
Abstract
Introduction
Caffeine (3,7-dihydro-13,7-trimethyl-1H-purine-2,6-dione) was first discovered in coffee in 1820 and has taken its place as one of the most consumed central nervous system stimulants in the world (Butt and Tauseef Sultan, 2011; Egawa et al., 2006; Quadra et al., 2020). The use of caffeine has become a habit since the past, and it has been used and continues to be used as an appetite suppressant to stay awake and even lose weight (Cappelletti et al., 2014; Schubert et al., 2017). Caffeine intake is thought to be at the highest level in Scandinavian countries, where coffee consumption is the highest in the world (Köksal et al., 2017).
Taking caffeine in the moderate dose range (200–300 mg) for adults has been associated with a reduction in the risk of chronic diseases such as type-2 diabetes and obesity, along with health benefits such as keeping people fit, increasing athletic performance and concentration, and stronger memory. In addition, up to 400 mg of caffeine per day for adults and children, and 200 mg per day for pregnant and lactating women is considered safe (Gaspar and Ramos, 2016; Kumar et al., 2018). However, using more than safe doses may cause an increase in headache, anxiety, hypertension and cardiovascular disease risks (Chen et al., 2019; Gaspar and Ramos, 2016; Heckman et al., 2010).
Caffeine is usually obtained from sources such as coffee, tea, cola, chocolate, cocoa and is found locally in the kola nut in Africa and the guarana seed in Brazil (Kumar et al., 2018; Oestreich-Janzen, 2010; Verster and Koenig, 2018). After caffeine is absorbed into the body, it is quickly absorbed and almost all of the absorption occurs in the stomach and small intestine. Approximately 30–60 min after caffeine intake, the plasma concentration increases and it is distributed to all organs including the brain after absorption occurs (Bessada et al., 2018; Ludwig et al., 2014). Genetic factors as well as age, gender and hormones play an important role in the metabolism of caffeine (Nehlig, 2018; Zhou and Hyppönen, 2019).
Cardiovascular diseases (CVDs) are one of the leading health problems in the world (De Rosa et al., 2018). World Health Organization (WHO) predicts that 32% of deaths in the World (17.9 million) are caused by cardiovascular diseases in 2019 (WHO, 2021).
Caffeine can have significant effects on the cardiovascular system in the body (Holstege and Holstege, 2014). At the same time, the central nervous system and some related diseases affect many systems (Kolahdouzan and Hamadeh, 2017), especially the inflammatory response (Cano-Marquina et al., 2013). Caffeine consumption and its effects on individuals as a result of consumption differ, and high amounts of caffeine intake (>400 mg) may have some acute and chronic toxicity effects in general (Nehlig, 2018; Willson, 2018). Therefore, it is advocated that caution should be exercised in caffeine consumption due to its potential harmful effects on individuals with heart disease and pregnant women (Reyes and Cornelis, 2018; Temple et al., 2017).
Caffeine has direct or indirect effects which occur as a result of different mechanisms and molecules on vascular tissue. It achieves these effects by interacting with cardiovascular receptors in a dose-dependent manner (Voskoboinik et al., 2019). There is conflicting evidence as to whether caffeine doses a risk of cardiovascular disease, but in recent years, the view that caffeine reduces vascular function, causes hypertension, ventricular arrhythmias, and cardiac arrest due to fibrillation has become increasingly prevalent. Contrary to these studies, there are also studies showing the positive effects of caffeine-containing beverages on certain cardiovascular markers (Muraro et al., 2016; Papamichael et al., 2005; Turnbull et al., 2017).
It has been revealed that caffeine taken through the diet causes a continuous increase in blood pressure. Considering the important relationship between high blood pressure and the risk of cardiovascular disease, it is stated that caffeine is an indirect cardiovascular disease trigger, but individuals with regular caffeine consumption may develop different levels of tolerance to the acute effects of this substance (James, 2004; Köksal et al., 2017). A decrease in heart rate was determined as a result of moderate caffeine consumption. This decrease is due to the fact that blood pressure regulators of the body create negative feedback against increased blood pressure (Grant, Magruder and Friedman, 2018). It is known that caffeine has positive effects on mental state as well as reducing the risks of diabetes, Parkinson's and Alzheimer's disease (Kumar et al., 2018). In some recent animal studies, it has been shown that caffeine has a beneficial effect on some parameters which of indicators such as hypertension, endothelial dysfunction, and inflammation that are indicative of cardiovascular diseases (Turnbull et al., 2017; Zulli et al., 2016).
Therefore, this study aimed to investigate caffeine intake in cardiovascular patients and those without a diagnosis of the disease.
Methods
Sample size and data collection
The study which is a cross-sectional descriptive was conducted with participants who applied to Tekirdağ Namık Kemal University (TNKU) Health Practice and Research Hospital between October 2019 and January 2020.
The sample of study was selected from people who applied to the TNKU cardiology policlinic. Total of 120 individuals who informed consent and met study eligibility criteria participated. Aged between 18–65 and had blood parameters for the last three months were inclusion criteria. Professional athletes, hospitalized, had a surgical operation in the last year, diabetic, and don't have blood analysis results were exclusion criteria for the study. Fifty of the cardiovascular diseases (CVDs) diagnosed people (follow-up patient) and 40 of the non-diagnosed (ND) with any chronic diseases people as a total of 90 people accepted to participate in the study. The study has been completed with 90 individuals.
The individuals who met the conditions for participation in the study were asked to fill in a questionnaire asking demographic information, anthropometric measurements (height (cm), weight (kg), waist circumference (cm)), and eating habits using the face-to-face interview method. The waist circumference of the individuals was measured by the researchers with a tape measure. According to the evaluated questionnaire results, individuals who had one or more of the exclusion criteria including being pregnant and breastfeeding, obese, diagnosed with diabetes, hypertension, liver diseases, and kidney diseases were not included in the study.
Ethical statements
This study was conducted according to do guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by the TNKU Faculty of Medicine Non-invasive Clinical Research Ethics Committee with ethics number 2019.109.07.05.
Food frequency
Individuals participating in the study were asked to fill out the food frequency questionnaire by considering the last year. The food frequency questionnaire has been revised from Walter Willet's food frequency questionnaire (Grobbee et al., 1990; Lopez-Garcia et al., 2006; López-Jaramillo et al., 2013; Mekary et al., 2012). This questionnaire includes questioning the consumption frequency of foods and beverages with high caffeine content. Food consumption amounts were recorded in terms of measure and gram/milliliter and daily consumption amount was calculated based on these recorded values. The participants were presented with 7 options in terms of consumption frequency of foods. These options were every day, 5–6 times a week, 3–4 times a week, 1–2 times a week, once in 15 days, once a month and no consumption at all. Participants were asked to fill in one of these options and then asked how much they consume at a time. The results of the food frequency questionnaire were evaluated with the BeBiS (nutrition information systems) software (“BeBis,” 2021). The amount of caffeine intake has been defined with BeBiS program results.
Laboratory findings
Within the scope of the study, fasting blood glucose (FBG), triglyceride, total cholesterol, LDL cholesterol and HDL cholesterol biochemical parameters of the participants were examined. Biochemical parameters were obtained from the data that participants had at the time when they applied to the policlinic or from the database of TNKU Health Practice and Research Hospital. While collecting the biochemical parameters of the participants, it was paid attention that the blood was given no more than three months ago. Individuals who did not give blood in the last three months were not included in the study.
Statistical analysis
The statistical analysis of the research data was done with IBM SPSS Statistics software package version 22. Basic statistical methods such as mean and standard deviation were used in the evaluation. Chi-square and Fisher's exact tests were used in a comparison of percentages and proportions, and Mann Whitney U test was used in a comparison of two numerical groups. Results were accepted at 95% confidence interval and the significance level as p <0.05.
Results
The average age of the ND group was 33.65 ± 11.85 years, and the average age of the CVDs group was 50.92 ± 11.39 years as can be seen in Table 1. While 67.50% of the individuals in the ND group were women, 38% of the CVDs group were women. There was no statistically significant difference between the two groups in terms of evaluating physical activity and sleep duration (p > 0.05).
General Characteristics of the Study Groups.
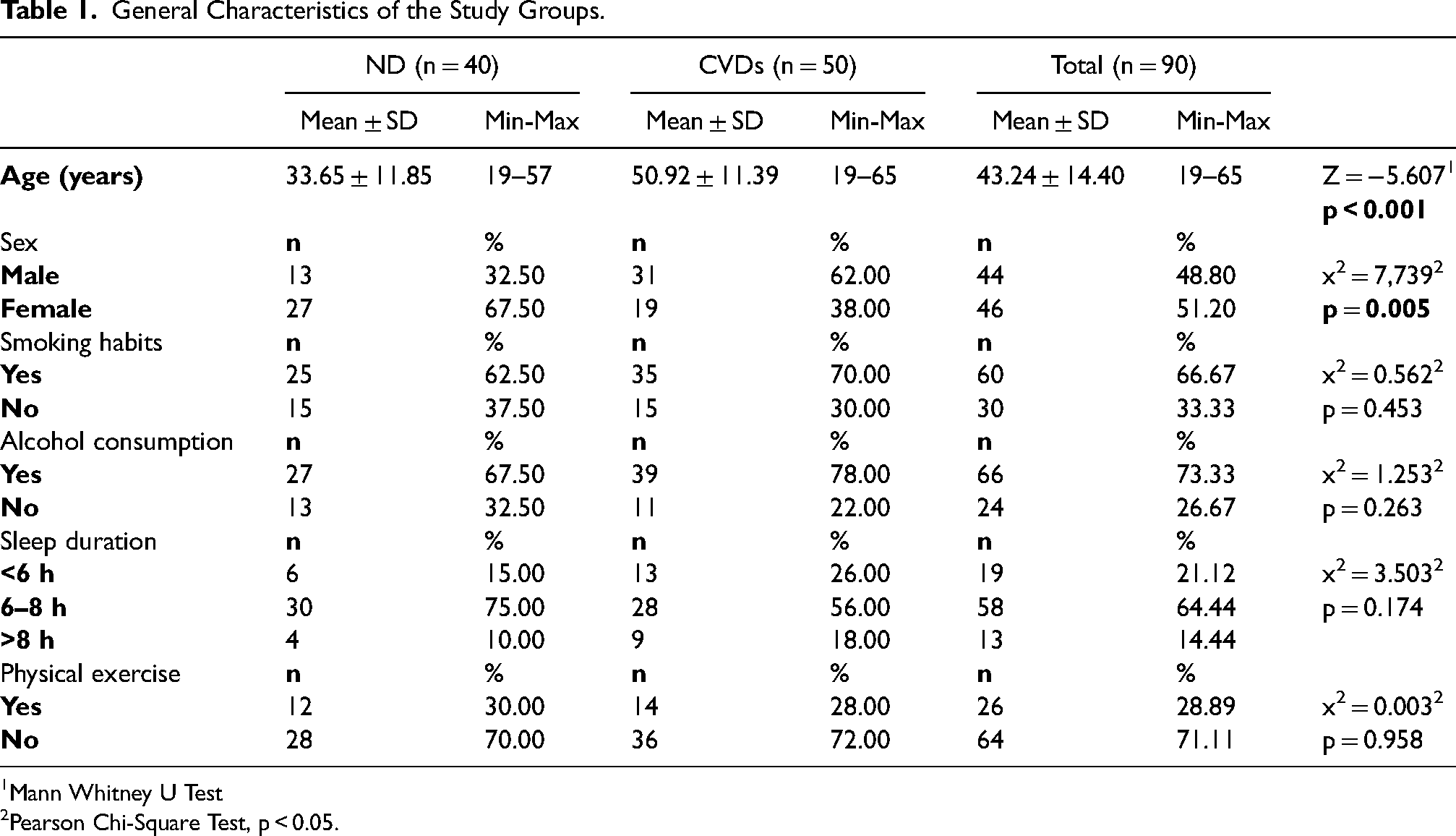
Mann Whitney U Test
Pearson Chi-Square Test, p < 0.05.
When Table 2 was examined, it was found that 20% of the CVDs group consumed 4 meals a day while 35% of the ND group consumed 3 meals a day. Furthermore, there was no statistically significant difference between the two groups in terms of meal patterns (p > 0.05).
Eating Habits of the study groups.
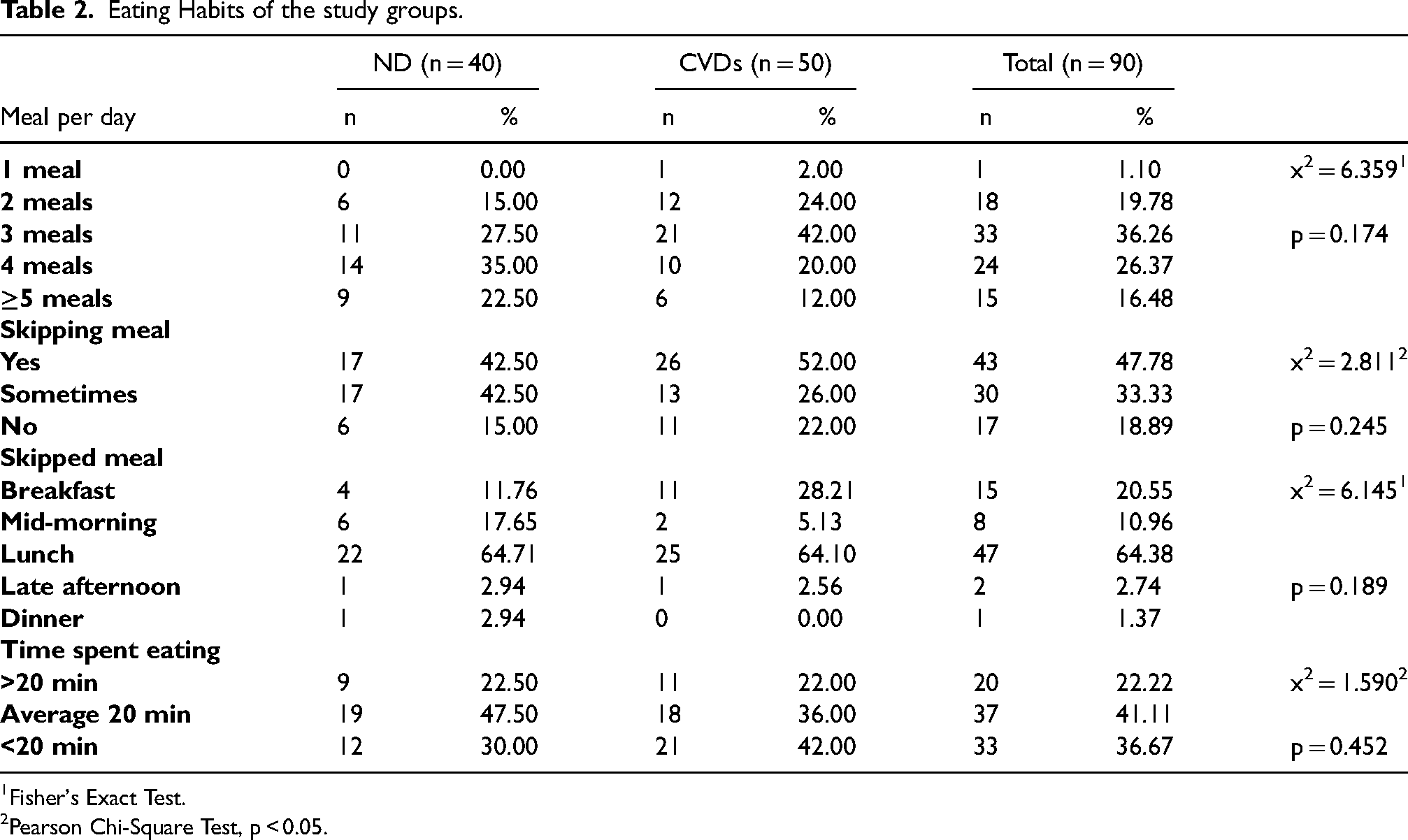
Fisher's Exact Test.
Pearson Chi-Square Test, p < 0.05.
When BMI and waist circumference were evaluated, a statistically significant difference was found between the two groups (p < 0.001). Furthermore, LDL cholesterol and total cholesterol did not show a statistically significant difference between the two groups (p > 0.05) (Table 3).
Investigation of the Body Mass Index (BMI), Waist Circumference and Biochemical parameters of the Study Groups.
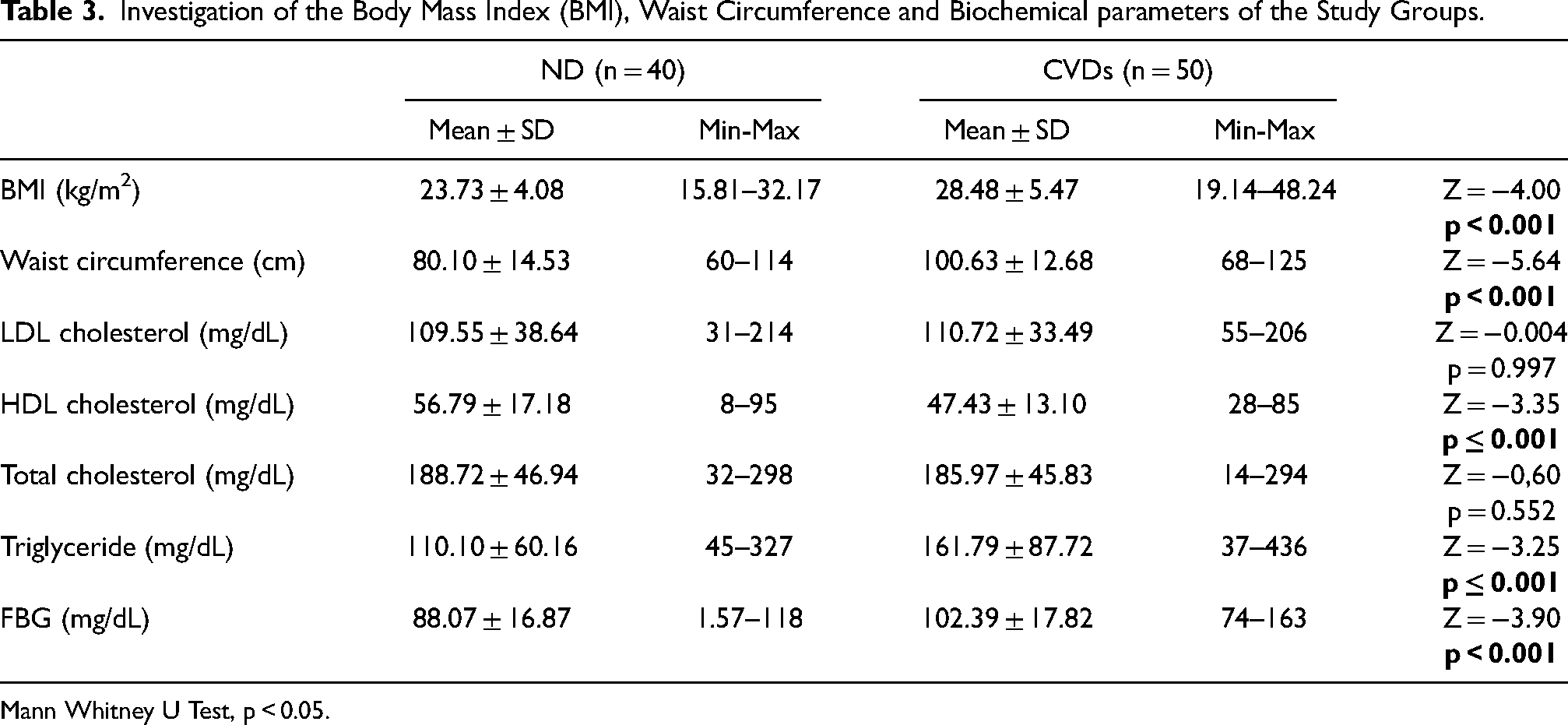
Mann Whitney U Test, p < 0.05.
There was no statistical significance between the two groups in terms of total caffeine (total caffeine intake was calculated by using BeBis program) and black tea consumption. It was determined that green tea, Turkish coffee, filter coffee and milk chocolate consumption were significantly higher in the ND group than the CVDs group (p < 0.001) (Table 4).
Total Caffeine and Caffeine-Containing Food Consumption Status of the Study Groups.
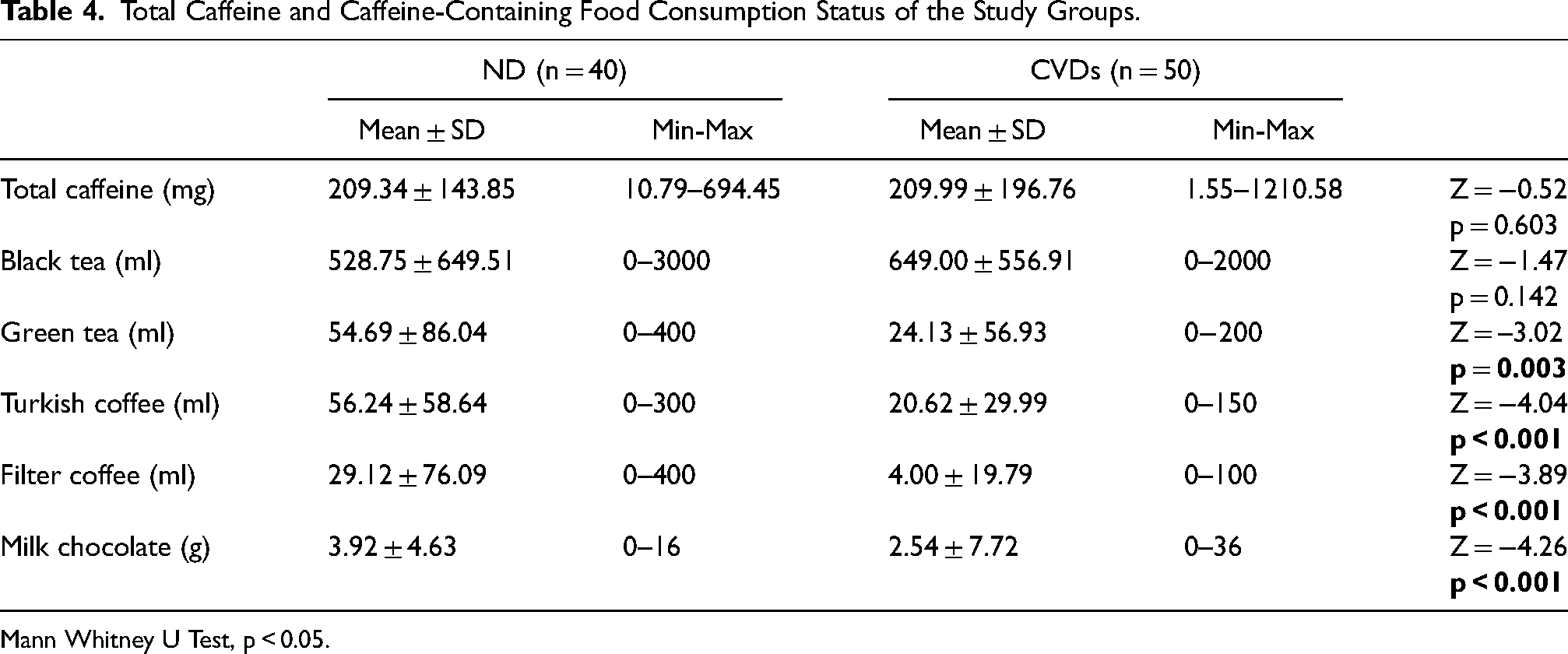
Mann Whitney U Test, p < 0.05.
It was observed that 77.5% of the ND group and 94% of the CVDs group had black tea consumption every day while 67.5% of the ND group and 96% of the CVDs group did not have filter coffee consumption. When the consumption of Turkish coffee was evaluated, it was determined that 52.5% of the ND group and 26% of the CVDs group consumed it every day (Supplemental Figure 1–2).
When the correlation between the total amount of caffeine consumed by the study group and blood parameters was examined, it was seen that there was a negative and significant correlation with HDL cholesterol levels, while there was no significant correlation with other biochemical parameters (Table 5).
Correlations between Total Caffeine and Biochemical parameters.
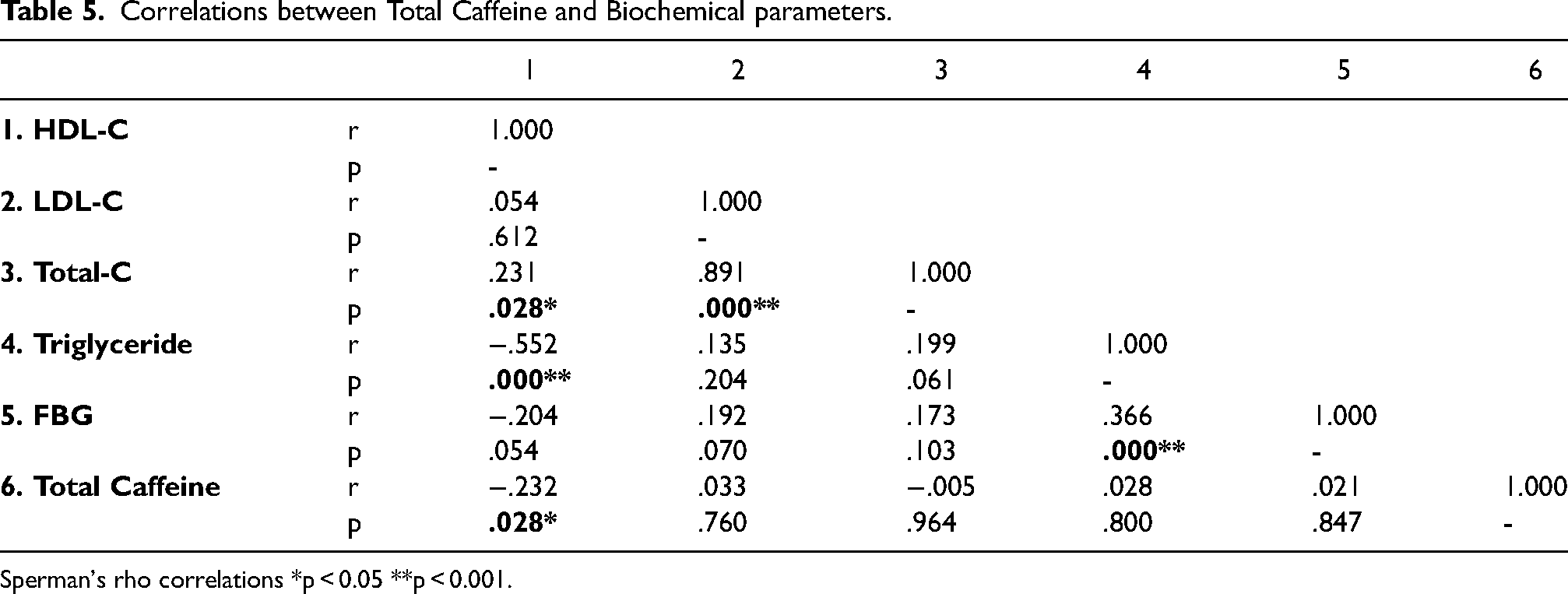
Sperman's rho correlations *p < 0.05 **p < 0.001.
While the correlations between caffeine consumption and blood parameters were not significant in the ND group, a negative correlation was observed between caffeine consumption and HDL levels in the CVDs group (r = − 0.309, p = 0.029). In addition, there was a moderately significant correlation between fasting blood glucose and LDL (r = 0.308, p = 0.030) and total cholesterol levels (r = 0.321, p = 0.023) in the CVDs group.
Discussion
It has been shown that caffeine can be beneficial or harmful in different groups depending on the dose. However, there is uncertainty about the effect of this molecule, which is frequently taken into the body, on cardiovascular diseases. The aim of this study is to evaluate caffeine intake in individuals with or without cardiovascular disease and to determine whether it is associated with some biochemical parameters.
Increased blood glucose level in non-diabetic individuals is considered as a marker for the risk of cardiovascular disease (Adeva-Andany et al., 2019). In a study involving healthy individuals, it was shown that increased caffeine consumption for 1 week did not cause a significant difference in serum glucose level compared to placebo intake (MacKenzie et al., 2007). In non-diabetic persons, consumption of ≥ 4 cups/day of coffee did not change the blood glucose level in men compared to those who did not consume it at all, however, decreased it significantly in women (Paynter et al., 2006). In similar studies, there have been no significant contribution of coffee consumption to plasma glucose level between those who consume coffee and those who do not (Mirmiran et al., 2018; Yamashita et al., 2012). In our results, although the total caffeine intake was similar between with CVDs and without CVDs individuals, coffee consumption was significantly higher in ND individuals, and in parallel with other studies, the FBG level was found significantly lower than the CVDs group.
Among the general risk factors of cardiovascular diseases, the values of the blood lipids as total cholesterol, triglyceride and LDL cholesterol are higher than the reference value, while HDL cholesterol is lower (Pletcher and Moran, 2017). Besides, it has been shown that caffeine consumption more than 200 mg significantly increased the total cholesterol level in women (Shirlow and Mathers, 1984). When the consumption of caffeinated and decaffeinated coffee, there was no significant difference in terms of total cholesterol, LDL and HDL in both men and women (Lopez-Garcia et al., 2006). In another study, a significantly negative relationship was reported between coffee consumption and triglyceride level, a significantly positive association with total cholesterol and LDL cholesterol, and no relationship with HDL cholesterol (Yamashita et al., 2012). More consumption of unfiltered coffee was associated with increases in total cholesterol, LDL cholesterol and triglycerides, according to a meta-analysis based on results from 12 studies (Cai et al., 2012). In the present study, lower coffee consumption, significantly higher triglyceride and low HDL levels were found in individuals with CVDs compared to the ND group, moreover, there was no statistically significant difference in total cholesterol and LDL levels between the two groups.
In parallel with the increase in daily coffee consumption from none to 4≥ cups, it has been determined that the incidence of the cardiovascular disease tends to increase in individuals younger than 60 years of age, and to decrease in individuals over 60 years of age (Grobbee et al., 1990). In a study examining the relationship between caffeinated coffee consumption and cardiovascular diseases in elderly individuals, no significant difference in terms of cardiovascular, cerebrovascular and coronary events was found between those who did not consume coffee at all and those who consumed 1≥ cup/day (Greenberg et al., 2008).
Lopez-Garcia et al. showed that long-term coffee consumption was not associated with coronary artery disease in men, but positively in women (Lopez-Garcia et al., 2006). Moreover, in the same study, it was found that high coffee consumption (6 cups/day) reduced the risk of death from coronary artery disease. Furthermore, there was no significant difference in calcified atherosclerotic plaque formation between adult men and women who consume and do not consume coffee (Patel et al., 2017).
In our study, both Turkish coffee and filter coffee consumption was found to be significantly higher in the ND group than CVDs group. When non-diagnosed individuals were compared with those with coronary artery disease, which constitutes a significant part of the CVDs group, the significant relationship between the two groups did not change. It was determined that cardiovascular events were significantly lower in individuals who consume 1 cup of tea daily compared to those who do not consume tea (Miller et al., 2017). In another study, it has been shown that increasing black tea consumption up to 6 cups/day decreases the occurrence of coronary artery disease, however, moderate coffee consumption can also reduce the risk of this disease (de Koning Gans et al., 2010). In the results we obtained from this study, while there was no significant difference between ND individuals and individuals with CVDs in terms of black tea consumption, green tea consumption was found to be significantly higher in the non-diagnosed group.
As a result, it is still unknown whether daily caffeine intake has an effect on cardiovascular disease, independent of other risk factors. The diversity of cardiovascular diseases and risk factors cause contradictory results. In ND individuals participating in the study, consumption frequency of foods containing caffeine was found to be significantly higher than those with CVDs, while the total amount of caffeine consumed was similar. It is thought that this study can contribute to the literature in terms of eliminating CVDs risk factors as much as possible and disease homogeneity in the CVDs group. More detailed and standardized studies are needed on different doses of caffeine effect on CVDs.
Limitations and strengths
Individuals’ blood pressure has not been assessed because of a lack of records. In addition, other foods consumed by subjects other than caffeine-containing foods as a limiting factor in terms of cardiovascular diseases. The present study is important because in Turkey have not been enough studies about caffeine intake in CVDs diseases.
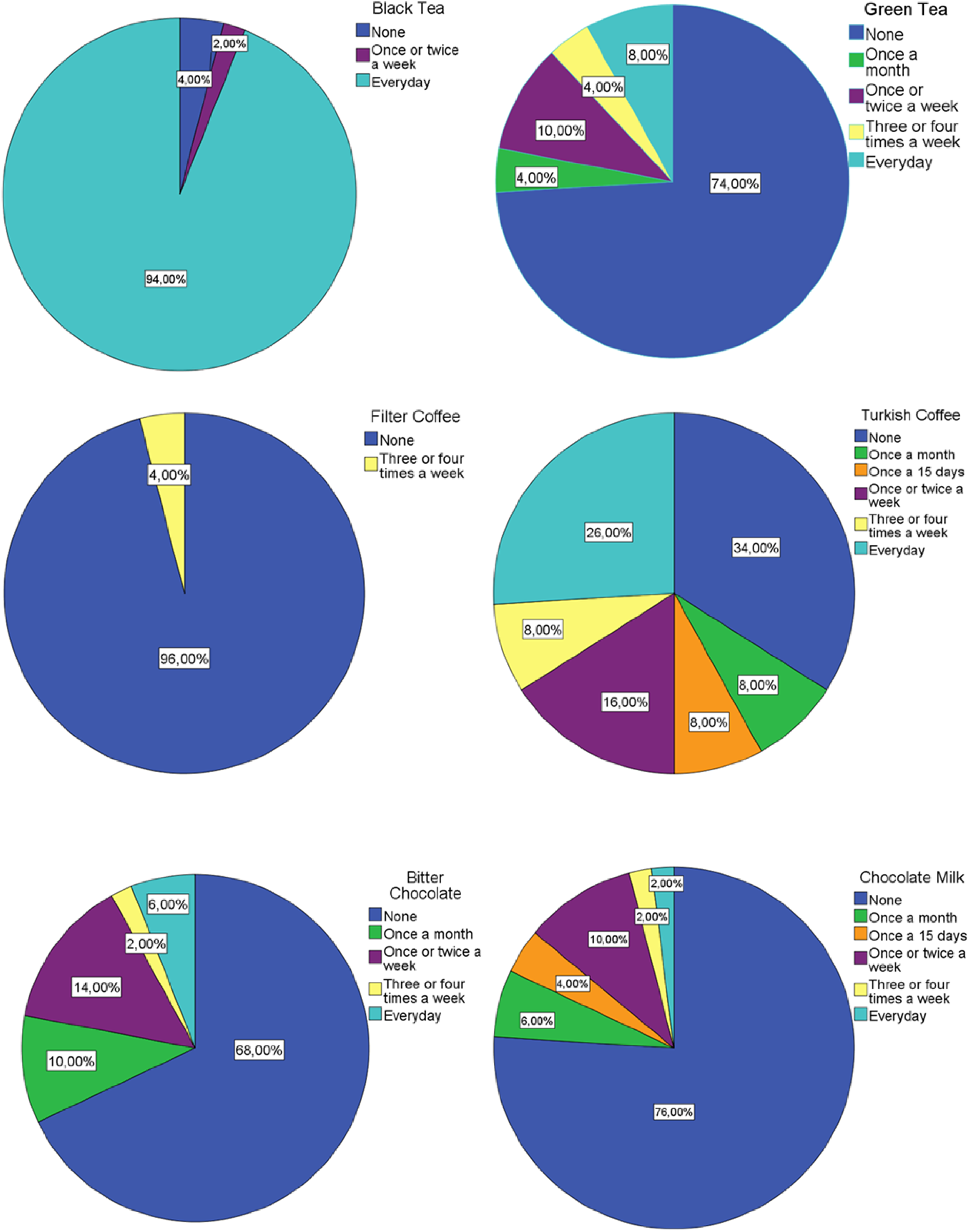
Black Tea, green, filter coffee, turkish coffee, bitter chocolate, chocolate milk of consumption in CVDs group.
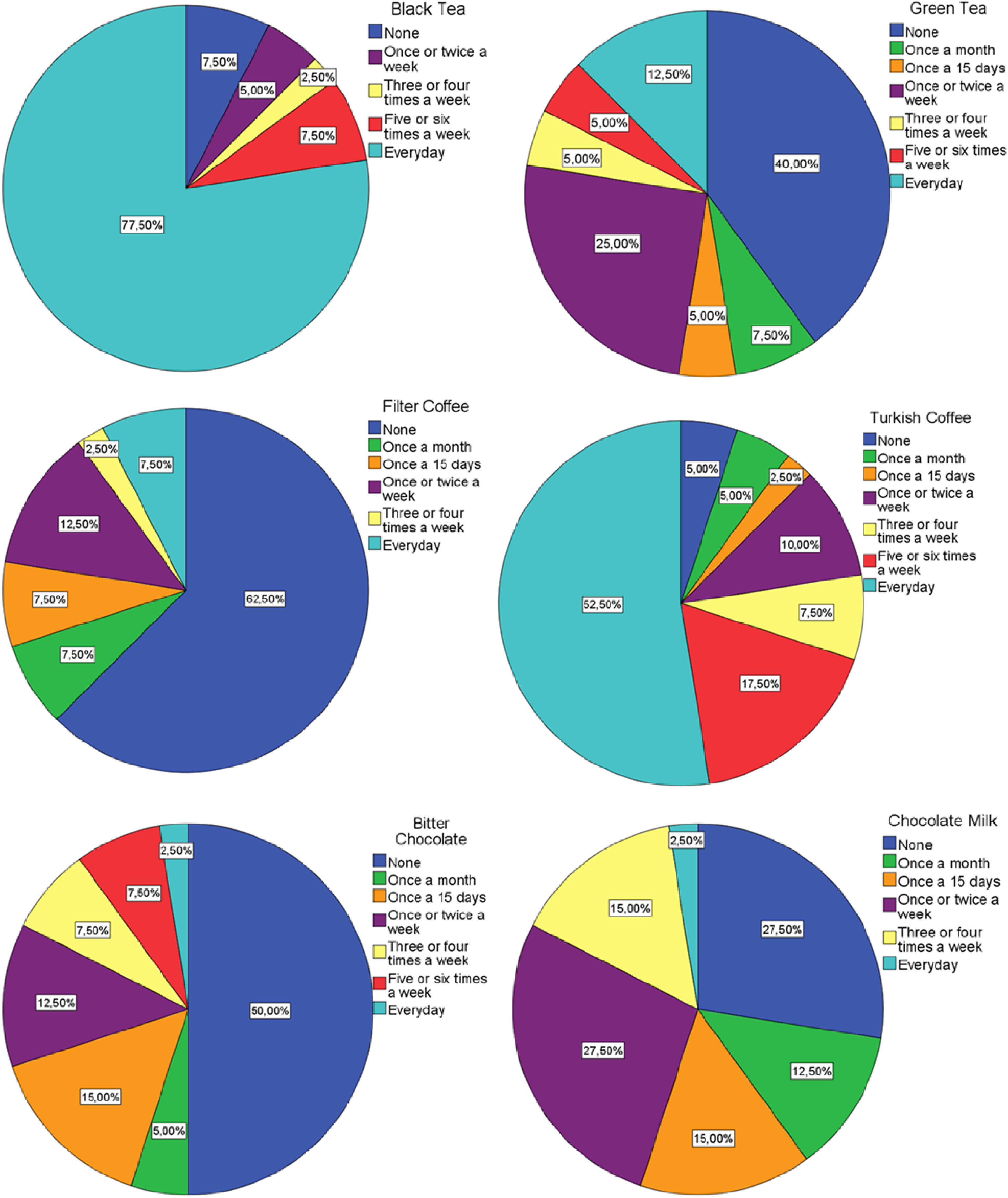
Black Tea, green, filter coffee, turkish coffee, bitter chocolate, chocolate milk of consumption in ND group.
Footnotes
Acknowledgment
Thanks to the participants and care staff for their cooperation.
Availability of data and materials
Data will be made available upon request
Authors’ contributions
C. Bozkir, S. Tuggüm, N Kagan and B. Nizam designed the study, C. Bozkir, S.Tuggüm, N Kagan, B. Nizam and S. Alpsoy collected data, C. Bozkir, S. Tuggüm, N Kagan and B. Nizam analyzed the data and wrote the manuscript. All the authors have read and approved the final draft.
Consent for publication
The authors give permission for the Journal to publish this work.
Ethical approval
This study was conducted according to do guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by the TNKU Faculty of Medicine Non-invasive Clinical Research Ethics Committee with ethics number 2019.109.07.05.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.