
Abstract
The Rohingya refugees are among the most vulnerable victims of COVID-19 pandemic in Bangladesh. In refugee camps, they frequently lack access to safe and nutritious foods, drinking water, and a healthy environment. Despite the fact that numerous national and international organizations are sincerely collaborating to meet their nutritional and medical needs, the pace of work has slowed due to COVID-19. Combating COVID-19 demands a robust immune system, which relies heavily on a nutritious diet. The development of strong immunity to protect Rohingya refugees, particularly children and women, through the provision of nutrient-dense foods is thus highly necessary. Consequently, the current commentary focused on the nutritional health status of Rohingya refugees in Bangladesh during COVID-19. In addition, we provided a multilevel implementation framework that could assist stakeholders and policymakers in taking effective measures to recover their nutritional health.
Introduction
When disaster strikes any part of the world, as a pandemic, natural disaster, or economic collapse, the underprivileged people suffer the most compare to others. In particular, the forcibly migrated people in the refugee camps might hold the top position on the list of such people. In Bangladesh, the novel coronavirus (COVID-19) posed an extreme threat to Rohingya refugees. The violence in Myanmar in August 2017 forced another 6,93,000 Rohingyas to migrate to Bangladesh, bringing the total to almost 1 million by June 2018 (Joarder et al., 2020). Prior to then, according to the United Nations Refugee Agency (UNHCR), Bangladesh was home to around 265,000 Rohingya refugees (UNHCR, 2011). At that time, Rohingya refugees had settled in over 30 camps in Cox's Bazar, where they had limited access to safe food, potable water, and adequate sanitation (Limon et al., 2020). However, the real number of displaced refugees may vary based on the sources. Although the population has risen since then due to births and the number of camps has also increased in which they reside. These camps are highly overcrowded and the residents are facing several difficulties including severe malnutrition, notable sexual violence, and instability of physical and mental health (Jubayer et al., 2022).
World Health Organization (WHO) declared COVID-19 a global health emergency because, arguably, it posed the greatest threat to modern human civilization. The entire refugee settlement in Cox's Bazar possesses the characteristics of a likely epicenter of disease transmission. Additionally, COVID-19 susceptibility has been identified in refugee camps in other countries also (Vonen et al., 2021). In Bangladesh, the first COVID-19 case was detected in a Rohingya camp on 14 May 2020 (Jubayer et al., 2021). To prevent the spread of COVID-19, people must take precautions such as staying at home, maintaining a physical distance, avoiding public places and public transportation, wearing masks, washing their hands frequently, etc. The COVID-19 outbreak is likely to have a significant impact on the psychological wellbeing of the refugee population. Current conditions in all Cox's Bazar refugee camps include a lack of social distance, food insecurity, and a lack of knowledge and awareness about COVID-19 (Jubayer et al., 2022). Boosting immunity through the consumption of nutrient-rich foods and supplements is essential in this situation, with children and women having the greatest need. During COVID-19, hunger and food insecurity increased among Rohingya adolescents, and their self-reported health deteriorated (Guglielmi et al., 2020). When an outbreak of disease arises in any refugee camps, there are certain conditions that place malnourished children at a greater risk, prolonging the vicious cycle between starvation and infection (Browne et al., 2021). In light of these facts, we feel compelled to shed additional light on the risks and effects of COVID-19 on the nutritional health of the Rohingya in Bangladesh. This work explores how a pandemic outbreak among refugee populations in Cox's Bazar would likely impact health and nutrition in the camps that house hundreds of thousands of vulnerable refugees. In addition, we proposed a multilevel action framework to assist stakeholders and policymakers in taking the necessary steps to restore the nutritional health of this refugee population during the pandemic.
Nutritional health of Rohingya refugees during COVID-19 pandemic
The current situation of these Rohingya refugees in Bangladesh has made them more vulnerable to infectious diseases, particularly women and children who suffer from severe malnutrition (Joarder et al., 2020). From the beginning, a substantial percentage of Rohingya children suffered from stunting, wasting, anemia, and global acute malnutrition (Leidman et al., 2018). If we look at the information prior to the emergence of COVID-19, according to WHO, 4.1% of the children had severe acute malnutrition (SAM) and 4.2% had moderate acute malnutrition (MAM), respectively (WHO, 2018). In these camps, nutritional and health conditions for adolescent girls, pregnant women, and breastfeeding mothers are deplorable. Approximately 10% of women in the Rohingya community of Bangladesh are malnourished, and their immunity is deteriorating daily (Leidman et al., 2018). According to a recent study, the children in the camp settings are malnourished due to a lack of basic food (Parvin, 2022). Another study indicated that the majority of Rohingya children studied were underweight and wasted (Roy et al., 2022).
In addition, COVID-19 has significantly disrupted global food supplies and reduced food options. Additionally, the pandemic has affected service delivery in both Rohingya camps and host communities. The outreach activities and coverage of community nutrition services have decelerated due to restricted movement, which began in March 2020. A report exhibited that the nutrition screening coverage in Rohingya camps decreased from 132,507 in January 2020 to 64,653 in April (Rahimov et al., 2021). In addition to refugee camps, food insecurity is a significant and visible problem in host households. People within the camps claim that COVID-19 has rendered them unable to work as before and that they are starving. The price of every food item has increased due to increased demand and limited supply. A 17-year-old married Rohingya girl narrated the changes in her household since COVID-19 as “Sometimes we have to eat rice only with salt. We could sell food and buy something for ourselves before. But [now] they give us food like we are beggars. The potatoes were 15–16 taka before. Now the price has risen to 30–32 taka. They used to give eight eggs per person, but now they give five eggs” (Guglielmi et al., 2020). The vast majority of refugee families have experienced at least one of the following three forms of severe food insecurity:
There is no food in the household due to a lack of resources; At least one household member goes to bed hungry due to a lack of food; and Due to a lack of food, one household member may go an entire day and night without eating. Currently, adolescents are less likely to consume protein-rich foods. A 15-year-old Rohingya girl clarified as “We have no money, so we can't buy raw food items like vegetables, fish, and meat. We are unable to consume fresh food” (Guglielmi et al., 2020).
Ongoing assistance activities in Rohingya camps
World Food Program (WFP) is provided food assistance to the forcibly displaced Myanmar nationals worldwide including the Rohingya people of Bangladesh. Currently, the Rohingya community staying in different camps can receive food assistance in two forms: (1) general food distribution and (2) electronic food vouchers (e-voucher) (Hoddinott et al., 2020). WFP made 19 different types of locally grown vegetables accessible through 15 fresh food corners (FFC). Besides, the most vulnerable 39,393 families received a supplementary US$3 to diversify their diets by shopping at FFC (WFP, 2021). The nutrition response in Cox's Bazar is overseen by the Nutrition Sector, which is led by the Ministry of Health and Family Welfare in collaboration with UNICEF. This response plan was primarily concerned on the treatment, management, and prevention of acute malnutrition, with definite interventions such as community-based management of acute malnutrition (CMAM) for children aged 6 to 59 months and community-based management of at-risk mothers and infants (below 6 months) (Rahimov et al., 2021). Since 2020, 46 integrated nutrition facilities (INF) have provided all nutrition assistance, which includes outpatient therapeutic programs for severe wasting, targeted supplementary feeding programs for moderate wasting, and blanket supplementary feeding programs. Iron and folic acid supplementation is also aimed at adolescent girls and pregnant and lactating women (Rahimov et al., 2020). Through 45 nutrition sites, WFP provided malnutrition treatment and prevention facilities to nearly 40,000 pregnant and lactating women and about 161K children (under 5 years) in refugee camps (WFP, 2021). Any child identified with SAM or MAM based on adapted global nutrition cluster (GNC), Mid-Upper Arm Circumference (MUAC) cut-offs (SAM, MUAC < 120 mm; MAM, MUAC ≥ 120 and <135 mm) was referred to the adjacent INF for treatment (Rahimov et al., 2020).
Current challenges and proposed multilevel action framework
Due to restrictions imposed to prevent the spread of COVID-19, there are a limited number of humanitarian workers in the camps. The restrictions on entering and leaving the camps resulted in a reduction of available personnel by more than 50%. The pandemic of COVID-19 has had far-reaching effects on nutrition programs. In 2019, community nutrition volunteers screened an average of 135,000 refugee children per month for malnutrition, but these services have been suspended due to COVID-19 mitigation measures (Jean, 2020). While CMAM services could be maintained, several changes were required to safeguard the security of beneficiaries and staff, as well as effective infection prevention control within INFs. These modifications were influenced by the guidance issued by UNICEF, the GNC, and the global technical assistance mechanism for nutrition (Dube et al., 2020).
Nevertheless, based on the preceding discussion, we propose a multilevel framework to support nutritional health in the face of COVID-19, employing the individual, community, and national levels of the ecological health model. The nutritional framework concept is suggested through a recent study by Naja and Hamadeh, (2020) for maintaining the physical and mental health of an individual during COVID-19. It was a social-ecological model (SEM) that was adopted and modified by the author. In addition, Islam et al. (2022) applied the same model framework for addressing and resolving problems in the agro machinery sectors of Bangladesh. Figure 1 depicts a multilevel action framework based on the SEM to improve Rohingya refugees’ nutritional health during COVID-19.
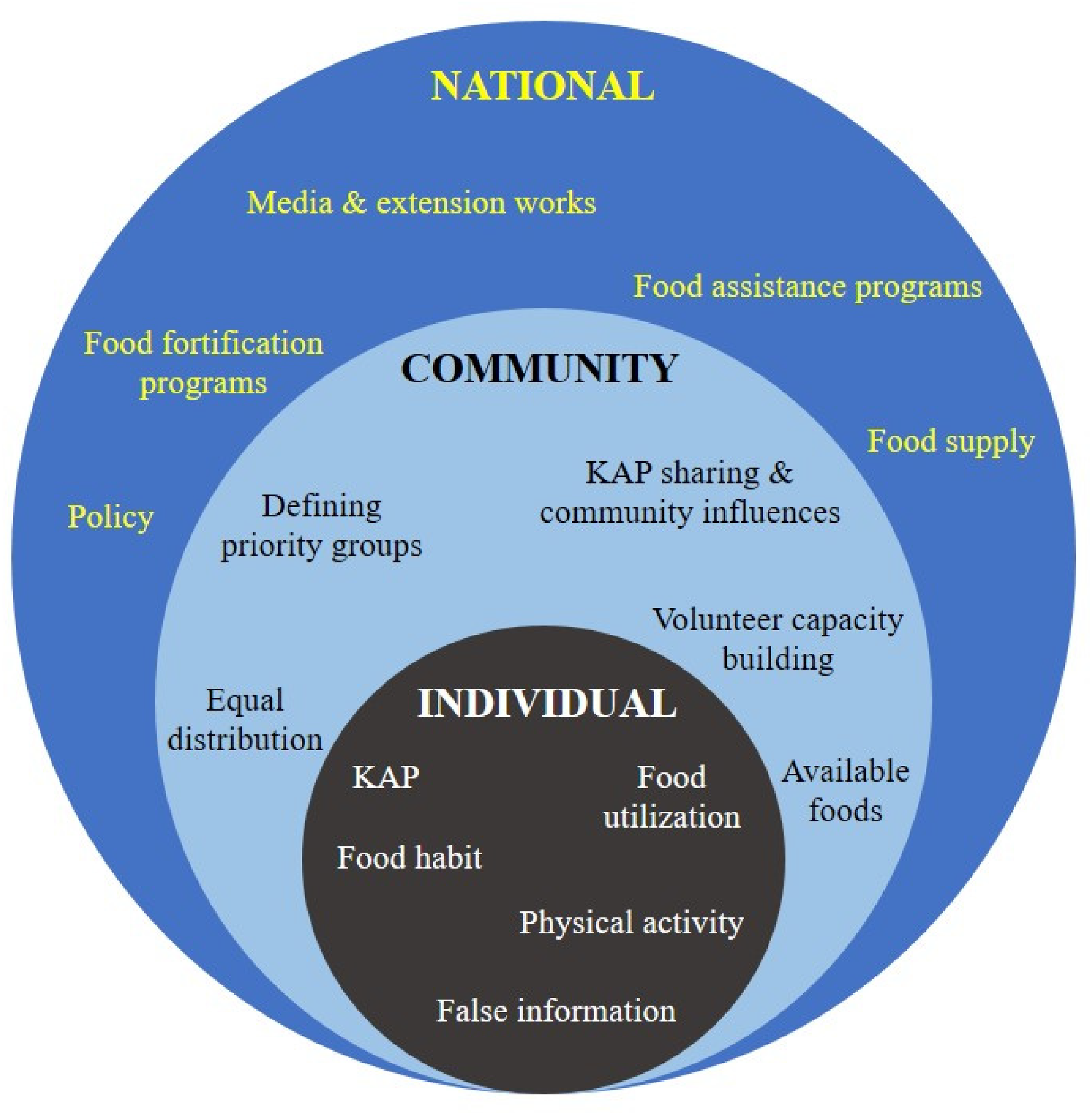
A multilevel framework for action to support the nutritional health of Rohingya refugees during COVID-19.
Individually, the relationship between diet and immunity is the driving force behind the vast majority of nutrition and dietary recommendations for combating viral infections, including COVID-19 (Naja and Hamadeh, 2020). Therefore, those within the camps must have the appropriate knowledge and attitude regarding this topic. For financial necessity, many refugees are found selling food to members of the host community. Additionally, it is desirable to utilize the provided foods for oneself and one's family. Even for brief durations, low levels of physical activity can be detrimental to physical and mental health. The Rohingya are already in a position where they have nothing to do, and the situation has significantly deteriorated due to their confinement. Therefore, it may be advantageous to train and accustom them to regular physical exercise. Importantly, steps should be taken to limit the dissemination of false information regarding dietary intake and nutritional management.
Due to transportation, distribution, and allocation challenges, the COVID-19 outbreak's repercussions at the community level primarily threaten food accessibility and availability. Due to the decreased frequency of visits, programmers may be able to increase the number of rations provided to beneficiaries at each visit if sufficient therapeutic and supplementary food supplies are prepositioned. Prepositioning of inventory is also essential for preparing for potential supply chain disruptions in the event of unanticipated lockdowns. Critical adaptations can be implemented if sufficient supply stocks are available. Instead of deploying service providers from outside the region, community nutrition volunteers from the Rohingya population should be hired to support campaign efforts. During the COVID-19 pandemic, older adults and patients with chronic diseases seem to have been especially vulnerable and at-risk of nutritional imbalance (Naja and Hamadeh, 2020). Food should be equitably distributed, with priority given to children, pregnant women, patients, and aged people. On the other hand, at the level of the community, the Knowledge, attitude, and practice (KAP) of individual refugees should convert into KAP sharing and community influences on KAP-based behaviors.
At the national level, while the government of this country is dealing with the issue of food safety and security, providing adequate health and nutritional support to the Rohingya community is a significant challenge. Instead of importing food, more emphasis should be placed on domestically grown and manufactured agricultural products. Significant policy planning is necessary to facilitate the production, distribution, and availability of this food basket in all camp settings. Food fortification is essential for Rohingya women and children in order to boost their immunity against COVID-19 and prevent prevalent malnutrition and nutritional disorders. To accomplish this goal, local governments, nongovernmental organizations, and food industries may launch a pilot food fortification program on a small scale. The significant prevalence of anemia and lack of dietary diversity underscores the need for more varied family rations, greater distributions of additional fortified foods, and continuous breastfeeding support. To avoid big crowds of children and caregivers, vitamin A pills should be delivered door-to-door as opposed to at fixed distribution facilities. For such a door-to-door campaign, the utilization of various media, such as leaflets, local newspapers, television, etc., may be advantageous. Utilizing advanced technologies, including as mobile phones, apps, and social media, in Rohingya communities could be one method for addressing these challenges. However, the application of technology may not be adequate for such a circumstance, although some recent studies attempted to employ such an application in humanitarian operations. Drolia et al., (2022) mentioned a number of applications that were used for the refugee peoples around the world. At the same time, some health-related apps were developed for the refuge people in Lebanon (Saleh et al., 2018) and Syria (El-Khatib et al., 2020).
Conclusion
The nutritional status of the Rohingya people in Myanmar was deplorable, and it has not improved while they are living in the various camps in Cox's Bazar. The current COVID-19 pandemic makes their situation considerably more challenging. Women, children, and the elderly are at-risk for malnutrition, which negatively impacts their nutritional health. To improve the nutritional health of these refugees during COVID-19, the government and relevant stakeholders should reconsider existing programs and develop new ones. The framework proposed in this commentary suggests a three-dimensional implementation strategy that will help Rohingya refugees improve their nutritional health not only during the COVID-19 pandemic, but also in the postpandemic period.
Footnotes
Availability of data and materials
Not applicable.
Authors’ contributions
All authors contributed equally to this paper.
Consent for publication
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.