
Abstract
Background:
Opioid use disorder (OUD), particularly injection drug use (IDU), is on the rise and is associated with complications such as blood-borne infections, overdosing, and seizures, among others. Understanding factors distinguishing non-injecting opioid users (NIOU) and IDUs is essential for the development of effective prevention and management strategies. This study aimed to compare sociodemographic, clinical, and psychosocial factors between IDUs and NIOUs.
Methods:
A cross-sectional study was conducted at a tertiary care center in North India, including 100 opioid-dependent males (50 NIOUs and 50 IDUs). Sociodemographic, clinical, and psychosocial variables were assessed using structured interviews and validated instruments, including the Maudsley Addiction Profile, the severity of dependence scale (SDS), the high-risk behavior scale (HRBS), the sensation seeking scale (SSS), the Barratt Impulsiveness Scale (BIS), and the WHO-ASSIST.
Results:
IDUs had significantly higher histories of alcohol use, duration of cannabis use, and family history of substance use, and significantly higher scores on HRBS, BIS, and the SSS (p < .05). WHO-ASSIST and SDS scores were comparable between the groups. IDUs had a substantially higher number of days of heroin use in the last month and days of conflicts with relatives (p < .05). Mean duration of the transition period from NIOU to IDU was 4 ± 3.3 years.
Conclusions:
Family history of drug use, higher sensation seeking, impulsivity, and risk-taking behavior were found to be important factors related to IDU. Interventions targeting these factors are essential for preventing the transition from NIOU to IDU.
Question: What are the differences in sociodemographic, clinical, and psychosocial parameters between men who are dependent on injecting versus non-injecting opioids? Findings: Among injection drug users, there was higher sensation seeking, impulsivity, risk-taking behavior, and family history of substance use, compared to non-injection users. Meaning: These factors may be targeted in interventions aiming to prevent transition from non-injecting to injection drug use.Key Messages:
Opioid use disorder (OUD) is a major health concern contributing to a significant burden of morbidity and mortality and affecting over 40 million people worldwide. 1 OUD, particularly injection drug use (IDU), is associated with harms such as the risk of blood-borne infections and overdose-related harms, among others. 1 According to the World Drug Report 2025, opioids are the second most common controlled drugs used worldwide, with a prevalence of 6.1%, and the largest number of people using opioids is from South Asia. 2 The report also highlighted a 14% rise in IDU in the last decade, with around 14 million individuals injecting drugs in 2023. 2 IDU was associated with blood-borne infections such as Human Immunodeficiency Virus (HIV) and Hepatitis C in a substantial portion of IDUs. 2 OUD, liver cirrhosis, and other chronic liver diseases contribute to two-thirds of the years of life lost (YLL) due to drug use. In India, the National Survey on Extent and Pattern of Substance Use in India (2019) found that 2.1% of the population aged 10–75 use opioids. 3 Moreover, among the people who inject drugs (PWID), opioids (heroin > pharmaceutical opioids) were the most commonly injected drugs.
In India, PWID have the highest HIV prevalence (6.26%) among all high-risk groups, which include men who have sex with men (MSM), and female sex workers (FSW). 4 It is reported that around 76% PWID begin opioid use through non-injecting routes in India, with a transition period of 1–5 years before starting IDU.5,6 This period offers an essential opportunity for preventive interventions to reduce morbidity and mortality associated with IDU.
Globally, factors associated with the transition from non-injecting routes to IDU include risk-taking behavior, peer influence, poor socioeconomic status, homelessness, and exposure to high-risk environments, among others.7,8 Other studies reporting that non-IDU often precedes IDU have found factors like unemployment, homelessness, early-onset substance abuse, and high severity of dependence associated with the transition.9,10 Community influences have also been reported to play a role, including proximity to injecting users, peer encouragement, sexual relationships with injecting users, and family history of injecting use.11,12 Economic factors may also be involved with the injection of drugs being more affordable, leading to the appeal of this route. 13
Among Indian studies on the transition from NIOU to IDU, factors such as a decrease in supply and an increased price of heroin, as well as easy availability of parenteral pharmaceutical opioids, have been found.14,15 In addition, studies have reported that factors such as lower education and employment, family history of substance use, larger peer groups, lower age of initiation of substance use, and longer duration of dependence are more commonly associated with IDUs compared to NIOUs.6,16,17 Studies focusing on social factors are primarily based on individuals from north-east India. 6 Moreover, although studies have evaluated characteristics of PWIDs in general, comparative analyses of NIOU versus IDU integrating sociodemographic, clinical, and psychosocial parameters remain limited, particularly studies examining psychological factors such as impulsivity and sensation seeking in an Indian population. Identifying factors associated with the transition to IDU in the Indian-context is essential for developing targeted prevention and intervention strategies to reduce the morbidity and mortality associated with OUD. The current study aimed to assess and compare sociodemographic, clinical, and psychosocial factors between IDUs and NIOU in opioid-dependent Indian males. We hypothesized that there would be significant differences in sociodemographic, social, and clinical factors between injecting and non-injecting opioid-dependent males.
Methods
Data collection for the study began in September 2022 and was completed in July 2023.
Ethical Considerations: The study was approved by the Institutional Ethics Committee. Written informed consent was obtained from all participants before recruitment. Participation or refusal did not influence medical care, and all participants continued to receive standard treatment at the center.
The manuscript was prepared in accordance with the STROBE reporting guidelines, and the completed checklist has been uploaded as “supplementary online material.”
This was a cross-sectional observational study conducted at a tertiary care drug dependence treatment center in North India. The study included adult male participants with OUD seeking treatment at the center. Using purposive sampling, 100 participants, including 50 injecting opioid users (IDU) and 50 non-injecting opioid users (NIOU), were recruited, with the sample size determined primarily by feasibility considerations. Inclusion criteria for IDU (n = 50) were male, aged ≥ 18 years, meeting ICD-10 criteria for OUD, 18 having history of injecting opioids at least once in the last 3 months, and not having received treatment in the previous 3 months. Inclusion criteria for NIOU (n = 50) were male, aged ≥ 18 years, meeting ICD-10 criteria for OUD, with no history of injecting opioids for non-medical reasons, and not having received treatment in the last 3 months. We recruited participants at the time of treatment entry to minimize any changes that may have occurred after treatment. Participants who refused to provide informed consent or had a severe physical/psychiatric illness affecting their ability to cooperate with the study were excluded.
Tools
For data collection, a semi-structured questionnaire was designed to capture sociodemographic and clinical characteristics, including family and peer influences, as well as psychosocial profiles. In addition, we used the WHO Alcohol, Smoking, and Substance Involvement Screening Test (WHO-ASSIST) for assessing recent substance use patterns. 19 It is an 8-item questionnaire used to identify hazardous or harmful use of substances like alcohol, tobacco, and illicit drugs. We also used the Maudsley Addiction Profile (MAP), which is a 60-item questionnaire that evaluates substance use, health risk behavior, physical and psychological health, and social functioning. 20 It is used to assess treatment outcomes and to compare pre- and post-treatment profiles.
For assessing the severity of dependence, we used the severity of dependence scale (SDS). 21 It is a 5-item scale assessing the degree of psychological dependence, with higher scores indicating greater severity. Moreover, we used the HIV Risk-taking Behavior Scale (HRBS), which is an 11-item scale that assesses risk-taking behaviors, particularly related to injecting drug use and HIV risk. 22 To assess sensation seeking, we used the sensation seeking scale (SSS), a 40-item instrument that measures an individual’s need for varied, novel experiences and their willingness to take risks. 23 The Indian adaptation was employed to enhance cultural relevance. 24 We also used the Barratt Impulsiveness Scale (BIS-11), a 30-item measure of impulsivity across three domains: motor, non-planning, and cognitive. 25 A validated Indian adaptation was used for the study. 26
Statistical Analysis
Data were analyzed using IBM SPSS version 29. 27 Descriptive statistics were analyzed using measures such as mean, median, mode, frequency, and percentage. For comparison between IDU and NIOU, analyses were conducted using the chi-square test (for categorical variables) and the t-test (for continuous variables). A p value of <.05 was considered significant.
Results
The two groups (IDU and NIOU) were comparable with respect to age, religion, marital status, number of family members, education, employment, income, and living arrangements (Table 1).
Sociodemographic Profile of Participants.
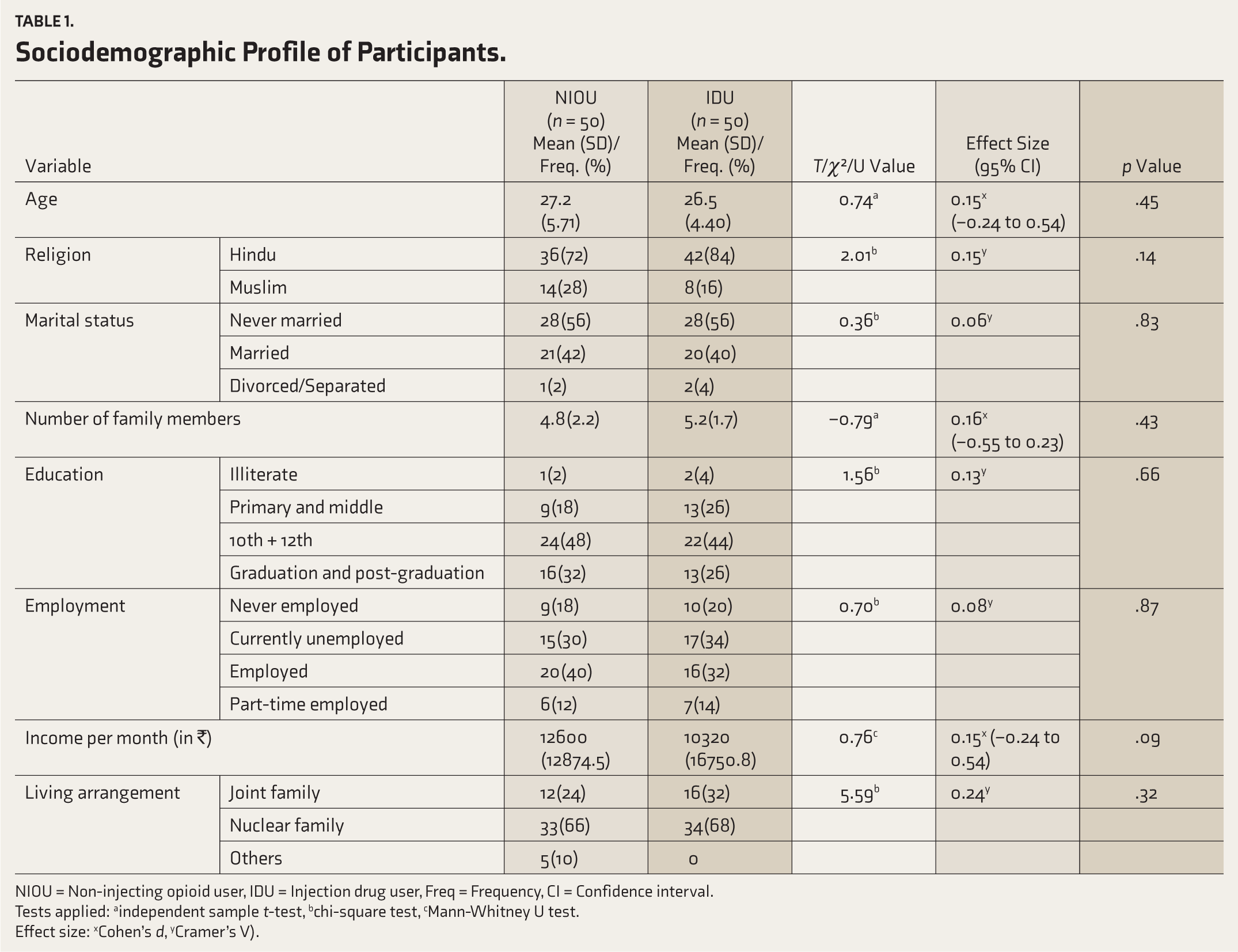
NIOU = Non-injecting opioid user, IDU = Injection drug user, Freq = Frequency, CI = Confidence interval.
Tests applied: aindependent sample t-test, bchi-square test, cMann-Whitney U test.
Effect size: xCohen’s d, yCramer’s V).
Among both groups, tobacco, cannabis, heroin, and alcohol were the most common substances reported to have been used ever. Among the two groups, there was no significant difference in the number of participants reporting ever use of opioids. In contrast, the history of ever use of alcohol was significantly higher among the IDU compared to the NIOU (86% vs. 64%, p = .01).
Regarding the use of substances in the last month, tobacco, cannabis, and alcohol were the most commonly used substances in both groups. Heroin use was more prevalent among NIOUs than IDUs (98% vs. 82%, p = .02), whereas IDUs reported higher use of other opioids, including Norphin, Buprenorphine, Tramadol (46% vs. 10%, p < .001), and cannabis (50% vs. 42%, p < .001).
Tobacco was reported to be the first substance used among both groups, and the average age of its initiation was comparable (17.1 years in NIOU vs. 16 years in IDU). The average age of initiation for most substances, including heroin (NIOU = 22.8, vs. IDU 20.2 years), was also comparable between the two groups. The total duration of substance use had comparable patterns between NIOU and IDUs across most substances. However, the average duration of cannabis use was significantly higher in the IDU group compared to the NIOU group (8 ± 4.65 years vs. 5.8 ± 4.2 years, p = .03).
The risk profiles of all substances, assessed using WHO-ASSIST across two groups, were comparable. Opioid users across both groups were predominantly in the high-risk category, whereas tobacco use was predominantly in the moderate-risk category in both groups. Moreover, both groups were comparable in terms of the severity of opioid dependence on the SDS.
Among IDUs (n = 50), 88% reported injecting drugs in the last month. Heroin was the most commonly injected substance, reported by 54% of IDUs in the past month, followed by Norphin/Buprenorphine injection and tablet buprenorphine (Table 2). The mean age of onset of IDU was 24.7(4.6) years. The median total duration of IDU was 3 years, and the average time of transition from NIOU to IDU was 4.4(3.3) years.
Substances Injected in the Last 1 Month Among IDU (n = 50).

IDU = Injection drug user, Inj. = Injection.
The number of people in the drug-using group (Median = 4) was comparable between IDUs and NIOU. However, IDUs had a significantly higher number of friends who inject drugs compared to NIOU (4.14 vs. 1.06, p = .001). Both groups were comparable in terms of having friends who do not use drugs. 16% of IDU individuals reported having a sexual partner who had IDU compared to none from NIOU (p = .001).
Both groups were comparable in the number of individuals who had ever engaged in illegal activities. However, a higher proportion of IDUs reported involvement in serious crimes, including shoplifting (p = .001), snatching (p = .03), and theft (p = .02). In contrast, NIOU had significantly higher involvement in activities such as pickpocketing (p = .001). Additionally, two individuals from the IDU group were also involved in drug peddling. Both groups were comparable with respect to history of incarceration(ever) and number of times incarcerated.
Family history of ever use of drugs as well as family history of alcohol use were significantly higher among the IDUs compared to the NIOU (p = .04 and .001, respectively).
Regarding awareness of harms and motivations for treatment, more IDUs, as compared to NIOU, were aware of pain and bleeding at the injection prick site (p = .04). Awareness of other health-related harms associated with IDU was comparable across groups. More IDUs, as compared to NIOU, were aware that HIV is transmitted by sharing syringes/needles (p = .05). For motivations for seeking treatment, significantly more IDUs reported health issues, fear of death, and fear of acquiring infections as motivating factors to seek treatment, as compared to NIOU. The influence of other motivating factors was comparable across the two groups.
On the MAP, the mean number of days using substances in the last 30 days was comparable between the groups for tobacco, alcohol, benzodiazepines, and cannabis. However, IDUs had a significantly higher number of days of heroin use compared to NIOU (28.5 vs. 25.92, p = .01). Among IDUs, the median days injected in the past month was 26 days, and the median number of times injected on a typical day was two times/day. The sexual risk behavior in the past 30 days was comparable between the two groups. Significantly more physical and psychological health symptoms were reported by IDUs in the past 30 days (p = .001). Both groups were comparable on all psychosocial parameters over the past 30 days, except that the IDU group had significantly more days of conflict with relatives (p = .01).
The IDUs had significantly higher scores on the HIV Risk-taking Behavior Scale (HRBS) (7.48 vs. 2.28, p = .001). Similarly, IDUs had a higher score on the Barratt Impulsivity Scale (BIS-11) (76.98 vs. 70.66, p = .003). Furthermore, on the SSS, there was a significant difference in the mean disinhibition (DIS) score and total score between NIOU and IDU individuals (p < .05) (Table 3).
Modified Sensation Seeking Scale Scores of Participants.
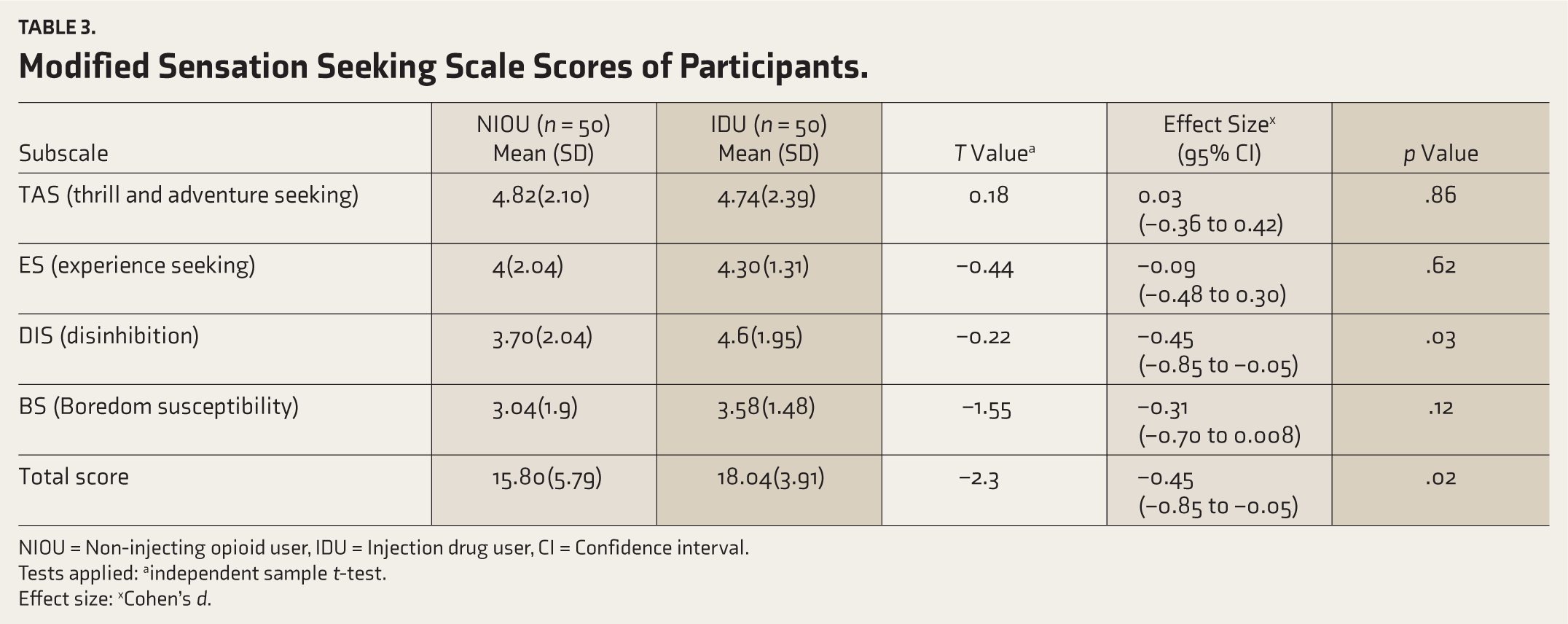
NIOU = Non-injecting opioid user, IDU = Injection drug user, CI = Confidence interval.
Tests applied: aindependent sample t-test.
Effect size: xCohen’s d.
Discussion
This study aimed to compare IDUs and NIOUs on sociodemographic, psychological, and clinical parameters to identify factors associated with IDU. The study found significant differences between the groups in terms of HIV risk-taking behaviors, impulsivity, sensation seeking, and substance use patterns while showing similarities in sociodemographic profiles and severity of dependence. Knowledge of these distinguishing factors may help identify characteristics that differ between NIOUs and IDUs. However, our data cannot determine whether these characteristics precede or follow IDU.
The two groups (IDUs and NIOU) were comparable across most sociodemographic variables, including age, education, occupation, marital status, and living arrangements. This is unlike a previous Indian multisite comparative study, in which IDUs, although of similar age group and sociocultural background, had lower educational attainment, were more likely to be unmarried, and were employed in skilled or unskilled labor compared with NIOU. 6 Our finding of a comparable sociodemographic profile may be because, in our study, both groups (IDUs and NIOS) come from a tertiary care drug dependence treatment center, and our sample size is smaller than some previous studies, with some NIOU at potential risk of transitioning to IDU. The mean age of participants in our study (NIOU = 27.2 years, IDU = 26.5 years) was lower than in some previous Indian studies that compared IDUs and NIOUs.6,16,28 This may be attributed to increased awareness and the availability of more treatment opportunities in the urban areas of our study. However, in a recent Indian study comparing IDUs and NIOU, the mean age was 26 years, consistent with our findings. 17 In our study, marital status was found to be comparable between the groups, which is in line with a previous study. 17 Another study reported that a higher percentage of IDUs were unmarried than NIOU (49% vs. 41%). 6 Employment status was also found to be comparable between the groups in our study, which is in line with a previous cross-sectional study from North India. 16 However, higher employment rates in NIOU compared to IDUs were reported by previous studies.6,17 Similarly, the finding of comparable educational status between the two groups in our study contrasts with previous studies that reported lower educational attainment among IDUs.6,17
Among the IDUs and NIOUs, the most common substance ever used other than opioids was tobacco (96% vs. 98%), followed by alcohol (86% vs. 64%) and cannabis (78% vs. 74%). Similar findings have been reported in another comparative multisite study from India. 6 In this study, use of other substances (tobacco, alcohol, and sedatives) was reported by a significantly higher proportion of IDUs, unlike in our study, where only alcohol use was significantly higher in the IDUs compared to NIOU. Another study has reported that individuals who consume alcohol daily are 2.6 times more likely to initiate IDU. 29 This highlights the potential association between alcohol use and initiation of IDU. Possible explanations for this association include the behavioral disinhibition and risk-taking that may occur during periods of alcohol intoxication. 30 The association may also be explained by common factors such as high impulsivity and sensation seeking. 30
In our study, there was no significant difference between NIOU and IDUs in the age of initiation of opioids and other substances. This is in line with another comparative analysis, which found no significant difference in the age of onset of heroin and other substances among the two groups. 6 However, in another study from the United States of America, the median age of first alcohol, cannabis, inhalant, heroin, crack, or cocaine use was significantly younger for IDUs compared to NIOUs. 31 A previous Indian study also reported an earlier onset of heroin use among IDUs compared to NIOU. 17 A study from Iran reported that IDUs started smoking cigarettes significantly earlier than non-IDUs. 10 Findings of these studies suggest that IDUs may tend to engage in substance use earlier, but our data cannot establish temporality regarding substance initiation.
In our study, there was no significant difference in the average severity of dependence between non-IDUs and IDUs. Two previous studies have reported similar findings.17,32 This may be because a higher severity of drug use, even in NIOU, is seen in patients who present to our tertiary care center. Hence, the severity of dependence did not differ significantly.
The most common drug injected by IDUs in our study was heroin (54%), followed by pharmaceutical drugs (46%), including buprenorphine and tramadol. This is in line with previous Indian studies.33–35 In an Indian study from Manipur and Nagaland, 46.7% of participants injected SP (Spasmo-Proxyvon), 18.1% injected heroin, and 23.1% were injecting both simultaneously. 36 Heroin was the most frequently (76%) injected substance in another study from Chennai. 37 In a more recent population-based, cross-sectional survey in four states of India (Manipur, Meghalaya, Mizoram, and Nagaland), the most common drug injected in the past 3 months was heroin in all states except in Nagaland (Dextropropoxyphene). 38 However, in a large multisite study, pharmaceutical opioids were the most frequently injected drug, accounting for 64.5% (582 individuals) of injections, followed by heroin at 34.3%. 6 Thus, there is considerable heterogeneity in the type of opioid injected in various regions.
In our study, the mean (SD) age of onset of use of heroin via the injecting route was 24.7(4.6) years, and the mean (SD) duration of transition from non-injecting to injecting route was 4.4(3.3) years. In a previous multisite study, the mean age of first use of injection heroin was 23.13 ± 4.65 years. 6 In a cross-sectional study in North India, the mean age of initiation of IDU was 20.1 years, 36 whereas a study from Chennai reported a mean age at IDU initiation of 25 years. 37
In our study, the mean duration of transition from non-injecting opioid use to the injecting route was around 4(3.3) years. This finding is consistent with previous research from India, which indicates that before starting injection use, a majority of PWID report having consumed drugs through non-injecting routes and make a transition to injecting drug use (IDU) after a period of approximately 2–10 years. 14 In a national study of about 1,000 IDUs in India, there was a gap of 1–5 years before transition to injecting routes. 39 In a more recent study, a majority (54.6%) reported consuming opioids through a non-injectable route for 2–5 years before initiating IDU, while another 26.5% reported transition to IDU within 2 years. 6 Our study replicates the finding from previous studies that there are often several years of non-IDU before initiation of IDU. Knowledge about this time duration is essential as it provides a chance for intervention to prevent the transition to injecting drug use. However, the cross-sectional design of our study cannot determine the individual transition pathways.
The median number of drug users in the peer group (four) was comparable between IDUs and NIOU. A multisite study with a large sample reported a median of three peers in the IDU group. 40 A more recent Indian study reported a larger peer group among IDUs than among NIOU. 17 Moreover, in our study, IDUs had a significantly higher number of drug-injecting friends. Having peers who use IDU has been reported as an essential factor in the transition to IDU. 6 In another Indian study, IDUs had a higher mean total network size than non-injectors. 36 The study also reported that individuals with larger IDU networks were 1.65 times more likely to have shared a syringe. 40 In addition, we found that 16% IDUs had a sexual partner who was injecting drugs, compared to none among the NIOU. Having a close friend or a sexual partner with IDU has been reported to be a risk factor for transition to IDU. A previous study reported that living with an IDU was associated with a two-times higher likelihood of reporting IDU compared to those who do not live with an IDU. 41 Overall, a larger substance-using personal network, particularly those who inject drugs, appears to be an essential factor associated with IDU.
The number of individuals involved in illegal activities was comparable between the two groups. However, IDUs reported higher involvement in serious crimes like shoplifting, snatching, and theft, while non-IDUs were more likely to engage in pickpocketing. Additionally, two individuals from the IDU group were also involved in drug peddling. There was no significant difference in incarceration history between the groups. In an Indian study, conducted in Chennai, out of 1158 IDUs, 12.8% of patients reported a history of at least one night in prison. 37 In a comparative study from Iran, 55% of IDUs and 36.7% of non-IDUs had a history of imprisonment. 10 In another study, the IDU group reported a higher number of criminal charges than non-IDUs, and IDUs were more likely to be charged with crimes related to the drugs, such as possessing or selling drugs. 32 In another cross-sectional study among injecting heroin users from Vietnam, 22.5% of participants had experienced imprisonment, and 64.3% reported being detained in a drug facility. 42 Overall involvement in serious crimes and illegal activities related to drug use appears to be associated more with IDUs compared to NIOU.
The family history of drug use was significantly higher in the IDUs compared to the NIOU. Similar to our study, in a comparative study among IDU and NIOU, the family history of illicit drug use was 87% and 21.7%, respectively. 10 Our findings are consistent with previous research, although the cross-sectional design precludes determining whether family-related factors contribute to the initiation of injection.
Awareness about health-related harms due to IDU was comparable among the groups, except for pain and bleeding at the injection site, regarding which more IDUs reported being aware. Also, more IDUs, as compared to NIOU, were aware that HIV is transmitted by sharing syringes/needles. In another study, a noticeable difference was reported in HIV/AIDS-related knowledge and attitudes between PWID and NIOU, with PWID demonstrating a superior overall understanding of transmission and prevention strategies for HIV. 6
Significantly more IDUs reported health issues, fear of death, and fear of acquiring infections as motivating factors to seek treatment, as compared to NIOU. Various reasons have been identified across studies as motivating treatment-seeking. In a cross-sectional, observational study, among 100 NIOU users, the most common reason to seek treatment was the inability to afford opiates. 43 In another cross-sectional Indian study, the most common reasons to seek treatment were becoming a habitual user (80%), followed by taking a substance for a long time (81%), and the need to take it every day (72%). 44 Various personal and psychological factors play essential roles for different individuals in seeking treatment. Psychoeducation about the health hazards of IDU may enhance treatment-seeking for some patients.
Regarding the MAP, in our study, IDUs had a significantly higher number of days of heroin use (in the last 30 days) compared to NIOU. A previous study from the Netherlands reported that a higher proportion of current IDUs reported heroin, alcohol, and amphetamine use in the last month. However, the study did not involve the MAP for assessment. 45 IDUs also reported significantly more physical and psychological health symptoms, and a higher number of days of conflict with relatives. These findings are in line with a multisite study with a large sample size from Canada, which reported significantly higher levels of mental and physical health problems compared to the NIOU. 46
The IDUs had significantly higher scores on the HIV Risk-taking Behavior Scale. This is in line with a previous Indian hospital-based study reporting that IDUs engage in high-risk sexual behaviors. 47 A study conducted on 1712 patients from Manipur and Nagaland reported that IDUs engaged in high-risk sexual practices, increasing the risk of HIV transmission. 48 Moreover, in our study, IDUs had a higher score on the Barratt Impulsivity Scale (BIS-11). A similar finding of high impulsivity among IDUs was reported in a previous study, which also found a strong positive correlation between high-risk behavior and impulsivity. 47 Another study from Sri Lanka reported that rash-impulsivity (defined as the tendency to indulge in approach behaviors regardless of outcome) was associated with high-risk behaviors and injection heroin use. 49 Furthermore, on the SSS, there was a significant difference in the mean disinhibition (DIS) score and total score between NIOU and IDU individuals (p < .05) in our study. In a Canadian study, sensation seeking was found to be associated with IDU and risk of indulging in drug-related behaviors, which are predictors of injection initiation. 50 Overall, our findings reflect the association of factors such as impulsivity, sensation seeking, and high-risk behavior with IDU.
Although the present study is cross-sectional and cannot infer causality, the findings may have practical relevance for treatment planning and prevention. The higher levels of impulsivity, sensation seeking, and risk-taking behaviors found among IDUs suggest that patients may benefit from targeted psychosocial interventions. As most IDUs report using opioids through non-injection routes before transitioning to IDU, interventions focused on the at-risk NIOU may play a role in deterring this transition. 6 Timely treatment of OUD may be critical in preventing the transition. Moreover, given the essential role of social factors, particularly the peer group, in the transition to IDU, peer-led interventions may be employed.
Strengths and Limitations
The present study compared injecting and non-injecting male opioid-dependent patients on sociodemographic, social, and clinical factors to assess factors associated with IDU. There are very few studies in India that have compared the non-injecting and injecting opioid users. In addition to a semi-structured questionnaire designed for the study, we used standard, validated instruments to assess multiple parameters, including sociodemographic, drug-use-related, and personality-related factors. Another strength of the study is the recruitment of participants at the time of treatment entry, thereby eliminating post-treatment changes.
The study also has certain limitations. As it was conducted at a tertiary care hospital, the study sample may not be representative of opioid users in the community. The information about the pattern of psychoactive substance use was based on self-reporting by participants, which is a limitation due to potential recall bias and socially desirable responses. Purposive sampling was used in the study for feasibility, with participant recruitment conducted non-randomly. This can lead to selection bias. However, purposive sampling was used for feasibility reasons and was not intended to exclude any patient groups. As this is a cross-sectional study, all findings represent associations only; temporal or causal relationships cannot be inferred. Moreover, the inclusion of only male participants may also reduce the generalizability of our findings. The study involved multiple statistical comparisons, increasing the risk of Type I error. As formal correction methods for multiple comparisons were not applied, due to correlations among variables and the exploratory nature of the analysis, the results should be interpreted with caution. Finally, several potential confounding variables, including socioeconomic status, trauma history, common mental disorders, and personality pathology, were not assessed or controlled for. These unmeasured variables may account for the observed associations between psychological traits and IDU status.
Conclusion
In this study of adult males with OUD, IDUs had higher rates of alcohol use, longer cannabis use duration, and a stronger family history of substance use. They also had more social connections to drug users and were more likely to engage in serious crimes. IDUs reported greater awareness of injection-related risks and more motivations for treatment, often driven by health concerns. Furthermore, IDUs experienced more physical and psychological symptoms, family conflicts, and exhibited higher risk-taking and impulsivity. It remains unclear if these traits precede or follow the initiation of injection use. Our findings highlight the need for targeted harm-reduction strategies and psychosocial interventions; future research should include larger samples and non-clinical populations to further explore these differences.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
The authors have no acknowledgments to declare.
Data Availability Statement
Deidentified individual participant data (including data dictionaries) will be made available, in addition to study protocols, the statistical analysis plan, and the informed consent form. The data will be made available upon publication to researchers who provide a methodologically sound proposal to achieve the goals of the approved proposal. Proposals should be submitted to
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethics Approval
The study was approved by the Institute Ethics Committee, All India Institute of Medical Sciences (AIIMS), New Delhi (Approval Ref. No. IECPG-337/27.04/22, RT-38/26.05.22; approved on 27 May 2022).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from all participants prior to recruitment in the study.
Prior Presentation
The manuscript has not been presented previously.
PROSPERO/CTRI Registration
Not applicable.
Simultaneous Submission
The manuscript has not been submitted to any other journal or resource.
Study Status (for Study Protocol)
Not applicable.
Trial Registration
Not applicable, as the current study was not an interventional study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.