
Abstract
As per the India Brand Equity Foundation, by 2022, India’s healthcare market is expected to reach US$372 billion. While exponential growth in the availability of private hospitals has been recorded in the past few years, many hospitals are not able to attract enough patients due to poor quality of services, unavailability of skilled healthcare workers, and unethical medical practices. These issues were painfully exposed during the COVID-19 pandemic. Patients rely on recommendations from friends and relatives to select a physician or hospital. This study undertakes a customer-oriented view of patients to explore patients’ perceptions of physicians’ communication and how it influences the recommendation of a physician. For the study, data are collected from 626 patients spread across three cities of North India. We find that physician communication leads to favourable recommendations, and the patient’s perceived influence and satisfaction play an important role in this process. The physician should display empathy and compassion while communicating to patients, which helps build a favourable perception of the physician. This leads to a higher level of satisfaction with the healthcare provider. Furthermore, the study also examines the effects of socio-demographic variables, such as patient’s income, patient’s gender, and physician’s gender. People with high (vs low) income are more satisfied with physician communication, whereas people with low (vs high) income are more likely to recommend a physician. Interestingly, female patients are more satisfied with a physician’s communication skills than males. Aligned with the patriarchal society, patients show more acceptance of male (vs female) doctors, but in contrast, patients are more likely to recommend a female (vs male) doctor. So, we recommend that healthcare providers ensure that patients get sufficient time to spend with their physicians to discuss problems and not ‘rush’ the patients to improve revenues.
Keywords
INTRODUCTION
As per the India Brand Equity Foundation, by 2022, India’s healthcare market is expected to reach US$372 billion. Exponential growth has been recorded in the availability of private hospitals in the past few years. However, many hospitals are unable to attract enough patients due to poor quality of services, unavailability of skilled healthcare workers, and unethical medical practices (Kaul, 2019). Furthermore, peoples’ decision to visit a physician is based on the perceived reputation of the physician or hospital, the criticality of the need, and favourable references from known contacts (Gordon et al., 2015).
The importance of recommendations for products and services is well documented in the research (Berger, 2014, 2016). In the product context, most consumers make purchase decisions based on word-of-mouth (WOM) recommendations from their friends, relatives, or colleagues (Leisen & Hyman, 2004; Mishra & Satish, 2016). A positive WOM can increase revenues, whereas a negative WOM can severely affect the reputation and sales of products/services (Mishra & Satish, 2016). Hence, favourable recommendations for a product or service are imperative and critical to the success of any business.
The extant research broadly classifies typical WOM behaviour into two possible categories: consumer-specific and product-specific (Mishra & Satish, 2016). Examples of consumer-specific motivations are altruism, collectivism, and satisfaction, whereas product-specific motives are quality, price, and novelty. For services, consumers may recommend a service provider if they are satisfied with the overall service experience (Martin et al., 2019). While we noticed a vast amount of research on WOM is available for products and services, such as tourism, hospitality, and travel, research in healthcare services is limited due to its unique characteristics, such as information asymmetry, confidentiality rules, and the extremely critical nature of the services (Berry & Bendapudi, 2007; Martin, 2017b).
Healthcare services are expensive and have a critical impact on individuals, with many complexities involved in the treatment process. The success of any treatment depends on factors specific to individuals, such as age, medical history, and physical condition (Martin et al., 2019). Therefore, the duration and outcome of treatment may significantly differ for patients undergoing treatment with the same doctor, which impacts patients’ satisfaction and likelihood to recommend a physician (Burroughs et al., 1999).
A critical difference in WOM behaviour in the healthcare sector is the role of communication and the perceived influence of physicians (Martin, 2017b). Patients prefer physicians with whom they have had a positive experience or who are recommended by friends and relatives (Lockie et al., 2015). Moreover, a physician’s communication style and attention towards patients’ symptoms are critical to enhance the service experience. There are certain favourable factors, such as physician’s communication, expertise, clinical competence, and process quality, which are under the control of service providers and result in further recommendations (Martin, 2017a). However, the mechanism of how a physician’s communication leads to recommendations is not a well-explored area in healthcare research. For example, a physician uses affective communication and prescribes proper medicines to patients. However, for some reasons (e.g., cost of medications or the waiting time at the clinic), a patient may not be satisfied with the physician and hence does not recommend the physician to others. Some of these cases result in a negative outcome, such as medical violence, malpractice litigation, performance payouts, health outcomes, and treatment compliance (Argan, 2016).
Patients are more likely to recommend a physician with reputed credentials and clinical expertise (Lockie et al., 2015). From a consumer-oriented perspective, the impact of patients’ evaluation of a physician’s technical expertise on satisfaction is another research gap. Recent research has looked at the role of a patient’s gender in the process of recommendation (Martin et al., 2019), yet the effect of a physician’s gender is not well established in the research. Furthermore, India is considered a male-dominant society where people have strong gender stereotypes for many professions. Therefore, we believe that it would be interesting to explore the effects of the gender of physicians and patients in patient–physician interactions. Moreover, we also examine the influence of a patient’s income, since affluent consumers generally have higher expectations from a service provider (Sharma & Narang, 2011). Therefore, this study has the following research objectives:
To understand how a physician’s communication impacts recommendations of her/him and the mediating role of perceived influence and patient’s satisfaction in this process. To examine the influence of gender and income in the above process.
To address the research gaps and meet the stated objectives, this study uses the social interaction model of health communication as the theoretical foundation to examine patients’ perceptions of physician’s communication in outpatient clinics and their recommendation behaviour. The research contributes to the literature on WOM recommendations in the context of healthcare services. It attempts to answer the call for research by Martin et al. (2019) about investigating antecedents to physicians’ recommendations by patients. The results reveal that a physician’s communication is imperative for patients’ satisfaction. Perceived influence of physician’s expertise and patient’s satisfaction are the intervening variables that influence physician recommendations. Moreover, the income and gender of a patient significantly influence her/his satisfaction and recommendations of a physician.
LITERATURE REVIEW AND HYPOTHESIS FORMULATION
The social interaction theory (Turner, 1988) has been widely used to explain physician–patient communications. The physician–patient interaction is a face-to-face communication where patients build an impression of the physician based on the communication style and expertise demonstrated by the physician (Lockie et al., 2015). The interactions differ from other professional client interactions due to the presence of emotion or affective dimension of communication (Ben-Sira, 1976; Martin, 2017a, 2017b).
Earlier research suggested that patients took cognizance of a physician’s communication skills only when he/she was unhappy with the treatment and the physician’s expertise (Ben-Sira, 1976). These findings attracted criticism, because they suggested that under normal circumstances, a physician’s communication skills ranked lower than her/his expertise and the treatment offered at the clinic. Later studies, for example, Buller and Buller (1987), concluded that communication skills were more important, since patients spent more time conversing with a physician than on the actual treatment.
Furthermore, the social influence theory and persuasion psychology suggest that individuals get influenced by the positional authority of the person and are more likely to propagate information under the perceived influence (Berger, 2016). Therefore, based on these theories, we present our conceptual model in Figure 1.
Physician Communication and Recommendations
Described as a multifaceted social behaviour, clinical communication between a patient and a physician is at the core of patient-centred care (Baker & Watson, 2015). Clinical communication is considered similar to a therapeutic relationship, as it involves communicative acts, such as active listening, address of patient’s concerns, and frequent, jargon-free information updates (Roter & Hall, 2006). The other dimensions of communication include psychosocial behaviour promoting social interactions, small talks, and informal conversations, which positively influence patients’ well-being (Stewart, 2001).
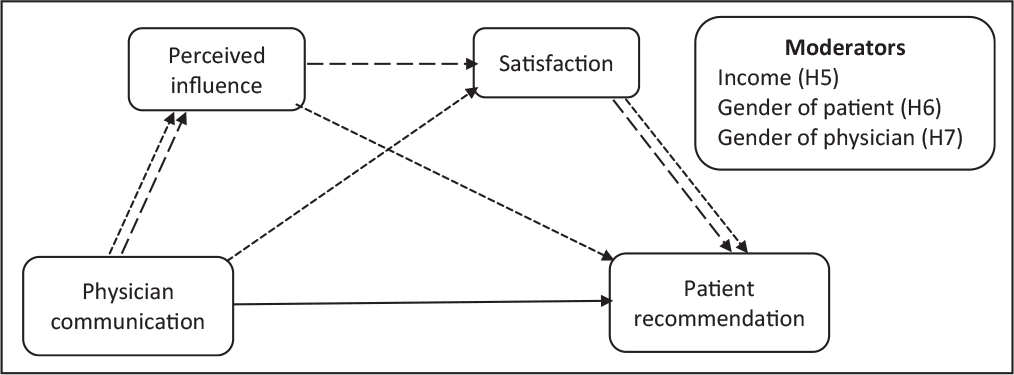
Notes: The solid line represents the direct effect (H1).
Kim et al. (2004) differentiated between cognitive empathy and affective empathy and concluded that patients were influenced much more by the latter than by the former. Their study described the importance of the listening and emotional responses of physicians towards their patients and concluded that patient distress was negatively correlated with physician attentiveness and empathy. This is similar to the classification by Roter and Hall (2006), who identified two types of communication behaviours: instrumental (cure or task-focused) and affective (care or socio-emotional). Instrumental utterances include medical directives, such as giving and receiving information, making decisions, soliciting questions, advising, and prescribing. In contrast, affective utterances are related to empathetic communication, counselling, show of kindness, active listening, proper eye contact, and a smiling expression. Patients are more likely to trust and commit to physicians who adopt an empowering communication style (Wright et al., 2006).
Healthcare services are classified as credence services, because it is difficult for a consumer to evaluate service quality. The duo of patient and physician participate in a co-creation process, as inputs from both parties are critical to the final satisfaction outcomes (Sahi et al., 2017). In many developing countries, patients lack access to accurate and complete information on healthcare services. The preferred channels of communication with friends and relatives form the basis of selecting a physician or a hospital (Cheng et al., 2003). Therefore, WOM recommendations are vital for the success of any healthcare service provider (Martin et al., 2019).
The extant research provides mixed results on the relationship between physician communication and patients’ recommendation of a physician. For example, the likelihood of recommendation depends on many factors, such as mutual respect towards each other, atmospherics, and understandable instructions from physicians (Boudreaux et al., 2000). On the other hand, Cheng et al. (2003) suggested that communication skills could predict patients’ advocacy for certain types of disease categories. Moreover, each patient’s experience is distinct from others’, and hence the technical aspects of care are more important than interpersonal skills in determining patient recommendation of a hospital (Cheng et al., 2003). However, recent research favours the argument that imparting communication skills training to physicians significantly improves patients’ satisfaction with overall care and willingness to recommend a physician (Haskard & Summer, 2008; Martin et al., 2019; Wright et al., 2006). Hence, we propose the following hypothesis.
Mediating Role of Perceived Influence
The effectiveness of physicians’ communication depends on how patients perceive and evaluate it (Baker & Watson, 2015). As in any typical service delivery, consumers rate their satisfaction on many dimensions, such as time taken in delivery, service quality, previous service encounters, and quality of interactions with service providers (Danaher & Gallan, 2016). Past studies have concluded that excellent provider–patient communication is essential for patient’s confidence, compliance, and recall (Wright et al., 2006). However, patients and physicians differ in quality perceptions of their interactions (Leisen & Hyman, 2004). While physicians give much importance to shared decision-making, choice of language, and efficacy, patients prioritize explanations of outcomes, flexibility, and continuity (Martin, 2017b). Research in persuasion psychology suggests that authority and likeability are two critical factors that influence people and create a favourable image for information propagation (Cialdini, 1987). Thus, physicians can use affective communication to signal their empathy and technical expertise to cement their authority and expertise.
Patients discover a new set of medical terminology when they interact with their physicians. They are more likely to use these technical terms to signal their knowledge of the medical problem with authority while talking to friends or relatives (Heisler et al., 2002). In fact, sometimes they may imitate a physician’s language to convey their expertise and advise others having similar symptoms. This behaviour is consistent with the theories of social influence and WOM behaviour, where people share information due to imitation or altruism (Berger, 2014, 2016). Therefore, a physician’s communication influences perceived influence, which in turn impacts patients’ recommendation of the physician. Thus, we hypothesize the following.
Mediating Role of Patients’ Satisfaction
A physician’s communication style can impact a patient’s satisfaction with the physician (Smajdor et al., 2011). Social interactions and affective communications with physicians lead to greater satisfaction in patients (Buller & Buller, 1987; Wright et al., 2006). Physicians can significantly influence patients’ satisfaction by using simple words, asking questions, and showing empathy in their interactions (Sullivan & Beeman, 2008). Furthermore, patients’ perceptions of their connections and bonding with physicians considerably impact overall satisfaction and health-related concerns (Clever et al., 2008). Patients’ satisfaction reflects a hospital’s service quality (rather than clinical quality) and has a significant positive relationship with the communication behaviour of physicians (Clever et al., 2008). However, given the diversity of patients in terms of their background and expectations, physicians should focus on a personalized rather than a standard communication style (Bosko & Wilson, 2016).
When consumers are satisfied with a product or service, they are more likely to recommend the brand or service provider, which ultimately helps firms generate higher revenues (You et al., 2015). In the healthcare sector, many factors affect the satisfaction of a patient, such as the behaviour of medical assistants, quality of administration, hygiene, and atmospherics (Martin, 2017b). However, the physician’s knowledge and behaviour have the highest impact on patients’ satisfaction (Sharma & Chahal, 1999). For example, a physician may have excellent communication skills and show passion for treating patients, but if a patient is unhappy with the treatment outcome, he/she would not recommend the physician. In fact, an unsatisfied patient may share negative recommendations about a physician. In contrast, satisfied patients are more compliant and loyal to their physicians (Halfon et al., 2004). Generally, loyal consumers are more likely to talk well about products or services (Berger, 2014). Hence, an emphatic and empowering communication from physicians leads to patients’ satisfaction, which further increases the chances of recommendations. Thus, we propose the following.
When a service provider offers satisfactory services, consumers make recommendations via positive WOM (Sahi et al., 2017). In healthcare services, patients feel more satisfied if they make a positive evaluation (perception) of the physician (Baron-Epel et al., 2001). Physicians can make use of affective communications to signal their knowledge and empathy with patients (Bosko & Wilson, 2016) and to create a favourable perceived influence among patients. Under a positive influence, patients may report higher satisfaction levels with services, leading to increased recommendations (Argan, 2016). Therefore, we argue that the effect of a physician’s communication on recommendations by a patient depends on the perceived influence and the patient’s satisfaction with the service. Thus, we propose a serial mediation hypothesis.
Moderating Role of Income, Gender of Patient, and Gender of Physician
People with a high income have access to high-value services, which they frequently experience (e.g., tourism and personal care). Such consumers may expect similar levels of service quality in healthcare services. Based on the expectation confirmation theory, people with a high income expect high levels of service quality and display different levels of satisfaction than people with a low income (Sharma & Narang, 2011). Moreover, people with a high income (vs low income) are more inconsistent in their evaluation of service quality and expectations (Gagliano & Hathcote, 1994). We expect a similar effect of income in the context of healthcare services.
Prior research provides mixed results on how the gender of the patient and the physician impact the patient’s satisfaction and perceived influence. For example, female patients were more satisfied with healthcare units and reported a higher degree of satisfaction with female (vs male) doctors (e.g., Bertakis et al., 1995; Sharma & Chahal, 1999). In contrast, some studies reported no significant differences in patients’ satisfaction based on gender (e.g., Roter & Hall, 2006). In the Indian healthcare system, we need to carefully understand the societal structure that is patriarchal. Interestingly, many women in India study medicine, but few practice (Nagarajan, 2016). Moreover, most female healthcare workers are employed at junior-to-middle levels, and male physicians dominate senior positions in the healthcare profession. We expect female patients to be more susceptible to the perceived influence of a physician and hence more satisfied with the physician’s communication style, leading to higher recommendations. Along similar lines, we expect that patients will perceive male (vs female) physicians as more influential and display higher levels of satisfaction and recommendations. Therefore, we hypothesize the following.
METHODOLOGY
Sample and Procedures
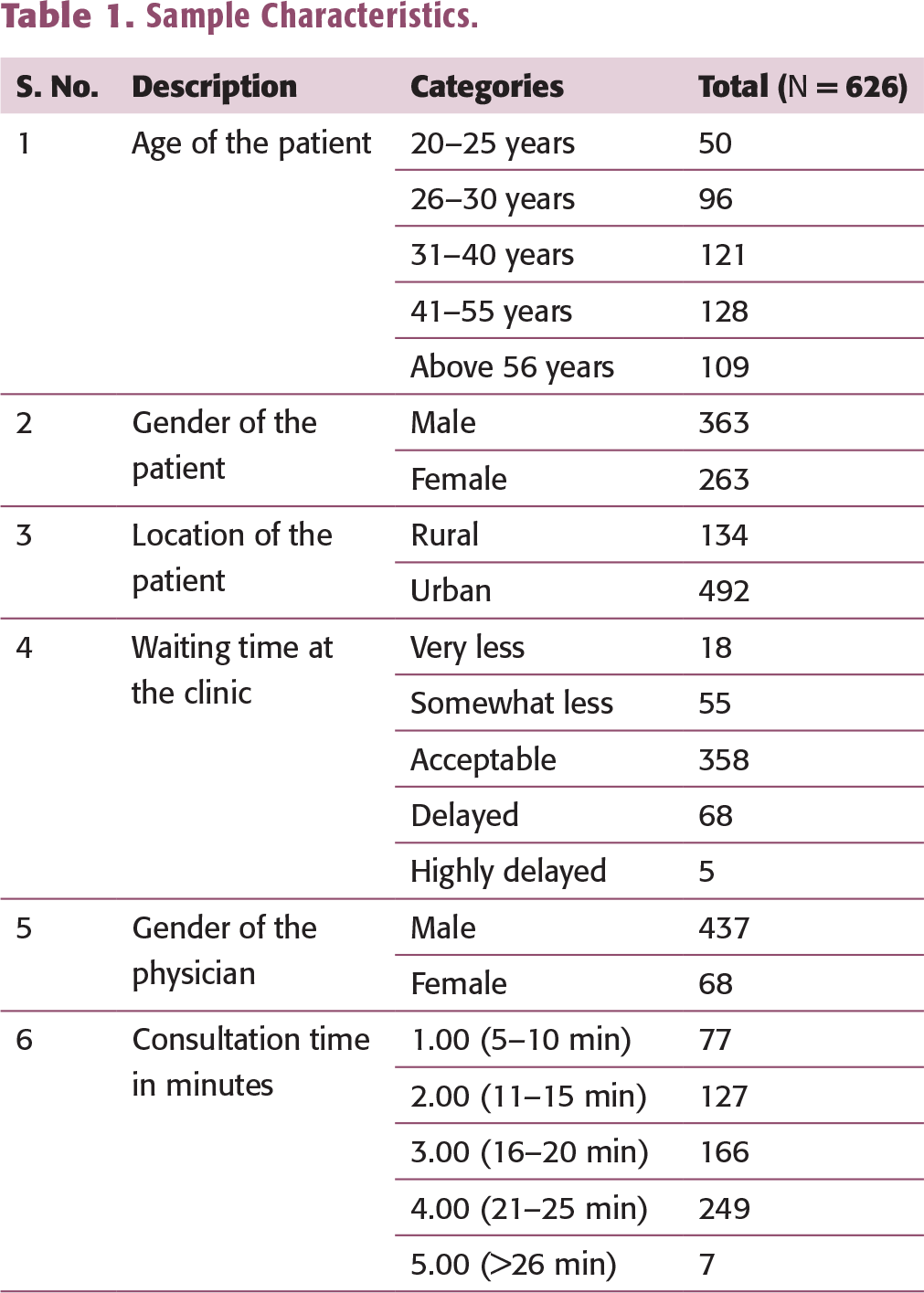
This cross-sectional study (funded by the Institute Seed Money Grant No. 198) was conducted in three major cities of India: Lucknow, Kanpur, and New Delhi. A structured questionnaire was used to collect data from patients who visited private clinics or public hospitals between August 2014 and December 2016. Prior to the data collection, the physician’s permission was taken to interview patients immediately after the consultation. The questionnaire was prepared in the English and Hindi languages to cater to the diverse sample. In the data coding and data cleaning processes, invalid or incomplete responses were removed, such that a total of 626 responses were included in the final analysis (see Table 1 for sample characteristics). Among all the patients, 58% knew the doctor before the visit, and 38% were referred by another doctor. The sample of doctors included general physicians (75.4%) and specialists (24.6%).
Measures
Sample Characteristics.
Control Variables
To ensure the robustness of the results, we included many control variables, such as age, education, employment, nature of the disease, prior knowledge about the physician, and location of the clinic (e.g., Clever et al., 2008; Martin, 2017a; Sharma & Chahal, 1999; Sharma & Narang, 2011).
ANALYSIS AND RESULTS
The data were analysed using the partial least squares (PLS) approach of the structural equation modelling (SEM) method. There were two main reasons for using PLS. First, the research model was predictive, and second, we needed latent scores for serial mediation analysis. The SmartPLS software (version 3.2.8) was used for PLS-SEM analysis (Ringle et al., 2015). First, we tested the measurement model to check for the validity and reliability of the constructs. Then, we tested the structural model to measure path coefficients. This two-step approach is recommended by Hair et al. (2014). The serial mediation model was tested using the PROCESS tool (Hayes, 2013). The moderation analysis was conducted using the PLS multi-group analysis (PLS MGA).
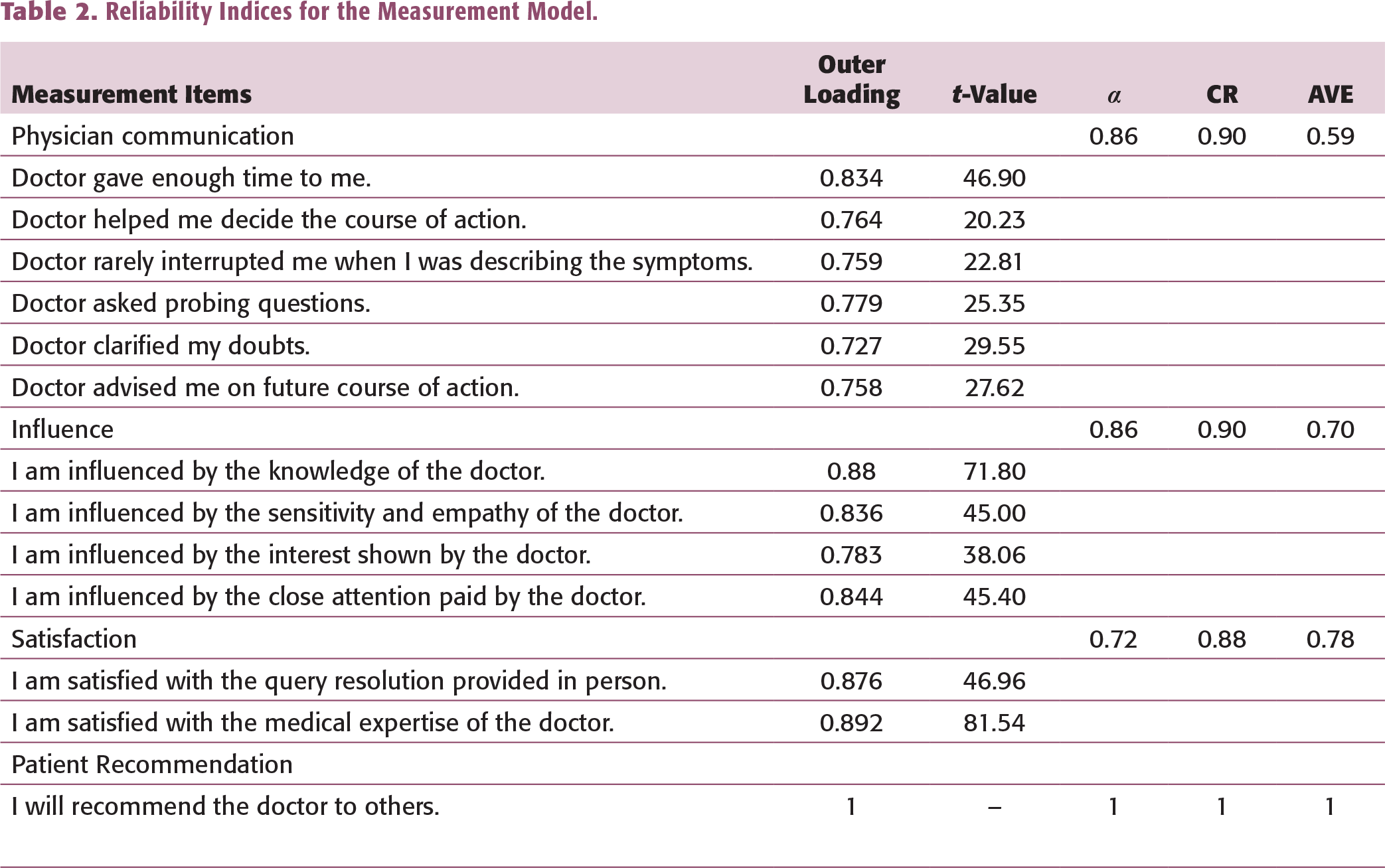
Measurement Model
Reliability Indices for the Measurement Model.
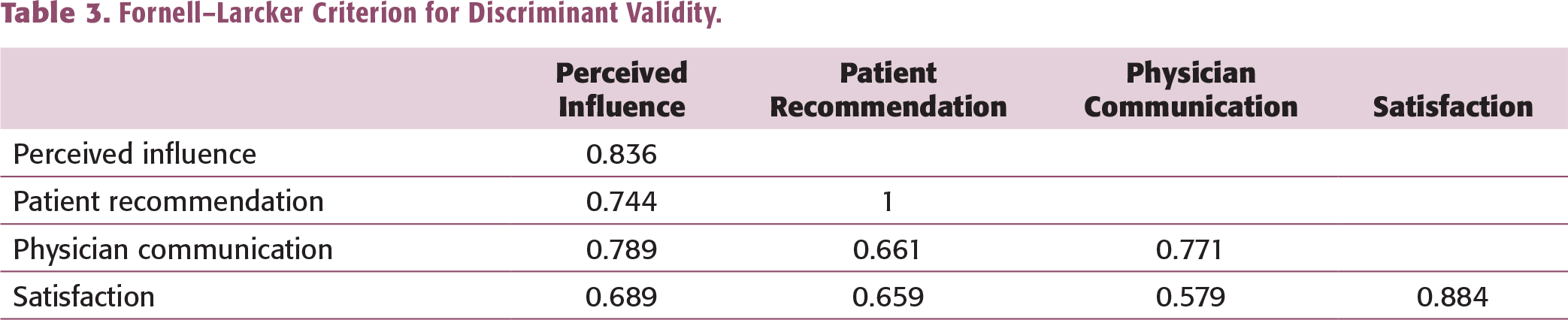
Fornell–Larcker Criterion for Discriminant Validity.
Structural Model
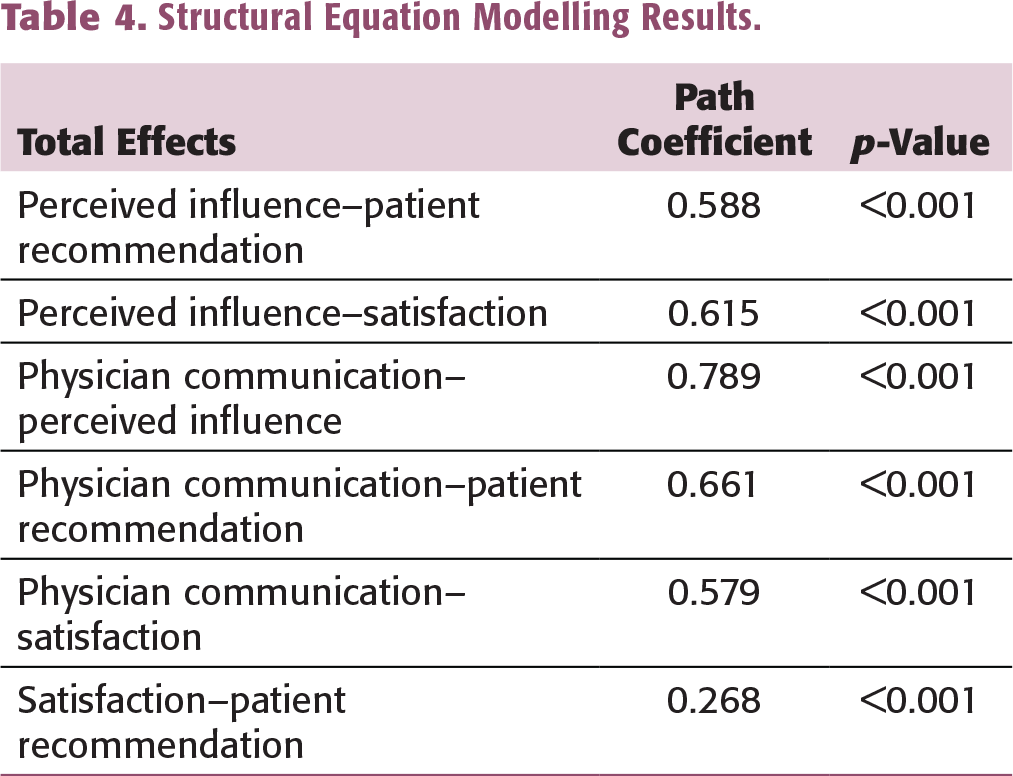
The structural model was estimated using the bias-corrected and accelerated bootstrapping procedure with 5,000 resamples. Multicollinearity was checked using variance inflation factor (VIF) values for each construct, which were lower than the recommended value of 5 (Hair et al., 2014). The R2 values were obtained for the following constructs: influence (0.62), patient’s recommendation of physician (0.60), and patient’s satisfaction (0.48). None of the control variables was significantly related to satisfaction. The model was then tested for its predictive strength using the blindfolding procedure. The resulting positive Q2 values indicated that the model had predictive relevance: influence (0.41), patient’s recommendation (0.58), and satisfaction (0.36). The overall model fit was evaluated using the standardized root mean square residual (SRMR) as an index for model validation (Henseler et al., 2014). The SRMR value was 0.066 with PLS and 0.046 with PLSc. Generally, values below 0.08 are considered favourable (Hu & Bentler, 1999). Hence, the model showed a good fit. The path coefficients (total effects) for all the relationships were significant in the model (Table 4). It was found that a physician’s communication significantly influenced patients’ perception of influence of the physician, satisfaction with the physician, and recommendation of the physician.
Serial Mediation
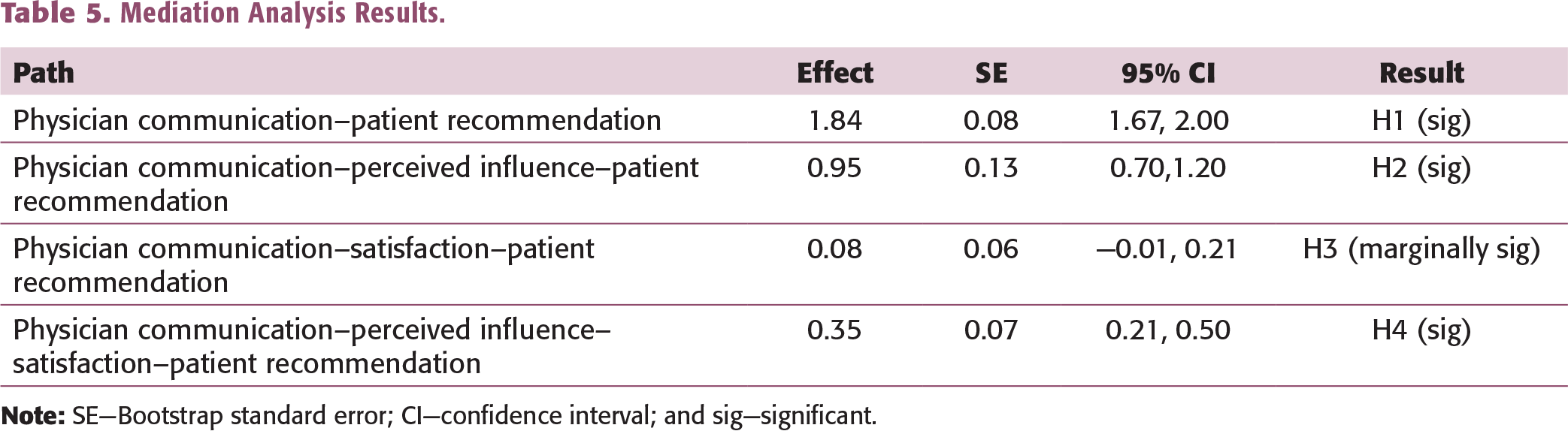
The mediation analysis was conducted using the latent variable scores from the PLS-SEM procedure. Serial mediation was tested in the PROCESS tool (model 6, Hayes, 2013) with 10,000 bootstrap resamples. The absence of 0 in the 95% confidence interval confirmed the significance of the indirect effect/mediation (Table 5). The results show that the mediation via influence (CI = [0.70,1.20]) is significant but it is marginally significant via satisfaction (p < 0.10, CI = [0.001, 0.21]). Moreover, serial mediation via the two mediators for the relationship between physician communication and patient recommendation is significant (CI = [0.21, 0.50]).
Moderation Analysis
Structural Equation Modelling Results.
DISCUSSION AND IMPLICATIONS
The healthcare sector provides many research opportunities to examine the influence of physician–patient interactions on service quality (Berry & Bendapudi, 2007). Drawing from the WOM literature and theories of social interactions, this study examines how a physician’s communication can influence patients’ satisfaction and recommendation of the physician. Our study contributes to the WOM literature, specifically in the healthcare domain, and provides actionable recommendations to healthcare providers and physicians.
Mediation Analysis Results.
Multi-group Analysis for Testing the Moderation Effects.
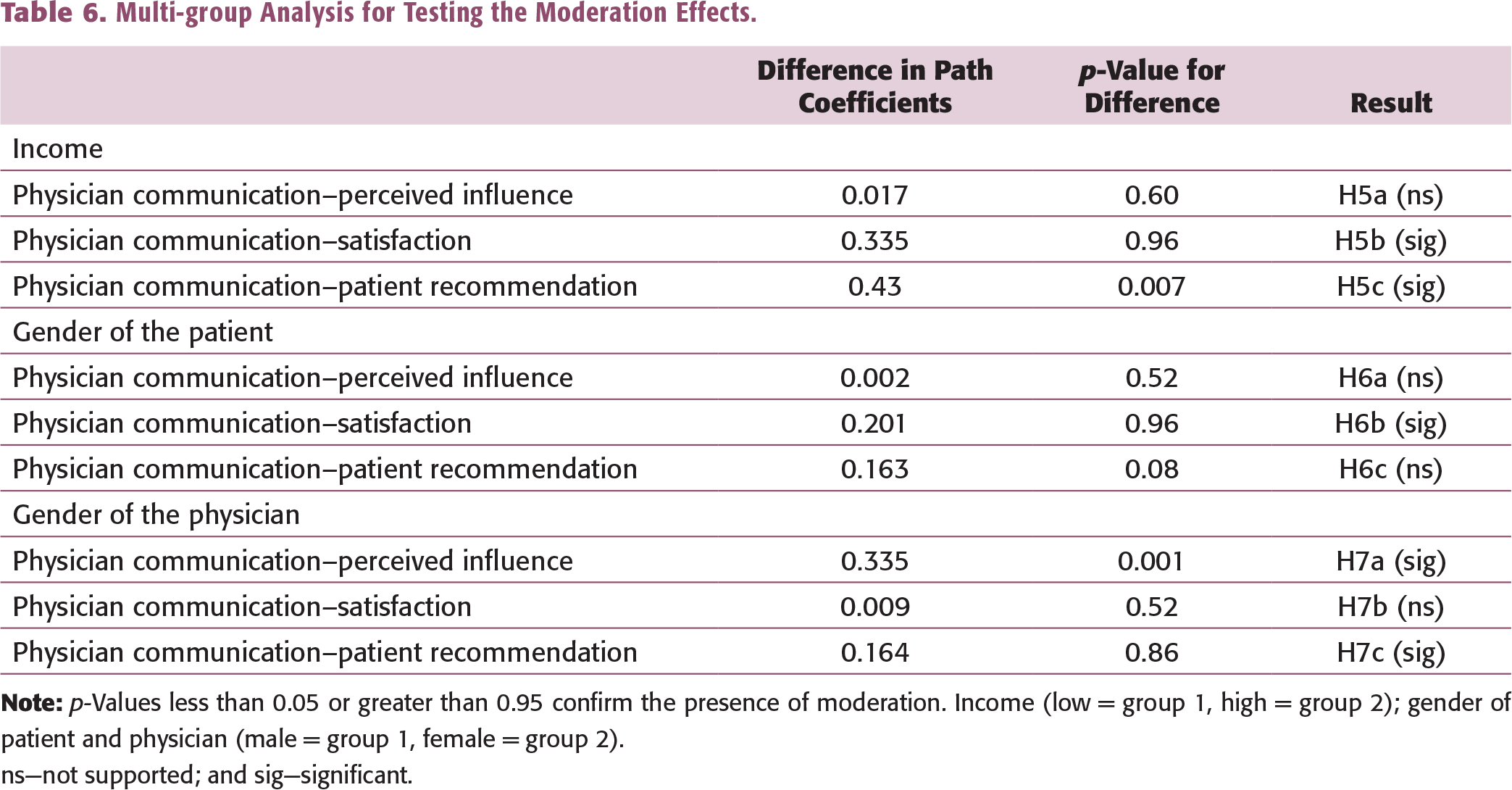
ns—not supported; and sig—significant.
Consumers evaluate a product based on its quality, durability, and value for money. In a healthcare service, a physician’s communication reflects the technical expertise and quality of consultancy. Physicians establish their knowledge supremacy and caring intents via affective and cognitive communication (Martin, 2017b). Our results suggest that the perceived influence mediates the relationship between communication and recommendation. Similarly, affective communication also leads to higher levels of satisfaction. Moreover, perceived influence positively influences satisfaction and has a stronger effect on patients’ recommendations than satisfaction. In fact, perceived influence appears as an antecedent to patients’ satisfaction and a significant link between communication and recommendations. The findings validate the social interaction theory in the context of micro-interactions, confirming the notion that the patient is an active participant in the physician–patient interaction processes (Sahi et al., 2017).
While most of the existing studies have looked at the income of physicians (Martin et al., 2019), we examine how the patient’s income affects satisfaction and recommendations. Interestingly, income shows a different result for the two relationships. People with a high (vs low) income are more satisfied with physicians’ communication, whereas people with a low (vs high) income are more likely to recommend a physician. Healthcare providers can prepare distinct strategies to address the different needs of patients based on their income.
With respect to the gender of the patient, we find that female patients are more satisfied with the physician’s communication than males. We do not find any significant effect of gender on recommendations as reported in prior research (e.g., Martin et al., 2019). A possible explanation could lie in the social structure of India and the position of women in society. Furthermore, patients displayed a stronger perceived influence of male (vs female) doctors, but patients were more likely to recommend a female (vs male) doctor. Thus, we get some interesting results about the impact of the gender of the patient and physician on influence, satisfaction, and recommendations. We think that patients may feel more comfortable with a female physician, who may be more compassionate by nature and therefore receive more recommendations. Thus, healthcare providers must work on including female physicians to get more recommendations.
Finally, we believe that the process of recommendations in the healthcare domain slightly differs from that in the existing literature on WOM in other services. Our results confirm the importance of communication in delivering service quality (Zeithaml et al., 1988) and establish that for a WOM recommendation, the quality of patient–physician communication is crucial, apart from other service-related factors. We recommend that healthcare providers, typically more concerned with the technical side of service delivery, focus on improving patient–physician interactions. There should be a high emphasis on developing face-to-face micro-level interactions (such as a smile or a grimace, nodding while listening and making genuine eye contact).
LIMITATIONS OF THE STUDY AND FUTURE DIRECTIONS
As with any empirical study, this study has certain limitations that can be explored in further research. First, India is a diverse country with many languages. Our study sample was predominantly from North India, and the questionnaire was in Hindi and English. We think that studies from other regions with different native languages can further extend the findings of this study. We did not control for the effect of the image or brand value of the hospital. There are some well-known private hospitals in India whose brand image may influence patients’ perceptions. Moreover, we think that the type of clinic (e.g., private clinic or public hospital) and the specialization of the physician (e.g., general physician or specialist) can influence a patient’s perceptions of and overall experience with the service encounter. Thus, further research can examine these factors.
Healthcare services cover people of all ages and specific diseases. Our study did not focus on gender-specific consultations or symptoms (e.g., pregnancy or delivery), which can be examined in further research. For example, physician–patient interactions may differ significantly for a gynaecologist versus a paediatrician. In such cases, further research can explore how the gender of a patient (or physician) influences satisfaction or recommendations. Finally, the total cost of the treatment (including consultation) can be another topic for a longitudinal study, which may cover the whole process from the patient’s first trip to completion of the treatment.
Annexure 1. Questionnaire
Doctor gave enough time to me.
Doctor helped me to decide the course of action.
Doctor rarely interrupted me when I was describing the symptoms.
Doctor asked probing questions.
Doctor clarified my doubts.
Doctor advised me on future course of action.
I am influenced by the knowledge of the doctor.
I am influenced by the sensitivity and empathy of the doctor.
I am influenced by the interest shown by the doctor.
I am influenced by the close attention paid by the doctor.
I am satisfied with the query resolution provide in person.
I am satisfied with the query resolution provide on phone.
I am satisfied with the medical expertise of the doctor.
I am satisfied with the technical expertise of the doctor.
I will recommend the doctor to the others.
I will talk good about the doctor with others.