underweight is a composite indicator of both acute malnutrition and stunting or weight loss (FAO, 2021).
Prevalence levels for classification of the severity of malnutrition in children under 5 years (De Onis et al., 2019; Namene, 2022).
Data on meal items, feeding practices, health services, and educational materials were analysed as frequencies. SPSS was used for analysis, with descriptive statistics (mean, mode, median, SD) reported for continuous variables (e.g. age, weight, height, MUAC). Frequencies, counts, and proportions were used for categorical variables (e.g. gender, age group, food types). Graphs included frequency tables for continuous variables and bar graphs and tables for categorical variables.
Ethical consideration
This study adhered to ethical principles, with approval obtained from Stellenbosch University HREC (reference number: S23/09/206) and the Ministry of Gender Equality, Poverty Eradication and Social Welfare (MGEPESW), the custodian of the ECD Programme in Namibia. Permission was sought from ECD centre owners for participation. Informed consent was obtained from ECD caretakers and parents or legal guardians of children, with identification confirmed via identity documents and verbal affirmation. Participation was voluntary, and all information was used solely for research purposes. Confidentiality was maintained by using codes instead of real names, and anonymity was ensured by coding ECD centres and participants. No discrimination based on gender, race, tribe, social class, religion, or nationality occurred. Electronic data was securely stored on password-protected servers, primarily on Stellenbosch University OneDrive, while paper-based data was sent for storage at the Division of Human Nutrition. Participants received food portion-friendly plate and a cup as gifts and as tokens of appreciation. No risks were anticipated, but precautions were taken to ensure privacy and minimize discomfort.
Results
Sample population
As demonstrated in Figure 1, the study targeted a total of 17 ECD centres that had a capacity of 143 children aged 36 months and younger. During the participants’ recruitment, a total of 15 ECD centres consented (with a total capacity of 132 children) to partake in the study except two ECD centres (with a capacity of total of eight children). Then, two (10% of 15 ECD centres) (with eight children) took part in the pilot study, while 13 ECD centres with 124 children were recruited for the main study. The pilot study data were not pooled with the main study data. Among 124 child–parent pairs, n = 110 consented while 14 did not provide consent to participate.
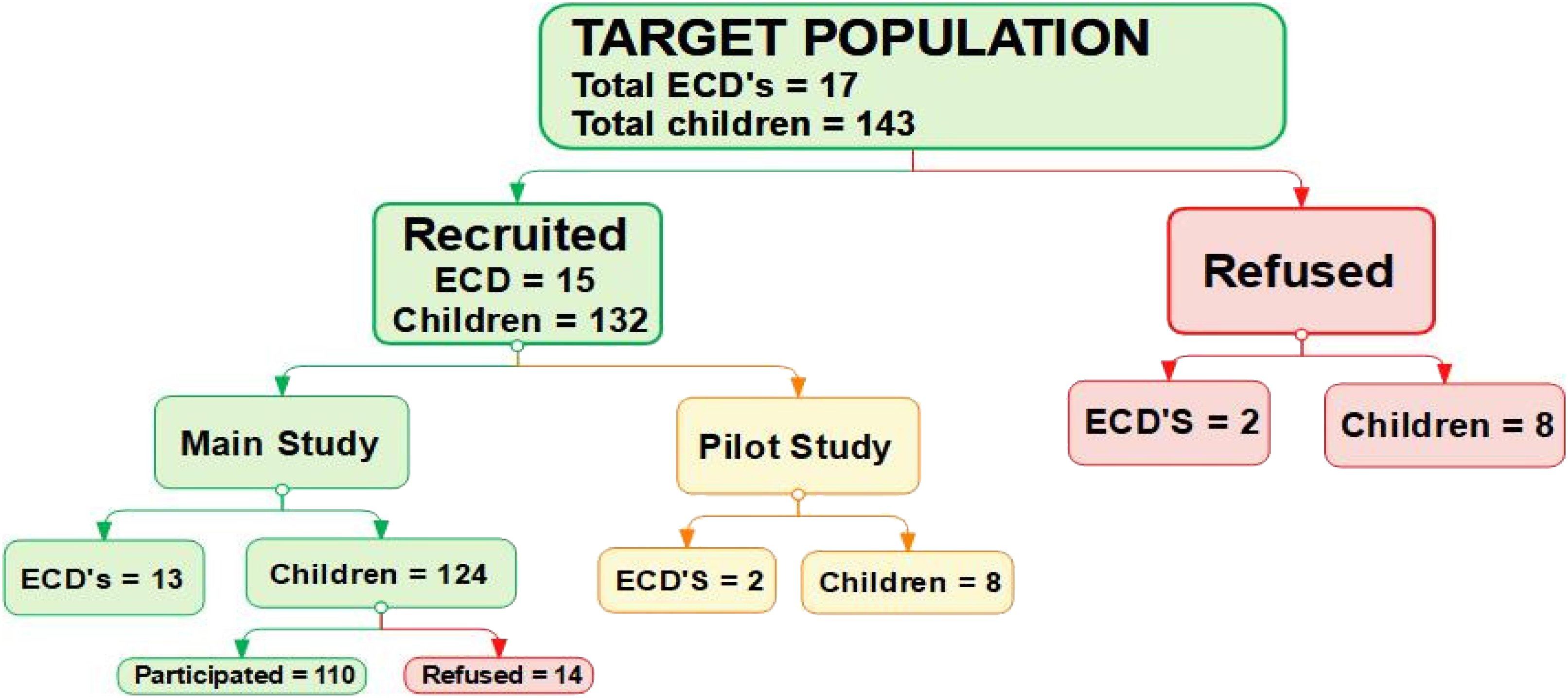
Schematic chart of an inclusion and exclusion process during field data collection in the ECD centre. ECD: Early Childhood Development.
Demographic indicators
As shown in Table 2, the study included 110 children, with a nearly even gender distribution: 50.9% boys (n = 56) and 49.1% girls (n = 54). Most children were in the older age category (≥24 months, n = 49; 44.5%), while fewer were in the younger groups, particularly <6 months (n = 11; 10%). All ECD caretakers were female, with most under 30 years old (n = 5; 38.5%), and one over 50 years old (n = 1; 7.7%). Over half of the caretakers had completed secondary education (n = 7; 53.8%), and 23.1% (n = 3) had tertiary education. More than half (n = 7; 53.8%) had worked at the ECD centres for more than 5 years, and 84.6% (n = 11) had never received child feeding training.
Demographic information of the participants and the characteristic of ECD centres.
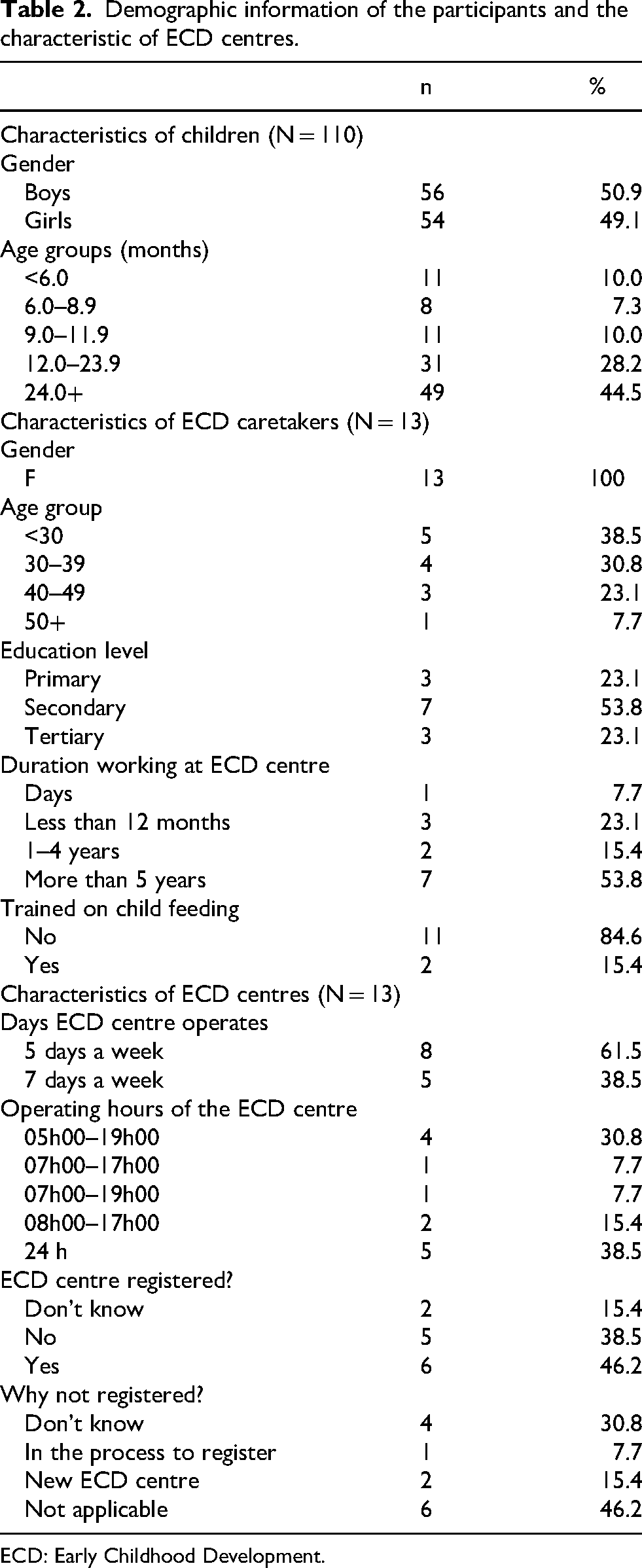
ECD: Early Childhood Development.
Regarding the ECD centres, most operated 5 days a week (n = 8; 61.4%), with a few open 7 days a week (n = 5; 38.5%). Operational hours varied, with 38.5% (n = 5) open 24 h a day. Six centres (46.2%) were registered with the MGEPESW, while five (38.5%) were not registered, citing reasons such as being “new” or in the registration process.
The anthropometrical profile of children attending Early Childhood Development centres
Anthropometric status of the children
The WHZ results revealed that 5.5% (n = 6) of the children were wasted, including 4.5% (n = 5) severely wasted and 0.9% (n = 1) moderately wasted. Overweight was observed in 5.5% (n = 6) of the children, with no cases of obesity. Regarding HAZ, 8.2% (n = 9) were stunted, with 0.9% (n = 1) severely stunted and 7.3% (n = 8) moderately stunted. For WAZ, 4.5% (n = 5) were underweight, including 3.6% (n = 4) severely underweight and 0.9% (n = 1) moderately underweight. Additionally, 103 children aged 6 to 36 months were assessed for MUAC as a supplementary measure of wasting, complementing WHZ. MUAC measurements indicated that 2.9% (n = 3) of the children had moderate acute malnutrition, none (n = 0) had severe acute malnutrition, and the majority, 97.1% (n = 100), were classified as normal. The most common form of malnutrition was stunting (8.2%), while underweight was the least prevalent (4.5%).
Children referred due to health conditions
During data collection, 18.2% (n = 20) of children were identified with health conditions and referred to the nearest primary health facility. Their anthropometric measurements were included in the analysis. The highest proportion were those presented with malnutrition (n = 13; 65%), followed by diarrhoea (n = 4; 20%), skin conditions (n = 2; 10%), and one child was diabetic (on insulin treatment) (n = 1; 5%).
The prevalence of malnutrition by gender, age and health condition
The results show that 26 out of 110 children presented with various types of malnutrition, including stunting, wasting, underweight, and overweight. The prevalence of malnutrition was compared by gender, age group, and health condition. Wasting and overweight were equally distributed between genders, while stunting was more common in boys (n = 6; 66.7%) and underweight was more prevalent in girls (n = 3; 60%). The highest prevalence of wasting was observed in children aged 12 months and above, while stunting and underweight were most common in the 12–23 months age group (n = 5; 55.6% and n = 2; 40.0%, respectively). Overweight was most prevalent in children aged 24 months and above. No malnourished children were found in the 6–8 months category (Figure 2).
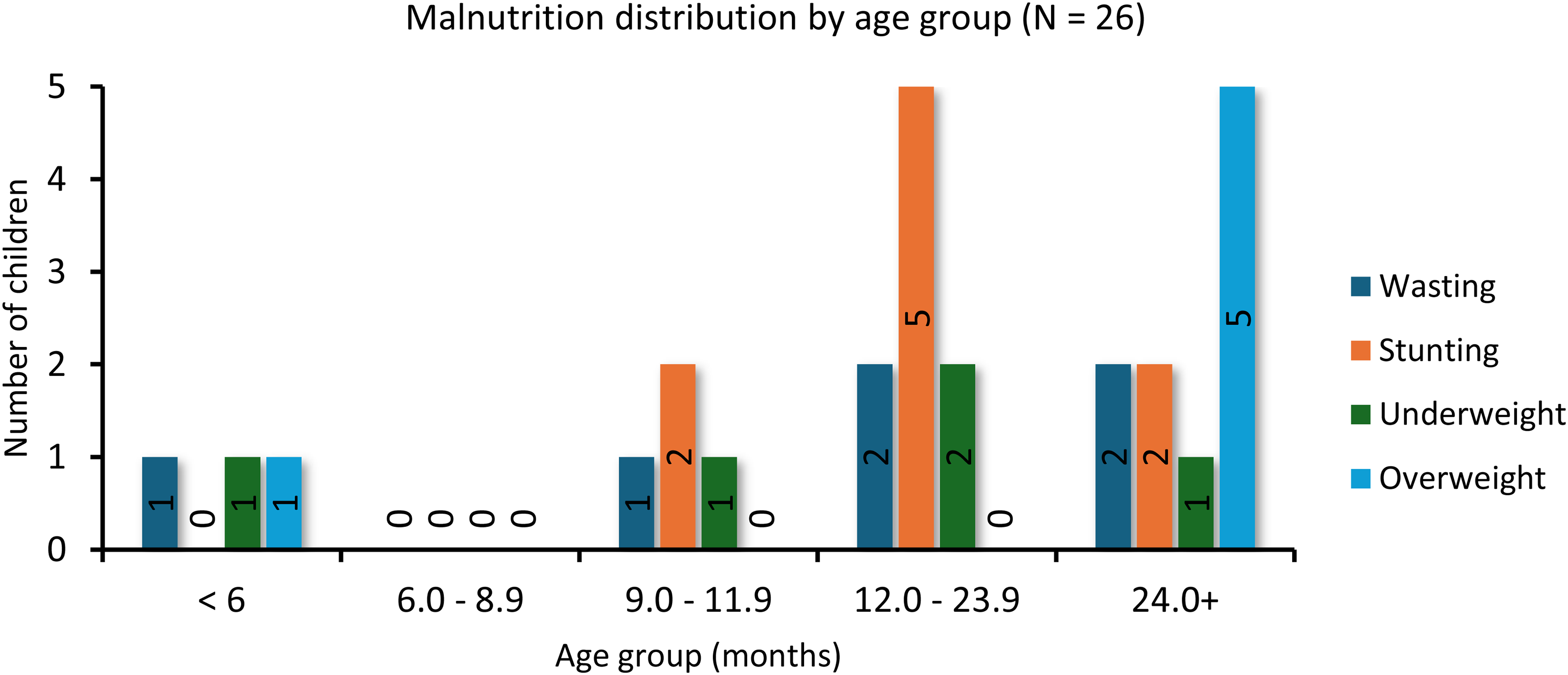
Distribution of different forms of malnutrition among age groups of children attending ECD centres. Among the 26 children aged 0–36 months, wasting was more prevalent in children aged 12 months and above, and similar in children within the 12–39 months and ≥24 months age category with 33.3%, respectively. Overall, the 12–23 months age category had the highest prevalence of stunting (n = 5; 55.6%) and underweight (n = 2; 40.0%). Overweight was highest in children aged 2 years and above. ECD: Early Childhood Development.
The status of food provisioning in Early Childhood Development centres
Food supply
All children (100%) brought food or snacks from home, as none of the ECD centres provided food. Teachers explained that some parents preferred to send their own food, and some centres lacked kitchens or adequate space for food preparation. Additionally, some parents could not afford higher fees that would include food services. None of the centres received food donations or had menus or food gardens.
Food brought from home
The food and beverages brought from home by children in the 24 h prior to the study mostly included yoghurt (n = 13; 100%), bread and jam (n = 12; 92.3%), pasta and noodles (n = 12; 92.3%), cooked rice, and fruits (n = 11; 84.6%). Other frequently reported foods were mahangu (pearl millet) porridge, maize meal soft porridge, red meat, beans, lentils (n = 10; 76.9%), and eggs and milk (n = 9; 69.2%). Chicken and fish were reported by eight centres (n = 8; 61.5%), while soya mince and margarine on bread were the least consumed (n = 2; 15.4%).
In terms of beverages, Oshikundu, a traditional Namibian cereal-based drink (Pohamba, 2021), was the most common (n = 11; 84.6%), followed by fruit juice (n = 10; 76.9%). Tea was the least consumed (n = 7; 53.8%). All children brought drinking water (n = 13; 100%), and when it was finished, most centres provided tap water (n = 10; 76.9%), with some offering bottled water (n = 3; 23.1%).
Feeding practices
The types of feeding practices for children under 12 months were assessed. Only one ECD centre (n = 1; 7.7%) reported that mothers returned during breaks to breastfeed, while most centres used bottles (n = 12; 92.3%) and fewer used cups (n = 3; 23.1%). The majority (n = 10; 76.9%) reported that parents sent pre-prepared food, while fewer prepared food on-site.
The results also present the types of foods supplied for children under 12 months, with most centres receiving more CMFs from mothers (n = 10; 76.9%) than expressed breast milk (EBM) (n = 3; 23.1%). One centre (n = 1; 7.7%) reported buying CMF when parents did not provide enough food.
Challenges faced by caretakers included children lacking appetite (n = 8; 61.5%), monotonous diets (n = 7; 53.8%), and inadequate food from some mothers (n = 6; 46.2%). To address these, caretakers used food as a reward (n = 7; 53.8%) or threat (n = 5; 38.5%).
Food preparation, handling, and storage
Of the 13 ECD centres, five caretakers (38.5%) prepared food brought from home, and six (46.2%) did so even when sick. Most centres (n = 11; 84.6%) had clean food preparation areas, with the majority using cold or hot water (n = 6; 46.2%) to wash children's utensils. Only one centre (n = 1; 7.7%) reported that parents preferred to wash the utensils at home. Most centres (n = 10; 76.9%) washed fruits and vegetables before feeding the children, while one (n = 1; 7.7%) never washed fruits.
Regarding food storage, one-third of the centres (n = 5; 38.5%) had fridges for perishable items, and more than a third stored food appropriately to prevent spoilage (Elsaed and Ibrahim, 2020). Close to two-thirds (n = 8; 61.5%) had working food reheating equipment (microwaves). Most centres (n = 12; 92.3%) covered the food during storage, and none had pests around food prep areas.
Health, nutrition education, hygiene, and sanitation
It was reported that in the past 12 months, four (30.8%) of the ECD centres were visited by nurse/healthcare workers to provide primary healthcare outreach services, including vitamin A supplementation, deworming treatment, clinical assessment, and MUAC measurement. Of the centres, two (15.4%) ECD staff reported that they were given health education by the nurses.
Discussion
The anthropometrical status of children attending Early Childhood Development centres
This study examined the anthropometric status of children in ECD centres, focusing on stunting, wasting, underweight, and overweight. Results revealed a low prevalence of stunting but medium concerns regarding wasting and overweight, indicating mixed nutritional status among the children. These indicators are essential for understanding the nutritional challenges faced by young children (Namene, 2022).
At national level in Namibia, in 2017, stunting (22.7%) was classified as a high public health concern, followed by underweight (13%). Wasting (7.1%) was considered as a medium concern, while overweight (4%) was classified a low (Johannes, 2024). In a similar context, a study conducted in Busia town, Busia County, Kenya, found the prevalence of wasting, stunting, underweight, and overweight among 53 children enrolled in a daycare centre to be 4.2%, 12.2%, 15.1%, and 22.9%, respectively (Makau and Thuku, 2024).
Compared to these settings, the current study showed lower prevalence rates of stunting, wasting, and underweight than the national averages but a higher prevalence of overweight. However, caution is necessary when comparing these figures, as this study had a smaller sample size focused on children under 3 years in a single geographic area, whereas national data generally encompass larger, more diverse populations including children under 5 years. In addition, malnutrition prevalence may also differ due to aspects such as the season and socio-economic characteristics (Namene, 2022).
Despite being classified as low public health concerns, stunting and underweight remain critical issues due to their long-term impact on children's growth, survival, and cognitive development (WHO, 2024). Stunting was more prevalent in boys, which is consistent with other studies (Sello et al., 2023). Wasting and underweight were most common in children aged 12–23 months, an age when children are more susceptible to infections and face nutritional challenges due to the transition from breastfeeding to complementary feeding (Namene, 2022, Tahangnacca et al., 2020).
Although overweight was classified as low prevalence in this study, it is a concern that should not be overlooked. The rising prevalence of childhood overweight aligns with global trends previously seen mainly in high-income countries (HICs) (Sello et al., 2023). Childhood overweight increases the risk of obesity in adulthood, which is associated with noncommunicable diseases such as diabetes, cardiovascular disease, cancer, and stroke (UNICEF, 2025).
Additionally, 18% of children were diagnosed with health conditions such as diarrhoea and skin infections, which were linked to higher rates of stunting, wasting, and underweight. Diarrhoea worsens malnutrition by reducing nutrient absorption (Komo, 2021). These findings stress the importance of integrating healthcare services into ECD centres, including routine healthcare worker visits for deworming, vitamin A supplementation, and health education (MoEAC, 2019).
In conclusion, this study highlights the dual burden of malnutrition in ECD settings, where both undernutrition and overnutrition pose significant challenges. It emphasizes the need for comprehensive interventions to address the nutritional needs of young children and strengthen healthcare outreach within communities.
The status of food provisioning in Early Childhood Development centres
This study highlights significant challenges in food provisioning within ECD centres. Despite the Namibian school feeding policy (MoEAC, 2019) recommending regular training for staff on meal planning and hygiene, most ECD caretakers in the study had never received such training. The lack of nutrition experts in these centres further limits their ability to plan balanced, nutritious meals. Similar issues are observed across many sub-Saharan African countries (Atinmo and Oyewole, 2016), where the shortage of qualified professionals hampers effective nutrition interventions (Elhady et al., 2023).
All children in the study brought food from home, with no centres utilizing food gardens or receiving donations, contrary to the policy that encourages registered centres to benefit from government support and school gardens (MoEAC, 2019). The food items brought included staple foods like bread, pasta, fruits, and protein-rich foods such as eggs and meat. However, these diets were often monotonous, raising concerns about nutrient diversity and potential undernutrition. The most common beverage was Oshikundu, a traditional Namibian drink, which aligns with the policy's encouragement of locally sourced foods. In contrast, other studies have reported tea and juice as popular beverages; these are typically high in sugar and energy-dense but offer little nutritional value, despite being inexpensive and palatable (Jannah, 2023).The findings of this study align with reports from HICs, where most daycare centres provide meals and use structured meal plans or menus, in contrast to many low- and middle-income countries (de Oliveira et al., 2022, Makau and Thuku, 2024, Sello et al., 2023).
A distinctive aspect of food provisioning in the ECD centres studied was the regular inclusion of local foods brought from home, a practice rarely reported in other studies. de Oliveira et al. (2022) recommends incorporating locally available foods to diversify menus and respect local food habits, which can improve nutritional quality and cultural relevance in these settings.
This study highlighted ongoing concerns regarding infant feeding practices, particularly the use of bottles and the reliance on CMF rather than EBM. Similarly, a study by Makau and Thuku (2024) found that a proportion of respondents (7.1%) reported using CMF, reflecting a trend that diverges from WHO recommendations. WHO discourages bottle feeding because of the challenges in maintaining hygiene and the increased risk of transmitting pathogens, instead promoting cup/soon feeding of EBM as a safer and more effective alternative to feeding from the breast (WHO, 2021). Additionally, the widespread use of CMF presents further complications, as aggressive marketing of CMF has been linked to higher rates of child morbidity and mortality, leading to global efforts such as the International Code of Marketing of Breastmilk Substitutes to regulate these products (WHO, 2024). Breastmilk remains the ideal source of nutrition, offering, among other benefits, essential nutrients and immune-supporting components vital for infant growth and development and should be promoted, protected, and supported (Fanzo and Davis, 2021, NAFSAN, 2024).
In conclusion, while there are some positive practices in food provisioning at ECD centres, significant gaps in training, food variety, and adherence to national guidelines remain. Addressing these issues is essential for improving children's nutritional health and overall well-being.
Limitations of the study
Limitations included challenges in accessing parents, the lack of menus and food provisioning in ECD centres, and financial constraints that reduced the sample size from 157 to 110 children. Obtaining parental consent was difficult but was addressed through strategies like visiting homes or workplaces. As the study was limited to one community, the results may not be generalizable to Walvis Bay or Namibia as it may introduce potential sampling bias (Hughes et al., 2021). Additionally, the study did not collect detailed dietary intake data or assess children's lunchboxes individually, which limits the ability to evaluate the nutritional adequacy of the foods consumed. Without this information, it is difficult to determine whether children's diets meet their daily nutrient requirements, restricting the conclusions that can be drawn about diet quality and its impact on nutritional status.
Conclusion and recommendations
Conclusion
It can be concluded that children in the ECD centres in Tutaleni present with low prevalence of stunting and moderate levels of wasting and overweight. Stunting was more common in boys and older children. Malnutrition rates were lower than the national averages for stunting, wasting, and underweight, while the prevalence of overweight exceeded national levels.
The ECD centres in the study did not provide meals, and children brought food from home, with staff reporting that the food was often monotonous and occasionally inadequate. However, the study did not assess the nutritional quality or variety of the food children brought.
Overall, individual dietary assessments are needed to evaluate food quality, and regular healthcare visits and caregiver training on optimal child feeding practices and malnutrition identification are essential for improving nutrition.
Recommendations
This study identified several gaps that, if addressed, could improve child nutrition and the food environment in ECD centres. The following recommendations are proposed:
While the study conducted anthropometric assessments, it did not evaluate nutritional status in relation to dietary intake. Further research is needed to correlate children's nutritional status with their individual diets in ECD centres. An experimental study could assess the effectiveness of educational and training programmes for ECD caregivers and mothers on child feeding and care practices.(Makau and Thuku, 2024) Interventions such as home/daycare gardening, fortified food donations, and micronutrient supplementation should be explored. Expanding the National School Feeding Programme to include ECD centres in vulnerable areas may support these efforts. There is a need to develop standardized dietary guidelines that provide age-appropriate recommendations to meet the daily nutrient requirements of children attending ECD centres. Nutrition professionals, such as dietitians or nutritionists, should be employed by government and non-governmental organizations to plan and supervise menus for toddlers in ECD centres. Their expertise can help ensure that meals align with national nutrition policies and contribute to improving the dietary quality of food provided.
Footnotes
Acknowledgments
We, the authors, wish to express our heartfelt gratitude to Mr Daniel Mashishi, a statistician from Stellenbosch University, for his insightful contributions to data analysis and interpretation. We are also grateful to Dr Selma Kangwiya for her exceptional creative input and steadfast support throughout the development and completion of this research. Lastly, we extend our sincere thanks to the Early Childhood Development (ECD) centres, the participating children's parents, and the research assistants whose contributions were crucial to the success of this project.
Ethical approval
The Health Research Ethics Committee (HREC) of Stellenbosch University approved the research on 21 October 2023, under reference number S23/09/206. Additionally, the MGEPESW, the custodian of the ECD Programme in Namibia, granted approval. Permission for the ECD centres to participate in the study was obtained from the respective owners of the centres.
Consent to participate
Prior to participation in the study, written informed consent was obtained from all respondents, including the caretakers of the ECD centres, as well as the parents and/or legal guardians of the children involved.
Consent for publication
Not applicable.
Author contribution
All authors contributed to the article and approved the submitted manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: By submitting this research electronically, I hereby declare that the entire work contained therein is my own original creation, and that I am the sole author thereof. I affirm that the reproduction and publication of this work by the Nutrition and Health Journal will not infringe upon any third-party rights. Furthermore, I confirm that this work has not been previously submitted, in whole or in part, for publication to any other publisher. The views expressed in this publication are those of the author and do not necessarily reflect the views of any supporting organization or the publisher.
Data availability
The datasets generated and analysed during this study are available from the corresponding author upon reasonable request.