
Abstract
Background
The understanding, appreciation, and application of integrated healthcare by health professional students can shape future health promotion and intervention strategies. This involves blending nutrition, lifestyle, and conventional medical approaches from educational curricula to the professional practice arena.
Aims
To assess targeted healthcare students from three institutions for associations between demographics and survey parameters of knowledge, attitudes, and practices regarding nutrition and integrated healthcare approaches, and to evaluate students’ prospects for integrating lifestyle-based and conventional healthcare approaches, within the context of the Knowledge-Attitude-Practice (KAP) model.
Methods
Survey questions and responses based on a previously validated electronic questionnaire were used to evaluate university-level healthcare students enrolled in the nutrition (n = 92) and nursing (n = 195) disciplines. Demographic data were analyzed alongside scored items assessing knowledge, attitudes, and practices. Descriptive statistics, chi-square tests, Kruskal–Wallis tests, Dunn–Bonferroni tests, Spearman's rho, and partial correlations were conducted.
Results
Most students demonstrated high overall knowledge (74%), attitude (93%), and practice (84%) scores. However, significant differences (p < 0.05) in the knowledge scores were observed across institutions, academic levels, and disciplines. Although relatively weak, knowledge had a significant and positive relationship with attitude (rho = 0.263, < 0.001), but not with practice. The strength of relationships was moderated by controlling for socio-demographic factors such as specific degree/discipline, institutional and environmental context, race, religion, and age.
Conclusion
The findings of this study highlight the benefits of using KAP-based learning outcomes for healthcare training programs and demonstrate its relevance in informing tailored educational strategies and clinical interventions and policy initiatives that support integrated healthcare approaches.
Keywords
Introduction
Globally, there is a growing recognition of the role that integrated healthcare approaches play in preventing and managing chronic diseases (WHO, 2019; Bendowska and Baum, (2023). It encompasses nutrition, physical activity, and conventional medicine. Health professionals, including medical nutrition therapists and nurses, are uniquely positioned to advocate for and apply such strategies in patient care. However, their effectiveness depends on foundational knowledge, positive attitudes, and evidence-based practices (Somerville et al., 2019).
Health knowledge and perceptions can influence lifestyle decisions and behaviors. It can also significantly impact healthcare students’ approaches to promoting and implementing care measures for individuals, families, and communities. Therefore, healthcare students must be equipped with the necessary knowledge, skills, and attitudes that positively influence their healthcare behaviors and outcomes.
According to Turan et al. (2021: p. 7), “health behaviors can include healthy nutrition, regular physical activity, avoiding smoking and alcohol consumption, stress management, getting rest and spiritual growth.” It is believed that as students become more literate, they are more likely to integrate health behaviors into their lifestyles. This, in turn, places them in a better position to give credible advice, educate, and support patients in making positive health choices, ultimately resulting in a reduced risk of illness and disease.
The Knowledge, Attitude, and Practice (KAP) model provides a framework for understanding how learning may translate into behavioral outcomes (Lee et al., 2021). It posits that knowledge acquisition fosters attitudinal change, which, in turn, informs behavior. In this model, knowledge refers to the information individuals acquire about a particular subject, whereas attitudes represent their feelings, beliefs, concepts, and perspectives towards that information. Practice or behavior refers to the application of this knowledge in daily life. The basic assumption of KAP theory is that enhancing an individual's knowledge of a given topic, particularly in areas such as health or lifestyle, can positively shape their attitude towards it, which can then lead to better practices or behavioral changes. However, some scholars argue that attitudes and practices are not solely determined by knowledge, because social, cultural, and environmental factors also play significant roles (Ajzen, 1991).
Although the KAP model is widely applied in public health research, its application to allied health students in the context of integrated health care remains underexplored. The current study builds on this premise using questions from a previously developed and validated electronic questionnaire by the Triple-P Collaborative Research Team, as reported by Dyett et al. (2025). It aims to assess healthcare students’ demographics with KAP survey parameters regarding nutrition and integrated healthcare approaches. It also seeks to evaluate students’ prospects for integrating lifestyle-based and conventional healthcare approaches within the context of the KAP framework.
Methods
Study design and participants
This cross-sectional study involved analyzed response data from an online survey administered to healthcare students at three different higher education institutions situated in a region with a high burden of non-communicable diseases. Eligible participants included individuals enrolled in nutrition or nursing programs, as well as registered or practicing professionals in these disciplines who were pursuing higher academic degrees or continuing education at the time of the study. Participants were required to be at least 18 years of age.
Experimental protocol
Ethical approval and institutional permissions were obtained from all participating institutions. Informed consent was secured electronically from all participants. Recruitment was conducted via official institutional communication channels targeting enrolled students. In order to capture as many willing participants as possible, convenience sampling was used. However, a sample size was not used because the sampling frame for a particular nursing program with potential participants was not made available.
The survey instrument
The questionnaire was pilot-tested on a small sample of students across all three institutions. Relevant healthcare educators proof-read and finalized the 40-item electronic survey with 8 demographic items and 32 KAP items resulting in an overall Cronbach's alpha of 0.61 and a standardized items alpha of 0.71.
Because inter-construct relationships can be dynamic, reciprocal, and even interacting (Schrader and Lawless, 2004) with overlap among KAP items (Andrade et al., 2020), face and content validity were employed. Questions largely considered to be objective, subjective, and behavioral were used for the KAP framework as knowledge, attitude, and practice items, respectively. The KAP internal consistency differed based on ordinal-inclusive versus mainly dichotomous coding (e.g. 0.6 vs. 0.4 for attitude, respectively). The supplementary material provides a copy of the KAP questions with scoring examples at the end.
Knowledge, Attitudes, and Practices parameters
Statistical methods
Data variables were coded, missing data (0–3% per variable) were labeled, and various analyses were conducted. Descriptive statistics were used to summarize the participant characteristics and KAP scores. Chi-square and Kruskal–Wallis H tests with Dunn–Bonferroni post hoc multiple comparisons tests were performed to explore the associations between the demographic variables and KAP scores. Spearman's rho was used to assess the relationship between knowledge, attitudes, and practices, and Spearman's partial rho (Conover, 1999) was used to control for demographic influences.
Results
Participants
Table 1 provides the students’ demographic data along with their mean KAP scores.
Students’ mean KAP scores.
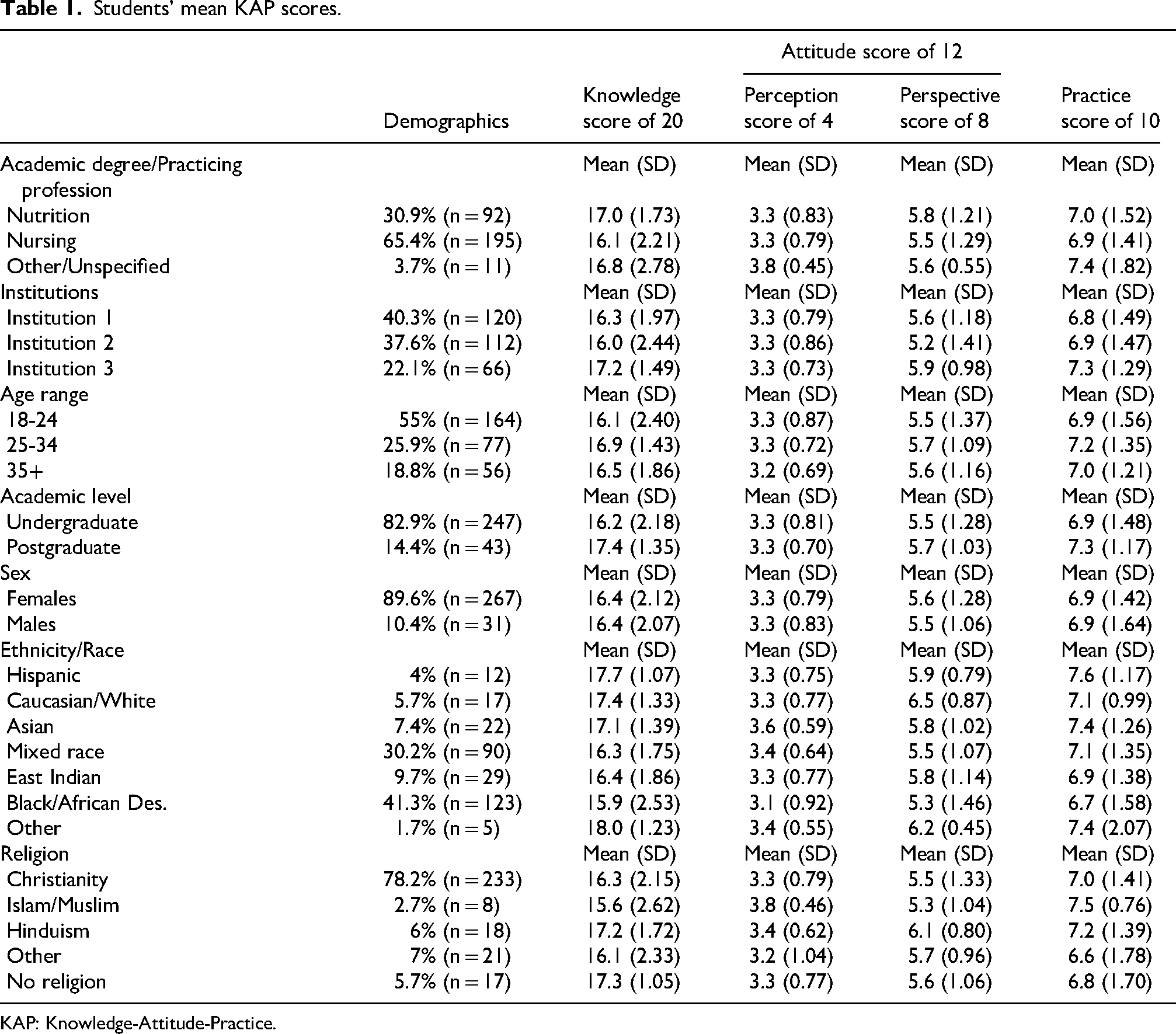
KAP: Knowledge-Attitude-Practice.
Students’ knowledge, attitude, and practice outcomes
Knowledge and perspective scores
Figures 1 and 2 show the distribution of the total knowledge and perspective scores out of 20, and 8, respectively. The bar graphs depict minimum, maximum, mode, and frequency values. The mean knowledge score was 16.38 (2.11 SD), and the mean perspective score was 5.5 (1.26 SD). The distribution of the attitude score is presented as a boxplot in Figure 3.
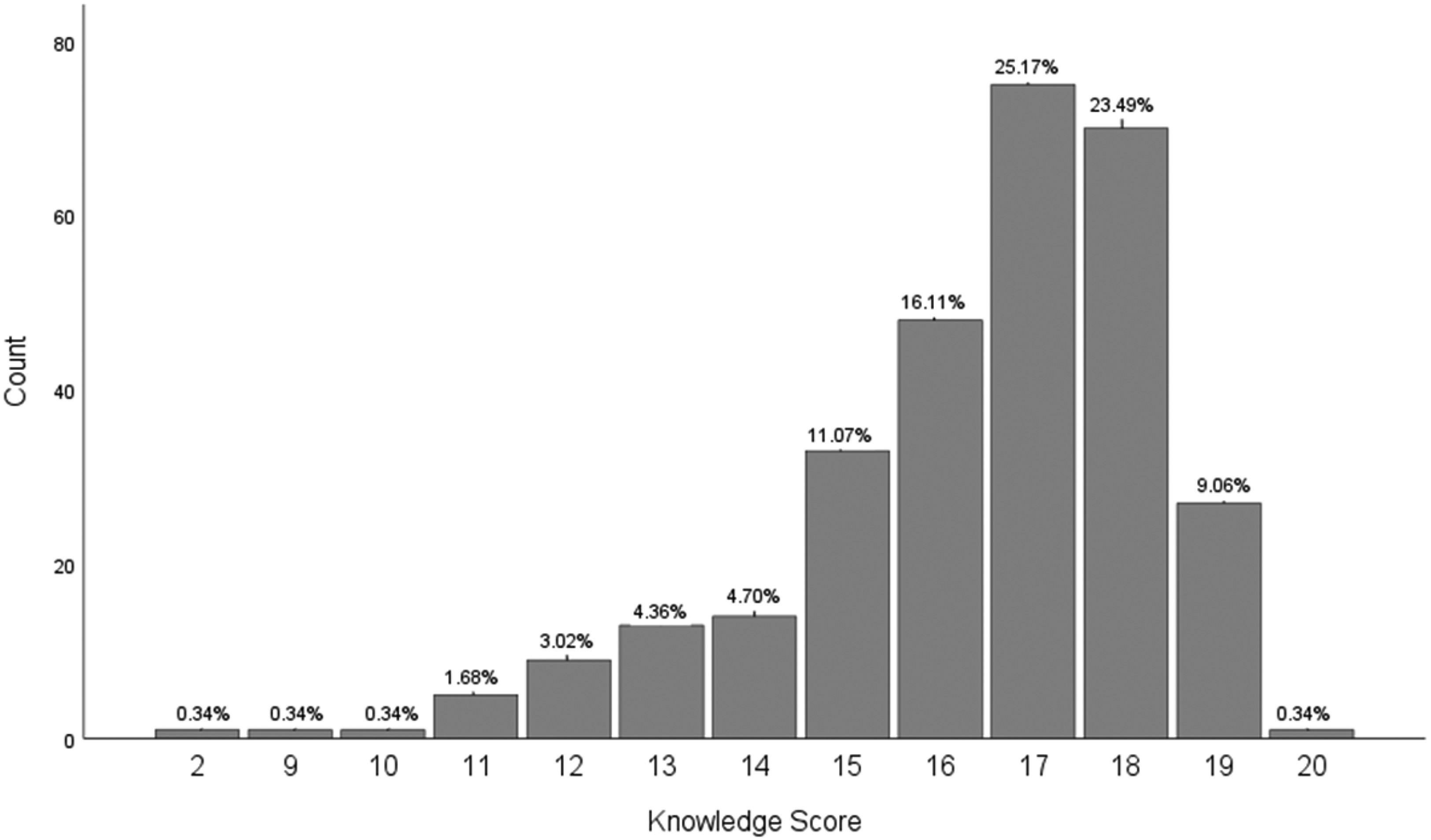
Percentage distribution of total knowledge score (out of 20).
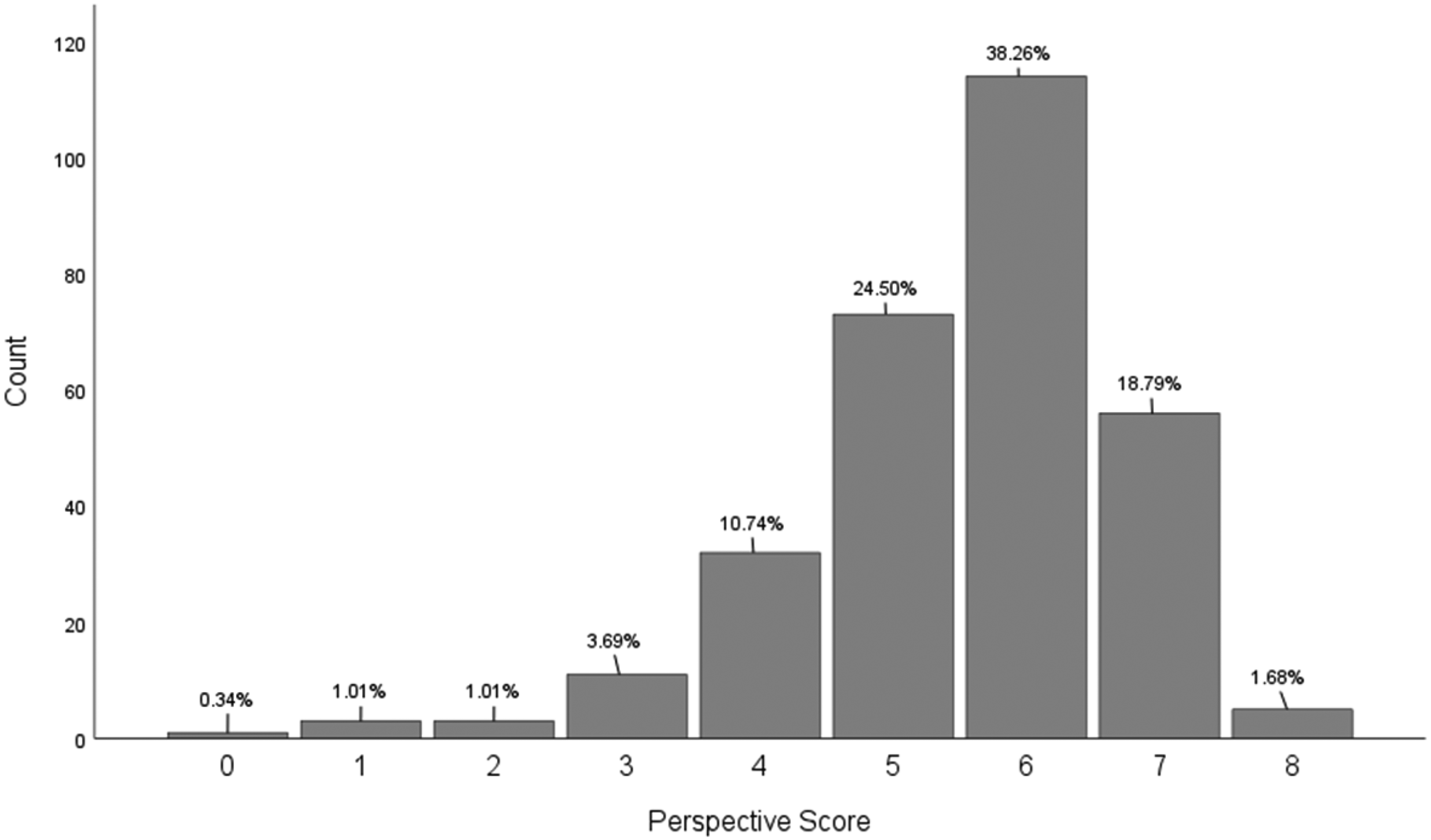
Distribution of attained perspective scores (out of 8).
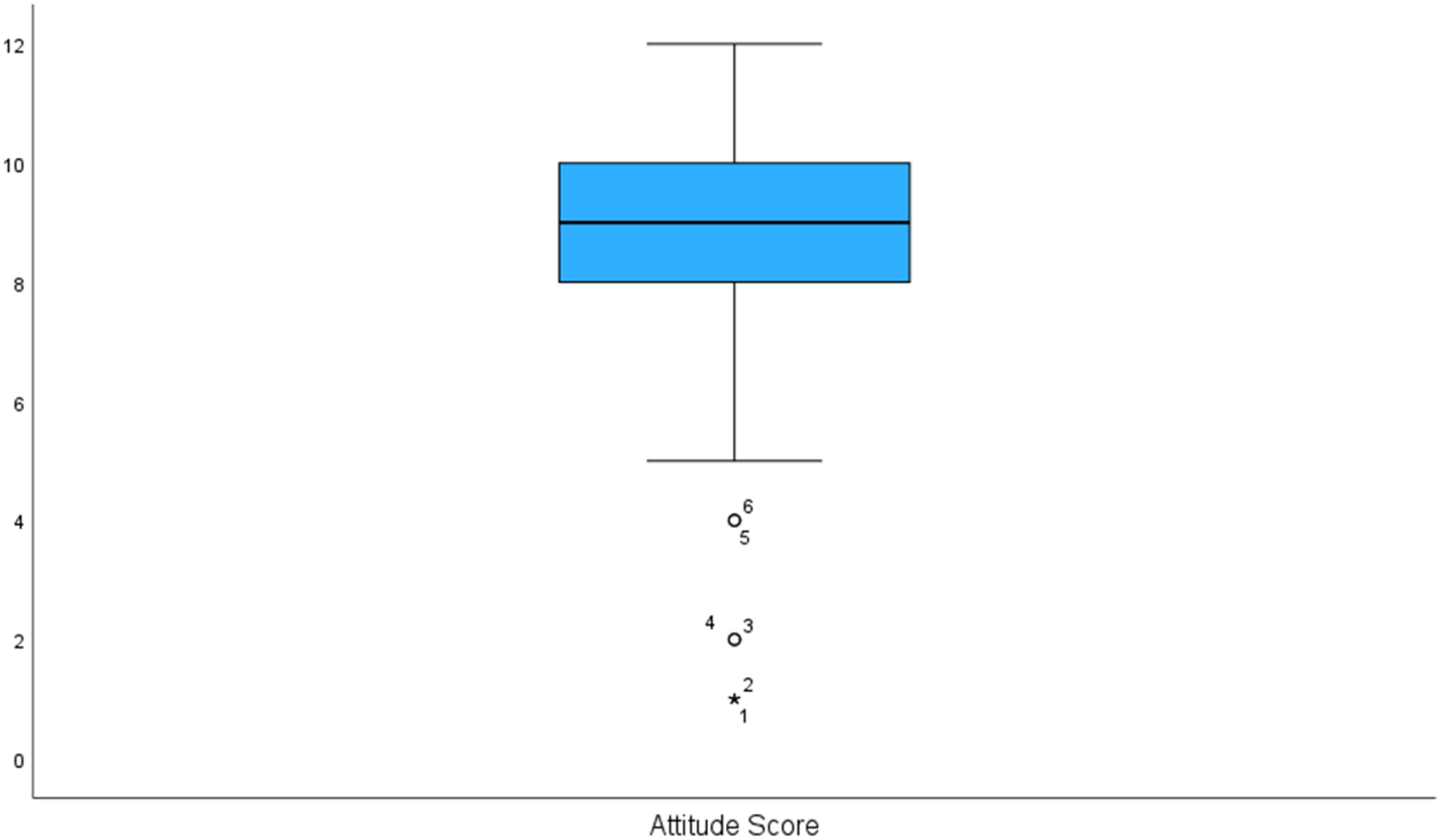
Boxplot of the attitude score distribution (out of 12).
Perception and practice scores
With a total maximum score of 4, the summary statistics for perception were as follows: minimum (0.0, n = 2, 0.7%), median (3.0, n = 119, 39.9%), maximum (4.0, n = 136, 45.6%), mode (4.0, n = 136, 45.6%), and mean (3.28, 0.80 SD). The distribution of the practice score is presented as a boxplot in Figure 4.
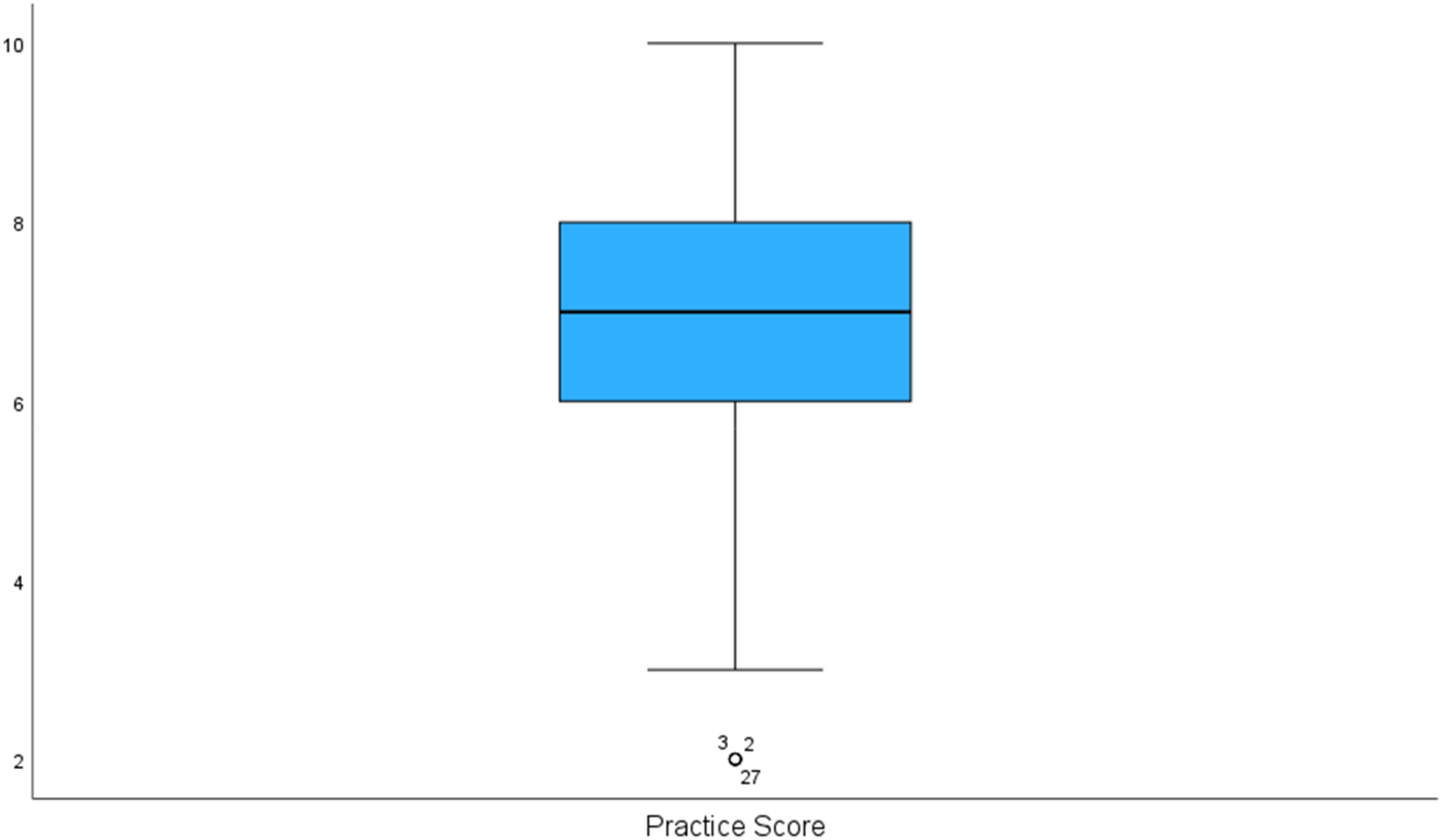
Boxplot of the practice score distribution (out of 10).
Attributed levels of Knowledge-Attitude-Practice (KAP) scores
The total scores for knowledge, attitude, and practice were used to create the attributed score levels using the Equal Interval method. The highest and lowest possible scores were used as the reference end-points of the score scale, with equal band ranges between to classify scores into simple, straightforward, and easily understood segments of performance.
Knowledge levels
Very Low (0–5) or Low (6–10) to Medium (11–15) vs. High (16–20). Descriptive tests showed the following distribution: very/low knowledge level: n = 3, (1%); medium knowledge level: n = 74 (24.83%); high knowledge level: n = 221 (74.2%).
Attitude levels
Perception Levels: Poor/fair desirability (0–2) vs. high desirability (3–4). Two hundred and fifty-five students (85.5%) obtained high perception scores.
Perspective Levels: Poor/low desirability: (0–2) to fair desirability (3–5), and high desirability (6–8). One hundred and seventy-five students (58.7%) obtained high perspective scores. However, 93% had high attitude scores.
Practice levels
Poor to Fair: (0–5) vs. Good/Desirable (6–10). Frequency analysis showed that 48 (16.1%) students demonstrated poor to fair practice scores, while 250 (83.9%) demonstrated desirable levels.
Associations between demographic characteristics and Knowledge-Attitude-Practice (KAP) score levels
Table 2 outlines the significant associations resulting from the chi-square tests of demographic factors with KAP score levels. Post hoc analyses are also presented as the proportion of students in each demographic category with high/good/desirable score levels versus low/poor or medium/fair score levels for the KAP attributes. Figure 5 is a visual representation of the healthcare students’ perspective outcome by academic discipline.
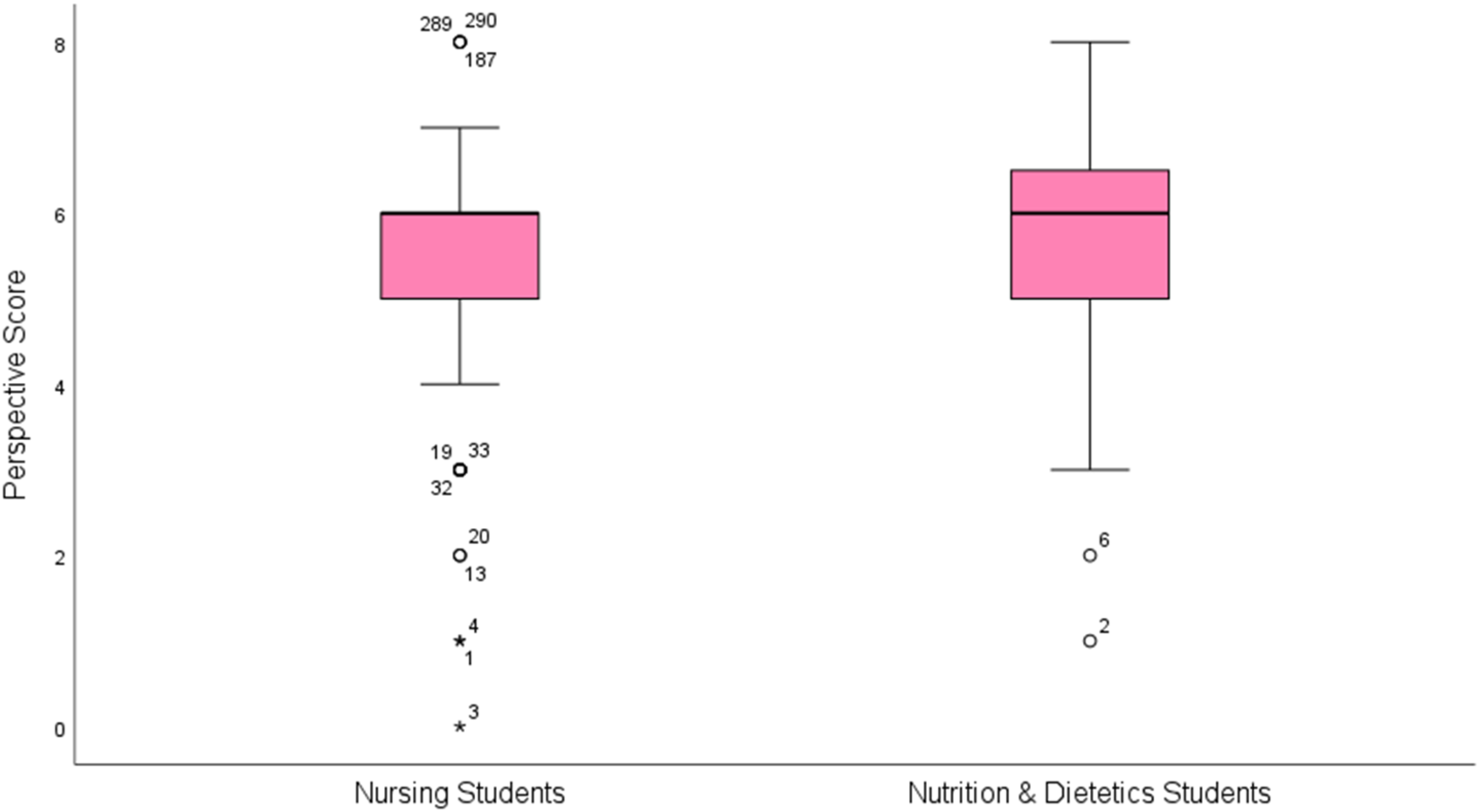
Boxplot of the perspective score distribution by academic discipline.
Chi-square tests of KAP score levels and student demographics.
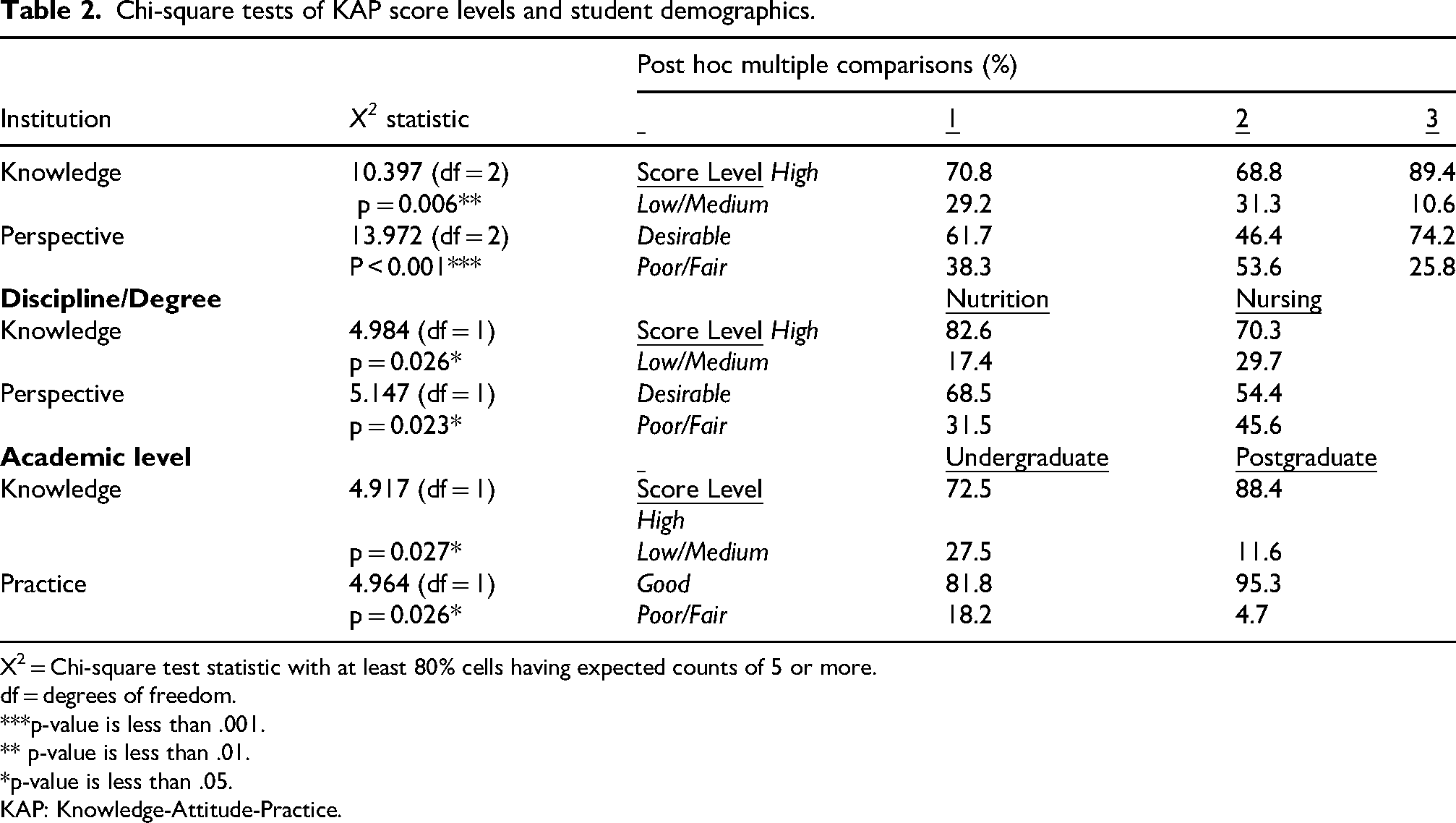
X2 = Chi-square test statistic with at least 80% cells having expected counts of 5 or more.
df = degrees of freedom.
***p-value is less than .001.
** p-value is less than .01.
*p-value is less than .05.
KAP: Knowledge-Attitude-Practice.
Kruskal–Wallis non-parametric and post hoc tests revealed the following significant results:
The mean knowledge score rank among institutions, H(2) = 13.80 (p = .001, η2 = 0.04), was significantly higher for institution 3 (183.58) than for Institutions 1 (140.997, p = 0.003) and 2 (138.519, p = 0.002). The mean knowledge score rank between healthcare disciplines, H(1) = 13.34 (p < 0.001, η2 = 0.047), was significantly higher for nutrition students (169.58) than for nursing students (131.93). The mean knowledge score rank between academic levels, H(1) = 14.33 (p < 0.001, η2 = 0.050), was significantly higher for postgraduates (189.35) than for undergraduates (137.87). The mean knowledge score rank among academic year groups, H(7) = 25.14 (p < 0.001, η2 = 0.064). Postgraduates had a significantly higher mean rank (229.29) than Year 1 freshmen (123.35, p = 0.000), Year 3 (137.10, p = 0.002), Year 3 seniors (133.90, p = 0.003), and Year 4 seniors (143.31, p = 0.007). The mean knowledge score rank among age groups, H(2) = 7.24 (p = 0.027, η2 = 0.017), was significantly higher for the 25–34 age group (169.58) than for the 18–24 age group (138.39, p = 0.022). The mean perspective score rank between healthcare disciplines, H(1) = 4.30 (p = 0.038, η2 = 0.015), was significantly lower for nursing students (137.30) than nutrition students (158.20). The mean perspective score rank among institutions, H(2) = 12.07 (p = 0.002, η2 = 0.034), was significantly higher for institution 3 (172.84) than Institution 2 (129.90, p = 0.002). The mean attitude (perception plus perspective) score rank among institutions: H(2) = 8.12 (p = 0.017, η2 = 0.021), was significantly higher for institution 3 (171.45) than Institution 2 (134.50, p = 0.014).
Application of the Knowledge-Attitude-Practice (KAP) framework
Correlations
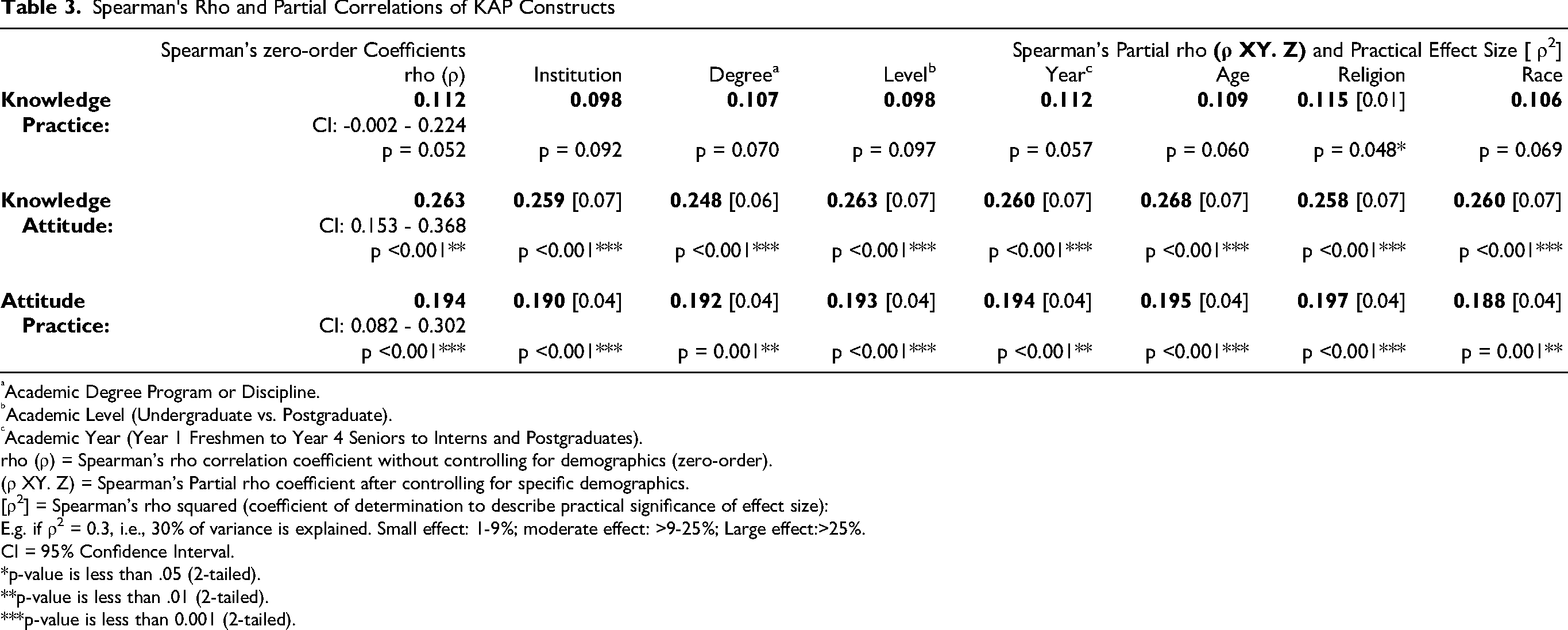
Table 3 shows Spearman's correlation trends for the KAP constructs. No significant correlation was observed between knowledge and practice. But positive directional relationships were observed between knowledge and attitudes and between attitudes and practice, though relatively weak. Figure 6 is a visual representation for knowledge by attitudes.
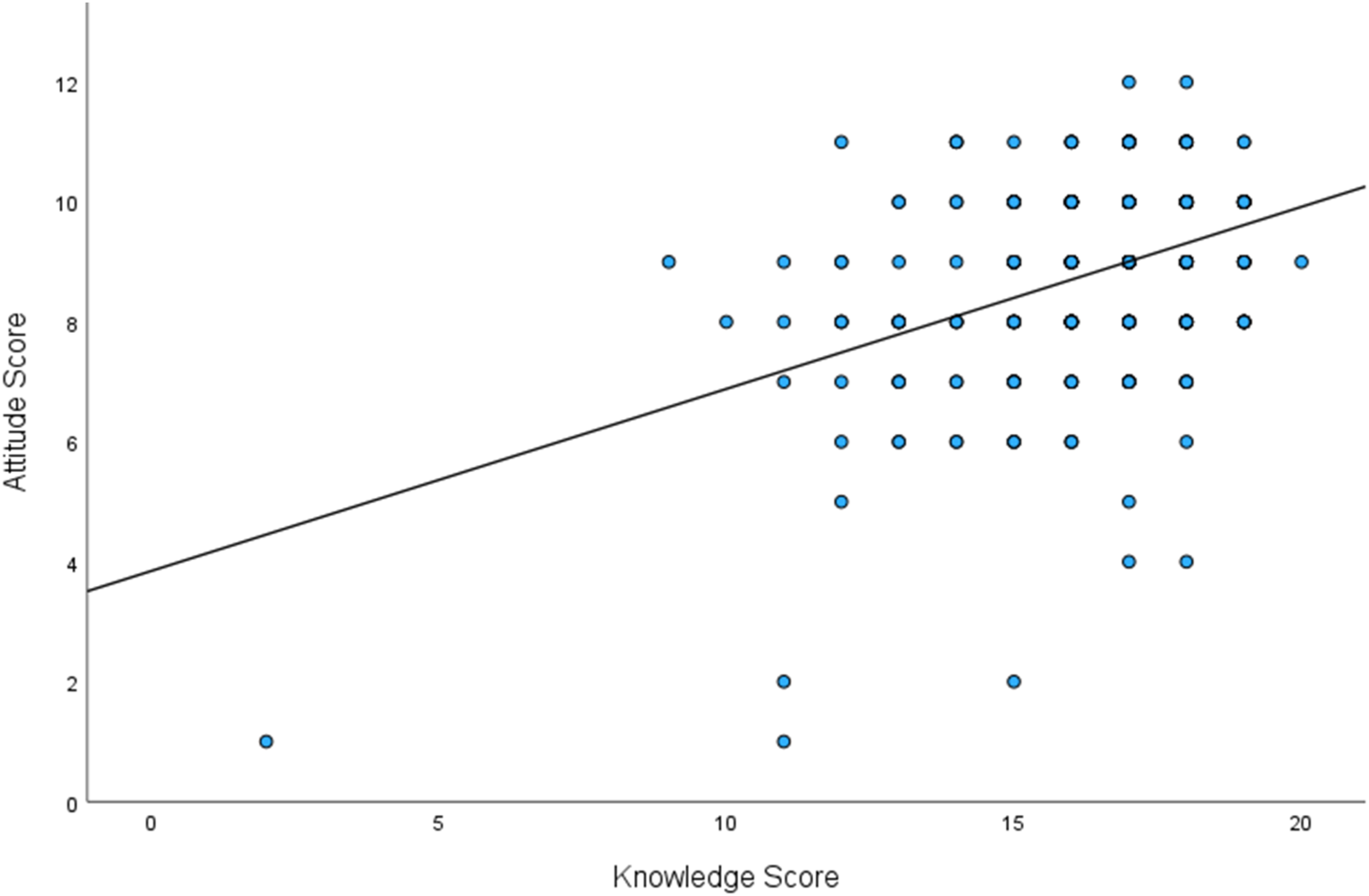
Boxplot of knowledge by attitude scores.
Spearman's Rho and Partial Correlations of KAP Constructs
Academic Degree Program or Discipline.
Academic Level (Undergraduate vs. Postgraduate).
Academic Year (Year 1 Freshmen to Year 4 Seniors to Interns and Postgraduates).
rho (ρ) = Spearman’s rho correlation coefficient without controlling for demographics (zero-order).
(ρ XY. Z) = Spearman’s Partial rho coefficient after controlling for specific demographics.
[ρ2] = Spearman’s rho squared (coefficient of determination to describe practical significance of effect size):
E.g. if ρ2 = 0.3, i.e., 30% of variance is explained. Small effect: 1-9%; moderate effect: >9-25%; Large effect:>25%.
CI = 95% Confidence Interval.
*p-value is less than .05 (2-tailed).
**p-value is less than .01 (2-tailed).
***p-value is less than 0.001 (2-tailed).
Spearman's partial correlation was statistically significant with a positive directional relationship between knowledge and practice when religion was controlled for. Except for academic level and age, reduced strength of relationship was observed between knowledge and attitude when demographics were controlled for. A similar trend in reduction was observed for the relationship between attitude and practice, except when academic year, age, and religion were controlled for.
Discussion
As knowledge about a subject matter increases, there should be a positive attitude towards new knowledge, which will then be reflected in positive practice changes (Kang and Bagaoisan, 2024). This is the concept behind the KAP Theory. It is based on knowledge and driven by individual attitudes, ultimately achieving practice change. The KAP model was beneficial to the current study because it successfully helped the researchers evaluate the relationship between the targeted nutrition and nursing students’ knowledge and attitudes and their actual or intended healthcare practice.
As shown, positive, but weak correlations and coefficients of determination were observed between knowledge and attitude, and between attitude and practice. Small effect sizes can still have practical and clinical significance, especially in health-related fields, and are educationally meaningful within the context of the KAP framework (Davis et al., 2021). The present study, however, focused not only on strength of relationship, but also on KAP directional trends.
The role of knowledge in the Knowledge-Attitude-Practice (KAP) framework
A systematic literature review by Mancin et al. (2023) evaluated 4853 nursing students from all years of a nursing program. This systematic review aimed to assess students’ basic nutrition knowledge. The questionnaires revealed that, on average, students scored lower than 50%, suggesting that the nutritional knowledge of nursing students was inadequate and that the school curricula should be adapted to integrate nutritional education with the curricula. In contrast, 70% of the nursing students and 83% of the nutrition students in the current study scored 80% or above for knowledge of nutrition, lifestyle, and health.
The application of the KAP theory was observed in a study by Laing and Crowley (2021), which showed that when different teaching methodologies were introduced to nursing students, there was an increase in their knowledge of nutrition. Wu et al. (2024) also suggested that even though a lecture can improve dietary knowledge, the effects are not always long-lasting. They recommend incorporating active teaching methodologies and targeted interventions that can address knowledge gaps and promote what will be viewed as healthier lifestyle choices among nursing students, further suggesting that improving knowledge and academic techniques can influence attitudes that can lead to practice changes (Coakley and Pribis, 2021).
The role of attitude in the Knowledge-Attitude-Practice (KAP) framework
Wu et al. (2024) found that using the KAP model among students revealed that a person's attitudes towards nutrition influenced dietary practice and outlook. The current study applied the KAP model and observed the highest correlation between knowledge and attitudes. This finding affirms prior work which suggests that attitude can be a critical mediating factor between knowledge and health behaviors (Algahtani et al., 2020; Lee et al., 2021).
Azizi et al. (2011) evaluated nutrition KAP among college students. Their findings indicated significant differences among all majors for knowledge and attitude. The higher scores were among nursing and physical education students compared to other majors such as business management, which had the lowest scores. Positive and significant correlations were also noted between attitudes and practices.
In the current study, the correlation between attitude and practice was also significant, but relatively weak. This might be due to the fact that only 59% of the students obtained perspective scores of 75% or higher, which may be attributed to the different socio-demographic and environmental influences among the targeted students. A similar view was put forward by Azjen (1991), who proposed that knowledge, attitude, and practice are influenced not only by each other but are also mediated by social, cultural, and environmental factors.
The role of socio-demographic and environmental factors in Knowledge-Attitude-Practice (KAP)
Various social and environmental factors can influence both knowledge and attitudes, which can in turn impact the degree and direction of expected or desired practice outcomes.
Degree program & career discipline
Researchers have recognized that the benefits of collaboration are critical. Leipzig et al. (2002) explored the attitudes of healthcare professionals towards working on an interdisciplinary healthcare team. The disciplines included in their study were internal or family practice medical residents, advanced practice nursing, and social work students. They reported that such teamwork among disciplines can enhance patient care and aid in utilizing time wisely, as all disciplines have the opportunity to participate. Their research, however, found that while most students in each profession agreed that the interdisciplinary team approach benefits patients and is a productive use of time, the agreement by medical residents was consistently rated lower than that of other disciplines.
In the current study, the knowledge and perspective scores of nursing students regarding nutrition, lifestyle, and integrated healthcare were consistently lower than those of nutrition students. Nutrition and lifestyle education are crucial elements of healthcare training. Adequate knowledge of nutrition allows healthcare workers to provide informed advice and interventions to prevent and manage various health conditions. Given the growing prevalence of diet-related chronic conditions such as obesity, diabetes, and cardiovascular diseases, it is essential for healthcare professionals and systems to be equipped with up-to-date knowledge and strategies on nutrition and healthy lifestyle practices (Sadiq, 2023; Salam et al., 2019).
The curricula of clinical nutrition programs facilitate the deep-diving of students into course content such as food science, nutritional metabolism, healthy lifestyle habits, diet planning, and medical nutrition therapy (Mancin et al., 2023). This is not the case for most nursing programs. Hwang and Oh (2020) suggested that health-promoting behaviors should be incorporated into the nursing curriculum to assist students with nutrition and health choices. They reasoned that such programs would empower nursing students to perform health-promoting practices. Ibrahim and Aldawsari (2024) concur and add that when nursing students have a strong understanding of nutrition, it is usually due to the fact that nursing courses effectively include nutrition teaching, resulting in nursing students making healthier choices and practice decisions. In the current study, when degree/discipline was controlled for, the relationships between knowledge and attitude and between attitude and practice were reduced. A regression-adjusted R-square for knowledge with degree alone was increased with interaction analysis between degree and academic level (not shown).
Academic level, year, and age
In the current study, the institution with students obtaining the lowest survey scores had only undergraduate students, while the sites generating higher scores had a mix of both undergraduate and postgraduate students. Other research supports the consistent findings of higher knowledge among higher level students, since graduate students typically possess higher health knowledge than undergraduates. This could be due to the advanced curriculum, more specialized coursework, and professional exposure offered by graduate-level programs, particularly in fields such as healthcare, nursing, and dietetics (Mancin et al., 2023).
The current study also included registered, practicing, and experienced nurses and dietitians who were enrolled in higher academic degree programs or continuing educational programs at the time of the study. The majority of their scores were higher than those of lower degree level or inexperienced students. Moreover, students’ academic years played a significant role in their health knowledge acquisition. For example, freshmen tend to have lower levels of health and nutrition knowledge, as they are often exposed to such topics for the first time at university (Antwi et al., 2025).
This was also observed in the present study. The mediating effect of age and maturity may also have been implicated. The relationship between knowledge and attitude and between attitude and practice demonstrated an increase in strength when age was controlled for. Most of the older, more experienced students were also postgraduate students who performed better on both the knowledge and attitude scales, which may have indirectly suppressed the strength of the direct knowledge-attitude and attitude-practice relationships.
As students matriculate during their academic years, they accumulate more knowledge through both formal coursework and experiential learning. Seniors, particularly those in their final year, possess significantly more comprehensive knowledge on nutrition and healthcare than freshmen or sophomores.
However, Azjen (1991) reported that while graduate students may demonstrate better knowledge than lower level students, their practices are not always significantly superior. This supports the idea that knowledge alone is insufficient for behavioral changes. In contrast, the postgraduate students in the current study obtained higher knowledge scores and demonstrated higher practice scores. Environmental context may have contributed to this outcome.
Institutional, geographic, cultural, & environmental context
The specific academic environment, geographical location, and cultural experiences that students are exposed to can impact their healthcare approaches. In the current study, students at a particular institution demonstrated higher knowledge scores than the others. The health-promoting and lifestyle-related environment of the site, availability of appropriate facilities and resources, cultural context, and geographical location may have all played significant roles in the findings.
All sites had direct access to medical hospitals and facilities for practicum. However, the highest performing site (institution 3) also emphasizes health and lifestyle in curricula, campus foodservice offerings, and faith-based activities. Religious cultures can impact nutrition-related knowledge, attitudes and healthcare practices (Mahabir and Gulliford, 2017). Religious norms and generational beliefs can affect whether individual students or faith-based institutions are consistently more health-conscious or open to non-conventional healthcare concepts and approaches. In the current study, when religion was controlled for, the strength of the attitude-practice relationship increased.
Institution 3 is also well equipped with various health and lifestyle resources and facilities. Institution 2 on the other hand scored the lowest on both knowledge and perspective scales. Although it is located within a cultural context in which natural, nutritional, and lifestyle factors are readily embraced and promoted, resources are much more limited. Some researchers have highlighted that students in urban campuses, where access to health resources and information is more prevalent, tend to demonstrate higher levels of health knowledge compared to those at rural or remote campuses (Chen et al., 2019; Kesson, Boyle and Jamieson, 2019). They suggested that urban settings often offer better exposure to healthcare professionals, health campaigns, and cultural diversity, which can positively influence students’ awareness and knowledge regarding health topics, including nutrition.
Ramos et al. (2024) expressed a similar view. They stated that urban campuses often have access to advanced facilities, diverse patient populations, and interdisciplinary collaboration opportunities, which can enhance students’ education. While rural campuses may face limited resources, they can offer intimate learning environments and exposure to underserved communities, fostering a strong sense of community-oriented care. Almoraie et al. (2025) added that campus infrastructure and healthcare-focused programs influence students’ dietary behaviors and nutrition knowledge.
Additionally, findings from a systematic review that aimed to identify the factors contributing to success among undergraduate Latino students, indicated that multiple factors were incorporated (Crisp, Taggart and Nora, 2015). The authors mentioned social and cultural characteristics, academic self-confidence, beliefs or ethnic identity, past experiences before attending college, experience during the undergraduate journey, self-motivation and commitment, supportive networks, perceptions of the university or college environment, and type of educational institution. In the current study, Hispanics, Caucasians, and Asians had the highest mean KAP scores. When institutions and races were controlled for, the existing KAP relationships weakened.
The research team observed that socio-demographic and psychographic factors significantly impacted students’ practice scores.
The role of practice in the Knowledge-Attitude-Practice (KAP) framework
Practice represents the direct embodiment of knowledge and attitude within the KAP model (Kang and Bagaoisan, 2024). In this study, 84% of healthcare students scored highly on the practice scale, indicating a promising outlook for integrated healthcare. Degree program, curricular content, institutional context, academic level/year, age, and religion all influenced KAP parameters.
Limitations
The cross-sectional study design prevents cause and effect inferences. Self-reported attitude items can introduce a social desirability bias where responses are based on what is more acceptable or expected in society, despite having opposing personal viewpoints. This may have influenced the high practice scores. However, the anonymity of survey administration and response may have reduced such effects. Future studies might benefit from addressing inflated responses with the use of a social desirability scale.
Convenience sampling and the lack of a calculated sample size prevented response rate measures, more comprehensive representativeness, and may have also contributed to selection bias. These limitations may have also contributed to imbalances in race/ethnicity subgroupings, which, while seeking to preserve true/meaningful differences between groups, could have otherwise been addressed with methods such as stratified sampling or oversampling. In order to include data from all eligible participants however, some aggregation was performed by including an “other” group and using categorical test analyses with at least 80% cells having expected counts of 5 or more.
Generalizability was limited because of participation from only three institutions. Additionally, students with greater interest in nutrition or integrated healthcare may have been more likely to participate, further limiting generalizability. Nevertheless, findings are consistent with studies of healthcare students in other regions.
Recommendations
Future studies might benefit from the use of mixed-method approaches, which can provide context and explanations, reveal barriers, motivators, social norms, and cultural beliefs that influence how knowledge can translate into attitude and practice.
Longitudinal assessments can help to evaluate change in KAP development overtime.
Although the focus of this study was on the KAP model, other relevant frameworks can be used to provide deeper understanding and interpretations, e.g. The Theory of Planned Behavior (La Babera and Azjen (2021).
Integrated healthcare content should be embedded within core clinical modules.
Various teaching methods can link attitudes to practice. Some actionable educational interventions include simulation, case-based learning, and interprofessional modules that can help to bridge the observed gaps.
Conclusion
In summary, healthcare students in this study demonstrated relatively high levels of knowledge and positive attitudes regarding nutrition and integrated healthcare. Nutrition and dietetics students outperformed nursing students in knowledge and perspective scores. Attitude was positively correlated with current or intended practices, underscoring the relevance of the KAP model. However, the strength of these relationships was moderated by socio-demographic factors, including degree program, academic level, academic year, institutional and environmental context, religion, and age. These findings highlight the importance of tailored educational strategies and supportive environments which help to optimize the knowledge, attitude, and practice interrelationships that enhance integrative healthcare.
Supplemental Material
sj-pdf-1-nah-10.1177_02601060251390159 - Supplemental material for Nutrition and integrated healthcare knowledge, attitudes, and prospective practices among healthcare students: A theoretical model survey analysis
Supplemental material, sj-pdf-1-nah-10.1177_02601060251390159 for Nutrition and integrated healthcare knowledge, attitudes, and prospective practices among healthcare students: A theoretical model survey analysis by Patricia Dyett, George Legall, Lesley-Ann Foster-Nicholas, Claudette Mitchell, Adana Adams-Robinson, Vanessa Jones-Oyefeso, Paula Valley-Thom and Valerie Sealey-Tobias in Nutrition and Health
Footnotes
Acknowledgements
The authors are grateful to those who facilitated the development and availability of the survey for use, and to the participating institutions and students for the source of response data. The authors are also thankful to the institutional Statisticians who contributed to analyses.
ORCID iDs
Ethics approval
This study was approved by the Ethics Committee of the host institution (Ref.# CREC-SA.2437/12/2023) along with official permissions from all other universities.
Consent to participate
Informed consent was obtained electronically from all participants.
Authors’ contributions
All authors contributed to the study design and/or data management, analysis, and interpretation, along with drafting and final approval of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicts of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data & material availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.