
Abstract
Few previous review articles have focused on the associations between inadequate daily water intake (LOW) or urinary biomarkers of dehydration (UD; low urine volume or high urine osmolality) and multiple diseases. Accordingly, we conducted manual online searches (47 key words) of the PubMed, Embase, and Google Scholar databases with these inclusion criteria: English language, full-text, peer reviewed, no restriction on research design, and three publications minimum. Initially, 3,903 articles were identified based on their titles and abstracts. Evaluations of full length .pdf versions identified 96 studies that were acceptable for inclusion. We concluded that the evidence is insufficient or conflicting for seven disorders or diseases (i.e. suggesting the need for additional clarifying research) and it is lacking for all-cause mortality. Differential characterizations among women and men have been reported in the results of nine studies involving five diseases. Finally, the evidence for associations of LOW or UD is strong for both kidney stones and type 2 diabetes with hyperglycemia. This suggests that great public health value (i.e. reduced disease risk) may result from increased daily water intake—a simple and cost-effective dietary modification.
Keywords
Introduction
Water is essential for metabolism, digestion, circulation of essential cellular substrates, movement of substances across cell membranes, regulation of intracellular–extracellular concentration, and it accounts for 55–75% of body weight depending on body composition and age. Although these physiological and biophysical processes rely on the volume of water consumed each day to maintain whole body fluid-electrolyte balance, relatively little is known about the long-term health consequences of chronic mild underhydration (Armstrong, 2012; Armstrong et al., 2020; Kavouras, 2019; Negoianu and Goldfarb, 2008) and few previous review articles have focused on the associations of inadequate daily water intake or urinary biomarkers of dehydration with multiple diseases and disease mortality.
Recognizing the importance of daily water intake to a healthy lifestyle, the United States National Academy of Medicine (NAM) (Institute of Medicine USA, 2004), the European Food Safety Authority (EFSA) (Agostoni et al., 2010), and the Australian National Health and Medical Research Council (ARC) (Australian National Health and Medical Research Council, 2006) published daily water consumption Adequate Intake (AI) values for men (3.7, 2.5, and 3.4 L·d−1, respectively) and women (2.7, 2.0, and 2.8 L·d−1). These AI guidelines were created with the understanding that physiological requirements for water vary widely according to environmental conditions, physical activity, individual differences of metabolism, and sensitivity to the detrimental effects of water intake deficiency (Agostoni et al., 2010; Australian National Health and Medical Research Council, 2006; Institute of Medicine USA, 2004). The respective methods of deriving AI values employed by NAM, EFSA, and ARC are different among these organizations. However, they all sought a daily water intake that was expected to maintain good health for both sexes and representative age groups (i.e. men, women, children, adolescents, and older adults). Two fundamental assumptions supported these AI values: water and adequate hydration are essential for health, and insufficient daily water intake may lead to medical disorders or diseases (Agostoni et al., 2010; Australian National Health and Medical Research Council, 2006; Institute of Medicine USA, 2004). Lending support to these assumptions, Allen et al. (2019) subsequently analyzed data from the Atherosclerosis Risk in Communities study (ARIC investigators, 1989) and determined that human hydration status predicted the development of multiple age-related degenerative diseases and that even subclinical mild hypohydration may affect long-term health outcomes.
No international consensus exists regarding the precise definition of dehydration and no single biomarker allows a convincing clinical diagnosis of dehydration (Armstrong, 2007; Armstrong et al., 2013, 2016; Kavouras, 2019; Lacey et al., 2019; Perrier et al., 2013a, 2013b; Shirreffs, 2000). This is true in part because total body water and extracellular concentration fluctuate continuously throughout life in a circadian pattern (Perrier et al., 2013a) and because water-electrolyte losses vary across individuals, medical conditions, physical activity levels, and environments (Armstrong et al., 2020). In the present review, we represent dehydration in the form of four measured variables, as designated in previously published studies (Armstrong, 2007; Armstrong et al., 1994; Perrier et al., 2013a, 2013b): low daily water intake, low daily fluid intake (i.e. water + beverages + food moisture), plus the human biomarkers low urine volume and high urine osmolality.
Accordingly, the present review evaluates research articles that have reported associations of (or lack thereof) low daily water and fluid intake (LOW) or urinary biomarkers of dehydration (UD; low urine volume and high urine osmolality) (Johnson et al., 2015, 2016; Kavouras, 2019; Perrier et al., 2013a, 2013b; Stookey et al., 2020) with an increased disease risk, incidence, recurrence, or mortality. This is important because 25–35% of adults in the United States and Europe habitually consume considerably less than the AI for water recommended by EFSA and NAM (Armstrong et al., 2020; Johnson et al., 2015; Perrier et al., 2013b). The present review also identifies relevant gaps in the literature, diseases that warrant future research, and novel research questions. In terms of public health benefits, clarifying the associations (or lack thereof) between LOW, UD, diseases, and mortality is essential for developing suitable consumer dietary guidelines that effectively reduce the risk and incidence of multiple diseases.
Search methods
Our review began with the discovery and consideration of potential medical disorders or disease types (i.e. that may be influenced by hydration status) and key search terms that involved a preliminary review of government reports (Agostoni et al., 2010; Australian National Health and Medical Research Council, 2006; Institute of Medicine USA, 2004), relevant narrative reviews, systematic reviews, meta analyses, interventional research, and observational studies (Allen et al., 2019; Armstrong, 2012; Dmitrieva et al., 2023; Enhörning et al., 2019a; Kolasa et al., 2009; Lacey et al., 2019; Manz, 2007; Manz and Wentz, 2005; Perrier et al., 2021; Popkin et al., 2010). Manual searches for relevant articles were performed within the PubMed, Embase, and Google Scholar electronic databases using advanced search operators (e.g. and, or, quotation marks, pertinent phrases). Inclusion criteria for searches included English language, full-text, and peer-reviewed articles with no restriction on research design types or year of publication. Combinations of the following keywords during these searches emphasized the associations of medical disorders and diseases (i.e. including risk, incidence, recurrence, and mortality) with LOW (i.e. low daily water intake and low daily fluid intake) and UD (i.e. low urine volume and high urine osmolality). The following keywords focused on hydration state: “water consumption”, “water intake”, “low water intake”, “total water intake”, “water turnover”, “fluid restriction”, “fluid deprivation”, “urine osmolality”, “urine volume”, “dehydration”, “intracellular dehydration”, “extracellular hypovolemia”, and “osmolality”. The following keywords focused on the type of disease or mortality: “disease”, “chronic disease”, “urinary tract infection”, “uti”, “chronic kidney disease”, “autosomal dominant polycystic kidney disease”, “bladder cancer”, “urinary tract cancer”, “colorectal cancer”, “colon cancer”, “rectal cancer”, “breast cancer”, “diabetes mellitus”, “type 1 diabetes”, “insulin-dependent diabetes”, “type 2 diabetes”, “non-insulin-dependent diabetes”, “hyperglycemia”, “metabolic syndrome”, “calcium oxylate stones”, “renal stones”, “kidney stones”, “urolithiasis”, “chronic lung disease”, “hypertension”, “heart failure”, “cardiovascular disease”, “dementia”, “Alzheimer's Disease”, “depression”, “major depression”, “fatal coronary heart disease”, “stroke mortality”, and “all-cause mortality”. Although polycystic kidney disease is one form of chronic kidney disease, we separated these two diseases because the former arises from a genetic mutation whereas other forms of chronic kidney disease have no widely recognized genetic basis, and the research studies identified in the present manuscript specifically focus on one or the other disease.
Using these search terms within PubMed, Embase, and Google Scholar, 3,903 articles were initially identified based on the title and the abstract (i.e. expressing a focus on associations of LOW or UD with human medical disorder or disease). After removing duplicate records, the abstracts and titles of the remaining records were evaluated to determine which studies should be assessed further. We subsequently performed manual searches of each relevant article's reference list, as well as the bibliographies found in germane systematic reviews and meta-analyses. Finally, we investigated full text (.pdf) versions of all remaining articles to ascertain if they each fit the purposes of this review. Neither a systematic literature review nor a systematic assessment of study quality or bias was performed for this review. Alternatively, a scoping literature review approach was employed to determine the scope and types of relevant research meeting our water intake, dehydration, and disease association criteria. This method was more suitable, as we did not intend to estimate the unbiased effects of rectifying dehydration or increasing daily water intake in the prevention and therapy of any medical disorder or disease.
Results
The manual screenings of full length .pdf versions identified the articles that were acceptable for inclusion in Table 1. These articles examined associations of LOW or UD with the risk, incidence, recurrence, or mortality of 10 diseases. The general effects of “dehydration” (i.e. without measurements of LOW or UD) are not included because no international consensus exists regarding the precise definition of dehydration (Armstrong, 2007; Armstrong et al., 2013, 2016; Kavouras, 2019; Lacey et al., 2019; Perrier et al., 2013a, 2013b; Shirreffs, 2000). Columns 2 and 3 in Table 1 characterize the types of research (i.e. prospective cohort study, retrospective cohort study, cross-sectional study at a single point in time, randomized controlled trial, counterbalanced experimental design with a control trial, systematic review, meta-analysis, narrative review, practice guidelines produced by a panel of experts that outlines current best practices, case–control study, or quasi-experimental study). Column 4 of Table 1 provides the references of nine studies that reported different associations for women and men. Eleven articles in Table 1 described associations of LOW or UD with multiple diseases and thus are referenced more than once. Similarly, because six of the studies in Table 1 completed a systematic review and a meta-analysis (Cheungpasitporn et al., 2016; Fink et al., 2009; Janbozorgi et al., 2021; Lin et al., 2019; Majdi et al., 2021; Xu et al., 2015), they are cited in both research classifications.
Findings of research studies that evaluated the associations of low water or fluid intake (LOW), urinary biomarkers of dehydration (UD), and human disorder or disease risk, incidence, recurrence, or mortality.a,b
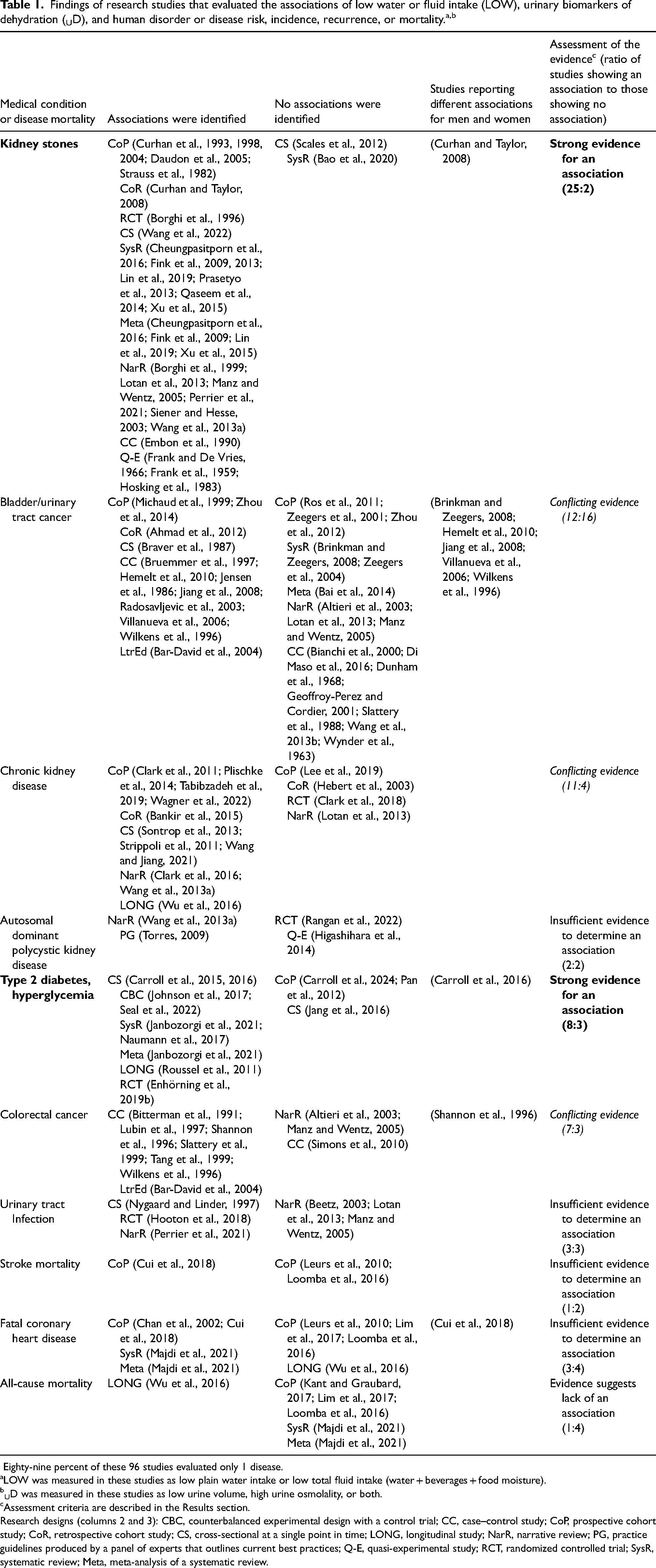
Eighty-nine percent of these 96 studies evaluated only 1 disease.
LOW was measured in these studies as low plain water intake or low total fluid intake (water + beverages + food moisture).
UD was measured in these studies as low urine volume, high urine osmolality, or both.
Assessment criteria are described in the Results section.
Research designs (columns 2 and 3): CBC, counterbalanced experimental design with a control trial; CC, case–control study; CoP, prospective cohort study; CoR, retrospective cohort study; CS, cross-sectional at a single point in time; LONG, longitudinal study; NarR, narrative review; PG, practice guidelines produced by a panel of experts that outlines current best practices; Q-E, quasi-experimental study; RCT, randomized controlled trial; SysR, systematic review; Meta, meta-analysis of a systematic review.
Column 5 of Table 1 presents the numerical ratio of studies showing an association to those indicating no association. This column also notes our assessments of the evidence for each medical condition, using the following four classifications: strong evidence for an association, conflicting evidence, insufficient evidence to determine an association, and evidence suggests lack of an association. These classifications (column 5) represent the unanimous consensus of all authors and are based on consideration of three criteria: (a) the ratio of studies showing an association (column 2) to those showing no association (column 3); (b) the total number of studies for each medical condition (columns 2 and 3); and (c) the strength of research designs, with randomized clinical trials, systematic reviews, and meta-analyses providing the strongest evidence (Bigby, 2014; Brighton et al., 2003; Cooper, 2016; Hooper et al., 2015; Lichtenstein et al., 2021; Song and Chung, 2010; Spill et al., 2022).
A minimum of three relevant publications were required for inclusion of any disease in Table 1. Our searches in the PubMed, Embase, and Google Scholar databases disclosed that 11 medical disorders and diseases did not reach this minimum inclusion criterion. Shown in parentheses is the number of articles found for each: breast cancer (0), type 1 diabetes (0), metabolic syndrome (0), dementia (1), Alzheimer's disease (0), depression (0), chronic lung disease (0), coronary artery disease (1), heart failure (0), mitral valve prolapse (0), and hypertension (0). In addition, two articles were initially considered for inclusion in Table 1 but were excluded (Palmer et al., 2014; Strippoli et al., 2011) because both employed a 145-item food frequency questionnaire which surveyed beverages (e.g. tea, coffee, milk, juices, sweetened drinks, and alcohol) but did not include a specific question about water consumption.
Discussion
This review highlights research studies in the extant literature that have reported associations of LOW (i.e. low water or fluid intake) or UD (i.e. urine volume or urine osmolality) with an increased risk, incidence, recurrence, or mortality of multiple diseases. Our scoping search of the literature indicated that 89% of the 96 identified studies examined only one disease. In contrast, Table 1 uniquely describes the strength of evidence for 10 disorders or diseases that were identified during extensive searches in three electronic databases that are highly utilized in medical and health fields. The clarification of the associations (or lack thereof) of LOW or UD with medical conditions and disease mortality is (a) valuable for the development of practical consumer dietary guidelines (notably including daily water intake) that effectively reduce the risk, incidence, and recurrence of disorders or diseases and (b) provides informed guidance for future research investigations. For example, the Table 1 evidence for kidney stones and for type 2 diabetes/hyperglycemia (T2D/H) is strong (column 5), based on the three criteria described above in the Results section. Using the same assessment criteria, the evidence regarding all-cause mortality suggests a lack of association with LOW or UD.
We recommend additional future investigations of the three diseases for which the evidence is conflicting (i.e. bladder/urinary tract cancer, chronic kidney disease, and colorectal cancer) and for four medical conditions for which evidence is insufficient to determine an association (i.e. urinary tract infection, autosomal dominant polycystic kidney disease, stroke mortality, and fatal coronary heart disease). All of these limited findings suggest that corresponding research is warranted. Similarly, 11 medical conditions (see Results section above) did not reach the minimum inclusion criterion for Table 1 (i.e. ≥ 3 publications), hence these diseases are worthy of future research.
Kidney stones
Strong evidence of association is presented in Table 1 (column 5) for kidney stones. It is noteworthy that kidney stones deposit at multiple anatomical sites (i.e. renal pelvis, ureters, bladder, and urethra) and have varied mineralogical compositions; calcium oxylate (CaOx) and calcium phosphate (CaP) are the most common. Regardless of composition, kidney stone formation is a complex and multistep phenomenon that includes urinary supersaturation, crystal nucleation, growth, and aggregation (Aggarwal et al., 2013; Hamamoto et al., 2011). Recent theories suggest that the following factors influence kidney stone formation: sex hormones, intestinal and renal microbiomes, and the immune response to urinary crystals (Wang et al., 2021). In addition, laboratory models have demonstrated that artificial stone formation and size are influenced by the supersaturation and pH of a solution as well as energy input which affects seed particle movements (Werner et al., 2021). Because supersaturation and crystal formation are the indispensable first steps in every type of urinary stone disease, enhancing urine dilution is the primary goal of investigators (Borghi et al., 1999; Daudon et al., 2005; Eccles et al., 1998; Finkielstein and Goldfarb, 2006; Pak et al., 1980) who accordingly recommend consuming ≥ 2 L of water per day to prevent kidney stones from recurring. This volume of water increases the minimum supersaturation required to elicit spontaneous crystallization of calcium salts (Pak et al., 1980; Siener and Hesse, 2003). Also, the American Urological Association (Pearle et al., 2014), American College of Physicians (Qaseem et al., 2014), European Association of Urologists (Skolarikos et al., 2023), and a consensus conference sponsored by the National Institute of Diabetes and Digestive & Kidney Diseases (Consensus Conference, 1988) recommend sufficient water intake to achieve a urine volume of 2.0–2.5 L·d−1. Combining this range with the fact that 24h urine volume is 0.8–1.4 L less than 24h total water intake (Cheungpasitporn et al., 2016; Johnson et al., 2015; Xu et al., 2013), the amount of total water/fluid intake needed per day for stone prevention is approximately 2.8–3.9 L·24−1 h, depending on daily activities, fluid losses, environmental heat stress, and body size. Whereas multiple strong recommendations support routine sufficient daily water intake to prevent the formation/reformation of kidney stones (Consensus Conference, 1988; Pak et al., 1980; Pearle et al., 2014; Qaseem et al., 2014; Siener and Hesse, 2003; Skolarikos et al., 2023), the recommended water intake to meet the urine volume threshold appears to be inadequate (Cheungpasitporn et al., 2016; Johnson et al., 2015; Xu et al., 2013).
Type 2 diabetes/hyperglycemia
Regarding the strong evidence for T2D/H, it is important to note that Table 1 does not include studies that assessed the effects of replacing caloric or noncaloric beverages with plain water. This is not surprising, as such effects typically are studied regarding obesity or weight loss during long-term studies (Daniels and Popkin, 2010; Naumann et al., 2017; Tate et al., 2012). Thus, row 5 of Table 1 presents only research that evaluated the associations of LOW or UD with T2D/H. However, although the process by which LOW or UD may affect glucose metabolism is not known (Carroll et al., 2015; Jansen et al., 2019), four theoretical mechanisms have been proposed. For example, LOW stimulates the secretion of arginine vasopressin (AVP) (Johnson et al., 2015, 2016; Perrier et al., 2013b) which is a vasoconstrictor and antidiuretic hormone. Because increased circulating AVP results in hyperglycemia, induces gluconeogenesis, and increases plasma glucagon concentration in humans and animals, LOW theoretically in turn increases T2D/H risk (Roussel et al., 2011; Spruce et al., 1985). Supporting this theory, blood AVP concentration is known to be elevated in T2D patients (Roussel et al., 2011; Zerbe et al., 1979). Similarly, the renin-angiotensin-aldosterone system can be activated by LOW or measurable body water loss, resulting in a rise of blood aldosterone concentration (Johnson et al., 2016). Elevated aldosterone has been shown to interrupt normal insulin signaling, consequently slowing the removal of glucose from the bloodstream (Verbalis, 2006). Also, LOW or chronic appreciable loss of body water may disrupt cell metabolism (Haussinger et al., 1994) in a way that leads to insulin resistance (Carroll et al., 2015; Tsai et al., 2005; Uribarri et al., 2007). Further, high glycemic load diets have been associated with an increased risk of T2D (Malik et al., 2010). Because water has no calories, its consumption with meals may reduce the glycemic load of food, dampen the postprandial glycemic response, and lead to reduced risk of T2D (Carroll et al., 2015). Finally, since only 10 research studies in Table 1 associated T2D/H with LOW and or UD, it is possible that a suitable mechanism has not yet been proposed and that future theories may offer viable explanations (Carroll et al., 2015; Jansen et al., 2019).
Future research
From the studies presented in Table 1, eight concepts are revealed that are relevant for the design of future research studies. First, among the 96 unique publications cited in Table 1, randomized controlled trials (n = 5), systematic reviews (n = 13), and meta-analyses (n = 7) are in the minority whereas prospective cohort studies (n = 24) represent the most common research design. Future investigations should critically consider experimental designs. Second, both kidney stones (n = 27) and bladder/urinary tract (n = 28) cancer are represented in Table 1 by nearly twice as many studies as any other medical conditions. This suggests that the remaining eight disorders and diseases in Table 1 are understudied and that water intake may not be widely recognized as a possible etiological factor in these conditions. Third, multiple authors designated their research as “longitudinal” but did not classify their research as prospective or retrospective. We recommend that this distinction be clearly stated in the Methods section of each article. Fourth, the literature regarding chronic kidney disease suggests that daily water intake recommendations may be different with regard to prevention than to the progression of existing disease (Tabibzadeh et al., 2019). For example, studies have reported that the risk of chronic kidney disease and the annual decline of kidney function were positively associated with higher urine osmolality (Plischke et al., 2014) but were inversely correlated with lower urine volume (Clark et al., 2011). This suggested that a higher daily water intake would be kidney protective (Tabibzadeh et al., 2019). However, when chronic kidney disease exists, its progression appears to be faster among individuals who sustain a high urine volume and low urine osmolality (Hebert et al., 2003; Higashihara et al., 2014). Importantly, these observational studies should not be construed as an endorsement of water restriction in patients with chronic renal insufficiency (i.e. where water restriction would result in elevated vasopressin levels), but rather should promote the conduct of randomized, long-term studies to reach more definitive conclusions (Hebert et al., 2003; Higashihara et al., 2014). Fifth, in prospective cohort studies, investigators screen patients and utilize statistics to control risk factors that may have influenced the onset and progression of a medical disorder or disease. However, some relevant factors may go unrecognized and uncontrolled. Bladder cancer is a case in point because the characteristics and incidence of this disease are different among racial/ethnic groups with equivalent healthcare (Porter et al., 2002; Wang et al., 2018). Moreover, bladder cancer susceptibility is greater among individuals who possess certain gene polymorphisms (Fontana et al., 2009; Hung et al., 2004; McGrath et al., 2006). Thus, the uncontrolled influences of racial or genetic factors may partly explain why the bladder cancer evidence in Table 1 is conflicting. Sixth, human exposure to surface water disinfection byproducts (DBP) is another influence on bladder cancer that is worthy of future study. DBP in public water systems are unintended consequences of chlorine disinfectants reacting with organic and inorganic compounds. More than 700 DBP are known (Ashbolt, 2004; Weisman et al., 2022; Zwiener et al., 2007) and DBP in public water supplies have been shown to increase bladder cancer risk (i.e. calculated odds ratio) in the United States (McGeehin et al., 1993; Vena et al., 1993; Weisman et al., 2022), Canada (King and Marrett, 1996), Finland (Koivusalo et al., 1998), and Europe (Nieuwenhuijsen et al., 2009; Vena et al., 1993). Seventh, animal research allows clarification of cellular processes that are challenging or unethical to explore in human subjects. The 2019 controlled laboratory investigation of Allen et al. (2019) is an excellent example. Mice were water restricted (WR) for their entire life starting at the age of 1 month, consumed only gelled food containing 30% water and 70% dry food, and received no additional water. During the first 12–14 months of life, despite an absence of obvious clinical symptoms, WR mice exhibited elevated urine osmolality and were in a state of low-grade inflammation and coagulation. This chronic inflammation (i.e. assessed by serum IL-6 level) was accelerated in the WR mice and their lifespan was shortened by about 6 months (18%), compared with control mice that had free access to water and consumed the same diet. This investigation (Allen et al., 2019) illustrates the value of animal research in identifying chronic disease-related effects of LOW and UD across the lifespan. Our final recommendation for future research focuses on the important topic of differential characterizations for women and men. The underlying causes for the sex differences in Table 1 (column 4) are not yet fully understood, but the following theoretical factors have been proposed: age-related changes of kidney function, diet, and urine electrolyte levels for kidney stones (Curhan and Taylor, 2008); frequency of urination, hormonal effects on micturition (Jiang et al., 2008; Villanueva et al., 2006), and urine specific gravity (Braver et al., 1987) for bladder cancer; female–male hormonal differences unspecified (Carroll et al., 2016) for T2D/H; as well as the volume of water consumed each day, fruit and vegetable intake, and dairy product consumption for colon cancer (Shannon et al., 1996). Considering the variety of these theoretical explanations and the complex disorder and disease etiologies involved, unraveling the underlying causes of sex differences will require a considerable number of comprehensive and strategic investigations across multiple populations that are specific to each medical condition and related influencing factors.
Summary
In summary, the range of medical conditions incorporated in the present review, as well as the strict criteria utilized for inclusion, represent a robust clarification of the associations between LOW, UD, disorders and diseases, and related mortality. Our findings regarding kidney stones, T2D/H, and all-cause mortality are unique in the medical and scientific literatures, largely because few previous studies have focused on LOW or UD. The 11 medical disorders/diseases that did not meet our inclusion criteria and the 10 medical conditions described in Table 1 demonstrate that many medical conditions remain understudied. Accordingly, we have provided seven recommendations for future research. Finally, the experimental designs which are employed to study the associations between LOW, UD, disorders and diseases, and mortality should prioritize randomized controlled trials, systematic reviews, and meta-analyses.
Footnotes
Authors’ contributions
Conceptualization, LEA; methodology, LEA, MFB; literature search, LEA; data interpretation, LEA, MFB, CXM, SAK; writing – original draft preparation, LEA, MFB, CXM; writing – reviewing and editing, LEA, MFB, CXM, SAK; approval of final manuscript, LEA, MFB, CXM, SAK.
Availability of data and materials
Table 1 provides the outcome (final screen) of the literature search (3 databases) for this review. No supplemental materials have been submitted.
Consent for publication
Not applicable.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LEA is a Board of Trustees member and occasional consultant for the Drinking Water Research Foundation, Alexandria, VA; MFB – no conflicts of interest; CXM – is an occasional consultant for and has an active research grant with Kraft Heinz Co.; SAK has active research grants during the past 36 months from the National Science Foundation, USDA, Kraft Heinz, Unilever, and Standard Process. During this time, he was a lead research aerospace physiologist at Luke Air Force Base, AZ and served as a member of the science advisory board for Hyduro Inc, Zico Rising, and Rockley Photonics. He has also provided scientific consultation to the American Beverage Association, Unilever, Pepsico, and Kraft Heinz Co.
Ethical approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.