
Abstract
Background:
A meal replacement (MR) with a low glycemic index (GI) is possibly beneficial for glycemic control. However, the effects of MR on diabetes mellitus have not been studied among Thai patients with type 2 diabetes (T2DM).
Aim:
To compare metabolic outcomes between T2DM patients receiving the new MR formula (ONCE PRO) and normal controlled diets.
Methods:
A multicenter, open-labeled, randomized controlled trial was conducted. Eligible patients received either ONCE PRO for one meal daily with controlled diets or only controlled diets for 3 months. The differences in metabolic profile between the baseline and end point of each group and between groups were measured.
Results:
110 participants were enrolled; the mean difference and standard deviation in hemoglobin A1C (HbA1c) (%) from baseline were –0.21 ± 0.78 (p = 0.060) and –0.27 ± 0.60 (p = 0.001) in the MR and control groups, respectively; however, there was no significant difference between groups (p = 0.637). Patients consuming a MR instead of breakfast had a significant decrease in HbA1c (p = 0.040). Body weight (BW) and body mass index (BMI) were significantly reduced in both groups. There were no significant change in waist circumference, fasting plasma glucose, total cholesterol and triglycerides. Low-density lipoprotein cholesterol (LDL-C) was significantly decreased in the MR group compared with the control group (p = 0.049).
Conclusions:
Short-term conventional diet control and the low-GI MR product were associated with a decreased BW and BMI. Changes in the other metabolic outcomes, HbA1c, total cholesterol and triglycerides, were comparable despite ONCE PRO as the MR having a better effect on LDL-C lowering.
Introduction
Diabetes mellitus (DM) is a critical global public health problem due to its steadily increasing prevalence and huge impact on both patients and society. The prevalence of DM among adults in 2015 was estimated to be 8.8% globally (Ogurtsova et al., 2017).
Optimizing glycemic control is fundamental to reducing and delaying complications in DM patients. The American Diabetes Association recommends that pharmacologic and nonpharmacologic treatment and personalized medical nutrition therapy should be given to both complex and chronic DM patients for better outcomes (Perera and Li, 2012; WHO, 2015; Tahrani et al., 2010).
Meal replacement (MR) is one of the effective tools for weight loss and weight control. A meta-analysis of six randomized controlled trials with 487 participants over 18 years of age, with and without DM, demonstrated that participants receiving MR shakes (beverages) had greater weight loss than to those who followed conventional reduced-calorie diets (Heymsfield et al., 2003). Allison and colleagues (2003) reported that overweight or obese adults receiving soy-based MR shakes showed significant weight loss and more positive changes in total cholesterol and low-density lipoprotein cholesterol (LDL-C) levels than the control group in a 12-week prospective randomized controlled trail. Furthermore, 120 overweight or obese individuals with type 2 diabetes (T2DM) who consumed MRs had greater HbA1 and weight reduction than those with a normal diet in a 6-month randomized controlled trial (Keogh and Clifton, 2012). The consumption of MR products, as part of a comprehensive behavioral strategy, was also shown to improve weight loss and metabolic outcomes in participants with T2DM who were overweight or obese in Look AHEAD (Action for Health in Diabetes) (Pi-Sunyer, 2014).
Several studies examining the efficacy of MRs in DM patients’ outcomes were improved by using diet variation; however, a low glycemic index (GI) diet has never been observed. Low-GI diets have shown to promote health and wellness in patients with DM (Aston, 2006; Blaak et al., 2012; Liljeberg et al., 1992; Livesey et al., 2008), such as controlling glucose levels and reducing the risk of coronary heart disease (Brand et al., 1991). A MR diet in DM patients with a randomized controlled trial has never been studied in Thailand: metabolic responses are varying depending on nationality and the study setting.
The MR formula was developed as a suitable macronutrient proportion for glycemic and metabolic control with a GI of 27.99 (Thai Otsuka Pharmaceutical Co., 2016a, 2016b). The ratio of carbohydrate:protein:fat is 40:20:40, respectively. Sources of carbohydrate were maltodextrin, isomaltulose and maltitol. Isomaltulose effects include slowing glucose absorption and stabilizing the glucose level and insulin level to avoid blood sugar spikes (König et al., 2012; Lina et al., 2002). Therefore, the body stores a more balanced and prolonged energy source in glucose format. Being low-insulinemic, isomaltulose also supports the improvement of fat oxidation during physical activity, as high insulin levels hinder the use of lipids as an energy source. Moreover, soluble fiber was added in the formula for its benefits in blood glucose level stabilization, insulin sensitivity and lowering cholesterol (EFSA Panel on Dietetic Products and Allergies, 2011; Katarzyna Slizewska et al., 2012; Kishimoto et al., 2009). Fat composition was selected from highly polyunsaturated fatty acids; eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). As recommended by the European Association for the study of Diabetes (EASD), canola oil, high oleic-safflower oil, rice bran oil and fish oil were opted as qualified fat sources (Inzucchi et al., 2012). Monounsaturated fatty acid (MUFA)-rich oil sources, such as canola oil, high oleic-safflower oil and rice bran oil were also recommended in a healthy diet. Several studies reported that MUFAs promote glycemic control and cardiovascular disease prevention, owing to better insulin sensitivity and diminishing metabolic syndrome risk factors (Association, 2014, 2015; Kotake et al., 2004; Kris-Etherton, 1999; Yang et al., 2011). Vannice and Rasmussen (2014) also state that MUFAs can be used to improve insulin sensitivity in T2DM patients. Whey protein isolate (WPI) and soy protein isolate were selected as qualified protein sources. WPI can reduce the postprandial blood glucose level and is considered a suitable ingredient for patients with DM (Frid et al., 2005; Petersen et al., 2009), whereas soy protein isolate can control the cholesterol level (Ramdath et al., 2017).
The purpose of this study was to compare metabolic outcomes, glycemic levels (fasting plasma glucose (FPG), hemoglobin A1C (HbA1c) and 2-hour postprandial glucose (2-hour PPG)), lipid profiles, body weight (BW), body mass index (BMI) and waist circumference (WC), between a group of patients receiving therapy with the new MR formula (ONCE PRO) and a group of patients receiving a normal controlled diet.
Materials and methods
Study design
This multicenter, open-label, randomized controlled study was conducted among patients with T2DM recruited from the outpatient departments of six university hospitals in Thailand (Phramongkutklao Hospital, Ramathibodi Hospital, Siriraj Hospital, Maharaj Nakorn Chiang Mai Hospital, Srinagarind Hospital and Songklanagarind Hospital) from December 2014 to October 2015. The study was reviewed and approved by relevant Institutional Review Boards or Independent Ethics Committees then conducted according to Good Clinical Practices, the Declaration of Helsinki and its subsequent amendments and national regulations. The study was registered with http://www.clinicaltrials.in.th, primary site ID: TCTR20131206002.
Study participants
Individuals were enrolled in the study if they met the following four criteria: an age of 18 years or older; a HbA1c level of 7–9%, a diagnosis of T2DM at least 6 months prior to enrollment; and a history of taking the same antihyperglycemic agents and lipid-lowering agents (if required) at stable doses for at least 3 months prior to enrollment. Certain individuals who met the study’s exclusion criteria were excluded from the study for the following reasons: a history of severe hypoglycemia (neuroglycopenia); severe complications (e.g., amputation or diabetic coma), gastrointestinal dysfunction (e.g., short bowel syndrome or colectomy); cardiovascular diseases (e.g., ischemic heart disease, stroke or history of heart failure up to 6 weeks before enrollment); abnormal laboratory values, including hemoglobin <10 g/dL, a white blood cell count <3 × 106/μL, a platelet count <100 × 106/μL, aspartate aminotransferase or alanine aminotransferase >3 times the upper limit of normal, total bilirubin >2 times the upper limit of normal or a glomerular filtration rate <60 mL/min/1.73m2 according to the modification of diet in the renal disease formula), psychiatric disorders; alcoholism; drug addiction; active thyroid dysfunction; malignancy within 5 years before enrollment; pregnancy or lactation or refusal to use an effective birth control method; the use of herbal products; taking corticosteroids (except topical steroids) for at least seven consecutive days or other investigational medication up to 4 weeks before the date of enrollment; and allergy to WPI, soy protein isolate or fish oil.
Study procedure
After informed consent was received, the participants were assigned a number in ascending order that corresponded to their admission in the study. The research team assigned the participants to be randomized in balanced blocks, generated by a statistician, with an equal probability of being assigned to the group that received MR for one meal per day plus normal controlled diets for their other meals (the MR group) or a group that ate only a normal controlled diet (the control group). The two groups followed the prescribed diets for 90 days. The participants in the MR group were given advice on how to prepare the MR, which contained 30% of the total daily energy requirement: mix the dry powder with drinking water and consume it as a replacement for one meal per day.
The MR product (called ONCE PRO) is a novel formula developed by the Thai Otsuka Pharmaceutical Company Limited (Thai Otsuka Pharmaceutical Co., 2016a, 2016b). ONCE PRO is a water soluble powder with a low GI (27.3) and the appropriate caloric distribution of carbohydrate, protein and fat (40%, 20% and 40%, respectively), improving glycemic control in DM patients (Boonyavarakul, 2013; Brown et al., 2015; Thai Otsuka Pharmaceutical Co., 2016a, 2016b) (Table 1). The intention of particular fat type and content, in this formula, is specifically to delay gastric emptying, which contributes to limitation of blood glucose fluctuations(Brown et al., 2015).
Meal replacement formula.
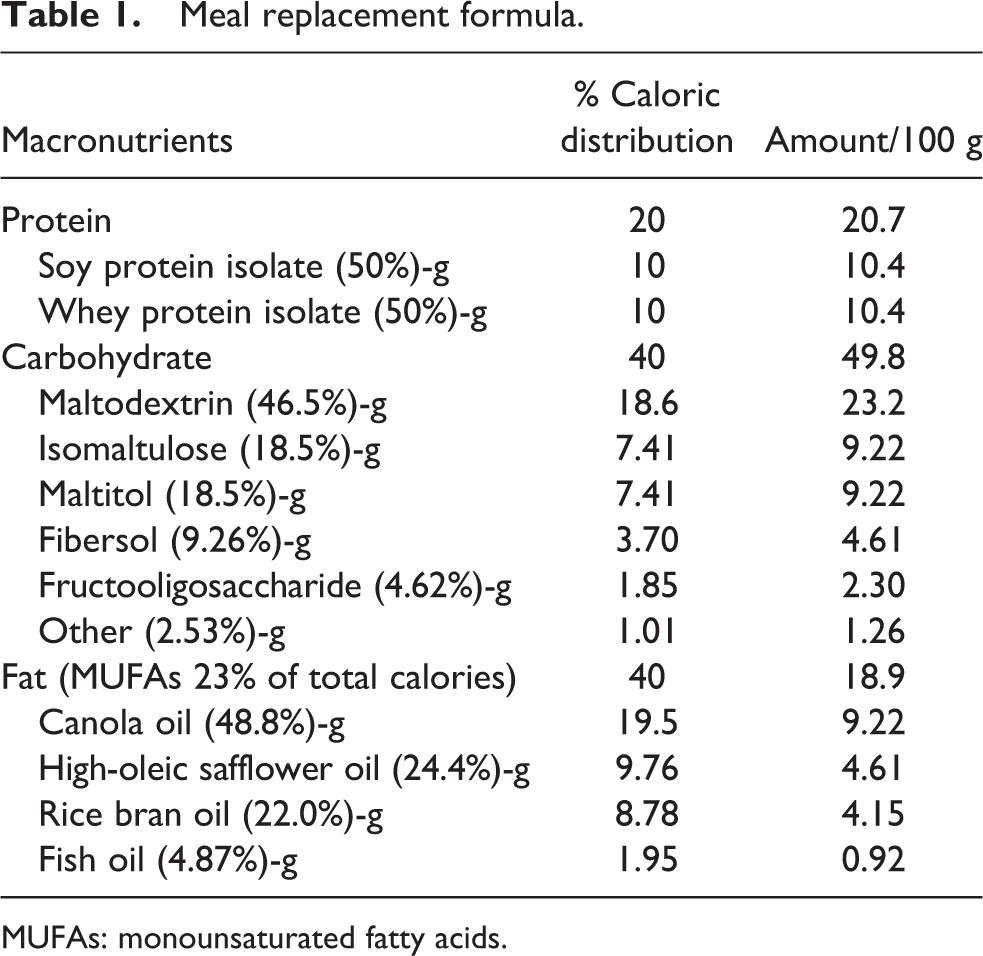
MUFAs: monounsaturated fatty acids.
All participants received a dietary record and individual dietary counseling sessions from trained nutritionists/dieticians of each hospital at baseline. The nutritional goal was to achieve 25–30 kcal/kg/day based on their ideal BW and physical activity (Newton and Garvey, 2012), with a caloric distribution of protein, fat and carbohydrate of 20%, 30% and 50%, respectively, due to expert doctors’ suggestions and recommendations from the Canadian Diabetes Association (Dworatzek et al., 2013). The ideal BW was calculated using the following equations from the Hamwi formula (Hamwi and Danowski, 1964): (1) 48 + 2.7 kg for each 2.5 cm over 150 cm for men and (2) 45.5 + 2.2 kg for each 2.5 cm over 150 cm for women.
During the study period, the participants periodically filled in a dietary record along with their individual dietary counseling sessions and dietary reviews for validating information. All participants were required to come to their respective hospitals at the baseline and at the end or during the study period to assess their FPG, HbA1c and lipid profiles, measured by each hospital’s central laboratory using automated analyzers of each center as well as their BW, BMI and WC. In a separate period of the study, to obtain information about the different glycemic responses to the MR and the reference formula, 2-hour PPG tests with 75 g of carbohydrate were performed in the MR group after the intake of the MR (148.9 g, 633 kcal) and reference formula (125 g, 563 kcal). Each formula was provided once on different days; the reference formula was an enteral product generally used in a hospital.
Efficacy assessment
The primary outcomes of this study were the differences in HbA1c levels between the baseline and end point (day 91) in each group and between groups. The secondary outcomes were the differences in FPG, lipid profiles, BW, BMI and WC between the baseline and end point in each group and between groups. The outcome assessments in the MR group were performed only on the participants who had followed the study’s dietary guidelines for 90 days.
Data analysis and statistical methods
The data were analyzed using per protocol analyses. All analyses were performed with SPSS version 18.0 (SPSS Inc., Chicago, IL, USA), using a two-sided test and a significance level of 0.05. The data distribution was evaluated using the Kolmogorov–Smirnov test and did not differ significantly from a normal distribution. The participants’ characteristics and study outcomes of the two groups were analyzed with a repeated-measures analysis of variance (ANOVA) for within-group comparisons and Student’s t-test and chi-square test for between-group comparisons.
The sample size was obtained using the formula developed by Rosner (Bernard, 2000). A total sample size of at least 66 (33per group) achieved 80% power to detect a mean difference of 1.3% in HbA1c. This assumed a SD of 1.88 and correlation between measures of 0.8, with the significance level of 0.05 based on a study by Tatti et al. (2010). To allow for a dropout rate of 20%, the total sample size for this study was 120 (60 per group).
Results
Participant baseline characteristics
A total of 152 individuals were screened, and only 119 were eligible. Among them, nine participants discontinued participation for the following reasons: three violated the protocol; two were unwilling to continue; two had hypoglycemia, one had diarrhea; and one suffered a loss of appetite and wished to drop out. Therefore, only 110 participants completed the study, 53 and 57 participants in the MR and control groups, respectively (Figure 1). The mean age was 56 years, and the average BMI was 27.8 kg/m2. There was no statistically significantly difference in BMI, energy intake or metabolic profiles, including the HbA1c, FPG and lipid profiles, between the two groups (Table 2).
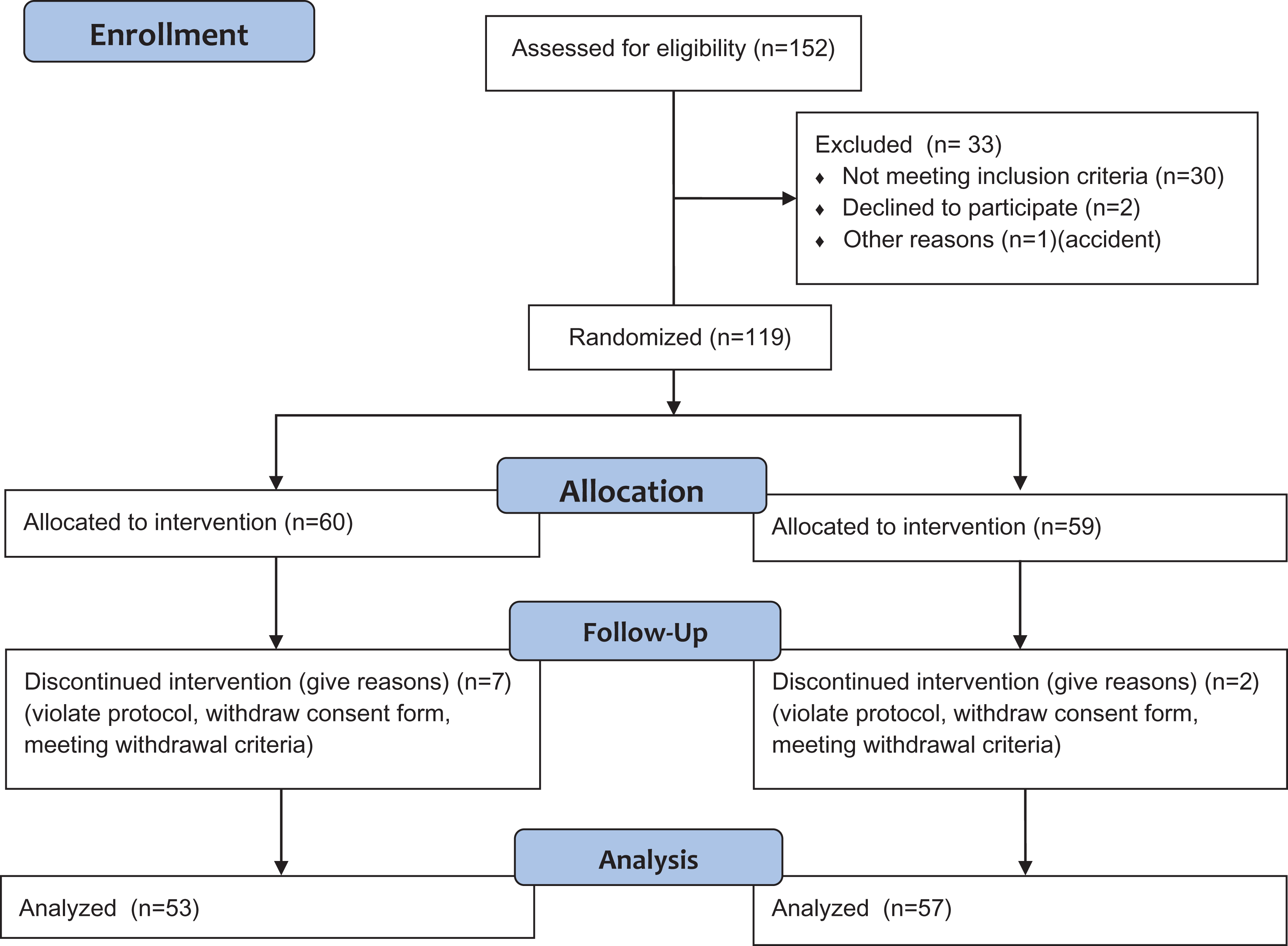
Study flow from recruitment and screening to the final analysis.
Measured baseline demographics of participants (n = 18). Data are presented as the frequency and mean ± SD.
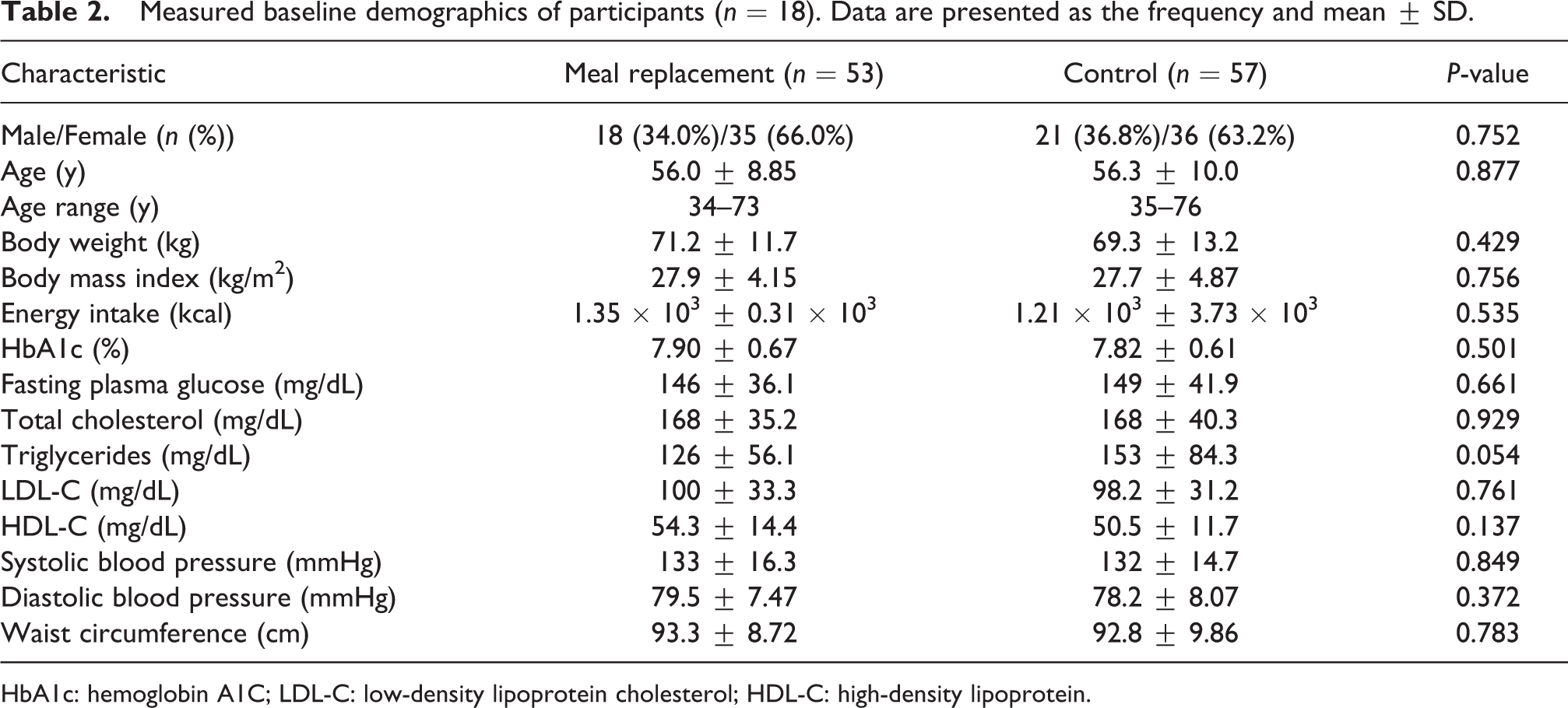
HbA1c: hemoglobin A1C; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein.
Changes in HbA1c level
The mean HbA1c level decreased gradually from baseline in both groups; however, HbA1c reduction at 3-month treatment was statistically significant only in the control group from 7.82 ± 0.61 to 7.55 ± 0.79, p = 0.001. In the MR group, the HbA1c level also decreased from 7.90 ± 0.67 to 7.69 ± 0.74, but it was not significantly different. Likewise, there was no significant difference in HbA1c levels between the two groups (p = 0.637) (Table 3). In the subgroup analysis, we found that only participants who consumed a MR for breakfast had a significant reduction in HbA1c compared with the baseline (p = 0.040) (Table 4).
Outcome assessment after 90-day period. Data are shown as the mean difference from the baseline
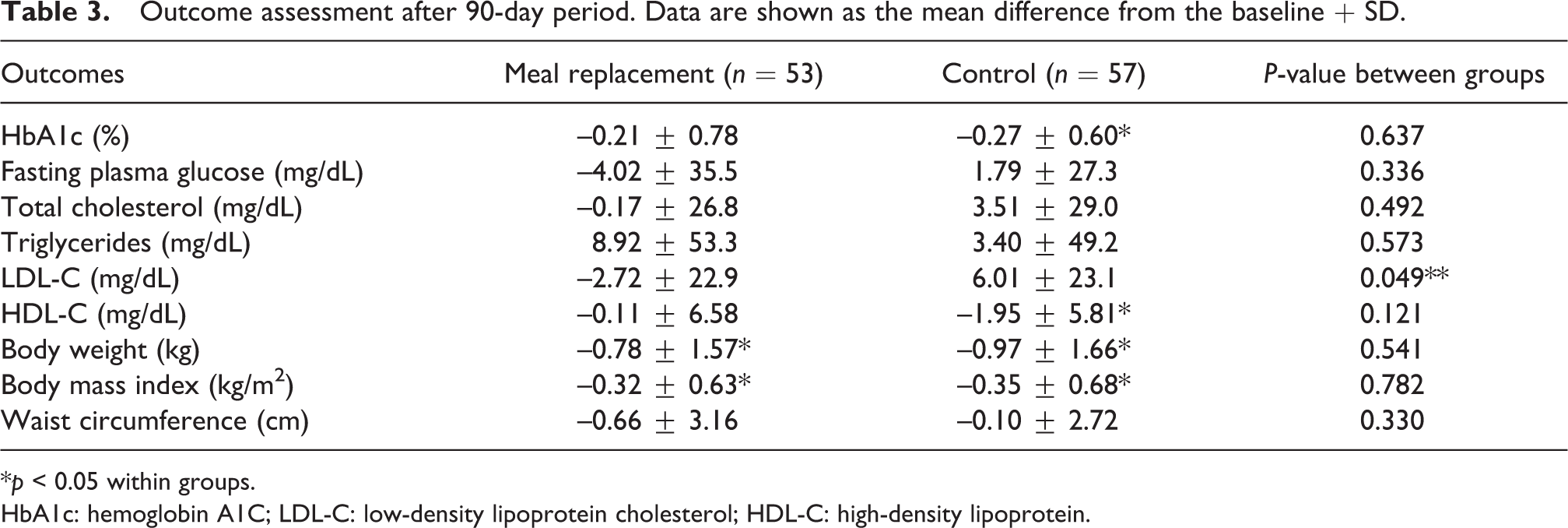
*p < 0.05 within groups.
HbA1c: hemoglobin A1C; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein.
Changes in hemoglobin A1C (HbA1c) (%) at different times of meal replacement consumption. Data are shown as the mean difference
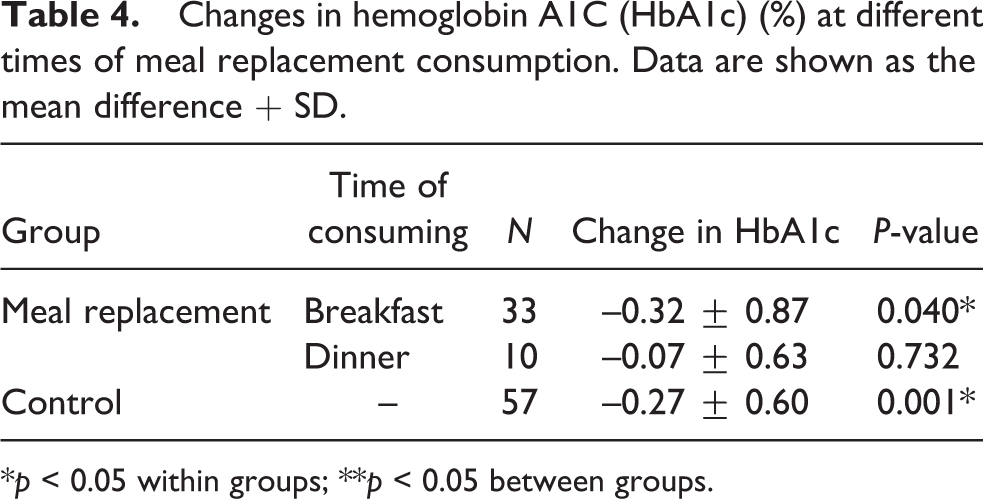
*p < 0.05 within groups; **p < 0.05 between groups.
Changes in 2-hour PPG
A statistically significant difference (p < 0.001) in 2-hour PPG levels between the intake of the MR and the reference formula was analyzed. Two-hour PPG levels after consumption of the reference formula increased by 111 mg/dL from 147 ± 33.3 to 258 ± 64.0 mg/dL, whereas there was a lower increase of 2-hour PPG of 71.5 mg/dL from 150 ± 34.2 to 222 ± 50.8 mg/dL after consumption of the MR (Figure 2).
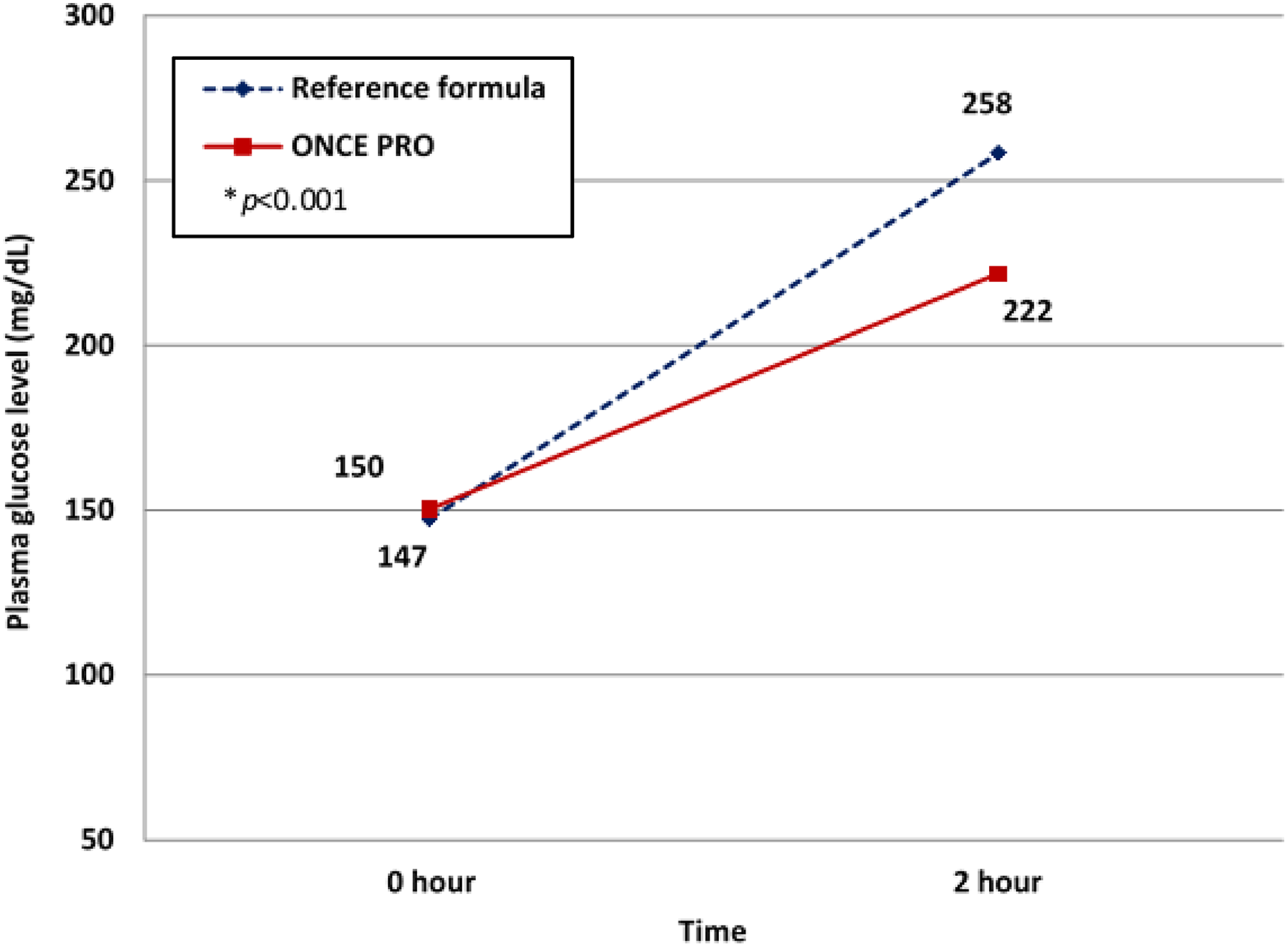
Two-hour postprandial plasma glucose level after consumption of 75 g of glucose through the reference formula (blue) and the meal replacement (red). (Color online only.)
Changes in BW and BMI
BW and BMI decreased significantly at 3-month treatment in both groups: 0.78 and 0.97 kg for BW and 0.32 and 0.35 kg/m2 for BMI in the MR and control groups, respectively. However, there were no statistically significant differences in BW and BMI between the two groups after the treatment (Table 3).
Changes in lipid profiles
LDL-C level decreased (–2.72 mg/dL) in the MR group but increased (+6.01 mg/dL) in the control group. In addition, the difference in LDL-C between groups was marked as significant (p = 0.049) (Table 3). High-density lipoprotein (HDL-C) decreased in both the MR and control groups, but only in the control group was this shown to be statistically significant.
In this study, total cholesterol decreased in the MR group, while in comparison it increased in the control group. Triglycerides were reported to have increased but did not reach statistical significance either within or between groups.
Discussion
Achieving an optimal HbA1c level is fundamental to T2DM management because it is associated with microvascular complication reduction (Shi et al., 2013). Moreover, weight loss from lifestyle modification has been shown to result in significant improvement in glycemic control, blood pressure and lipid profiles (Espeland, 2007). ONCE PRO is effective to lose weight and is beneficial for HbA1c reduction in those having a MR for breakfast.
This study demonstrated that a diet, either MR therapy or a controlled meal plan, with the nutritional goal of 25–30 kcal/kg/day based on ideal BW and physical activity, and a balanced caloric distribution of protein, fat and carbohydrate of 20%, 30% and 50%, respectively, could significantly reduce participants’ BW and BMI. Satisfactory HbA1c control and WC reduction were shown in both groups, yet the change of HbA1c was statistically significant only in the control group. The mean reduction of FPG was approximately 4 mg/dL in the MR group; on the contrary, it increased by 1.79 mg/dL in the control group. Reduction in BW, glucose, insulin and HbA1c levels in the MR group compared with the control group was in accordance with the study of Yip et al. (2001). In general, patients with DM are advised to have a smaller portion during dinners, compared with the others meals (Spence, 2017). Consequently, subgroup analysis demonstrated that only the MR for breakfast group was significantly effective in HbA1c reduction.
The PPG level is another crucial outcome in T2DM management due to its relation with risks of cardiovascular diseases and other DM-related complications (Ceriello, 2010; Ludwig, 2002). In the present study, the MR group showed greater capacity to control 2-hour PPG, compared with the reference formula, even though the MR provided higher caloric value. It can be concluded that low-GI carbohydrates (i.e., isomaltulose, maltitol, Fibersol and fructooligosaccharide (FOS)) in the formula benefit glycemic control. Further studies of maltodextrin and isomaltulose show similar results of reducing the glucose-uptake rate, stabilizing glucose and insulin levels and avoiding glucose spikes (van Can et al., 2012). Likewise, maltitol gives lower glycemic and blood insulin responses (Kamoi et al., 1972). Isomaltulose also promotes fat-provided energy, hence enhancing performance endurance (König et al., 2012; Lina et al., 2002). Soluble fibers, Fibersol and fructooligosaccharides in the formula, affected gastric emptying prolongation, blood glucose fluctuation prevention, the glucagon-like peptide-1 secretion inducer and gut microbes and lipid metabolism improvement (Abbott, 2014; Campbell, 2006; Festi et al., 2014; Kobyliak et al., 2015). Several studies have exhibited extensive positive effects of this MR formula on glycemic levels and insulin sensitivity (Keogh and Clifton, 2012; Kishimoto et al., 2009; Slizewska et al., 2012; Tetens, 2011).
Most participants have been taking lipid-lowering agents (statin) in proportions of 94.3% in the control group and 93.0% in the MR group; therefore, their LDL-C levels at baseline were in the normal range and there were no other beneficial effects, as expected, after daily intake and at the end of the study. Nevertheless, the MR group showed a statistically significant larger LDL-C reduction compared to the control group. According to Yip et al.’s study (2001), similar results were reported that MRs gave significant LDL-C reduction. Even though both groups received the same dietary counseling from nutritionists or dieticians, the results were still doubtful: an increase in LDL-C in the control group and triglyceride in both groups, in contrast to a decrease in HDL-C in the control group. These questionable results should be investigated in further studies. In the previous studies, MUFAs were mentioned to be of benefit to T2DM patients. To illustrate this, MUFAs promote insulin sensitivity, which can prevent cardiovascular disease in patients by reducing their risk factors. As a result, MUFAs in the formula present positive outcomes on total cholesterol and LDL-C lowering, while maintain the HDL-C level. WPI is a suitable protein source for DM patients due to its high content of branched-chain amino acids, which helps stabilize insulinotropic response and insulin secretion (incretin effect), resulting in PPG reduction (Floyd et al., 1966; Frid et al., 2005; Petersen et al., 2009).
The limitation of this study is the 3-month period, which is not considered as a long-term study. In additional, a nutrition counselor should be monitored strictly in both groups in order to obtain better compliance. Nevertheless this multi-center prospective study should be considered ONCE PRO as an option in treating T2DM and the factors that are altered by MR diet should be studied in the future trial.
Conclusion
The control of the plasma glucose level in diabetic patients can be achieved by using MRs as dietary control. Three-month consumption of a low-GI MR provided significant improvement in glucose control, lipid profile, BW and BMI. In conclusion, ONCE PRO can be considered as a practical and convenient MR to help DM patients with their diet.
Footnotes
Acknowledgements
The authors thank the DM nurses and dietitians of Phramongkutklao Hospital, Ramathibodi Hospital, Siriraj Hospital, Maharaj Nakorn Chiang Mai Hospital, Srinagarind Hospital and Songklanagarind Hospital for data collection and patient education.
Author contributions
All authors contributed equally to this work; Apussanee Boonyavarakul, Rattana Leelawattana, Chatlert Pongchaiyakul, Supawan Buranapin, Parinya Phanachet and Pornpoj Pramyothin performed the research; Apussanee Boonyavarakul contributed to editing, reviewing and final approval of article.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Consent for publication
Detail as attached file.
Ethical approval
The study was reviewed and approved by Ethic Committee of the Faculty of Medicine, Phramongkutklao Hospital, Price of Songkla University, The Khon Kaen University, Chiang Mai University, Ramathibodi Hospital and Siriraj Hospital Ethics Committee for Human Research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was sponsored by the Thai Otsuka Pharmaceutical Co., Ltd. This included study products, patient compensation and laboratory fee.