
Abstract
To date, the primary and only treatment recommended for effective management of celiac disease (CD) is adherence to a strict gluten-free diet (GFD) which entails a new approach to eating that affects the social quality of life (QoL) and physical activity (PA) of patients. This cross-sectional study aimed at assessing the social QoL and PA of adult Lebanese CD patients aged between 18 and 59 years old who are following a GFD. An online CD questionnaire was administered to 136 Lebanese celiac participants on a GFD. The findings of this study show a significant association between celiac patients following a GFD and their social QoL (P-value = 0.0001). The results also showed a significant association between the same population and their PA (p-value = 0.0001). Further awareness-raising and learning activities about gluten-free products are needed to improve the adherence to a strict GFD to facilitate its availability to the Lebanese population.
Introduction
Celiac disease (CD) is an autoimmune disorder triggered by sensitivity to dietary gluten in genetically susceptible persons (Theethira & Dennis, 2015; Lionetti & Catassi, 2015; Murray et al., 2008; Parzanese et al., 2017). The pathogenesis of this multifactorial illness can be triggered by environmental (gut microbiota, breastfeeding, viral infections, and smoking) or genetic (HLA DQ2 and DQ8 genes) factors (Rondanelli et al., 2019). However, the major factor involved in the etiology of celiac sprue is gluten consumption (Rondanelli et al., 2019). Celiac patients may have several deficiencies due to their malabsorption to some nutrients and their restriction to many foods which render their nutritional quality of life different from non-CD patients (Theethira & Dennis, 2015; Murray et al., 2008; Parzanese et al., 2017).
Health-related quality of life (HR-QoL) is a multi-dimensional concept that encompasses domains related to nutritional, mental, social, physical, and emotional functioning (Sosnowski et al., 2017; Wanden-Berghe et al., 2009; Amarantos & Dwyer, 2001). Scales aid in measuring the results of received healthcare and can be specific when related to a particular population, condition, or issue (Mosteller and Falotico-Taylor, 1989; Walker et al., 2012). A lifelong GFD requires an adherence to a strict pattern of eating that negatively affects the patient's life (Deepak et al., 2018). Social life plays an important role in being compliant with a gluten-free diet (Deepak et al., 2018). Celiac patients must be cautious when eating outside, at school, work, or at cocktail parties as it is challenging for them to find hidden sources of gluten in a discreet manner in front of family and friends without being judged (Deepak et al., 2018). A study conducted by Deepak et al. (2018) shows that the means of mental health composite scale score (MCS) and physical health composite scale score (PCS) are inferior in CD-patients with a worse HR-QoL in comparison to healthy controls but can be improved with a GFD. Moreover, a study conducted by Passananti et al. (2012) showed that patients suffering from CD suffer from fatigue and tend to reduce their social activities, which in turn could decrease their physical activity levels. Dowd et al. (2019) highlighted low levels of PA in CD female patients following a GFD based on the International Physical Activity Questionnaire. A similar study conducted by Burger et al. (2017) highlighted slightly worse HR-QoL scores while comparing CD patients on a GFD to healthy control. However, results showed the existence of a significant association between GFD and HR-QoL. GFD significantly improves HR-QoL for psychological general well-being (PGWB) (P-value = 0.008), PCS (P-value = 0.008) and MCS (P-value = 0.009) (Burger et al., 2017). The association was also seen in Harnett & Myers (2020) study, whereby for people following a GFD, the social subscale mean scores at baseline (41 ± 6.12) was less than the optimal score of 49. In contrast, a cross-sectional study carried out on in CD patients in Saudi Arabia revealed no existence of a relation between GFD and HR-QoL when controlling for age and educational degree (Al-Saikhan, 2020).
Nevertheless, regardless of progress in symptoms, patients will remain restricted in a way by various factors due to the fear of contamination of food with gluten (Deepak et al., 2018). To date, the primary and only cure suggested for effective management of CD is adherence to a strict gluten-free diet (GFD) (Progress et al., 2007; Caio et al., 2019). Being aware of gluten-containing foods, health awareness, and sessions on GFD could be beneficial because CD patients usually attribute their diet to negative emotions, feelings of isolation, frustration, and avoidance (Al-Toma et al., 2019; Pelkowski & Viera, 2014; Samasca et al., 2014). Gluten-free foods are many and can be found in a natural form in common nutritious sources such as vegetables, nuts, fruits, unprocessed meat, fish, poultry, eggs, and in whole grains like rice, quinoa, corn, buckwheat, amaranth, oat, etc. (Banai, 2004; Hlywiak, 2008). For that reason, it is always recommended to carefully read the label of any food product before consuming them (Hlywiak, 2008). However, gluten-free foods are often processed and can be high in saturated fats, sugar, sodium, and calories with a very low nutrient concentration such as gluten-free snacks (chocolate, chips, cookies, etc.) (Hlywiak, 2008; Vici et al., 2016; Pellegrini and Agostoni, 2015). This reality renders it a daily challenge for CD patients to consume healthy, gluten-free meals but instead rely on corn, potato, or tapioca flour as their source of nutrition (Panda and Garber, 2019). Additionally, gluten-free products are very expensive and less available, which further exacerbates accessibility and affordability barriers (Gorgitano & Sodano, 2019).
Prevalence of Cd in the Middle East and North Africa (MENA) region
CD is a major global public health problem (Singh et al., 2018; Barone et al., 2016). Unfortunately, the exact worldwide prevalence of CD is still unknown (Singh et al., 2018). Nevertheless, a meta-analysis shows that the prevalence of CD changes with age, sex, and location (Singh et al., 2018). CD prevalence in the Middle East and North Africa (MENA) area has significantly increased over the past decade to reach rates comparable to those studied in Western countries (Cataldo & Montalto, 2007). Moreover, the elevated observed frequencies of CD in the MENA area were correlated with the broad intake of wheat and barley as part of the Mediterranean eating habits, as well as the abundance of CD-predisposing genes in the majority of Arab countries (Cataldo & Montalto, 2007). Even though the prevalence and severity of CD is increasing in the Middle East region, there have not been sufficient studies about the disorder in this area (Abu-Zekry et al., 2008; Barada et al., 2010; Ertekin et al., 2005; Rawashdeh et al., 1996; Shamir et al., 2002).
Prevalence of CD in Lebanon
One of the countries with the highest rates of CD in the region is Lebanon (Barada et al., 2010; Rawashdeh et al., 1996). However, annual census and CD databases in the country have not been updated for decades (Barada et al., 2010; Rawashdeh et al., 1996). Several studies have suggested that there is a significant association between GFD and the social quality of life on one hand, and GFD and physical activity (PA) on the other hand (Deepak et al., 2018; Burger et al., 2017). To our knowledge, no previous research has examined this link in the Lebanese population.
Purpose of study
Therefore, this research aimed at assessing the impact of GFD on social quality of life and PA in Lebanese adults between the ages of 18 and 59 years old. Findings from this study can provide guidance on the development of an educational tool on how to adhere to a GFD, where to find new, available, and affordable substitutes to gluten-containing products, and on how to manage CD patients’ social QoL and PA levels when having to adhere to a GFD. This research will add value to the literature by surveying the Lebanese population and, correspondingly, conducting additional experimental research.
Methods
Study design & sample recruitment
A cross-sectional methodology was adopted and carried out for a period of two months (June-July 2021) to determine the association between following a GFD in relation to the social QoL and the PA of Lebanese CD participants. Precisely, this cross-sectional study involved a validated analytical survey to collect data about the desired factors and associations of interest A total of 142 celiac adults, originally from Lebanon, and aged between 18 and 59 years old were recruited in this study. However, only 136 participants were retained for analysis based on the inclusion/exclusion criteria.
Since there is no registered celiac organization in Lebanon, the authors reached out to “Happy Healthy Celiac”, a group that manages and raises awareness about CD in Lebanon, through its social media platforms (WhatsApp group, Facebook, and Instagram) that contain most CD patients in Lebanon. This group was created by a Lebanese CD patient with the goal of joining the maximum number of Lebanese CD patients to support and help each other in the management of the disease by increasing their knowledge on sources of gluten, grocery stores providing a wide variety of GF food items, and healthcare professionals who are willing to help with the dietary management of the disease. This organization has become known in the country and is currently formed of 300 members due to its widespread social media efforts.
Online recruitment strategies via “Happy Healthy Celiac” social media platforms were established since COVID-19 restrictions and social distancing mandates hindered in-person recruitment efforts. A full list of participants from each platform was generated, and the most active individuals on those platforms were recruited randomly to take part in the study. Simple random sampling was carried out using a sample size based on the proportion approach. Using a 95% CI and a calculated margin of error of 8.5%, the staple size of 136 participants was concluded to be statistically adequate for the scope of the study.
Inclusion and exclusion criteria
Members from the “Happy Healthy Celiac” organization were qualified for the study if they are (a) following a GFD, (b) had a medically confirmed diagnosis of CD from a healthcare professional, (c) were aged between 18–59 years old; (d) are Lebanese citizens; and (e) have accepted to participate in the study. Diagnosis of CD was carried out based on serologic testing or an intestinal biopsy. Excluded from the study were participants who identified as pregnant females, elderly/adolescents, those taking any medications that may affect weight, those having other gastrointestinal conditions that can interfere with a CD diagnosis or the associations we plan on examining (IBS, IBD, GERD, Colitis, Cystic Fibrosis, and Cancer) or those suffering from indigestion or malabsorption symptoms with no medical diagnosis of CDC. Pregnant females were excluded since their dietary needs might interfere with a GFD. Elderly and adolescents were excluded if they are older than 59 years or younger than 18 years, respectively. Additionally, participants who do not speak or understand English were excluded because the survey was in English.
Data collection and data management
Data collection was carried out using an online, validated, and self-administered questionnaire on “Happy Healthy Celiac” social media due to its easy administration, efficiency, and low cost Questions were derived from multiple validated questionnaires on adherence to a GFD in CD patients and its impact on QoL (Burger et al., 2017; Passananti et al., 2012; Selleski et al., 2020). The first set of questions were taken from Passananti’s et al. (2012) study examining the role of exercise and GFD. The second set of questions were taken from Burger’s et al., (2017) study evaluating the QoL of adult celiac in Argentina, and finally, the third set of questions were taken from Selleski’s et al. (2020) study looking at the association between dietary adherence and QoL in CD. Questions were tailored to fit the study objectives and thus assess the impact of GFD on Lebanese CD patients’ social QoL and PA levels (Appendix 2).
Before launching the questionnaire, a pilot study was completed to pre-test the survey, confirm the transition among the various sections and questions, determine the time needed for the completion of the questionnaire, and verify for technical problems. Twenty-five participants were included in the pilot study whose responses were not included in the main study's data. An announcement about the study was posted for 2 months (June and July of 2021) on social media platforms (WhatsApp, Facebook, and Instagram) in conjunction with the study duration. The announcement included an explanation about the study (Appendix 1) and the questionnaire (Appendix 2) with a link to be able to access the online survey.
The access to the questionnaire was on “Q survey” via a link sent on Whatsapp or found at the end of the announcement of the study. Moreover, participants were informed that participation is voluntary. To protect their confidentiality, a unique ID was assigned to the survey prior to the start of the data entry process. Before participation in the study, all the participants signed an informed consent form. The questionnaire comprised a total of thirty-seven questions and was divided into five categories, aiming to collect information about the participants’ socio-demographic characteristics, anthropometrics, CD questions, and finally their social QoL and PA. On average, participants spent 12 min filling the survey. Some participants completed the questionnaire on their own, while others sought support from the research team to understand some questions and answer them correctly. As mentioned previously, a total of 6 participants were excluded from this study since they didn’t fit the inclusion criteria. After considering the inclusion criteria and the completed questionnaires, 136 responses were eligible for data analysis.
Measured variables
Socio-Demographic Characteristics:
Data about participants’ age, gender, pregnancy status (in case of female), their district of residence (Mount-Lebanon, Beqaa, North, Beirut, Akkar, Nabatiyeh, South, Baalbek), their highest level of education (no schooling completed, school graduate, master, PhD/medicine), their personal monthly income in Lebanese Lira (less than 800,000 L.L, between 800,000 L.L and 1,500,000 ||L.L, 1,500,000 L.L and 3,000,000 L.L, and more than 3,000,000 L.L), their current marital status (single, married, divorced, widow), and their medical history (indigestion, malabsorption, and if they take any medications that may affect their weight) (yes/no) (Q1-Q8; Appendix 2).
(b) Anthropometrics (c) Celiac Disease Assessment (d) Social Quality of Life (e) Physical activity
Participants were asked to specify their height (cm) and weight (kg) to be able to classify their body mass index (BMI) based on the World Health Organization (WHO) criteria (Q9-Q10; Appendix 2).
This section collected information about CD (Q11-Q18; Appendix 2). Participants were asked if they were medically assessed for CD using serologic testing or biopsy (no/ yes, serologic test/ yes, biopsy), the period since they were diagnosed (less than 1 year, 1–4 years, 5–10 years, > 10 years), the symptoms they suffered from before their CD diagnosis (none, abdominal pain/bloating, classic diarrhea predominant, other) as well as the period they suffered from those symptoms (less than 1 year, 1–4 years, 5–10 years, > 10 years). They were also asked if they are following a GFD or not (yes/no), the period they have been on this type of diet (less than 1 year, 1–4 years, 5–10 years, > 10 years), if they continued to suffer from CD symptoms despite adherence to a GFD (yes/no), and finally if they are finding it difficult to follow a GFD (yes/no).
In this part of the questionnaire, questions were related to the participants’ social QoL in association with GFD (Q19-Q25; Appendix 2). Participants were asked if they feel socially stigmatized, feel limited in eating meals with coworkers, have trouble socializing with friends and family, find difficulty while traveling or taking long trips, were not living a normal life, refuse or avoid an invitation for dinner with friends or relatives, or feel isolated from or excluded by others. All those questions were directly associated with the GFD of the participants and were answered by the same Likert-scale (not at all/slightly, moderately, quite a bit, a great deal).
Finally, in this last section, participants were asked about their PA levels (Q26-Q37; Appendix 2). This section consisted of two parts: the PA rate of the CD patients, and the changes observed after following a GFD. First, the patients were asked if they considered themselves active (not at all/slightly, moderately, quite a bit, a great deal). After that, they were asked about the time of their vigorous or moderate intensity training per week (2 times per week or less, 3–5 times per week, more than 5 times, other) as well as its duration (60 min per week or less, 60–120 min per week, more than 150 min per week, other). In addition, patients were asked if they have been bothered by low energy levels, headaches, if they encounter any difficulties with recreational activities or sports, and how much intellectual and physical energy they had before and after following a GFD (not at all/slightly, moderately, quite a bit, a great deal).
Data analysis
Data entry and statistical analysis were conducted using Statistical Package for the Social Sciences software, SPSS version 25. Socio-demographic data and CD questions were analyzed using descriptive statistics including means, frequency, and standard deviation for each of age, gender, geographical location, level of education, income level, marital status, length of time since diagnosis, income, weight, and height. CD identification was assessed through a binary variable (yes/no). As for the continuous variables of social QoL and PA, they were measured through a series of questions using a 4-point Likert scale as already mentioned (not at all/slightly, moderately, quite a bit, a great deal). The lower the score for social QoL or PA, the worse it was. Therefore, celiac dietary adherence was also assessed through a binary variable (yes/no). BMI, which is calculated as the body weight (in kg) divided by the height (in m2), was recorded and classified per the WHO criteria as underweight (<18.5), normal (18.5–24.9), overweight (25–29.9), or obese (≥30). BMI was collected as a continuous variable and converted to z scores for age and grouped according to the WHO standards for descriptive purposes.
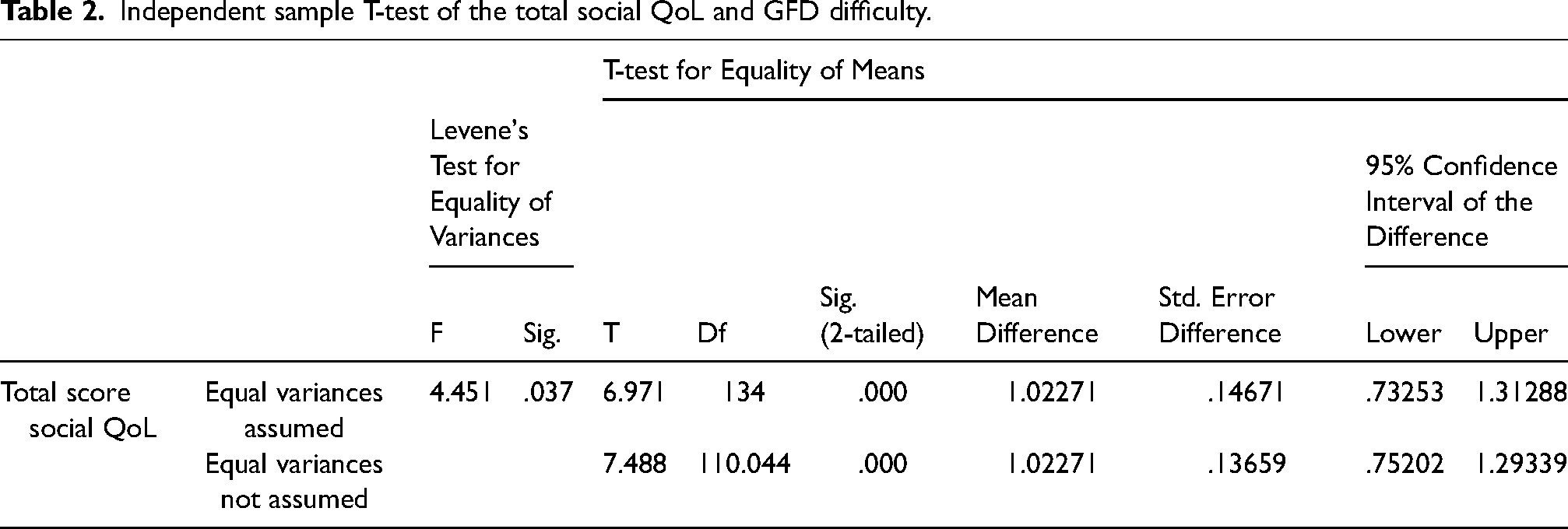
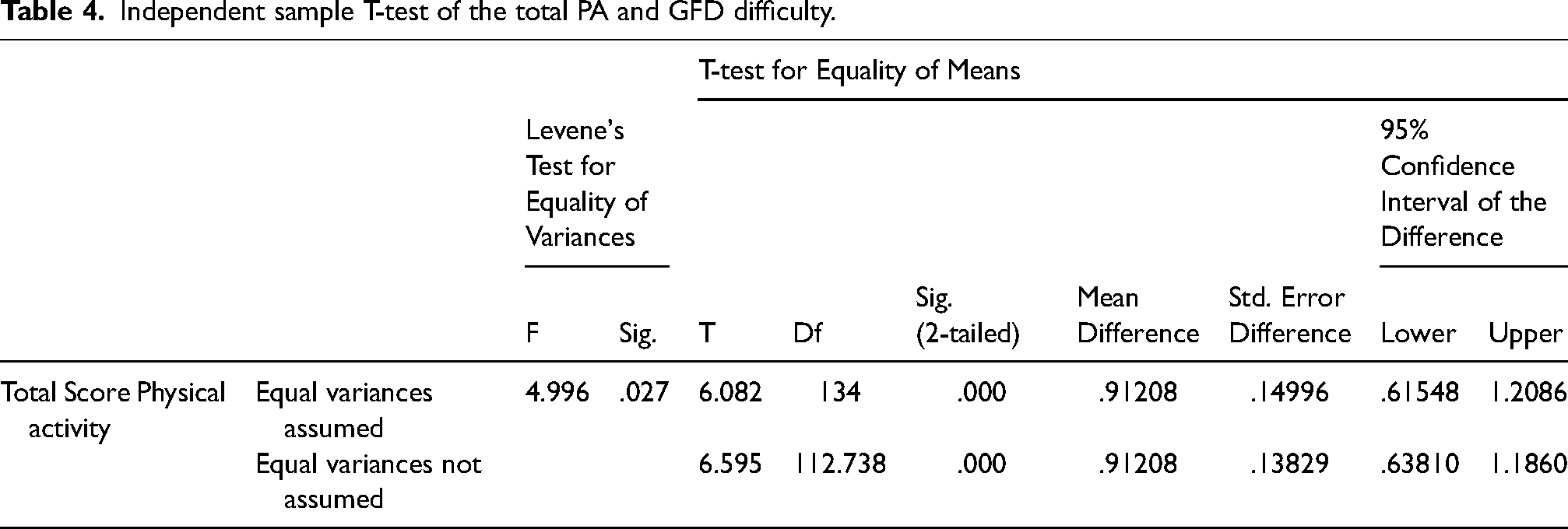
In addition to descriptive analysis, the one-sample T-test, the Kaiser-Meyer-Olkin (KMO) and Barlett's test, and the factorial analysis were conducted to assess the association between GFD and social QoL on one hand, and between GFD and PA on another hand. The T-test was applied to compare the means of a dependent quantitative variable (social QoL and PA) across the independent categorical variable (GFD) (Kim, 2015) (Tables 2 and 4). Moreover, the Kaiser-Meyer-Olkin (KMO) and Barlett's test was conducted on all the social QoL and PA questions to make sure that factorial analysis is applicable (> = 1.0; p-value <0.05). In addition, the factorial analysis was used to reduce the number of variables included in the social QoL and the PA section.
Independent sample T-test of the total social QoL and GFD difficulty.
Independent sample T-test of the total PA and GFD difficulty.
Ethical considerations
The following research study was approved by the Institutional Review Board (IRB) of the Holy Spirit University of Kaslik (USEK). Participants were informed about the purpose and goals of the study prior to data collection. To ensure confidentiality, only members of the research team had access to the data. Additionally, for anonymity purposes, any personal identifiers were replaced with codes, using SPSS software version 25 to encode the data.
Results
The following cross-sectional study aimed to investigate whether adherence to a GFD is associated with a higher social QoL and higher PA levels of CD Lebanese patients aged 18 to 59 years old.
Descriptive analysis
Sociodemographic Characteristics & Anthropometric Measures (BMI)
Analysis of socio-demographic characteristics were represented in Table 1. 78% of participants were females. Concerning age groups, 53% of celiac participants were aged between 25 and 39 years old, 28% were aged between 40 and 59 years old, and only 19% were aged between 18 and 24 years old. In terms of marital status, 55% were married, 41% were single, and 4% were divorced. Respondents were dispersed across all Lebanese districts, but the majority disclosed residing in Mount-Lebanon district (69%). Moreover, respondents were seen to be predominantly educated. Half of them have obtained a bachelor's degree (54%), 19% have a master's degree, 16% have a school degree, 9.5% had no schooling experience, and only 1.5% of participants had a PHD. Finally, socio-economic status was measured through monthly salaries. Results show that the majority of participants monthly income is between 800,000 L.L and 3,000,000 L.L: 35% had income between 800,000 L.L and 1,500,000 L.L, 32% between 1,500,000 L.L and 3,000,000 L.L, 20% less than 800,000 L.L and only 13% more than 3,000,000 L.L. The mean BMI was set at 22.67 kg/m2 (Table 1).
(b) CD data (Diagnosis, Symptoms, and Adherence to a GFD)
Demographic characteristics of Lebanese celiac disease (CD) participants.
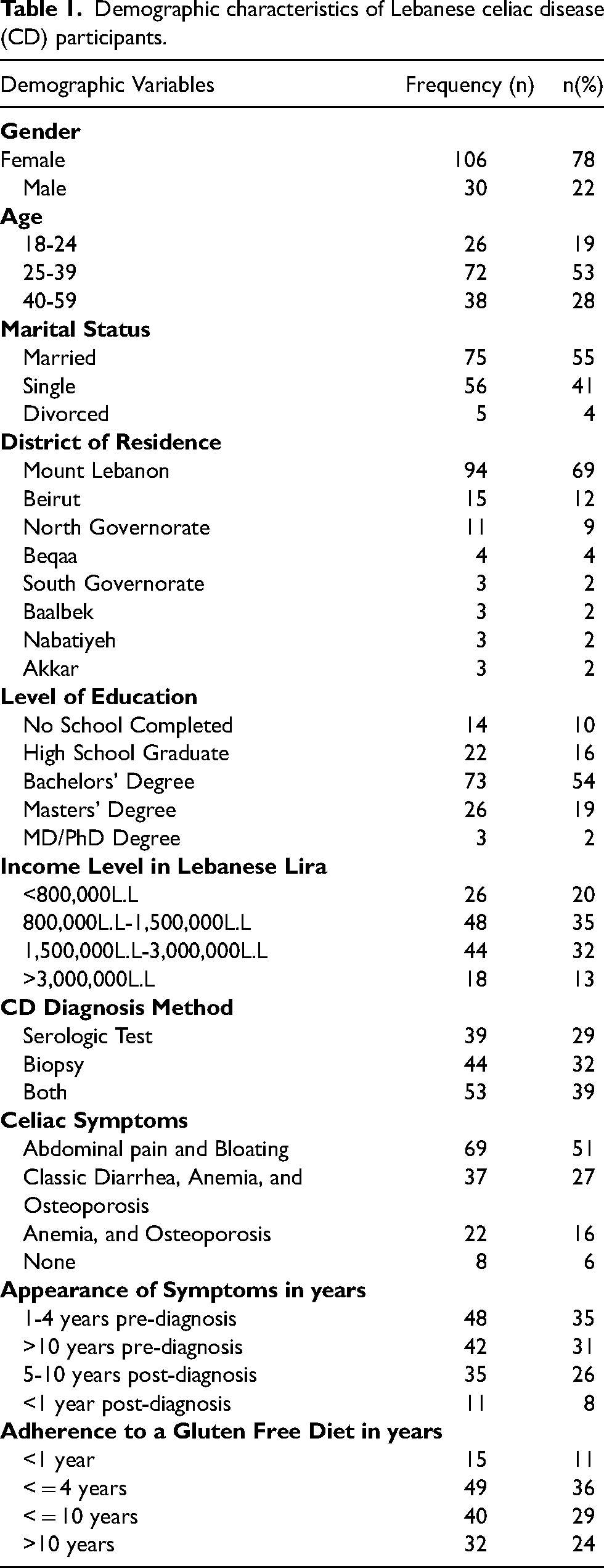
None of the participants suffered from any medical history (indigestion, malabsorption, or taking any medication that may affect their weight). In addition, out of 136 participants, 53 participants (39%) reported having conducted both serologic testing and biopsy proving that they suffer from CD, while 44 participants (32%) had only carried out biopsies proving their diagnosis and 39 (29%) participants had only done the serologic test Regarding CD point of diagnosis, 37% knew about their diagnosis from 1 to 4 years ago, 32% from 5 to 10 years ago, 23% from more than 10 years, and the rest (8%) knew from less than 1 year.
As for the symptoms of the disease, 51% of participants suffered from abdominal pain and bloating. In addition to the abdominal pain and bloating, 27% of those participants suffered from predominant classic diarrhea, anemia, and osteoporosis. Moreover, only 16% reported suffering from anemia, osteoporosis, and other symptoms and 6% do not exhibit any of those symptoms. All these symptoms were apparent before the celiac diagnosis. For 35% of participants, symptoms appeared 1 to 4 years before diagnosis, and 31% of those participants have been suffering from those symptoms for more than 10 years. Moreover, 26% suffered from celiac symptoms between 5 and 10 years, and only 8% suffered for less than 1 year from CD diagnosis.
All celiac disease patients disclosed following a GFD. The majority have been following this diet for more than a year, whereby 49 participants reported following a GFD for 4 years, 40 reported being on a GFD for 10 years, and 32 participants reported following this diet for more than a decade. Only 15 individuals reported being new followers of this type of diet, with adherence for less than a year. Symptoms disappeared for 117 participants (89%) after following the GFD, but only 15 participants (11%) are still suffering from celiac symptoms despite adherence to a GFD. 101 participants (74%) are encountering challenges in adhering to a GFD, while only 35 participants (26%) described the process as easy.
Analytical analysis
To reduce the number of variables used to measure each of the social QoL and PA, factorial analysis was carried out. The Kaiser-Meyer-Olkin (KMO) and Barlett's test were initially conducted on all the questions related to those variables, to make sure that factorial analysis is applicable. The results have shown a value of 0.87 > 0.5 which is considered acceptable and P-value = 0.0001 < 0.05 of KMO and Bartlett's test, respectively. Based on these results, factorial analysis was conducted. Two new variables, the total social QoL and the total PA, were created where all the information related to those two variables were combined to one final variable, in the purpose of studying their association with the GFD. The strongest factor loading is “the feeling of being socially stigmatized”, while the weakest factor loading is “the physical energy after GFD”. This finding implies that the social QoL factor affects more the GFD than the PA in our population of the study. To test the reliability of the scale used to measure each variable, Cronbach's alpha was calculated. Calculated Cronbach's alpha coefficients indicate that the measurement scales of the social QoL (0.948 > 0.70) and the PA (0.885 > 0.70) are highly consistent.
The eigenvalue represents the total amount of variance that can be explained by a given principal component. Since the goal of running a principal component analysis is to minimize our set of variables down, it would be useful to have a criterion for selecting the optimal number of components that are of course smaller than the total number of items. One criterion is to choose components that have eigenvalues greater than or equal to 1. Under the Total Variance Explained table (Appendix 3), we see that the first two components have an eigenvalue greater than 1. The total eigenvalue of the first retained component is equal to 5.82, and the total eigenvalue of the second retained component is equal to 4.31 (Appendix 3). The remaining components were not considered since the values of their respective eigenvalues are lower than 1. As shown in appendix 3, the total variance explained by the retained components is equal to 67.52%.
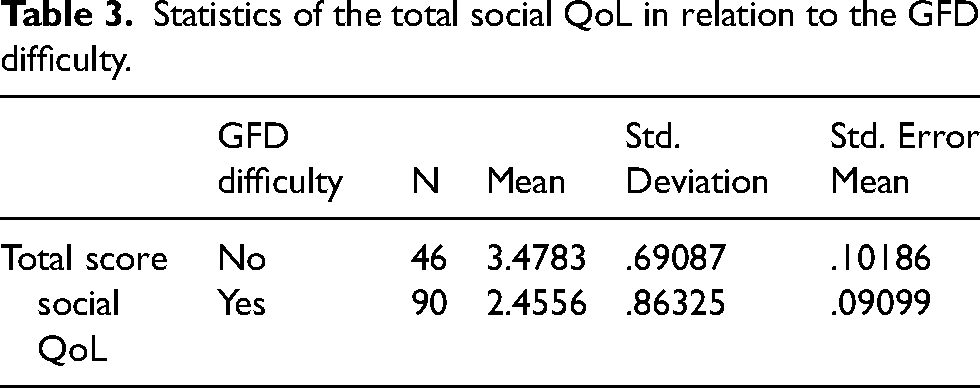
Based on the results, we can state that the average score of the sample is lower than the optimum score by 0.779, and that the 95% the confidence interval varies between −0.871 and −0.6878. Moreover, the descriptive statistics indicate that the mean of the sample is equal to 3.22 with a standard variation of 0.54011 showing low dispersion or variation among the respondents. In this context, we can conclude that the GFD did affect positively the PA of respondents since their score of 3.22 is equivalent to position 3 described as “Quite a bit” on the measuring scale. In addition to the validated hypothesis, an independent sample T-test was conducted to study the association between difficulty to adhere to a GFD d(independent variable) and the total social QoL and physical activity (dependent variables). A significant positive association between difficulty to adhere to a GFD and the total social QoL was observed (p-value>0.0001) (Table 3). Among the 136 respondents, 46 did not find difficulty in following a GFD, and stated a higher positive impact on their social QoL (average 3.4783 over 4). On the other hand, the 90 respondents who reported challenges in adherence to a GFD expressed a lower positive impact on their social indications (average 2.4556 over 4) (Table 5).
Statistics of the total social QoL in relation to the GFD difficulty.
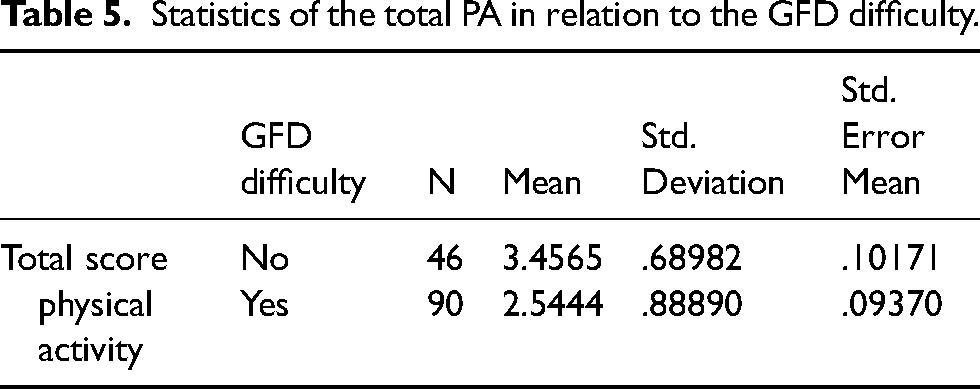
Statistics of the total PA in relation to the GFD difficulty.
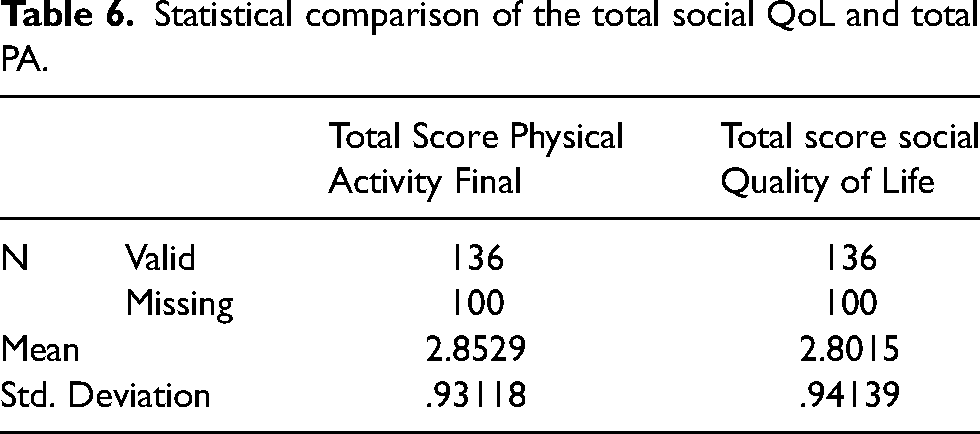
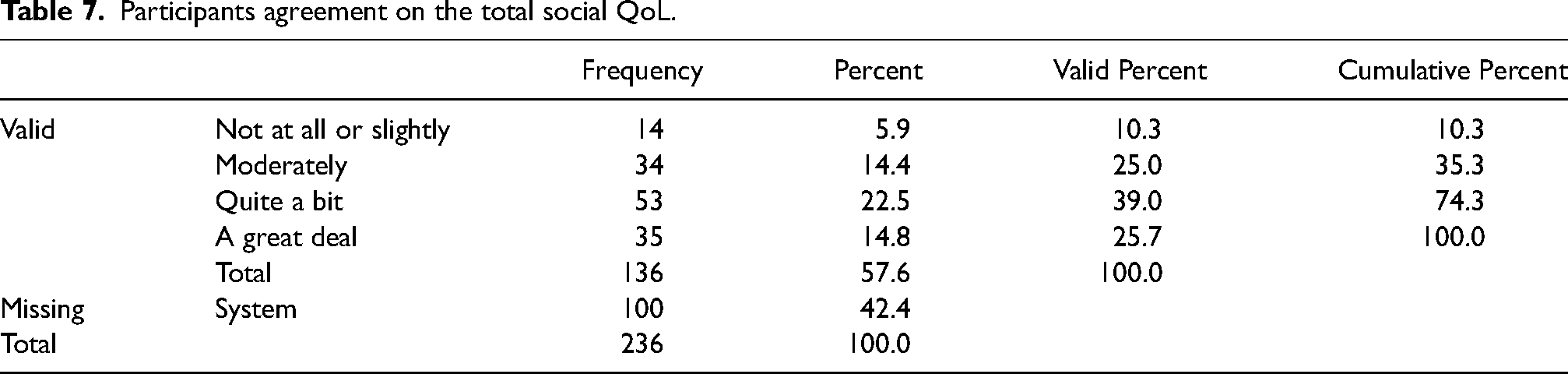
Moreover, the total social QoL score shows that most participants’ answers were positive (Table 6). 53 (39%) participants selected “Quite a bit” as an answer, while 35 (26%) participants answered with “A great deal”, 34 (25%) with “Moderately”, and the remaining participants (10%) with “Not at all” or “Slightly”, which further emphasizes the positive impact GFD adherence has on social QoL (Table 6). The total physical activity score also highlighted the positive impact that GFD has on PA since 58 (43%) participants answered by “Quite a bit”, 36 (26%) responded with “A great deal”, 28 (21%) selected “Moderately”, and the remaining participants (10%) selected the option “Not at all” or “Slightly” (Table 7).
Statistical comparison of the total social QoL and total PA.
Participants agreement on the total social QoL.
Discussion
The main aim of this cross-sectional study was to test the association between adherence to a GFD and each of the social QoL and PA of adult CD patients in Lebanon. Our results highlight significant associations between the variables of interest.
GFD adherence was positive for all participants which is normal since it is the only treatment for celiac patients to date. This result shows that all celiac patients are aware of celiac treatment since the majority are following the recommended current treatment for CD which is adherence to a GFD (Progress et al., 2007; Caio et al., 2019; Serena et al., 2020). However, difficulty in maintaining a GFD was also relevant in our sample. The difficulty of following a GFD was not correlated with the duration of being on a non-gluten diet, since many factors affected this diet directly and indirectly such as the availability of those products in the shops since a big part of the non-gluten products is out of stock, in addition to their expensive prices that cannot be afforded by all population groups in Lebanon amidst a historical economic crisis.
The results regarding the social QoL in association with a GFD have shown that there is a significant association between these two variables, (p-value = 0.0001) and thus demonstrating that GFD positively affects the social QoL. A study conducted by Zingone et al. (2015) shows that even after 10 years of diagnosis with CD, women were worried about the impact of CD on their social life and revealed a sense of loneliness specifically while they are socializing with others. Moreover, this study shows that a GFD is correlated to dietary restrictions and compromised daily social relationships, in addition to the ongoing concerns of celiac patients about coping with GFD specifically in social interaction and when going out (Zingone et al., 2015). Furthermore, a study conducted by Zarkadas et al. (2013) emphasized that most members of the Canadian Celiac Association avoid going to restaurants due to the limited options they can have on the menu, which affect their social life. A positive association was also seen between GFD difficulty and the social QoL (p-value = 0.0001). The mean value of the celiac patients who did not find difficulty following a GFD was higher than the mean of those facing difficulties with this type of diet (3.48 vs. 2.45). Additionally, a systematic review conducted by Möller et al. (2021) involving 3372 participants, shows that across all the studies, symptoms of anxiety and depression were the most examined psychosocial factors in celiac patients following a GFD. Adherence to GFD has been also reported to be associated with social isolation (Serena et al., 2020). Finally, several reports have described the difficulties of living with CD in adults, as regards to the impact of this condition on physical, social, and emotional factors (Zingone et al., 2015).
Regarding the PA levels, a significant association as well appeared with GFD (P-value = 0.0001) demonstrating that GFD affects positively the PA. In addition, participants mentioned that while following a strict GFD their PA is better than while ingesting gluten products or at the time of any case of gluten cross-contamination. Results regarding the association between GFD difficulty and the PA indicate a significant positive association between these two variables (p-value = 0.0001). The mean value of the patients who did not find difficulty following a GFD was more than the mean of celiac patients facing difficulties with this type of diet (3.46 vs. 2.54). Alavinejad et al. (2021) showed a significant improvement in the average score of the PA that was 0.88 before following a GFD and increased to 3.6 after the adherence to a GFD (P-value = 0.003). Another study revealed that the mean PA increased after following a GFD from 37.03 to 50.30 which shows that GFD can improve the PA and explain that there is a positive correlation between GFD and the PA (Deepak et al., 2018). Moreover, reviewed articles show that fatigue, a considerable complaint in CD patients, is significantly greater in comparison to healthy control subjects (mean 36.3 vs. 16.7, median 35 vs. 15) (Skjellerudsveen et al., 2019). A study conducted by Dowd et al. (2019) shows that celiac females are not very physically active with more than half of them (50%) engaging in only low levels of PA based on the International Physical Activity Questionnaire. These two studies highlight those celiac patients who have high risks of fatigue which can decrease their PA. The fatigue visual analog scale decreased after following a GFD (mean 66 vs. mean 51), which further stresses that non-gluten intake can reduce fatigue in celiac patients (Skjellerudsveen et al., 2019). However, the existing literature is characterized by significant methodological weaknesses. Hence, there is an unmet need to understand contributing factors for fatigue as well as the effect of fatigue in CD (Skjellerudsveen et al., 2019).
When looking at sociodemographic characteristics, participants in our study (n = 136) included 106 females (78%) and 30 males (22%), which shows an existing gender disparity in CD diagnosis in our sample, and potentially in Lebanon. Previous research studies have highlighted that CD occurs predominantly in women (Jansson-Knodell et al., 2018; Shah & Leffler, 2010). A study conducted by Shah & Leffler (2010) shows that in most populations, females represent 60–70% of individuals with diagnosed CD. Another study focusing on the gender-based differences in non-referral populations with CD stressed that 65% of the CD population were females, with a female to male ratio equal to 1.85:1 (Jansson-Knodell et al., 2018). However, our relative sample size is small and short in males, which renders it a possible limitation in our study. Thus, the assumption of having a gender disparity in CD diagnosis in the country should be further assessed with a relative larger sample size with a higher proportion of males to females.
With respect to age, the number of young participants is greater than the remaining age ranges (53% of celiac patients aged between 25 to 39 years old in comparison to 28% aged between 40 to 59 years old and 19% aged between 18 to 24 years old). One possible explanation for this result might be due to the younger population that is more open to understanding the disease and its effect on their lifestyle and are more willing to try to find new solutions that facilitate their life (Jansson-Knodell et al., 2018; Shah & Leffler, 2010;). Excluded participants who were not eligible yet interested to participate in the study were also classified as a relatively young age group (18–35 years old). Additionally, the main focus on social media for recruitment might have influenced the age range represented in our sample (Haas et al., 2017). The reason for focusing on social media predominantly for recruitment was the peak in COVID-19 in Lebanon at the time of participant recruitment for the study (Haas et al., 2017). Age plays a main role in the way that a CD patient manages to live with the disease (Jansson-Knodell et al., 2018). During this study, the young participants were very motivated and curious to know more about the results of the study since following a lifelong GFD is a part of their routine. Besides their answers to our questions, the young participants are quite knowledgeable about the different options of gluten-free food and have done much research about CD in general. Moreover, most of those participants have a bachelor's degree (54%) which facilitates their understanding of the disease, the importance of its treatment, and the adherence to a GFD.
The personal income of the majority (35%) was between 800,000 L.L and 1,500,000 L.L. Such a monthly income places most of our participants in the low-income category based on Lebanon's minimum wage (Al-Sunaid et al., 2021) and affects in a way the adherence to gluten-free products (GFP) since they are normally more expensive than other products. Besides the difficulty of managing CD, the current situation in Lebanon affects the CD patients as well. The respondents were not just worried about their disease, but they were stressed about how to afford adequate GF food. This result is convergent with Stevens and Rashid’s (2008) study who did a cost comparison analysis between gluten-containing products and GFP. The study shows that all the available commercial products labeled GF were significantly more expensive than comparable products (Stevens & Rashid, 2008). The mean unit price for GFP was $1.71 in comparison with $0.61 for regular products (P-value < 0.0001) (Stevens & Rashid, 2008). GFP was more expensive than regular products (Stevens & Rashid, 2008). Another study conducted by Al-Sunaid et al. (2021) highlighted the difficulty of following a GFD due to its limited availability (79%) and expensive prices (90%).
Limitations
Nevertheless, this research study suffers from limitations that should not be disregarded, mainly due to its reliance on self-reported data. Moreover, the small sample size may be attributed to the lack of motivation among Lebanese CD individuals who were impacted by the COVID-19 pandemic. Challenges in recruiting a larger sample were mainly a direct cause the absence of a CD public association in Lebanon. Additionally, no annua census, database, or any publications related to CD are available in Lebanon at the Ministry of Public Health. Furthermore, recall bias might have occurred since some questions required participants to remember some information such as their PA levels.
Conclusion
This research study is the first to address associations between adherence to a GFD and each of the social QoL and PA of Lebanese CD patients. It aims to add value to the literature by surveying the Lebanese population and, correspondingly, guiding future experimental research. Future research could focus on the association between GFD and other types of quality of life. In addition, follow-up studies should be implemented to address existing barriers and associated underlying barriers exacerbating adherence to a GFD in Lebanon. Further awareness-raising and learning activities about gluten-free products are needed to improve the adherence to a strict GFD and to facilitate the availability of gluten-free products to the Lebanese population. This could help us in building more scientific data about celiac disease in Lebanon.
Supplemental Material
sj-docx-1-nah-10.1177_02601060221095685 - Supplemental material for Assessment of the social quality of life and the physical activity of adult celiac disease patients following a gluten-free diet in Lebanon
Supplemental material, sj-docx-1-nah-10.1177_02601060221095685 for Assessment of the social quality of life and the physical activity of adult celiac disease patients following a gluten-free diet in Lebanon by Priscilla Bouery, Randa Attieh, Lea Sacca and Yonna Sacre in Nutrition and Health
Footnotes
Acknowledgements
N/A
Availability of data and material
The data that support the findings of this study are available from the corresponding author upon reasonable request
Research ethics and patient consent
The following medical research involving human subjects was conducted according to the World Medical Association Declaration of Helsinki.
Consent for publication
The Institutional Review Board at the Holy Spirit University of USEK has approved this study for publication.
Authors’ contributions
PB has contributed substantially to the conception and design of the study, as well as the acquisition, analysis, and interpretation of data for the study. RA has contributed to the design of the work and interpretation of the data. PB, RA, and LS have contributed to drafting the study. RA, LS, and YS have contributed to critically revising the study for important intellectual content. All authors provided final approval of version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
The institutional review board at Holy Spirit University of Kaslik (USEK) in Lebanon approved all research protocols, and participants provided written informed consent.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.