
Abstract
Technology innovation and adoption are key economic imperatives for growth in India’s economy, and especially in the healthcare sector. As an example of firm innovation adoption, this study explores the adoption of web accessibility standards by small health care organizations in India. Adoption is found to be uniformly poor, irrespective of the size, financial resources, or type of healthcare institution. Though small health care organizations located in the largest metros had better compliance, they too fell short of the standard. The findings highlight challenges of healthcare innovation adoption by small firms in a developing country context.
Executive Summary
Rapid adoption of information technology innovations has been identified as a key goal for economic growth and modernization in India. This is especially the case for the healthcare sector that has confronted challenges of service quality and cost efficacy. This study explores web accessibility in India’s healthcare sector by examining the compliance of the websites of small health care organizations (SHCOs) in the country with the internationally recognized Web Content Accessibility Guidelines 2.0 (WCAG 2.0) standards and the Indian 2016 Rights of Persons with Disabilities (RPD) Act, apart from assessing factors predicting compliance. While web accessibility for larger hospital websites in India has been previously studied, no comparable study has been done for smaller hospitals and healthcare centres where many Indians receive care. We measure the compliance of the websites of SHCOs—accredited by the National Accreditation Board for Hospitals and Healthcare Providers (NABH) in India—with the WCAG 2.0 using the Functional Accessibility Evaluator 2.0 (FAE 2.0) online tool. Following the Berry model of organizational innovation, we examine whether the financial resources of the hospitals, the type of services they provide (general healthcare or specialized), their location and the complexity of their websites could predict FAE scores. Ordinary least squares (OLS) regression is used to estimate the results. Only one of the 101 sampled websites achieved compliance with WCAG 2.0 standard, and that too, partially. Only the location was a significant predictor of accessibility compliance in the direction expected from theory. Compliance with web accessibility standards was uniformly poor, irrespective of the size, financial resources or type of healthcare institution. There is an urgent need to improve web accessibility standards, through awareness campaigns and policy initiatives, to ensure that the most disadvantaged patient groups, such as the elderly and people with disabilities, have access to healthcare information and services.
It has been well known since at least the 1970s that investments in capital and labour can only partially explain patterns in national economic growth, with the rest attributable to improvements in productivity (Abernathy & Utterback, 1978; Griliches, 1979; Quinn, 1979). Investments in research and development and policy frameworks encouraging firm innovation are imperative for economic growth, especially for developing countries such as India, seeking to rapidly modernize and technologically upgrade their economies. Though indigenous innovation remains the holy grail, the firm-level adoption of productivity-enhancing and quality-improving technologies can boost economic growth in the short term. However, significant challenges emerge when seeking to promote technology adoption and innovation in developing countries (Cirera & Maloney, 2017; Lee, 2019).
It is therefore inevitable that significant research attention is focused on the factors that predict the adoption of technology and business innovations by private enterprises, government agencies and other organizations (Almeida et al., 2017; Hovav et al., 2004; Wisdom et al., 2014). Research has sought to identify the factors that predict firm innovations, including organizational characteristics (Allen et al., 2017), attributes of innovations (Vagnani & Volpe, 2017), the process of adoption decision-making (Hameed et al., 2012) and the firm’s external environment (Oliveira & Martins, 2010). Various theories such as the technology–organization–environment (TOE) framework (Tornatzky & Fleischer, 1990), the technology acceptance model (TAM; Davis, 1989) and the unified theory of acceptance and use of technology (UTAT; Venkatesh et al., 2003) have been proposed to study firm-level technology adoption.
No sector of the economy is in a greater need of technology adoption than the healthcare sector. The problem is especially acute in large developing countries such as India, where the healthcare system is struggling to provide adequate services to a growing population with inadequate health insurance, a low doctor–patient ratio, concentration of doctors in big cities and the dual burden of coping with both communicable and non-communicable diseases (Mishra, 2021). The automation and online deployment of healthcare systems promises to be a cost-effective means of making medical services available to a wider public. Lack of access was especially critical during the COVID-19 pandemic. About 44% of the respondents in an American Association on Health and Disability survey reported experiencing challenges in access to medicines, treatments and medical professionals due to quarantine restrictions (Drum et al., 2020).
In this context, this article seeks to investigate the factors that predict the adoption of a technology innovation by healthcare institutions in India, a large developing country. We propose to study the adoption of web accessibility standards (specifically WCAG 2.0) on the websites of small, accredited hospitals and healthcare institutions as an example of technology innovation. While several national policy documents in India, including the 2006 National Policy for Persons with Disabilities (NPPWD) and the 2016 RPD Act, expect all public services should be provided in a ‘barrier-free environment’, they stop short of mandating an explicit web accessibility standard. The absence of a government mandate makes the voluntary adoption of web accessibility standards by healthcare institutions a good example of the adoption of new technology innovations by firms, driven exclusively by firm-specific factors. While web accessibility for larger hospital websites in India has been previously studied (Kaur et al., 2017), no comparable study has been done for smaller hospitals and healthcare centres where many Indians receive care. Due to the scarcity of studies on web accessibility standards in the Indian healthcare sector, our article is also in the form of a benchmarking study with the goal of advocating for improvement.
The article proceeds as follows. In the following section, we explicate the concept of web accessibility, the relevant policies in India and provide an outline of the Indian healthcare sector. We then present theories of organizational innovation and explain why we chose the public management innovations model (Berry, 1994) for our analysis. We then present our method, including our sample selection process and the FAE 2.0 online utility to measure the websites’ conformity to WCAG 2.0. Our findings and recommendations are presented thereafter.
WEB ACCESSIBILITY AND THE INDIAN HEALTHCARE SECTOR
According to the World Health Organization, disability refers to the ‘interaction between individuals with a health condition … and personal and environmental factors (e.g., negative attitudes, inaccessible transportation and public buildings and limited social support)’ (World Health Organization, 2021). People with disabilities face barriers in accessing health, education, transportation, information and work services, which increases dependence and limits their participation in society (Wagner, 2021).
For individuals with disabilities, lack of web accessibility can be a double disadvantage since many public and government services, including vitally important healthcare services, are increasingly migrating online. The World Wide Web Consortium recommends that people with diverse hearing, movement, sight and cognitive abilities must be able to ‘perceive, understand, navigate and interact with the Web’ (W3C, 2021). The W3C’s WCAG 2.0 includes testable success criteria and advisory techniques to make web content accessible to people with different disabilities such as ‘blindness and low vision, deafness and hearing loss, learning disabilities, cognitive limitations, limited movement, speech disabilities, photo sensitivity and combinations of these’ (W3C, 2008). For example, graphic elements (such as photographs, drawings and charts) presented on websites need to have ‘a text alternative that serves the equivalent purpose’ (W3C, 2019, section 1.1.1) that may be read by text-to-speech conversion software. Similarly, online audio materials (newscasts and podcasts) need to be close-captioned (W3C, 2019, section 1.2.4).
Although most countries have drafted web accessibility laws, their adoption across the globe has been uneven and incomplete (Kuzma et al., 2017). Kulkarni (2018) outlines barriers to accessibility in institutional, societal and technological contexts. Compliance to accessibility standards has been found to be poor in education (Acosta-Vargas et al., 2018; Nir & Rimmerman, 2018), transportation (Agrawal et al., 2019) and even on government websites (Bai et al., 2021). Several scholars have highlighted the poor accessibility of healthcare websites in various countries (Alajarmeh, 2022; Kaur et al., 2017; Llinás et al., 2008; Martins et al., 2016; Yi, 2020). An Indian study evaluated the accessibility, usability and security of hospital websites in the country’s metropolitan cities and found that the adoption of WCAG 2.0 guidelines remains low (Kaur et al., 2017). A more recent study evaluated the accessibility of public health websites of the top 25 countries affected by the COVID-19 pandemic and found that a vast majority exhibited accessibility problems of varying degrees (Alajarmeh, 2022).
What factors may explain non-adoption? One study of 343 county government websites in the United States found that financial constraints, lack of awareness in the leadership and location far from urban areas are likely to be associated with non-adoption (Bai et al., 2021). These factors are certainly prevalent among small healthcare institutions in India. But non-adoption of web accessibility standards in these institutions presents a special problem. A majority of Indians visit private healthcare institutions despite the cost of treatment being higher than that of public facilities (Chatterjee & Srinivasan, 2013). Private sector healthcare is highly fragmented, with 80% of them being small clinics and nursing homes (less than 30 beds), while 6%–7% are 100–200 bed size hospitals (Chatterjee & Srinivasan, 2013).
Compounding the reliance on small health clinics and hospitals is the low level of health spending in India. Total healthcare expenditures are estimated to be 3.9% of the gross domestic product (GDP), significantly below the world average of 9.9% (Tikkanen et al., 2020). An estimated 65% of this spending came from personal budgets and the rest from public expenditures. Consequently, India’s per capita public expenditure on healthcare is among the lowest in the world. A national health policy announced in 2017 declared that the country will increase its public health spending to 2.5% of GDP, but currently the sector remains woefully underfinanced.
With staff shortages, inadequate medical infrastructure and overcrowding, information technology has been proposed as a means of improving healthcare services, especially during a pandemic. The Indian government formulated guidelines to facilitate the effective practice of telemedicine in the country in 2020 (Mishra, 2020). However, telemedicine in a country like India is likely to widen existing disparities in access: the lack of access to good quality Internet, gender and geographical disparity in Internet access, poor infrastructure, lack of clarity in data protection and privacy laws pose major hurdles in the success of digital health practices (Dash & Ramasamy, 2020).
Online delivery of healthcare services is likely to be more challenging for persons with disabilities. According to the latest available decennial census (conducted in 2011), 2.1% of the total population of India lives with a disability (Kaur et al., 2017). However, one must consider the possibility that this figure could be an underestimate since the stigma associated with disability in India may have contributed to under-reporting, especially among women and people living in rural areas (Saxena & Saxena, 2015). Further, people with disabilities face technological barriers in their attempts to access healthcare services online, apart from attitudinal, physical, communication and financial barriers.
Although the Indian Constitution protects the rights of all individuals (including those with disabilities) against discrimination in education, employment and public services, including healthcare, the country has made inadequate progress in guaranteeing the online legal rights of persons with disabilities. The Persons with Disabilities (PWD) (Equal Opportunities, Protection of Rights and Full Participation) Act, 1995, promoted opportunities in government employment, housing, business loans for persons with disabilities (National Institute for Empowerment of Persons with Multiple Disabilities, 1995) but had no mention of non-discrimination in access to information technologies. The NPPWD of 2006 (Ministry of Social Justice and Empowerment, 2006) promoted assistive technologies (including Braille-enabled devices) and encouraged a ‘barrier-free environment’ in education and work. However, the policy focuses almost exclusively on the physical environment, such as ‘buildings, places, and transportation systems’, with no reference to the online environment.
The RPD Act, enacted in 2016, focused somewhat more on the online environment. It required the government to enunciate ‘standards of accessibility for the physical environment, transportation, information and communications, including appropriate technologies and systems’ (Chapter 8, Section 40) (Ministry of Law and Justice, 2016). While the Act promotes accessible formats for audio, print and electronic media; audio description, sign language interpretation and close captioning for television programming; and universal design for electronic goods and equipment, it does not identify a web accessibility standard or make one mandatory for all public and private websites. Previously, the 2009 Guidelines for Indian Government Websites (GIGWs) had said that government websites should be made ‘usable, user-centric and universally accessible’ and that all Indian government websites and apps should conform to WCAG guidelines (National Informatics Centre, 2018, p. 4), but as the name suggests, the GIGW standards apply only to government websites. No similar standard is operative in India currently for non-governmental websites.
As the above discussion makes clear, there is currently no government policy or regulatory mandate for the adoption of web accessibility standards by non-government websites in India. The voluntary adoption of web accessibility standards by healthcare institutions is an example of the adoption of new technology innovations or business practices by firms, driven exclusively by firm-specific factors. An extensive literature exists on the factors that incentivize and enable firms to adopt innovations. The following section reviews some of these theories as a means of identifying the variables to use in our empirical analysis.
THEORIES OF FIRM INNOVATION ADOPTION
Research interest in the diffusion of innovations has a pedigree that extends at least to over a century, much of which was reviewed and systematized in Everett Roger’s influential Diffusion of Innovations (1962). Rogers identified several characteristics of adopters (preference for novelty, dense social networks, higher income and education, etc.) and of innovations (relative advantage, compatibility, trialability, complexity, etc.) that contribute to faster rates of adoption. However, much of this tradition was focused on the adoption of innovations by individuals. Though the diffusion of innovation framework has been used to study adoption by firms as well (see, e.g., Hovav et al., 2004), theories specifically focused on innovation adoption by enterprises later emerged.
As the following discussion will make it clear, theories of innovation adoption have addressed adoption by many types of organizations, including private enterprises, community groups, non-profits and government agencies. For ease of exposition, all of these entities are hereafter referred to as ‘firms’. Research has helped identify factors in the adoption decision of firms that do not apply at the level of individuals: for example, government policies and regulatory mandates, intra-firm coordination, interconnection with supplier and client networks, the need to stay competitive within industries, the role of external consultants and industry bodies, etc. (Wisdom et al., 2014). Theories of innovation adoption by firms have been distinct from, even as they are strongly influenced by, Rogers’s theory of the diffusion of innovations.
Meta-analyses of the theories of firm innovation have found that theories focus on certain common elements: organizational characteristics (Allen et al., 2017), attributes of innovations (Vagnani & Volpe, 2017), the process of innovation adoption (Hameed et al., 2012) and the firm’s external environment (Oliveira & Martins, 2010). Wisdom et al. (2014) synthesized 20 theoretical frameworks on the basis of a ‘narrative synthesis approach’ and identified the following elements: external factors (such as government policy and regulation, financial incentives and social networks), organizational characteristics (absorptive capacity, leadership, organizational values and culture, and operational size and structure), innovation characteristics (complexity, relative advantage, observability, cost efficacy and ease of use) and staff/individual characteristics (attitudes, motivation, knowledge and skills).
Specific theories bring together these elements in various combinations. For example, the TOE framework theorizes how innovation attributes, firm characteristics and environmental pressures influence the adoption decision (Tornatzky & Fleischer, 1990). The TAM, applicable to both individual and firm-level adoption, posits that perceived usefulness and perceived ease of use influence adoption (Davis, 1989). The framework was later elaborated and extended to include additional factors such as subjective norms and voluntariness (TAM2), eventually resulting in a synthesis of eight theories of technology adoption in the UTAUT (Venkatesh et al., 2003). The public management innovation model posits four factors leading to firm innovation: agency resources, leadership, agency orientation (responsiveness to its market) and regional diffusion (Berry, 1994).
These theoretical insights have also generated an extensive empirical literature. Since the focus of this article is on innovation adoptions in the healthcare sector, we concentrated on the application of firm innovation theories in this subfield. Almeida et al. (2017) interviewed managers of public healthcare institutions in Brazil and identified eight drivers of information technology innovation in healthcare. Notably, some of these drivers, such as government mandates, community interest and the socio-economic characteristics of the local community, may be counted as part of the firm’s external environment. Baral and Verma (2021) studied cloud computing adoption in the Indian healthcare sector, using an extension of Tornatzky and Fleischer’s (1990) TOE model: in addition to technology factors (relative advantage, security and compliance), organizational factors (firm size, firm scope, leadership support and innovation acceptance) and environmental factors (competition, partner pressure and regulatory support), they added a fourth dimension, ethics, relevant for the deployment of cloud computing (managers’ sensitivity to data control, reliability of technology and prohibitions on unauthorized use of patients’ data). Structural equation modelling (SEM) found that the model was able to predict cloud computing adoption.
A major portion of the literature on healthcare innovation focuses on success factors and the consequences of adoption such as improved healthcare outcomes, efficiency and hospital productivity. For example, Cresswell and Sheikh (2013) conducted a meta-analysis of empirical research on healthcare information technology (HIT) and concluded that a key success factor was ensuring the ‘fit’ between the characteristics of the technology, the skills of healthcare personnel and organizational processes. Skinner and Staiger (2015) found that hospitals were able to improve treatment outcomes for cardiac patients while also increasing productivity by incorporating technology innovations.
Our theoretical model to study the adoption of web accessibility standards by Indian hospitals emerges out of this literature review. As shown earlier, most theoretical models include a combination of firm characteristics, innovation attributes and environmental factors. However, since our study focuses on a single innovation (adoption of WCAG 2.0), innovation attributes are not likely to be differentiators in the adoption decision. Also, since we focus on a relatively narrow set of adopters (NABH-certified small healthcare organizations in India), we do not anticipate wide discrepancies in environmental factors. We therefore decided to adopt Berry’s (1994) public management innovation model that focuses exclusively on firm characteristics as our theoretical framework. Specifically, we used a modified Berry model used by Bai et al. (2021) for this study. The key variables are defined as follows.
The following section presents our methodology and sources of data on Indian private hospitals, on the basis of which we analyse the current status of web accessibility compliance in the Indian healthcare sector.
METHODS
First, hospitals were selected from the hospitals listed with the National Accreditation Board for Hospitals and Healthcare Providers (NABH) that operates an accreditation programme for healthcare organizations. The NABH accredits a variety of healthcare providers, including hospitals, SHCOs, blood banks and blood storage centres, medical imaging providers, and dental clinics and eye care organizations (NABH, 2020). At the time of data collection, 870 hospitals, 502 SHCOs, 105 blood banks, etc. were accredited by the NABH. These are only a small percentage of the 43,486 private hospitals and 25,778 public hospitals in India (Jaffrelot & Jumle, 2020). Accreditation systems are only now emerging in India, and few hospitals are formally accredited, and fewer SHCOs. The accreditation programme for SHCOs was started in the year 2010. Hospitals, day care centres and super-speciality centres (with up to 50 beds) are eligible to apply for accreditation under this category.
To clean up our sample, SHCOs on the NABH list that did not have a website or had websites under maintenance were excluded. Institutions which were categorized as ‘To be removed from accredited list’; ‘Shifted to ECO (Eye Care Organization)’; ‘Renewal under process’; ‘Application closed’, etc., were also not included in the sample. From the remaining SHCOs, a random sample of 101 hospitals was selected.
In the second stage, data for the selected hospitals were coded from the information provided on the hospital website. Categories included the year of establishment, metro location, number of doctors, number of medical departments or specializations, mention of the word ‘disability’ and/or ‘inclusivity’ in the mission and vision statement of the hospital, and whether the hospital was a speciality unit or a general one. Websites were evaluated in December 2021 for WCAG 2.0 compliance using the Functional Accessibility Evaluator 2.0, an automated tool developed by the University of Illinois. 1 The FAE evaluates a website’s conformance to the WCAG 2.0 Standard of website accessibility. For each website, the FAE 2.0 generates a score ranging from 0 to 100, based on the number of elements that pass and fail the requirements, or require manual evaluation. A score below 50 indicates non-implementation, 50–90 partial implementation and a score above 90, full implementation.
In the third stage, we conducted our statistical analysis to benchmark the overall level of WCAG compliance in the Indian private healthcare sector, as well as to investigate the patterns in the data based on hospital characteristics. On the basis of Bai et al.’s (2021) adaptation of the Berry model, we investigate the importance of hospital size (number of doctors and number of departments), orientation (specialized versus general and age in years), regional diffusion (Metro4 and Metro10) and site complexity (number of URLs) as predictors of web accessibility standards compliance, as measured by the FAE 2.0 online evaluation tool.
RESULTS
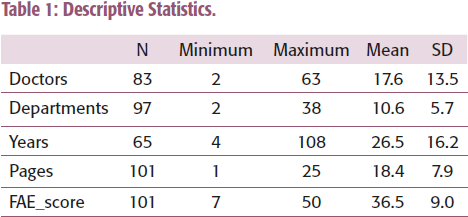
Descriptive statistics for the continuous (non-dummy) variables in our model are presented in Table 1. Not all websites provided lists of doctors or medical departments, or the year of founding. Accounting for these missing values, the number of observations (N) on each variable was different, as noted in the first column of Table 1. The SHCOs varied considerably by number of doctors (2–63), departments (2–38), age (3–108 years) and size of website (1–25 pages). The FAE scores averaged 36.5, with only one website reaching 50. Only a single website in our sample of 101 SHCOs implemented the WCAG standard. Though disappointing, this is hardly surprising since it conforms to the record of poor web accessibility found in the literature, in different sectors and countries.
Descriptive Statistics.
Next, we examine whether the location or type of SHCO (general versus specialized) made any difference to the size of the hospitals, their duration since establishment, the complexity of their websites and web accessibility standards (Table 2). In other words, we examine if hospitals in the largest cities differed from those in smaller cities, or if general hospitals differed from those that offering specialized services.
Comparison of Means by Location and Nature of Hospital.
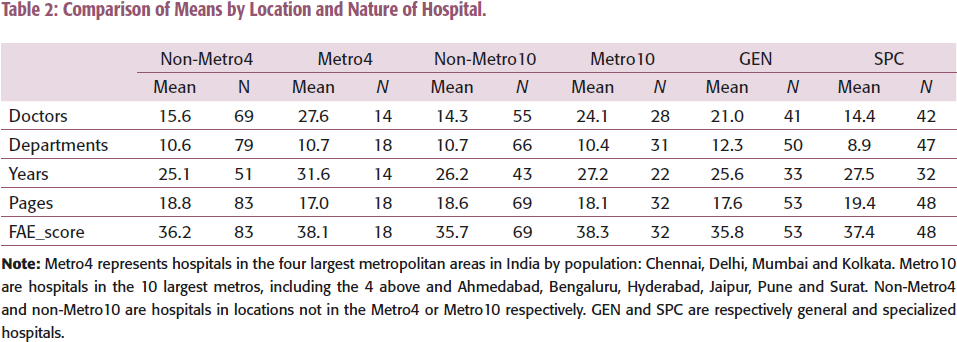
Metro4 hospitals had significantly more doctors than those in non-Metro4 areas (27.6/15.6) (F = 10.11, p = .002); a similar difference was noticed between Metro 10 and non-Metro10 hospitals as well (24.1/14.3) (F = 10.88, p = .001). As may be expected, the 48 specialized hospitals in our sample had significantly fewer doctors (14.4/21.0) (F = 5.17, p = .026) and fewer departments (8.9/12.3) (F = 9.05, p = .003). However, specialized hospitals are better staffed in the departments that they do offer, with slightly more doctors per department (1.99/1.79), though the difference is not significant.
The FAE score did not show much variation by the location of the hospital (Metro4 and Metro10) or specialization. Though the web accessibility scores were higher in the Metro4 (38.1/36.2), Metro10 (38.3/35.7) and in specialized hospitals (37.4/35.8), the differences were not large enough to be significant. Combined with the finding that WCAG scores were in the 7–50 range, with an average of 36.5 (see Table 1), we may conclude that accessibility standards were uniformly poor on Indian hospital websites.
Regression Analysis
An OLS regression of the dependent variable FAE score was run against the continuous and dummy variables in our dataset. Following Bai et al. (2021) who argued that the effect of size complexity on accessibility may be nonlinear, we added in ‘pages_sq’ (pages*pages) as a predictor. The results are reported in Table 3.
Regression Analysis (DV= FAE Score).
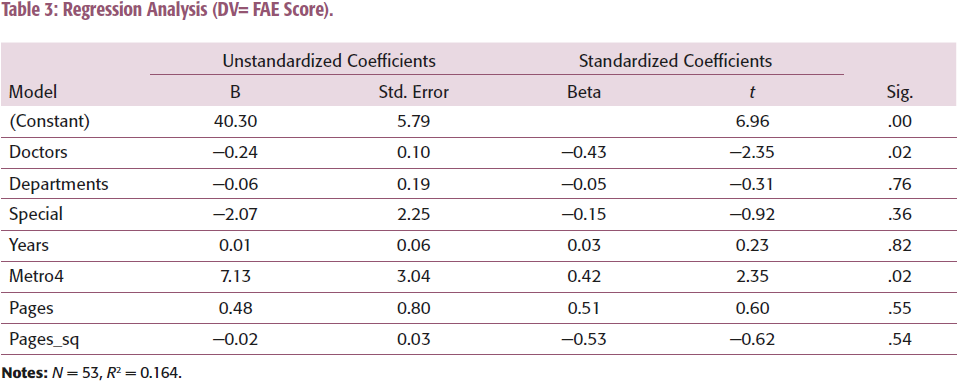
Contrary to expectations, the effect of SHCO size (as measured by the number of doctors and departments) is negative; theory suggests that organizations with greater financial resources are more likely to implement organizational innovations. However, it may be noted that the number of doctors and departments was used as a proxy for financial resources, since financial information on budgets, revenues and profitability is unavailable for the private SHCOs. The number of doctors and departments may not be good proxies for financial resources, or on the contrary, they may be indicators of personnel expenditures and therefore negative predictors of profitability. In the absence of financial data, this explanation remains speculative.
An alternative explanation for this unexpected result may be the correlation between the size of SHCOs and their location; as shown in Table 2, the number of doctors in Metro4 SHCOs is significantly more than in non-metros. To test whether this was the case, a point biserial correlation was run between Metro4 and the number of doctors (Rpb = 0.33, p = .002). Though significant, this correlation does not reach the threshold where multicollinearity is a concern. Since there is a theoretical justification for including both ‘doctors’ (a measure of agency resources) and ‘Metro4’ (a measure of regional diffusion) in the model (Bai et al., 2021; Berry, 1994), we retain both variables in the model.
Metrics for agency orientation (type of SHCO and years since founding) were not significant predictors of web accessibility implementation. There was no difference between general and specialized SHCOs, nor between older and younger SHCOs in terms of web accessibility. However, strong regional diffusion effects were observed. The Metro4 variable significantly increased web accessibility standards compliance.
Finally, site complexity (as measured by the number of URLs on the SHCO website) was not a significant predictor. As stated earlier, the model reported in Table 3 includes ‘pages-sq’ as a predictor to accommodate possible nonlinear effects on accessibility compliance. Neither ‘pages’ nor ‘pages_sq’ was significant. An alternative model with only linear effects (including only ‘pages’) was also run and showed no significant effect of site complexity. It is not reported in the interest of space.
In our analysis of SHCO websites, we also reviewed the mission and vision statements of hospitals to code for those that mentioned ‘disability’ or ‘wellness’. SHCOs that explicitly mentioned disability as part of their mission would be more likely to implement web accessibility standards. However, only one of the 101 websites surveyed mentioned disability in their mission statement. Similarly, we expected mentions of ‘wellness’ to indicate hospitals’ greater sensitivity to the well-being of their patients and their families. Again, only one website mentioned ‘wellness’ as part of the hospital’s mission. Since not enough observations were available for group-wise comparisons, these variables were not used in the regression analysis.
DISCUSSION
Our analysis confirmed the finding from the literature that web accessibility standards continue to be poorly implemented in different countries and economic sectors. The FAE scores averaged 36.5 in our sample of 101 SHCOs, with only one website reaching 50. In other words, the vast majority of our sample websites failed to implement the WCAG 2.0 standard, with less than 1% partially implementing the standard, highlighting the urgent need for improvement in accessibility in Indian healthcare.
Of the variables we tested as predictors of web accessibility compliance, only location was a significant predictor in the direction expected from theory: the location of SHCOs in the major metropolises was associated with significantly higher FAE scores. Location in our model was a proxy for regional diffusion effects, whereby adopting units learn from the example of others in their peer groups or to compete with others in the same market. However, we would be overstating the results if we attribute all location effects to peer learning. Urban areas have higher literacy (including digital literacy) and better computer and broadband access. Urban areas may also have a higher awareness of disability and greater sensitization to the rights of persons with disabilities. Thus, demand from consumers may be a factor encouraging urban hospitals to make their websites more accessible. Indeed, factors such as education, digital skills, percentage of individuals with disabilities in the local population and broadband access were included as predictors of the accessibility of local government websites by Bai et al. (2021). However, lack of information on the specific markets and neighbourhoods served by urban hospitals (and therefore of their demographics) makes it impossible to include these variables in our regression models.
Greater awareness of web accessibility and sensitivity to customer service in urban areas may also be some of the factors of awareness; indeed, several scholars have recommended training and awareness building for webmasters and administrators as a means of improving accessibility (Alajarmeh, 2022; Kuzma et al., 2017; Yi, 2020). Our findings suggest that awareness-building campaigns centred on industry associations and other trade bodies, and the demonstration effect of publicizing exemplars from the industry may help improve web accessibility in the healthcare sector. Policy mandates may also be useful. As we saw in the sections on health policy and regulations, there is no explicit requirement to implement web accessibility standards in the legal and policy documents on disability. This is a major oversight that future policy initiatives need to address.
Additionally, the market model of disability highlights customers with disability as an important segment (Saxena & Saxena, 2015). However, organizations, especially small ones with limited resources, are unlikely to address this segment due to a perception that such efforts would require large investments (Saxena & Saxena, 2015). In such a context, this study shows that making websites of small healthcare organizations accessible to people with disabilities requires awareness training of web designers, which may be considered a small investment considering the social and economic value such a move is likely to create. The findings of this study highlight an opportunity for small healthcare organizations to become socially responsible businesses.
Our study has several limitations. To investigate a heretofore unexplored segment of the Indian healthcare sector, we focused only on small private hospitals and nursing homes. The findings are therefore generalizable only to our population: small, accredited, private hospitals and nursing homes in India. We also acknowledge that accreditation is a relatively new practice in India, and accredited providers may be untypical of the enterprises in the sector. Future research may aim to replicate our methods for larger private hospitals, government-owned healthcare facilities and public health centres.
Second, our analysis was limited by the availability of data. Our sampling strategy, utilizing NABH-accredited SHCOs as our sampling frame, limited the size of our sample once observations with missing data were deleted. Though several of our variables had coefficients in the direction expected by theory, they lacked significance due to the small sample size. Future research may seek to identify alternative sampling frames to increase the power of the analysis.
Finally, we used only a limited set of variables in our model due to data availability. For example, we used proxies to measure for financial resources since revenue and profitability data are unavailable for the small private hospitals in our sample. Similarly, market characteristics such as broadband penetration and the number of Internet users in the service area of hospitals may predict traffic to hospital websites, leading to greater demands for accessibility. Similarly, a higher percentage of persons with disabilities in the service areas of hospitals can create pressure for web accessibility. It may be recalled that the urban location was one of the significant predictors of accessibility scores in the regression analysis. Though we consider regional diffusion effects—reinforced through peer learning—to be an important reason for the higher web accessibility standards in urban areas, it would be overstating our results to attribute all the observed differences to peer learning alone. The demographics of urban markets, including higher education, digital literacy, computer and broadband access, and awareness of disability rights would also be significant predictors. However, lack of information on the precise markets served by hospitals made it impossible to include these factors into this article. Future research may explore creative means of incorporating market or service area characteristics into models of web accessibility.
CONCLUSIONS AND POLICY RECOMMENDATIONS
This article sought to study the adoption of web accessibility standards in India as an example of voluntary technology adoption by firms in the absence of a regulatory mandate or policy directive from government. By focusing on a single innovation within the same economic sector (healthcare), we aimed to isolate the firm-specific factors that influence the adoption decision, without the influence of innovation attributes and environmental factors. The Public Management Innovation model (Berry, 1994) that focuses mostly on firm-specific factors was chosen as our theoretical framework for the same reason.
Compliance with web accessibility standards was uniformly poor in the Indian SHCO sector, irrespective of the size, financial resources or type of healthcare institution. Though SHCOs located in the largest metros had better compliance as a group, they too fell short of the standard. This finding raises important policy recommendations for government health agencies, healthcare accreditation organizations, as well as hospital managers and administrators. For government agencies, lack of web accessibility standards among small hospitals and healthcare clinics—which are often the primary care providers for large segments of the rural and urban poor populations—suggests the need to create regulatory or legislative mandates for accessible websites. Health accreditation organizations such as the NABH may also make the accessibility of websites a criterion in their accreditation reviews.
The recommendations for hospital managers and healthcare administrators are also no less clear. Accessible websites can play an important role in improving patient care, responsiveness and communications, leading to better customer satisfaction and outcomes. Web accessibility should also be an important element of hospitals’ cost management strategy—the lack of web accessibility that we found in our analysis should therefore be seen as an indicator of the unrealized potential of telemedicine and e-health delivery initiatives. Awareness-building campaigns through industry associations and trade bodies—for example, by highlighting the advantages of hospitals that have successfully implemented web accessibility standards—can also create wider adoption of accessible websites. There is an urgent need to improve web accessibility standards to ensure that the most disadvantaged patient groups, such as the elderly and persons with disability, have access to healthcare information and services.
Footnotes
ACKNOWLEDGEMENT
We thank Apratim Bhattacharya, a doctoral student at Visva-Bharati University, Shantiniketan, West Bengal, who worked as a research assistant on this project.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship and/or publication of this article.
NOTE
E-mail:
E-mail: