
Abstract
Introduction
Hypertension is the leading cause of cardiovascular and cerebrovascular disease (World Health Organization, 2013). Raised blood pressure (BP) (systolic BP ≥140mmHg or diastolic BP ≥90mmHg) prevalence among people ages ≥18 years has been declining in high-income countries (from 35.2% in 1975 to 22.6% in 2015), but it has been rising or stagnated in low- and middle-income countries (LMICs) (from 19.6%–23.2% in 1975 to 22.5%–21.7% in 2015) (World Health Organization, 2013, n.d.). According to the Indonesian national health survey 2018, raised BP prevalence among people ages ≥18 was 34.1% (Kementerian Kesehatan Republik Indonesia [Indonesian Ministry of Health], 2019). As in other countries, in Indonesia adults ages >40 years experience higher prevalence (Kementerian Kesehatan Republik Indonesia [Indonesian Ministry of Health] & Politeknik Kesehatan Palembang Prodi Keperawatan Lubuklinggau [Palembang Health Polytechnic Lubuklinggau Nursing Program], 2012).
Systematic reviews and meta-analyses of randomized controlled trials have consistently shown that reducing dietary salt is an important way to reduce hypertension (Graudal et al., 2011; He et al., 2013; Peng et al., 2014). Globally, it is estimated that the average consumption of salt is 9–12 grams per day, which is substantially higher than the recommended intake of 5 grams per day (World Health Organization, 2013). Indonesians tend to consume large amounts of salt, estimated to be on average about 15 grams per day (Kementerian Kesehatan Republik Indonesia [Indonesian Ministry of Health], 2009). The Indonesian national basic health survey 2013 found that 77.3% of the population (ages ≥10 years) add salty seasoning to their food (Kementerian Kesehatan Republik Indonesia [Indonesian Ministry of Health], 2013). Based on the World Health Organization's salt reduction strategies (World Health Organization, 2016a), the Indonesian Ministry of Health launched a plan to collect population-based data on knowledge, attitudes and behaviours related to salt intake in order to better develop national salt reduction strategies (George Institute for Global Health, n.d.). Thus, it is imperative to find the keys to limiting Indonesians' salt intake to help reduce their risk of developing hypertension.
Self-reported salt consumption is associated with actual salt intake (Lee et al., 2014). Thus, one important aspect of reducing dietary salt intake is to identify individual perceptions about salt reduction practices and their predictors. Predictors identified reported in other studies include beliefs about the negative health effects of salt (Zhang et al., 2016), thoughts related to different stages of behavior change (Ahn et al., 2017), and sense of self-efficacy (Irwan et al., 2016). However, dietary salt intake is typically a deeply embedded habit in people's cultural patterns of food consumption in everyday life (Crowe et al., 2017). A systematic review pointed out the effectiveness of community-level salt reduction programs and the necessity of conducting more robust evaluation studies (Christoforou et al., 2016). Thus, to promote lasting behavioral change, it is necessary to identify the predictors of salt reduction practices within the context of society and culture.
To date, relatively few studies have been conducted in LMICs to identify the correlates of salt reduction practices (Santos et al., 2017; Trieu et al., 2015). Interventions known to be effective in high-income countries are often not feasible or appropriate for implementation in LMICs (Trieu et al., 2016). A study in South Africa found the gaps in people's awareness and recommendations about salt reduction, and identified the need to provide content-specific educational interventions (Mushoriwa et al., 2017). Identifying salt reduction practices and their predictors among people with hypertension in rural Indonesia is an important initial step towards the development of effective community-level strategies for supporting changes in salt intake habits.
The aims of this study were: 1) to describe whether middle-aged adults with hypertension in rural Indonesia had ever attempted to reduce their salt intake in eating or cooking, and 2) to identify correlates of their salt reduction practices in order to better develop a community-level salt reduction strategy.
Methods
Theoretical framework and study design
We developed a theoretical framework (Figure 1) based on a preliminary study (Mizutani et al., 2016). This framework assumed that salt reduction practices would be enhanced by prior experience, social support, and health professional support, and that practices would be hindered by various personal factors (e.g., negative emotions about healthy eating), social factors (e.g., limited social support), and environmental barriers (e.g., unavailability of low-sodium foods at local stores). We used this framework to better understand participants' health practices because for middle-aged Muslims with hypertension in rural Indonesia health practices were based on their cultural and religious beliefs (Mizutani et al., 2016). To test this framework, we designed a cross-sectional survey.
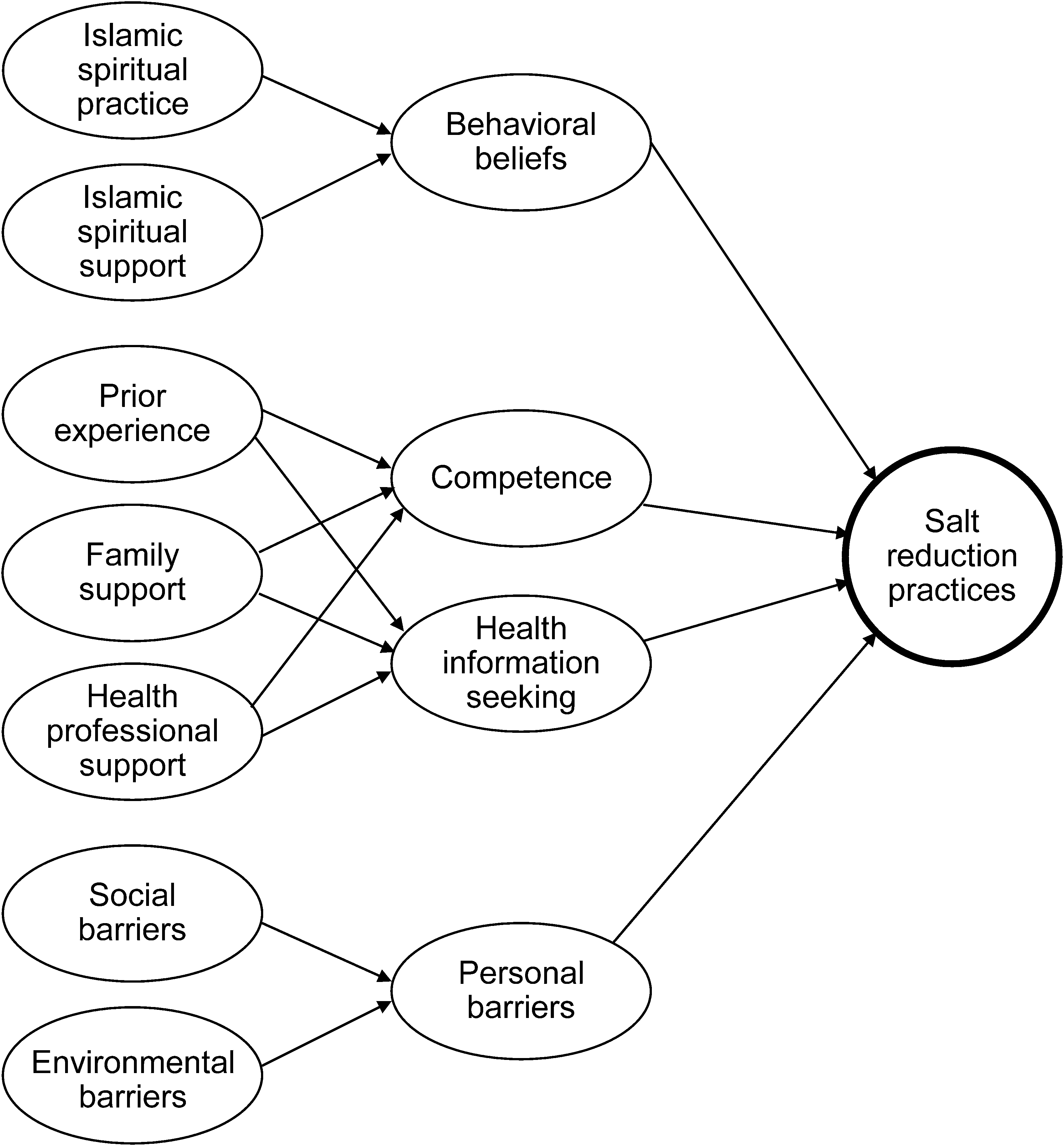
Theoretical framework: salt reduction practices and their predictors among middle-aged Muslims with hypertension in rural Indonesia.
Setting and participants
Indonesia has the fourth largest population in the world with a population of over 268 million, 56.6% of whom live on Java island (Kementerian Kesehatan Republik Indonesia [Indonesian Ministry of Health], 2020). West Java province is an important region because of its large population and higher hypertension prevalence compared to the national average (39.6% vs. 34.1%) (Kementerian Kesehatan Republik Indonesia [Indonesian Ministry of Health], 2019, 2020). In a rural district in West Java, we recruited potential participants from four puskesmas (community health centers). We used purposeful stratified random sampling to select four community health centers from a list of 49 in the district. We divided the 49 community health centers into four strata based on the population density of the sub-districts (high: ≥1000 people/km2 or low: <1000 people/km2) and location (i.e. coastal or inland). Then, we selected three community health centersfrom each stratum using simple random sampling. We selected one from the stratum through purposive sampling to ensure that the area would be safe for research assistants. Once we identified the four community health nurses in each center's staff introduced our research team to eligible participants who met the following inclusion criteria: ages 40–64 years, diagnosed with hypertension, Muslim, able to communicate, not pregnant, and willing to participate. Diagnostic criteria for hypertension were based on the Indonesian Ministry of Health guidelines: systolic BP 140 mmHg and above and/or diastolic BP 90 mmHg and above (Menteri Kesehatan Republik Indonesia [Indonesian Minister of Health], 2014).
In structural equation modeling, it is standard practice to conduct an analysis with a sample-to-parameter ratio ranging from 5:1 to 10:1 (Kline, 2011). We chose 8:1 as a realistic ratio. Our instrument contained 53 items, thus requiring a sample size of 424. To estimate the response rate, we used as a reference a national health survey that achieved a response rate of 95.9% for women (Badan Pusat Statistik [Statistics Indonesia] et al., 2013). Assuming a similar response rate, we calculated a minimum sample size of 435. To ensure that we would have ample data, we recruited 450 participants.
Study instruments
We developed a written questionnaire in Bahasa Indonesia language based on the study framework. The questionnaire measured participants’ socio-demographic characteristics, perceived salt reduction practices, and potential correlates. The participants’ stages of hypertension were classified based on the Indonesian Heart Association's Guidelines, which are similar to other international guidelines (Dubey et al., 2019; Perhimpunan Dokter Spesialis Kardiovaskular Indonesia [Association of Indonesian Cardiovascular Specialist Doctors], 2015).
Perceived salt reduction practices were measured using two items rated on a four-point Likert-type response format from 1 (never), 2 (often), 3 (sometimes), to 4 (routinely). Potential correlates of salt reduction practices were measured using 51 items dispersed among 11 subscales, rated with either a four-point Likert scale (1 = never to 4 = routinely) or a five-point Likert scale (1 = strongly disagree to 5 = strongly agree).
To ensure content validity of the questionnaire items on salt reduction practices and their correlates, we distributed a draft self-administered questionnaire assessment form to six experts (three faculty members in Indonesia and three nurses from the community health centers). In the assessment form, we asked the experts to rate each item's clarity and rate the relevance of each item to its related concept using a four-point Likert scale, with responses ranging from 1 (not relevant) to 4 (highly relevant). We asked faculty members to assess the clarity and relevancy from a theoretical perspective and nurses to assess them from a cultural perspective. The item-level content validity index (I-CVI) was calculated by counting the number of “3” or “4” ratings on the four-point relevance scale for each item, and then dividing this by the number of raters. An I-CVI of 0.78 or higher is recommended (Polit and Beck, 2017). Items with lower-than-desired I-CVIs were either revised or omitted after discussion among our research team.
Data collection
We decided to collect data by having research assistants ask participants face-to-face each questionnaire item and then having the research assistants record participants' answers on the questionnaires because of participants' somewhat low levels of formal education (Mizutani et al., 2016). Research assistants collected all data in September 2014 at a participants' preferred locations, typically at their homes. Research assistants were nursing students or public health students in a bachelor's degree program in the district. Prior to entering the field, the researchers trained the research assistants for two days on the study aims, methods, ethical considerations, and personal safety. During recruitment of participants, we informed potential participants about the study aims, methods, their voluntary participation and confidentiality.
Data analysis
We analyzed questionnaire data using SPSS Statistics and SPSS Amos (version 23; IBM Corp, Armonk, NY, USA). We calculated descriptive statistics for each variable. Consistent with previous studies (Nakayama et al., 2015; Osborne et al., 2013), we used one-factor confirmatory factor analysis to confirm the unidimensionality of each subscale of salt reduction practices and their correlates. SPSS Amos provided fit statistics for each factor. Acceptable model fit indices were as follows: goodness-of-fit index (GFI) >0.90, comparative fit index (CFI) >0.90, and root mean square error of approximation (RMSEA) <0.08 (Hair et al., 2010). Our research team named each factor to ensure cultural relevancy as well as to integrate the factors suitably within the study framework. To assess the internal consistency reliability of each factor, we used Cronbach's alpha with a value ≥0.70 set as desirable (Hair et al., 2010). We used independent t-tests and one-way analysis of variance (ANOVAs) to compare groups’ mean scores for salt reduction practices and their correlates. Then, we conducted structural equation modeling to identify potential direct and indirect relationships among observed and latent variables based on our study framework. Model fit was assessed using the GFI, CFI, and RMSEA. The RMSEA value was of particular importance because the developed model had a large number of degrees of freedom. GFI decreases when the degrees of freedom are large, while the RMSEA can express the model fit per degree of freedom (Toyoda, 2002). An RMSEA of ≤0.05 is generally considered indicative of a good fit for the data (Hair et al., 2010). P-values of less than 0.05 were considered to indicate statistical significance. Of the 450 participants surveyed, three had >10% missing data and were excluded from analysis (Hair et al., 2010). For the remaining 447 participants, 3.8% of variables had missing data. All missing values were imputed with the average item score for that variable.
Results
Participants’ characteristics
Of the 450 people contacted, all agreed to participate in the study. Among the 447 participants, the mean age was 54.1 years (SD = 7.2 years) and the majority (77.2%) were female (Table 1). Nearly two-thirds of the participants had not completed primary school and the majority worked in traditional occupations. Nearly three-quarters earned very limited income.
Participant characteristics (n = 447).
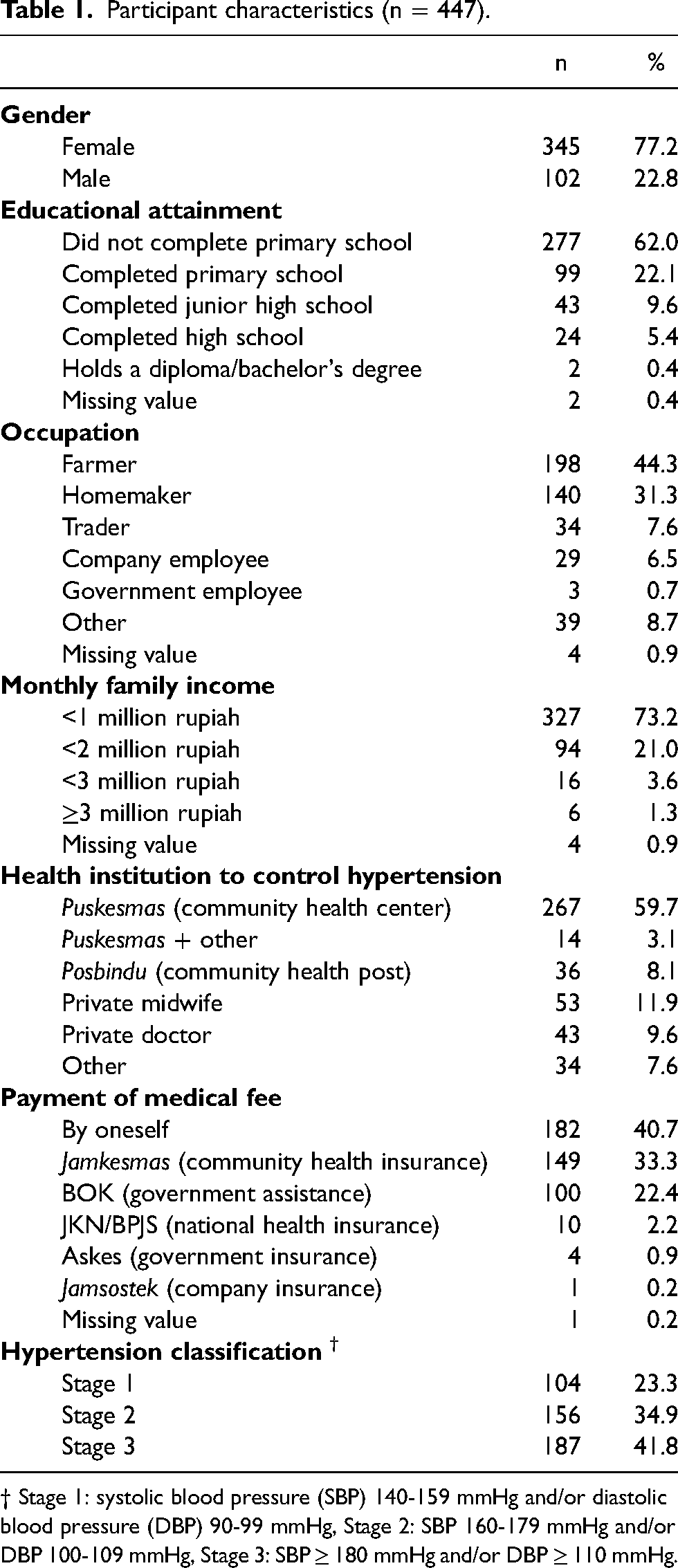
† Stage 1: systolic blood pressure (SBP) 140-159 mmHg and/or diastolic blood pressure (DBP) 90-99 mmHg, Stage 2: SBP 160-179 mmHg and/or DBP 100-109 mmHg, Stage 3: SBP ≥ 180 mmHg and/or DBP ≥ 110 mmHg.
Mean systolic BP was 169.3 mmHg (SD = 19.5 mmHg) and mean diastolic BP was 92.2 mmHg (SD = 10.7 mmHg). Many participants had elevated hypertension: Stage 3 (41.8%) and Stage 2 (34.9%). Nearly three-quarters of the participants obtained services to control their hypertension at their local community health center or posbindu (community health post).
Perceived salt reduction practices and their correlates
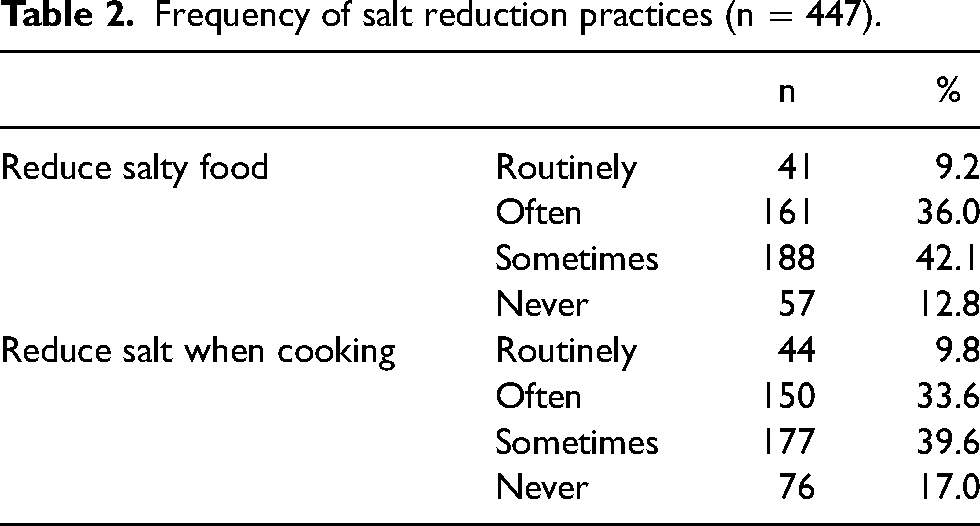
When asked for self-reports about personal management of salt intake (Table 2), 45.2% said that they had routinely or often reduced eating salty foods. Just 12.8% said they had never attempted to reduced eating salty foods and 42.1% reported doing so sometimes. Similarly, 43.4% reported that they had routinely or often reduced the amount of salt they used in cooking, while 17.0% said they had never done so and 39.6% said they had done so sometimes.
Frequency of salt reduction practices (n = 447).
In our confirmative factor analysis examining the reliability of questionnaire items (Table 3), we found that for all of the 12 factors generated, the GFI and CFI were within the acceptable cut-off limits. Based on an RMSEA >0.08, the model fit for eight factors was acceptable. The RMSEA tends to show better fit when the degrees of freedom are large, and thus it would, conversely, show worse fit when the degrees of freedom are small. As the other two indices were acceptable, we believed that all models showed an acceptable level of fit, thus confirming the unidimensionality of each factor. For each of the 12 factors, the Cronbach's alpha was ≥0.70, and ranged from 0.70 to 0.88. Thus, the reliability of the questionnaire was confirmed.
One-factor confirmatory factor analysis of questions about hypertension, factors and variables.
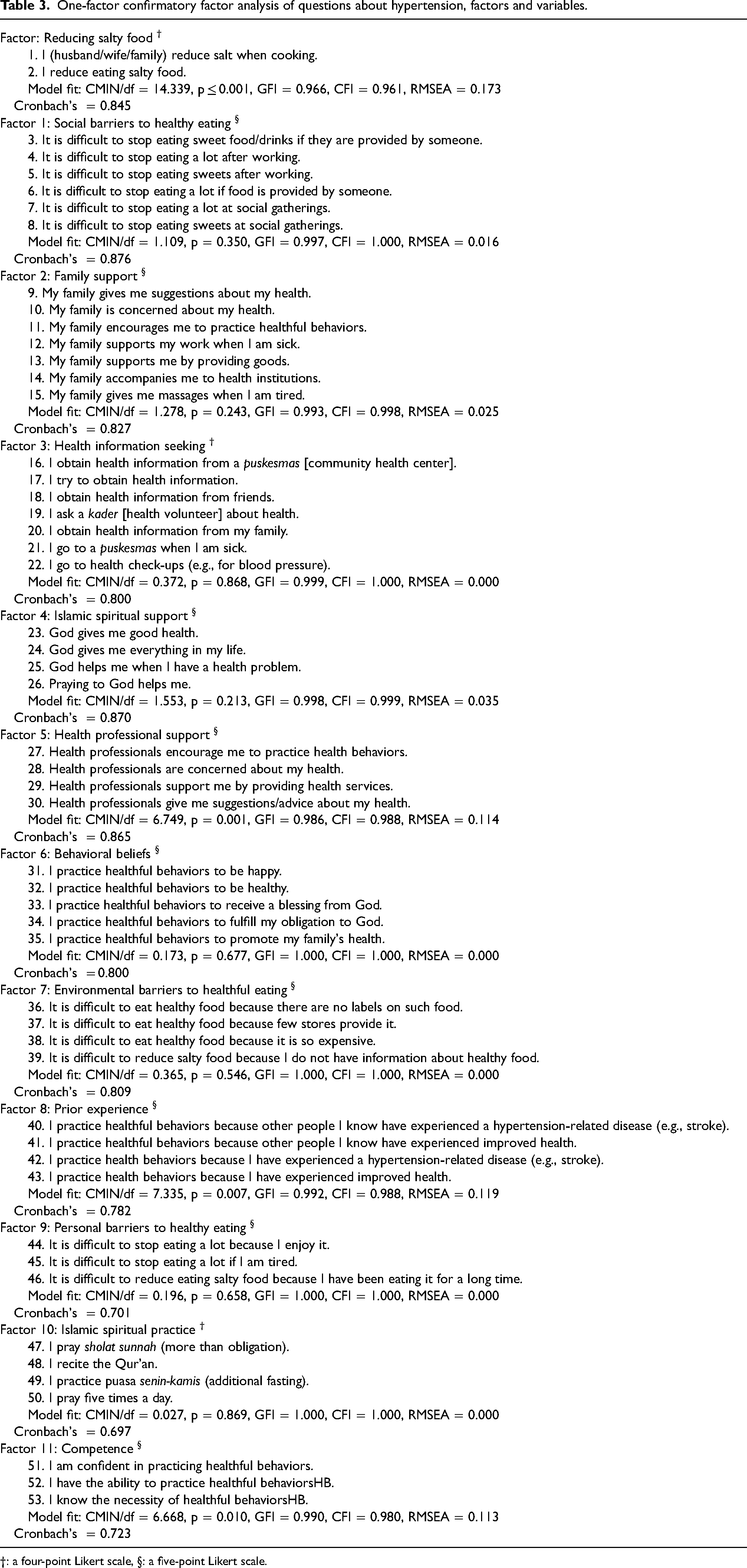
†: a four-point Likert scale, §: a five-point Likert scale.
Our analysis (Table 4) using independent t-tests revealed no differences between men and women in self-reported salt reduction practices (mean 2.3 and 2.4, SD 0.7 and 0.8, respectively). Of the 11 correlates of salt reduction practices, the means of 7 were virtually identical (means 2.3–4.2, SDs 0.4–0.8). Men reported significantly more difficulty when facing social barriers to eating a low-sodium diet than women. Women reported receiving slightly more family support and Islamic spiritual support than men. Our analysis using one-way ANOVA revealed some differences between men and women especially by education. Compared to participants who had not completed primary school education, significantly more participants who had completed a high school education reported frequently engaging in Islamic spiritual practices and seeking health information.
Mean scores of salt reduction practices, factors and tests of differences.
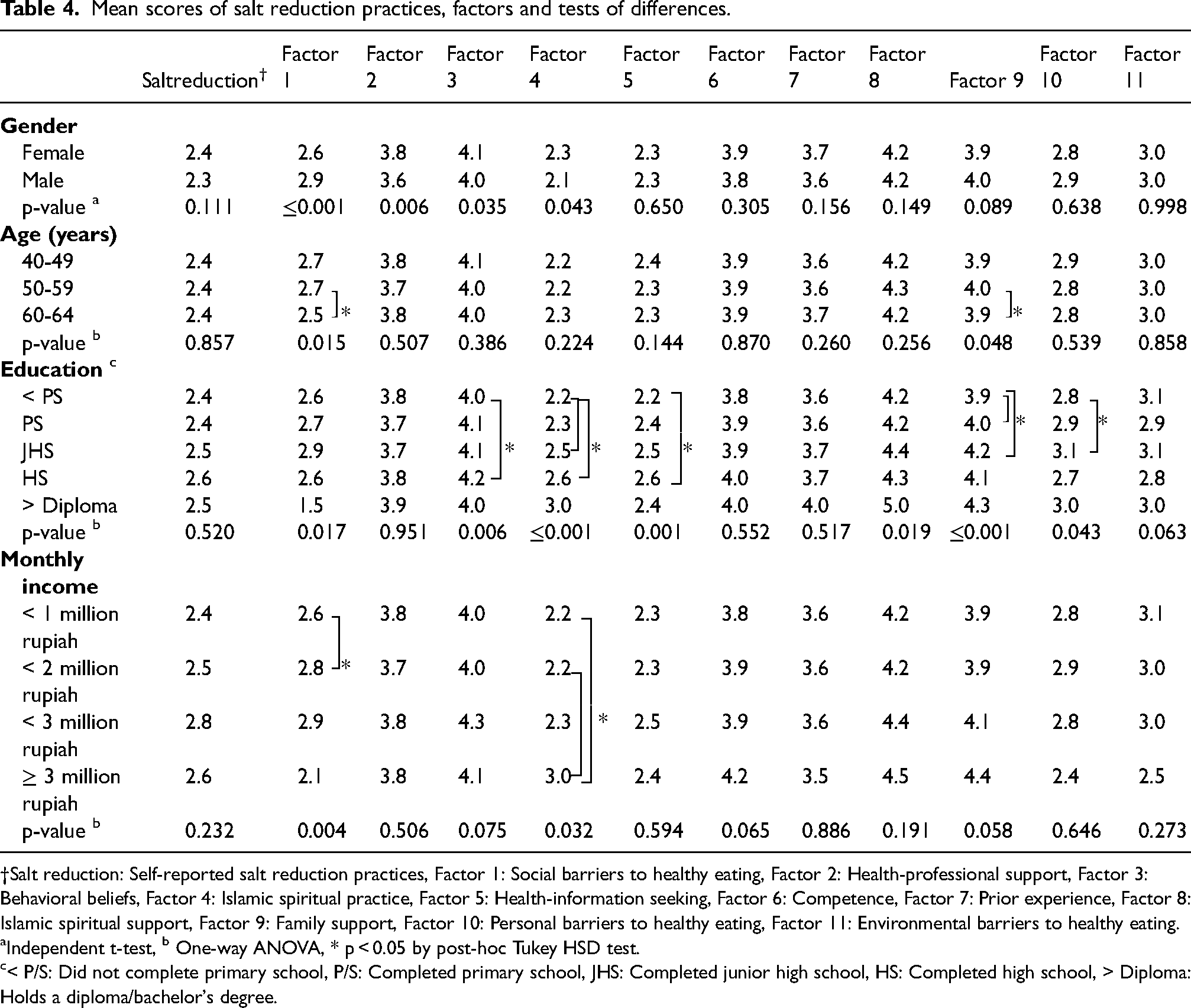
†Salt reduction: Self-reported salt reduction practices, Factor 1: Social barriers to healthy eating, Factor 2: Health-professional support, Factor 3: Behavioral beliefs, Factor 4: Islamic spiritual practice, Factor 5: Health-information seeking, Factor 6: Competence, Factor 7: Prior experience, Factor 8: Islamic spiritual support, Factor 9: Family support, Factor 10: Personal barriers to healthy eating, Factor 11: Environmental barriers to healthy eating.
Independent t-test, b One-way ANOVA, * p < 0.05 by post-hoc Tukey HSD test.
< P/S: Did not complete primary school, P/S: Completed primary school, JHS: Completed junior high school, HS: Completed high school, > Diploma: Holds a diploma/bachelor's degree.
Relationships between salt reduction practices and their correlates
To identify correlates of self-reported frequency of effort to reduce salt intake, we entered the latent variables into several structural equation models based on the study's theoretical framework. We modified the models using the modification index. The model presented in Figure 2 produced the best overall model fit (GFI = 0.904, CFI = 0.930, RMSEA = 0.047). All path coefficients were statistically significant at p < 0.05. Following the principle of parsimony, we excluded factors in the theoretical framework that reduced the model's fit.
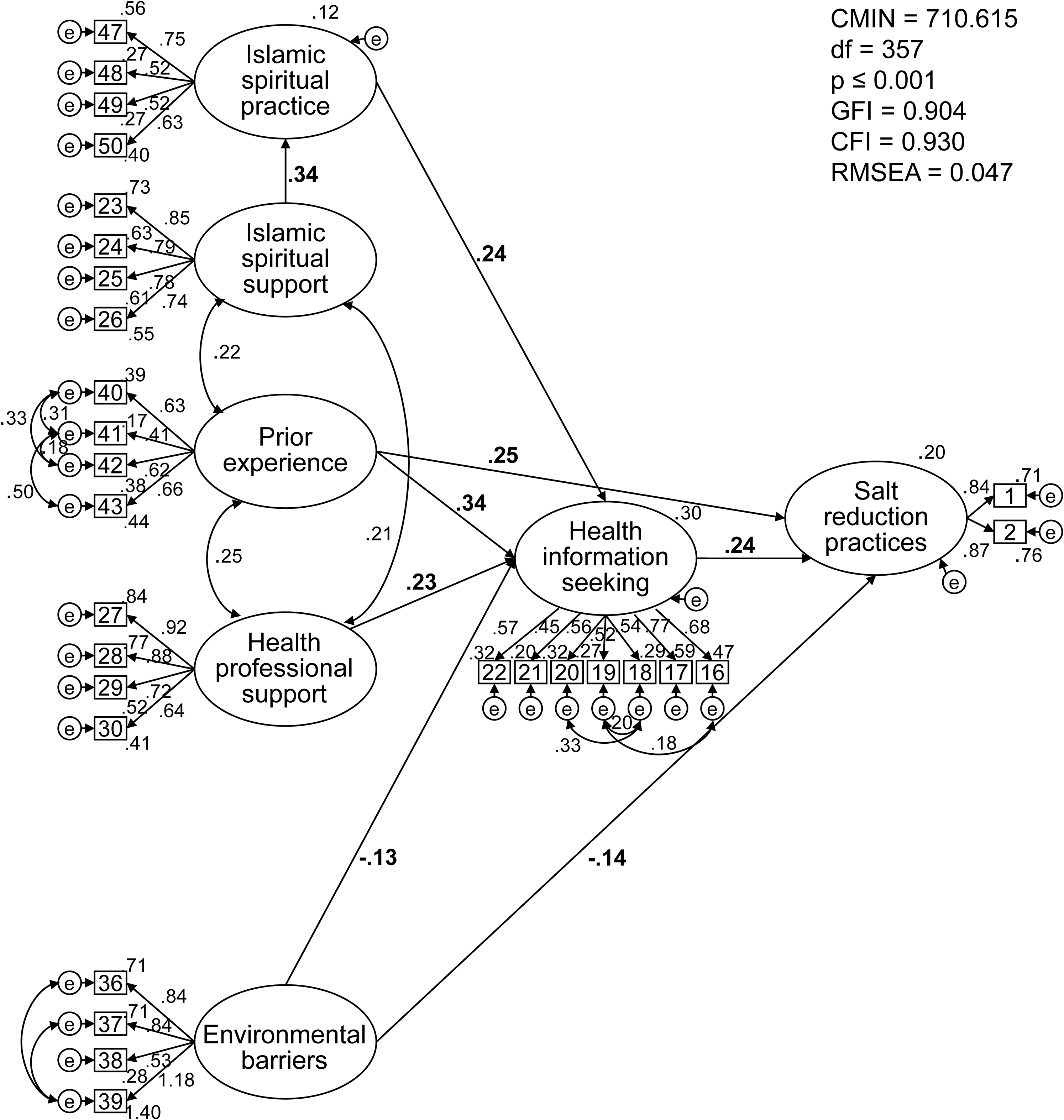
Structural equation model of salt reduction practices and their correlates among middle-aged Muslims with hypertension in rural Indonesia.
The results of our causal path analysis suggest that the participants’ self-reported frequency of effort to reduce their salt intake was most directly and positively associated with how strongly they had sought out health information (β = 0.24) and their prior health/illness experiences such as experiencing a hypertension-related disease and/or improved health (β = 0.25), and somewhat negatively associated with environmental barriers (β = -0.14). The model revealed that seeking health information was in turn correlated directly and positively with three exogenous variables: practice of Islamic rituals in their daily life (β = 0.24), prior health experiences (β = 0.34) and prior support received from health professionals (β = 0.23), and slightly negatively correlated with environmental barriers (β = -0.13). The factor loading showed that health professionals' encouragement and concern were particularly important elements of professional support. The strongest negative element of environmental barriers was the difficulty participants faced in trying to obtain information about healthy foods.
Discussion
This study reveals that about three quarters of our sample of middle-aged Muslims in rural Indonesia had substantially elevated Stage 2 or Stage 3 hypertension, which is much higher than previous study targeted adults ≥ 40 years (Hussain et al., 2016). There might be possible untreated or undiagnosed hypertension adults in rural Indonesia. Surprisingly, nearly all of the participants reported making at least some effort to reduce their intake of salt, although less than half reported doing so regularly. This finding suggests that most of the participants were at least somewhat aware of the negative health effects of salt in their diet, and they had attempted to make some efforts to change their habits and reduce their health risks from salt consumption.
Overall, this study shows that self-reported frequency of effort to reduce salt intake was associated with a constellation of six correlates, nearly all of which contributed positively or negatively at similar levels to frequency of effort to reduce salt intake. Our model did not identify a single “magic pill” that overwhelmingly influenced salt intake practices. Thus, the results show that the overall context is important.
In this study, the participants’ sense of importance of seeking health information has been revealed to be important correlate of salt reduction practices. This finding is consistent with existing literature in LMICs showing that health education focusing on salt reduction is a key element of controlling hypertension (Van De Vijver et al., 2012). Our results add to our understanding of the importance of seeking health information by identifying other experiences and conditions further upstream in the probable causal chain that motivated participants to strongly value seeking out health information.
Support from health professionals was also an important indirect correlate of salt reduction practices. When providing health education to this population, it appears that it would be essential for health professionals to express encouragement and concern. There are eight types of health professionals working in the community health centers in Indonesia, including nurses, midwives, community health workers, and nutritionists (Dewan Perwakilan Rakyat Republik Indonesia and Presiden Republik Indonesia [Parliament of Republic of Indonesia & President of Republic of Indonesia], 2014). The number of nursing and midwifery personnel per 10,000 population in Indonesia (13.7) (World Health Organization, 2012) is lower than the global average (17.6) (World Health Organization, 2016b). Fortunately, some kader (community health volunteers) who work in posbindu provide meaningful support and others can be activated. Community health workers in Ghana who provided health education were found to be effective in lowering the salt intake of people living in their communities (Cappuccio et al., 2006). Activating community professional and lay health workers is imperative in supporting healthy behaviors among community members, particularly in resource-limited settings in LMICs.
Our findings support the health education approach of formulating motivational messages that are connected with patients’ prior health experiences. According to the principles of adult education, prior experience (both personally and vicariously) provides a basis for learning (Knowles et al., 2005), making people more aware of the potential consequences of current health behaviors and possibly motivating behavior change. The direct and indirect positive influence of prior experiences is similar to findings in another study conducted in rural Indonesia that showed that practicing healthy behaviors was associated with previous experience of illness and observing improved health status among participants and their families and friends as a result of practicing such behaviors (Mizutani et al., 2016).
Our model suggests that there are some environmental barriers to reducing salt intake. Scarcity of information about health food was the greatest barrier, along with a limited supply of healthy food in stores, limited access to food with nutritional labels, and perceptions that healthy food was too expensive. Currently, many countries have a dietary salt reduction policy in place to create a healthier environment for citizens (Hyseni et al., 2017; Trieu et al., 2015). The Indonesian Ministry of Health has developed a national strategy to improve food labeling while strengthening regulation of the food industry and fast food restaurants (World Health Organization Regional Office for the South-East Asia Region, 2012). However, studies in other LMICs such as India have shown that unlabeled food is sold commonly in rural areas making it impossible for buyers to know the level of salt content (Gupta et al., 2016). To make it possible for people to reduce their salt intake, people who prepare food in rural areas need to also reduce the amount of salt they add to food.
In this population, connecting an overall approach to Islamic spiritual practices is likely to be effective because Islamic spiritual practices, associated with Islamic spiritual support, appeared to be positively correlated with seeking information which in turn was correlated with efforts to reduce salt intake. This finding is similar to findings in previous studies in Indonesia showing that Islamic religious beliefs are a significant reason for practicing healthy behaviors (Mizutani et al., 2016). Similarly, another study has shown that performing Buddhist religious practices was related to lowering BP (Stewart et al., 2014). As written in the Qur’an, Muslims are required to practice the Five Pillars of Islam, including Salat (praying five times a day), and if people carry out these obligations, they will be rewarded by God (Ali, 2016). Specifically in terms of eating behavior, teachings in the Qur’an say consuming healthy food and avoiding excess is recommended by God (Ali, 2016). This Islamic values, which are embedded in Indonesians’ social lives, might influence their salt reduction practices. Therefore, it is essential to provide health education that is appropriate for people's cultural sensibilities and values.
This study is the first to describe salt reduction practices and their correlates among middle-aged Muslims with hypertension in rural Indonesia, and one of very few to do so in an LMIC. One limitation of this study is that about three-quarters of the participants were female because they were recruited at puskesmas during the daytime when men were typically working. Still, our analysis showed few substantial differences between men and women in their responses, suggesting that the gender ratio may not have significantly influenced the results. Considering the difference in response rates between men and women, caution should be exercised when attempting to apply our findings into men. In this population, health behaviors may differ by gender, so the gender-specific factors should be considered in future studies to better understand men's perceptions.
Conclusion
Among middle-aged people with hypertension in rural Indonesia, salt reduction practices were directly positively associated with prior health/illness experiences and with seeking health information. Seeking health information was positively associated with prior health/illness experiences, receiving support from health professionals and Islamic spiritual practice. It is important for community health professionals at puskesmas and posbindu in rural Indonesia to provide health information on hypertension reduction that is culturally meaningful based on experiences and conditions identified in this study. Our study shows that salt reduction practices were also negatively associated with environmental barriers to healthy eating practices. Thus, it is equally essential to create environmental conditions that are conducive to healthy behaviors. Those working in the health sector should consider engaging in advocacy and policy making to ensure that international and domestic food companies supply Indonesians with a wide range of low-sodium foods.
Footnotes
Acknowledgements
We would like to thank each participant who was interviewed for sharing their experiences. We would also like to express our gratitude to the research assistants, the community health centers and the district health office. This work is part of a PhD dissertation submitted to St Luke's International University, Japan.
Author contributions
MM and JT conceived the study. MM, M, HS and R obtained permission to conduct the research, recruited health centers and participants, and managed the research assistants. MM conducted the statistical analysis. MM, JT, KN and JM contributed to interpreting the output of the statistical analysis. MM drafted the manuscript and all authors contributed substantially to its writing and revision.
Availability of data
The datasets of this study are restricted by the Research Ethics Committee of St Luke's International University (No. 14-029) in order to protect participants’ privacy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Research Ethics Committee of St Luke's International University (No. 14-029). We submitted our research protocol and a request for permission to conduct this study to Badan Kesatuan Bangsa, Politik dan Perlindungan Masyarakat (the Agency for National Unity, Politics, and Community Protection) and the Dinas Kesehatan Kabupaten (the District Health Office), and permissions were obtained (No.647/070/Rekomlit/Kesbangpol/2014, No.070/2040/Um.Peg, respectively). We obtained written informed consent from all participants.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Yamaji Fumiko Nursing Research Fund (grant number N/A).