
Abstract
Background:
We aimed to study the prevalence of behavioral problems among school-going children, the factors affecting them, and to establish normative scores for the Strengths and Difficulties Questionnaire (SDQ) parent form.
Methods:
A cross-sectional questionnaire-based study was conducted among schoolchildren aged 6–11 years from two primary schools in South India. Parents of children included in the study were asked to fill out the Kannada/English version of the SDQ Parent Form.
Results:
The SDQ parent report forms were filled by parents of 671 children, of which 49.8% (n = 334) were boys with a M: F ratio of 1:1.01. There was an equal distribution across different age groups. The comparison of scores between boys and girls showed no statistically significant difference in all scales except for the hyperactivity subscale, where the boys had a higher score with a median (IQR) of 4 (2,5) compared to the girls’ score of 3 (1,4) (p = .001). Regarding age, although the total difficulties score, conduct problems score, hyperactivity score, and internalizing score were higher in the 9–11-year-old group than in the 6–8-year-old group, the p value was not significant. Children of fathers with higher educational status scored better in the peer problems and prosocial scores. The newer cut-off scores have been generated and are divided into four bands, similar to the 4-band categorization on the SDQ scoring site.
Conclusions:
Boys had higher scores on the hyperactivity subscale than girls. Normative data for Indian children aged 6–11 years have been generated and are similar to UK data.
Boys in the 6–11-year age group have higher scores on the hyperactivity subscale of the SDQ parent form than girls. The SDQ scores for Indian children in this study were comparable to those in the UK.Key Messages:
Children suffering from chronic illness are prone to emotional and behavioral problems. 1 Children admitted for critical illness have often been found to have behavioral issues after discharge. 2 Even an apparently normal child could suffer from some level of psychosocial or behavioral impairment, which is essential to screen, identify, and address for better long-term performance. A significant number of children suffering from behavioral problems go unidentified because of a lack of screening. Early identification and treatment can help develop healthy individuals in the future.
The Strengths and Difficulties Questionnaire (SDQ) 3 is a screening instrument for behavioral problems in children. It comprises 25 items divided into five subscales: emotional problems, hyperactivity, peer problems, conduct problems, and prosocial behavior. The SDQ is available in parent, teacher, and self-report versions3,4 and is used worldwide to assess and screen for childhood behavioral and mental problems. The SDQ is found to have good validity in several studies.4,5
However, country-specific norms are required to provide a meaningful interpretation of this questionnaire that accounts for cultural differences, excludes sociodemographic factors, and takes into consideration the varied influencing factors that differ across countries. Also, age- and gender-specific norms are needed to address an individual’s changing needs and behaviors over time. Such country-specific norms are available for Dutch 6 and Australian children. 7 A study 8 among Indian adolescents showed that the cut-off scores were higher compared to the UK scores for the emotional and peer problems subscales, and the total difficulty score. Due to limited data on Indian children, we are currently using the UK cut-off scores. This might lead to overdiagnosis of emotional or behavioral problems in Indian children. There is a need to have Indian normative values to develop reliable cut-off scores for our pediatric population. This study was carried out to determine normative data for the SDQ parent form in Indian children aged 6–11 years.
Methods
Study Design, Participants, and Procedure
A cross-sectional questionnaire-based study was conducted among schoolchildren aged 6–11 years using convenience sampling from two primary schools in the field practice area of the authors’ institution in South India, over 2 months from August to September 2022. Approval was obtained from the Institutional Ethics Committee before the study was conducted. Children with a history of chronic illness, psychological disorder, or seizure disorder on antiepileptics were excluded. Children were recruited into the study after the principal granted permission to collect data, and each child’s parent provided consent. Demographic data such as age, gender, number of siblings, birth order, and parental educational status were collected in a predesigned pro forma. Parents of children included in the study were asked to fill out the Kannada 9 /English 3 version of the SDQ parent form.
Questionnaire Used
The SDQ parent form 3 has 25 items, with five items in each of the five subscales: emotional problems, conduct problems, hyperactivity, peer problems, and prosocial behavior. Each subscale’s score ranges from 0 to 10. Each item has three responses: Not true, somewhat true, and certainly true, scored as 0, 1, and 2, respectively, except for items 7, 11, 14, 21, and 25, where the score for each of the three responses is 2, 1, and 0, respectively. A high score is abnormal on all subscales except the prosocial subscale, where a low score is considered abnormal. The total difficulty score, which is the sum of all scales except the prosocial subscale, can range from 0 to 40. The internalizing and externalizing scores range from 0 to 20. The externalizing score is calculated by adding the scores of the hyperactivity and conduct problems subscales. In contrast, the internalizing score is calculated by adding the scores of the peer problems and emotional problems subscales. The scores are further classified as “close to average,” “slightly raised,” “high,” or “very high” based on a 4-fold classification derived from a large UK-based sample study.
Scoring was done individually for each subscale first using the standard SDQ scorecard. The total difficulties score and the externalizing and internalizing scores were calculated. Children were categorized into “close to average,” “slightly raised,” “high,” and “very high” based on the final scores. The association of sociodemographic factors with the total score and each subscale score was also studied. Based on the data, we developed cut-off scores for each subscale and the total difficulties score. Values corresponding to the top 5%, 10%, and 20% (bottom for the prosocial subscale) of the percentage bands were evaluated for each subscale and for the total difficulties score in the overall sample. Children who scored in the high/low and very high/very low categories were referred to the psychiatrist for further evaluation.
Sample Size with Proper Justification
Based on a literature review in a previous study conducted by Harikrishnan U, 10 it was found that 7.8% of the children had behavioral problems. In the present research, with a 5% absolute precision and a 95% confidence level, the minimum sample size required for the study was determined to be 264 children.
Statistical Methods
Qualitative variables, such as sociodemographic characteristics and children’s behavioral problems, were described using frequencies and percentages. Quantitative variables, such as age, were described using medians with interquartile ranges, as the data were not normally distributed. The chi-square test was used to compare scores across gender, parental educational status, family type, and age groups. The Mann–Whitney U test was used to compare median values across the various sociodemographic factors. Data were analyzed using SPSS version 20.0, 11 and p < .05 was considered to be statistically significant.
Results
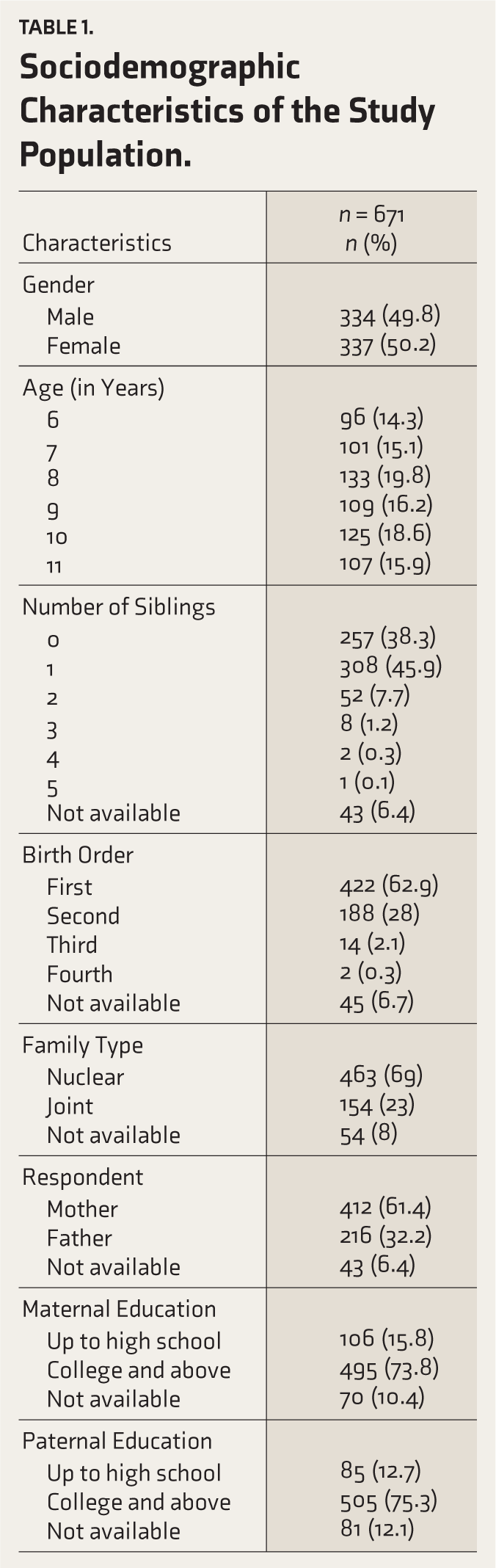
Of the 1046 forms distributed, the SDQ parent report forms 3 were completed by parents of 671 children, of whom 49.8% (n = 334) were boys and 50.2% (n = 337) were girls, with a M: F ratio of 1:1.01. There was an equal distribution across different age groups. The number of siblings ranged from 0 to 5, with the majority (n = 565, 84.2%) having less than two siblings. The birth order ranged from first to fourth, with the majority (n = 422, 62.9%) of the children being firstborn. The nuclear family was the predominant type in the majority of cases (n = 463, 69%). The mother filled most of the forms (n = 412, 61.4%). Seventy-four percent (n = 495) of the mothers and 75% (n = 505) of the fathers had studied beyond graduation (Table 1). The comparison of scores between boys and girls showed no statistically significant difference in any subscales except for the hyperactivity subscale, where the boys had a higher score with a median (IQR) of 4(2,5) compared to the girls’ score of 3(1,4) (p = .001) (Table 2). Regarding age, although the total difficulties score, conduct problems score, hyperactivity score, and internalizing score were higher in the 9–11-year-old group than in the 6–8-year-old group, the p value was not significant (Table 2). The scores of children living in a joint and nuclear family were comparable, with no statistically significant difference in the scores in all of the SDQ subscales.
Sociodemographic Characteristics of the Study Population.
Comparison of SDQ Scores with Respect to Gender and Age.
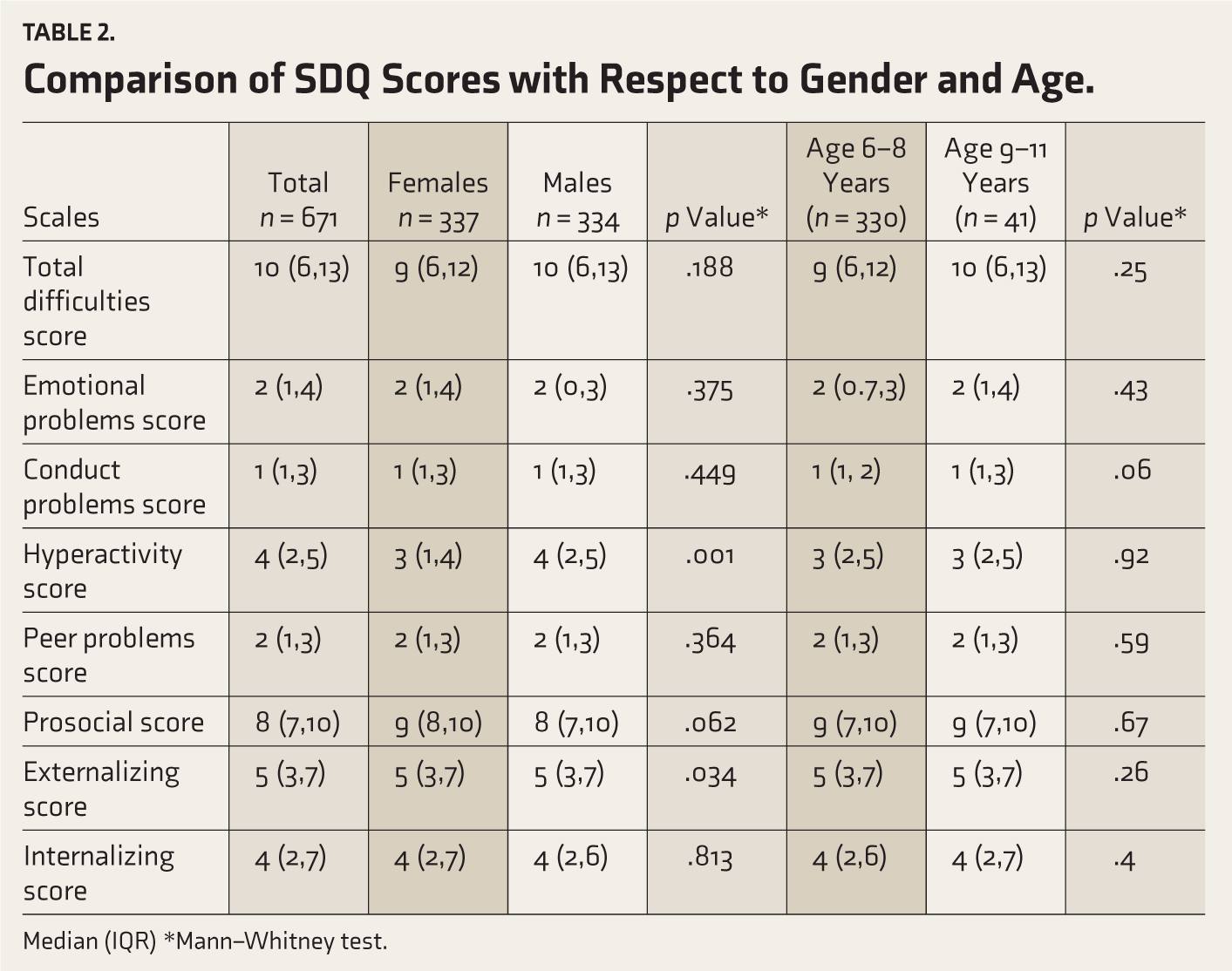
Median (IQR) *Mann–Whitney test.
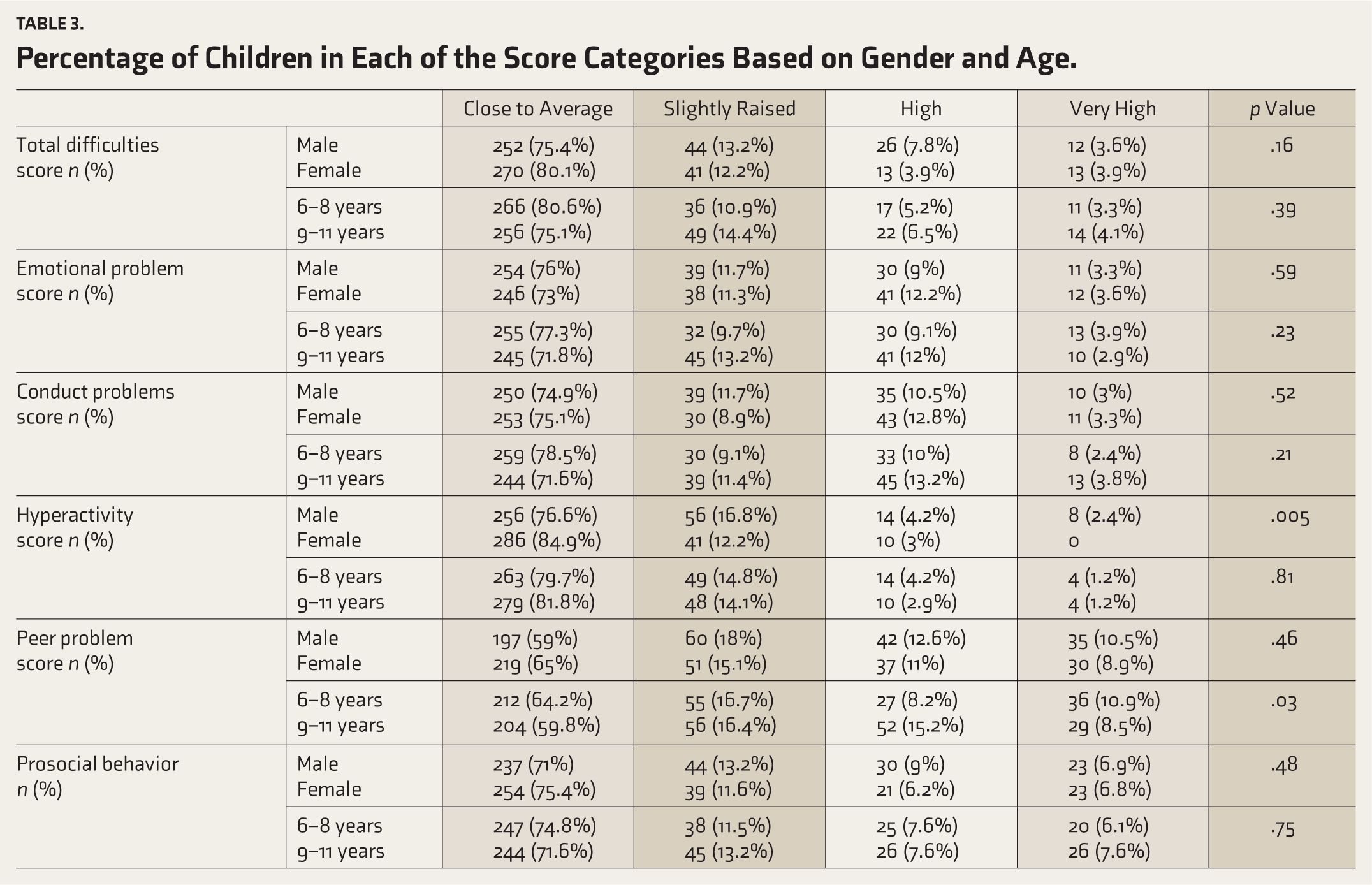
The percentages of children in each score category were calculated and compared. In the total difficulties score and most subscales, the majority were in the “close to average” category, with no significant differences by gender or age. However, on the hyperactivity subscale, there was statistical significance between males and females, with 2.8% (n = 7) of males and 0% (n = 0) and 2.8% (n = 7) of females scoring in the high-risk and high categories, respectively (p = −.005) (Table 3).
Percentage of Children in Each of the Score Categories Based on Gender and Age.
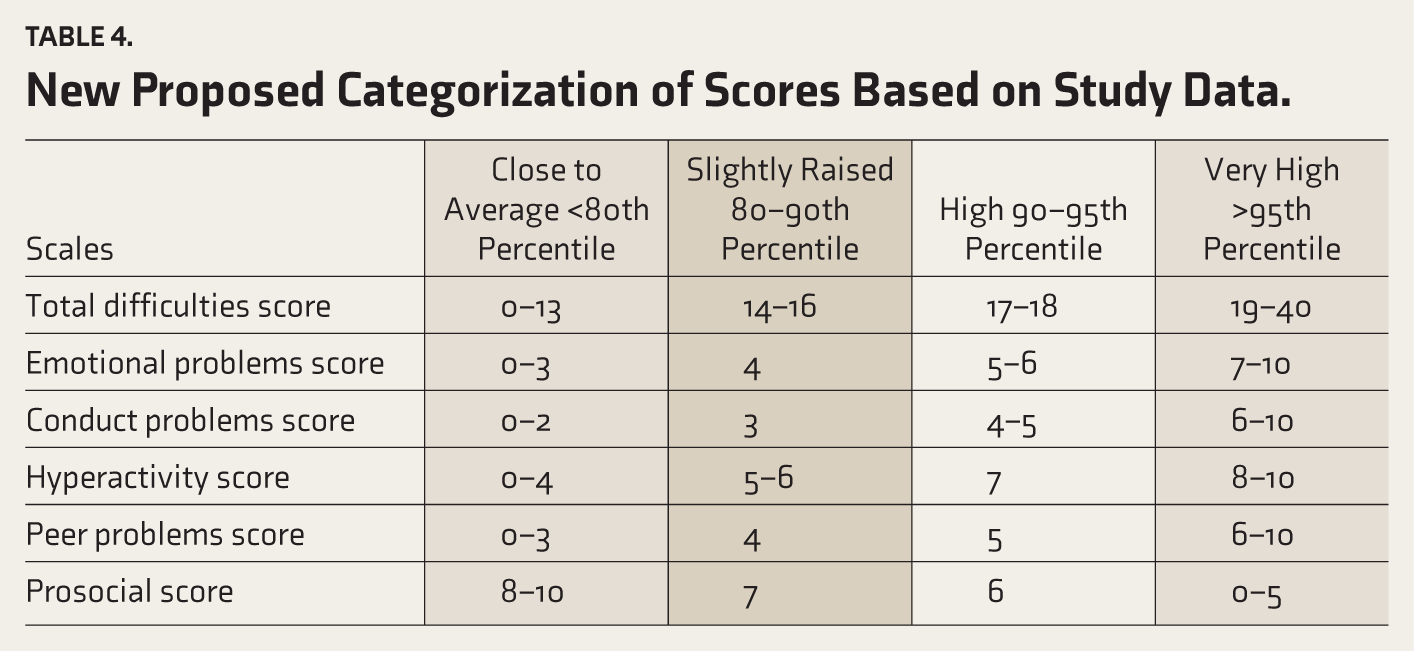
The newer cut-off scores generated from the study data are presented in Table 4. The scores are divided into four bands, similar to the 4-band categorization on the SDQ scoring site. The cut-off scores for “slightly raised,” “high,” and “very high” correspond to the 80th, 90th, and 95th percentiles, respectively, and for the prosocial scale, they correspond to the 5th, 10th, and 20th percentiles, respectively.
New Proposed Categorization of Scores Based on Study Data.
Discussion
The SDQ is a widely used psychometric screening tool, and this study aimed to develop age- and gender-specific norms for the Indian pediatric population, which previously relied on international cut-off scores. As examined in the study by Goodman A et al. 12 and as judged by the development and well-being assessment (DAWBA), the SDQ indicators and disorder rates vary across populations and require careful analysis, underscoring the urgent need to establish normative scores for Indian children. Another study by Goodman R et al. 13 assessed and concluded that the SDQ could be used at the community level for screening and diagnostic purposes to improve access to therapeutic interventions.
This study aimed to examine the prevalence of behavioral problems among school-going children and the factors affecting them, and to establish Indian normative scores for the SDQ parent form for children aged 6–11 years, further subdivided into age groups 6–8 years and 9–11 years. Studies on this questionnaire, like that by Kremer et al., 14 have usually focused on either an even younger age group or adolescents. There was equal representation across all ages and genders in this study. The parent education status in our study was diverse, ranging from illiterate to postgraduate/professional levels, with equal distribution across the sample.
This study found that boys scored higher on the hyperactivity subscale, with a significantly greater number scoring in the “high” and “very high” categories than girls. This finding was similar to the Dutch study, 15 in which boys aged 6–11 years had higher scores on the hyperactivity subscale. However, the study also found that boys scored higher than girls on the peer problems, prosocial behavior, externalizing, and total difficulties scores. This variation across gender was also consistent with previous studies among Dutch children aged 8–16 years, 6 and with findings from other European countries. 16 A study on Indian adolescents by Harikrishna U 10 showed significant gender differences on the emotional problems subscale, with girls scoring higher than boys, indicating a different trend compared to a younger population of children and confirming the need for age- and gender-specific norms in India. This gender difference in behavioral problems was also observed in studies by Pathak et al. 17 and Rimal and Pokharel et al., 18 in which boys had higher scores on the conduct problems subscale.
In comparison, no substantial difference in scores was seen between the younger and the older children in our study. A study by Mellor et al. 7 reported age differences in two of five subscales and the total difficulties scale. At the same time, research by Hawes and Dadds et al. 19 showed a linear increase (and decrease for prosocial behavior) across their sample. Results from an international study 20 focusing on younger children reported age-based differences in the SDQ scales, with lower scores (fewer difficulties) reported for 4-year-olds than for 3-year-old children. The reason could be that, with age, parents become more accustomed to their child’s habits and behaviors.
In this study, higher levels of paternal education were associated with a significantly greater number of children scoring in the “close to average” category on the peer problems subscale and the prosocial behavior subscale. However, neither maternal educational level nor family type had a significant influence on the scoring. The reason for these results could be differences in child-rearing practices or in socioeconomic backgrounds that vary from country to country and are also influenced by how developed the society is.
Based on our study, we generated normative cut-off scores that were similar to the UK scores, with minor variations. As our research did not show significant gen-der or age differences, we did not further classify the scoring by gender or age.
The study’s strength is its large sample size, which is almost evenly distributed across gender and age categories, ensuring adequate representation of the population. Another strong point is that this study is school-based, which eliminates the selection bias seen in hospital-based studies. However, the study has some limitations. It is debatable if the sample size was large enough to establish normative scores. The second limitation is that there is a dearth of multicentric, diverse data to further the accuracy and reliability of the established norms. The third limitation concerns the limited data available from the rural population, preventing comparisons between urban and rural children of the same age group and their prevalence of psychosocial problems. Further multicenter studies from different parts of the country involving the rural population would also help generate scores that are generalizable to the entire population. Also, the stratified random sampling technique was not used in our study, which could have helped minimize sample variance and improve precision across categories such as parent education. Demographic data, such as parental education status, birth order, and number of siblings, were not provided by the respondents for some questionnaires and could have influenced the results. As direct interviews with parents were not conducted and data were collected via questionnaires, this study is not free from bias. Also, children’s academic performance was not included in the study, which could have influenced the results. Another limitation is that although most of the questionnaires were completed by the mothers, a significant number were also completed by the fathers. This may also affect responses since the father’s view of the child might differ from the mother’s view. To determine this, further studies would need to be conducted in which both parents complete separate questionnaires for the same child, and the differences, if any, are compared.
Conclusions
In our study, scores were similar across ages and genders, except that boys showed a higher hyperactivity subscale score. The paternal educational status was associated with children’s peer problems and prosocial behavior. This study also establishes reference values for Indian children aged 6–11 years. The availability of indigenous normative data can help in more accurate screening, interpretation, and early identification of behavioral difficulties in Indian children. However, further multicenter studies across the country, including diverse socioeconomic and regional populations, are needed.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
We would like to acknowledge the parents for participating in the study and the school principals for permitting us to conduct the study.
Data Availability Statement
Deidentified individual participant data will be made available upon publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethics Approval
Ethical approval for the study was obtained from the Ramaiah Medical College Ethics Committee (Approval Ref. No. MSRMC/EC/SP-09/04-2002; dated 4 April 2022). Appropriate permissions were obtained from the concerned authorities.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ICMR STS (2022-08684).
Informed Consent
Written informed consent was obtained from the school principals and parents of the participating students.
Patient Consent
Patient consent has been taken and has been mentioned in the document.
Prior Presentations
None.
PROSPERO/CTRI Registration
Not applicable.
Simultaneous Submission
The manuscript has not been submitted simultaneously to any other journal or publication outlet.
Study Protocol Status
Not applicable.
Trial Registration
Not applicable, as this study was not an interventional trial.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.