
Abstract
Background:
Schizophrenia is a multifaceted and heterogeneous psychiatric disorder, marked by the presence of positive, negative, and cognitive symptom domains. In the chronic course, few symptoms remain persistent, leading to socio-occupational impairment. Few studies have used memantine (an NMDA receptor antagonist) as an adjunctive treatment, noting reductions in both positive and negative symptoms, accompanied by improvements in cognitive performance and overall functioning. The present study explored the effectiveness of adding memantine for cognitive symptoms in schizophrenia with a chronic course.
Methods:
This prospective, single-arm, open-label study used a pre-post design. A total of 30 individuals with schizophrenia, diagnosed based on ICD-10 criteria and having an illness duration of more than two years, were included. Socio-demographic data were collected, and the Addenbrooke’s Cognitive Examination Scale-Revised (ACE-R) was administered at baseline. Subsequently, memantine was added to their ongoing treatment regimen. The ACE-R assessment was repeated after eight weeks. Data was analyzed using R software version 4.4.1.
Results:
Different ACE-R score variables were compared before and after adding memantine. A significant relationship was found between ACE-R scores after adding memantine and the baseline scores (p < .001), except for the writing subcomponent of the language variable.
Conclusions:
The results of this study suggest that adding memantine to an antipsychotic treatment regimen may provide beneficial effects on cognitive symptoms in chronic schizophrenia, with good tolerability and minimal adverse effects.
Trial Registration:
The study was registered under the Clinical Trials Registry in India (CTRI), CTRI/2024/12/077774.
Question: Does adjunctive memantine improve cognitive symptoms in patients with chronic schizophrenia? Findings: Memantine added to antipsychotic treatment showed improvement in cognitive domains, though results were inconsistent across studies. Meaning: Memantine may offer cognitive benefits as an adjunct therapy in schizophrenia, warranting larger controlled trials.Key Messages:
Schizophrenia is a complex and heterogeneous psychotic disorder with variable phenotypic expressions, characterized by an intriguing set of symptoms that are classically grouped into three main categories: positive (hallucinations and delusions), negative (social withdrawal, apathy, emotional blunting), and cognitive symptoms (such as attention and memory impairments). 1 It has a significant impact on the social and occupational functioning of the patients and is currently among the 10 most disabling diseases. 1 Cognitive deficits are a core characteristic of schizophrenia, present in over 80% of patients, and represent a major contributor to functional disability as well as the indirect economic burden of the disorder. 2 The trajectory of cognitive deficits in schizophrenia continues to be debated, with one hypothesis positing that the disorder is neurodevelopmental in origin, wherein cognitive impairments arise from aberrant brain development and signify insufficient functional acquisition rather than subsequent deterioration. 3 The second hypothesis posits that, in addition to the first, there exists a neurodegenerative component that contributes to further cognitive decline following the onset of psychotic symptoms. Initially, the pathogenesis of schizophrenia was attributed solely to dopaminergic hyperactivity within the mesolimbic pathway; however, emerging evidence indicates that glutamatergic pathways, particularly involving N-methyl-D-aspartate receptors (NMDARs), also play a significant role in the disorder. 4
Numerous pharmacologic, genetic, and biochemical studies have demonstrated that NMDAR hypofunction is a significant contributing factor to cognitive symptoms and psychotic symptoms of schizophrenia. 5 Glutamate carboxypeptidase II (GCP-II) regulates the levels of N-acetyl-aspartyl-glutamate (NAAG), an endogenous antagonist of NMDAR and agonist of mGluR3. Evidence of decreased GCP-II activity and increased NAAG concentrations in the brains of individuals with schizophrenia supports the hypothesis that NAAG mediated signaling is dysregulated in the disorder. 6 Multiple lines of evidence implicate glutamatergic dysregulation in schizophrenia. 7 The NMDA receptor hypofunction hypothesis is supported by the psychotomimetic effects of NMDA channel antagonists such as ketamine and phencyclidine, as well as by observations of decreased cerebrospinal fluid glutamate levels in affected individuals. 8 Furthermore, clinical studies have demonstrated that adjunctive treatment with allosteric NMDA receptor agonists targeting the glycine B site is associated with improvements, particularly in negative and cognitive symptoms, among patients with schizophrenia. 9
The rationale for using memantine in schizophrenia comes from data suggesting neurodegenerative processes in schizophrenia. 10 Memantine is a non-competitive NMDA receptor antagonist with low affinity for the receptor and voltage/use-dependent action.11,12 Due to these characteristics, memantine lacks the severe toxic effects of the potent NMDA receptor blockers like ketamine and phencyclidine. In addition, it selectively inhibits extra-synaptic glutamate activity, thereby protecting against excitotoxic damage, while maintaining normal synaptic transmission. 13 These properties may underlie the lack of psychotomimetic/psychedelic effects and the low interference with normal physiological functions.11,14 A controlled pilot fMRI study in individuals with schizophrenia demonstrated that adjunctive memantine, when combined with atypical antipsychotics, enhanced activation in the left inferior frontal gyrus while reducing activation in the left inferior parietal lobule relative to placebo, indicating its modulatory effects on brain regions implicated in working memory deficits. 15
Memantine was officially licensed for the treatment of moderate to severe Alzheimer’s disease (AD). 16 It has a favorable safety and tolerability profile. 17 It has been hypothesized to have a neuroprotective action in schizophrenia and other psychiatric disorders. 18 Few case reports have explored its role as an off-label use in psychotic disorders. 19 Limited studies have examined the adjunctive use of memantine in schizophrenia, yielding inconsistent findings.20,21 As previous studies examining the efficacy of memantine have yielded inconclusive results, highlighting the need for further investigation to delineate its therapeutic potential in cognitive disturbances in schizophrenia. This study aims to systematically assess the clinical utility of memantine in combination with second-generation antipsychotics for addressing cognitive symptoms in schizophrenia, thereby contributing to the existing evidence.
Aim
To evaluate the effectiveness of memantine for cognitive symptoms in chronic schizophrenia.
Objectives:
To assess the baseline cognitive functions in patients with schizophrenia who have a chronic course. To assess the changes in various cognitive components after adding memantine as an adjunct to antipsychotic treatment.
Methods
Ethics
The study commenced following receipt of IEC approval (No: 20/30.09.2024) and was registered under a CTRI (CTRI/2024/12/077774). All identifying information was de-identified before analysis, and the data were accessible only to the researchers.
Design
This was a longitudinal, single-arm, open-trial study employing a pre-post design, following STROBE guidelines, where the intervention was the addition of memantine. The study spanned three months, from December 2024 to February 2025, in the department of psychiatry of a tertiary care teaching hospital. The STROBE guidelines were uploaded as supplementary online material.
Participants
The sample consists of 50 patients with schizophrenia. Inclusion criteria were (a) patients with an existing diagnosis of schizophrenia as per the ICD-10, 22 exceeding two years, who have been stable without active psychotic symptoms. Although individuals with negative symptoms were not explicitly excluded, symptom severity was not formally assessed, (b) between age groups of 18 and 65 years, and (c) patients with documented consent. Exclusion criteria were (a) patients taking any other CNS medications, and (b) any co-morbid psychiatric illnesses, including substance use disorders, excluded through expert clinical evaluation based on ICD-10 diagnostic criteria.
Procedure
Patients meeting the inclusion criteria were enrolled in the study after providing written informed consent. The Brief Psychiatry Rating Scale (BPRS), 23 was used to rule out patients with acute symptoms of schizophrenia. Patients who have had schizophrenia for more than 2 years were included in the study based on convenience sampling. Cognitive functions at baseline were assessed by a trained psychiatrist using the Addenbrooke’s Cognitive Examination-Revised (ACE-R) scale. 24 To maintain uniformity over all the participants, patients who were on risperidone had been recruited. Memantine was added to the ongoing treatment and titrated up to 10 mg once daily at night as an adjunctive, and the ACE-R scale was repeated at the end of eight weeks. Among these 20 patients were lost during follow-up. Thus, 30 patients were ultimately included in the statistical analysis.
Tool
The ACE-R, adapted for Telugu-speaking individuals, has been validated for both literate and illiterate populations, demonstrating satisfactory validity and reliability across multiple Telugu-speaking cohorts. 25 The ACE-R was selected for this study because it is feasible to administer in the local language, an important consideration given that the study population was drawn from a rural background. Although the ACE-R has been widely studied and is considered one of the most comprehensive cognitive assessment tools, only a few studies have applied it specifically to schizophrenia,26–28 and it has not yet been formally validated for assessing cognitive symptoms in this disorder. The ACE-R evaluates five cognitive dimensions: Attention and Orientation, Fluency, Memory, Language, and Visuospatial abilities, yielding a maximum score of 100. 29 The local language version used in this study was developed at NIMS, Hyderabad, and adapted for Telugu-speaking individuals. This adaptation demonstrated strong psychometric properties, with a sensitivity of 84% and specificity of 98% for diagnosing dementia at a threshold score of ≤82, and a specificity of 89% and sensitivity of 86% for identifying mild cognitive impairment with scores between 83 and 88. 30 The tool has also been extensively employed across several Indian languages, yielding results comparable to the English versions. 30
Statistical Analysis
The collected data were first organized in Microsoft Excel for preliminary data management, and subsequent analyses were conducted using R software, version 4.4.1, in R Studio 2024.04. 2+764.pro1.31,32 Packages like dplyr, summary tools, and ggplot2 are used in the R software. Descriptive analysis was conducted using the median and interquartile range (IQR). The inferential analysis was done by the Wilcoxon signed-rank test.
Results
Of the 50 participants initially enrolled, 20 (40%) were lost to follow-up. Reasons for loss to follow-up include relocation (n = 6), withdrawal of consent (n = 5), and inability to contact (n = 9). A comparison of baseline characteristics between completers and dropouts revealed no significant differences in age, sex, baseline scores, or treatment allocation (p > .05), suggesting that attrition was not systematic. Finally, 30 participants were included in the statistical analysis.
Socio-demographic details (Table 1):
The participants’ mean age was 36.8 years, ranging from 25 to 63 years. The sample consisted of 60% females and 40% males who had completed up to primary school. The majority were Housewives (46.7%), 63.3% were married, and the mean duration of illness was 6 years. 66.7% hailed from rural backgrounds, and 50% belonged to low socioeconomic status.
Socio-demographic Characteristics of the Participants.
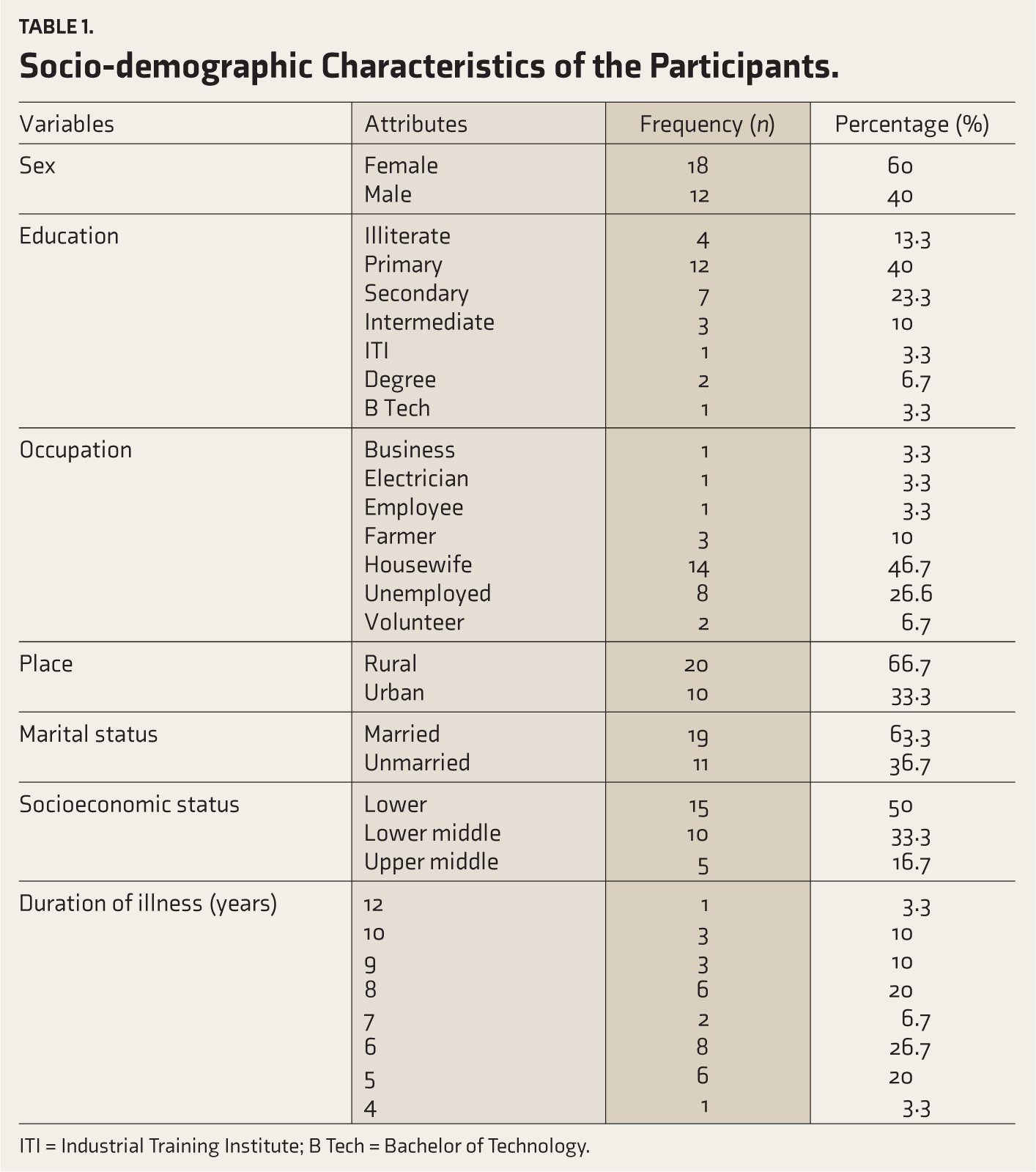
ITI = Industrial Training Institute; B Tech = Bachelor of Technology.
Comparison between different variables of ACE-R scores before and after adding memantine (Table 2).
Association Between Different Variables of the Addenbrooke’s Cognitive Examination Scale Before and After Adding Memantine.
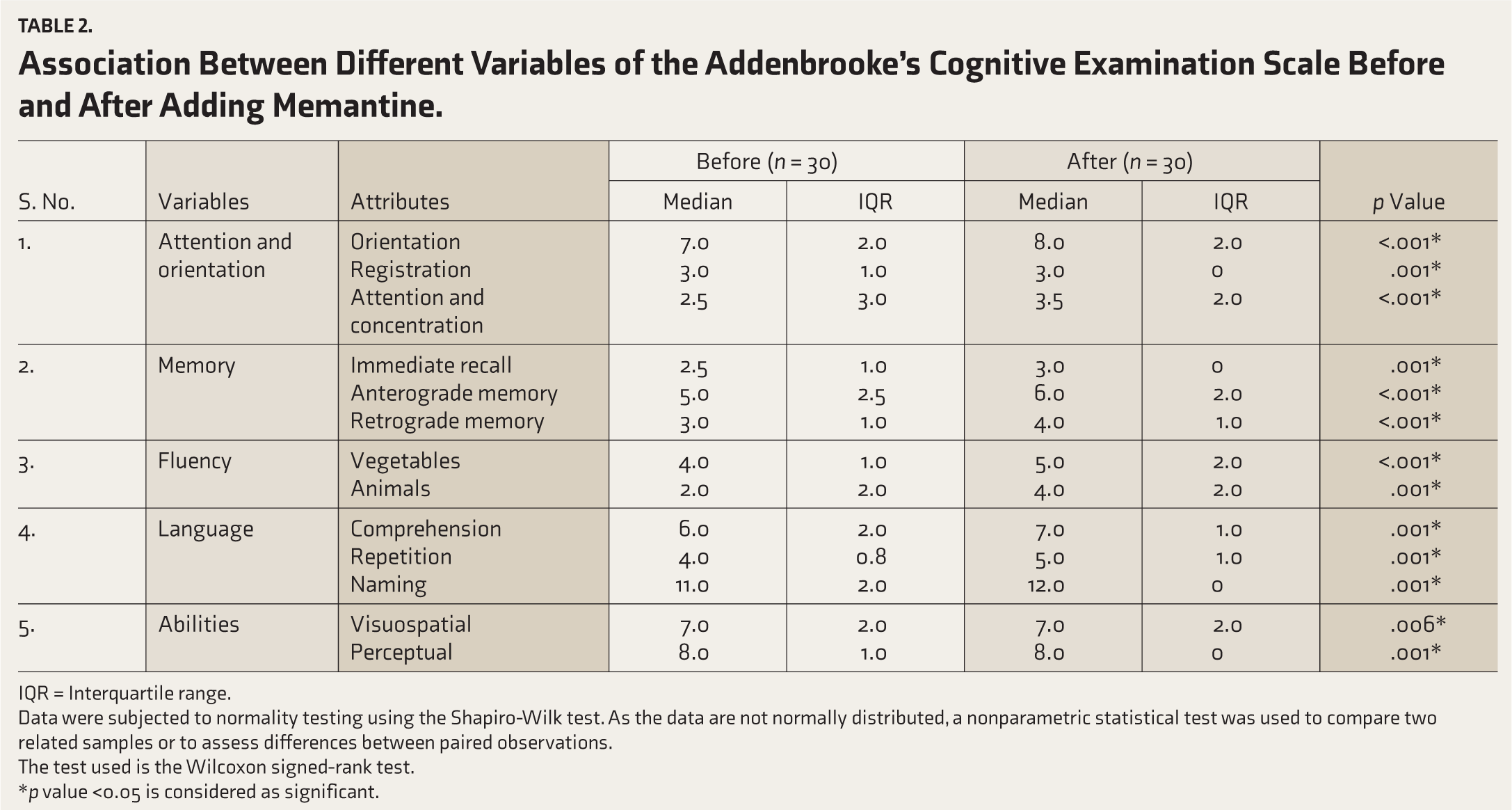
IQR = Interquartile range.
Data were subjected to normality testing using the Shapiro-Wilk test. As the data are not normally distributed, a nonparametric statistical test was used to compare two related samples or to assess differences between paired observations.
The test used is the Wilcoxon signed-rank test.
*p value <0.05 is considered as significant.
There was a significant association between variables of ACE-R scores at baseline and after adding memantine.
In the writing subdomain of the language domain, 10% of participants (3 out of 30) initially scored 0, while 90% (27 out of 30) scored 1. After memantine augmentation, the proportion of participants scoring 0 decreased to 6.7% (2 out of 30), while those scoring 1 increased to 93.3% (28 out of 30), indicating a slight improvement in writing performance. However, the analysis yielded a non-significant result (p > .99). All domains showed a significant improvement after adding memantine (p < .001), except for writing in the Language domain.
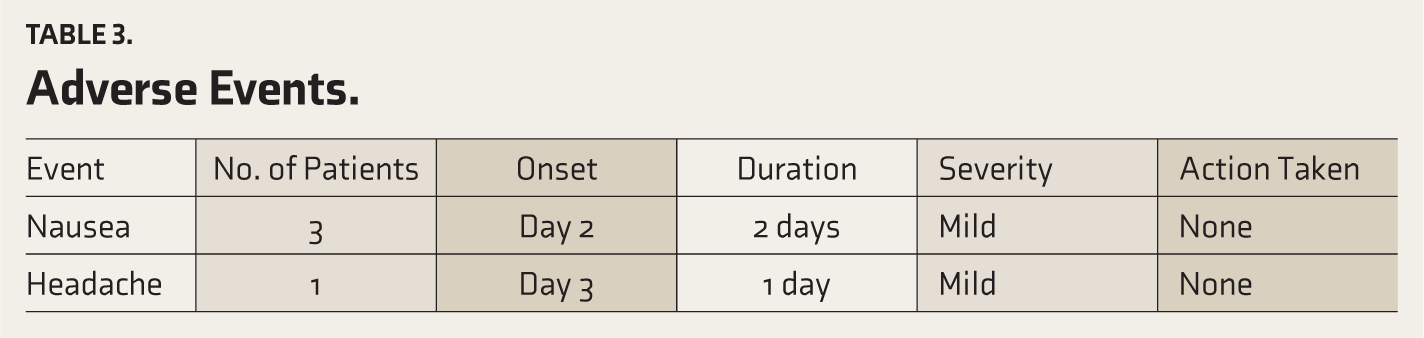
Adverse events (Table 3): No serious adverse events or deaths occurred. A few patients reported nausea and headaches in the initial days, which subsided after continued use. All adverse events were mild in severity and self-limiting, resolving without medical intervention.
Adverse Events.
Discussion
The current study explored the effect of memantine on cognitive functions in individuals with chronic schizophrenia. Several studies have been conducted regarding the clinical effectiveness and implications of memantine in schizophrenia management; however, the findings have been mixed, with some studies supporting this use and others being equivocal.
The results of the current study align with those reported by Mazinani and colleagues (2017), who demonstrated that the adjunctive use of memantine with risperidone led to significant improvements in both negative symptoms and cognitive functioning in individuals with schizophrenia. Their randomized, double-blind, placebo-controlled trial supports the potential role of memantine as an effective adjunctive treatment, particularly for symptom domains that are often less responsive to conventional antipsychotic therapy. 33 In terms of similarities, both the current and the earlier study by Mazinani and colleagues, 33 observed improvement in cognitive function following memantine treatment, along with certain differences, like the previous study recruited only male patients. They used the Mini-Mental Status Examination (MMSE) to assess cognitive function.
Similarly, Schaefer and colleagues explored the effects of a 6- or 24-week memantine adjunct to risperidone on cognitive and negative symptoms in patients with acute or chronic schizophrenia in a proof-of-concept study. Their findings indicated that acute schizophrenia patients treated with memantine showed marked improvements in verbal learning, cognitive flexibility, problem-solving, and attention. In chronic schizophrenia patients, memantine administration was associated with significantly enhanced immediate memory performance. 34 The current study aligns with the study by Schaefer and colleagues, 34 with certain findings like improvement in immediate memory and attention domains following memantine administration, and diverges in aspects that they have included both acute and chronic schizophrenia patients, used various neuropsychological measures to assess cognitive functions like Continuous Performance Test (CPT), Trail Making Test A (TMT A), Benton Learning Test (BLT), Digit Span backward, Digit Span forward, Wisconsin Card-Sorting test and other various tests.
In another study, Hasaanpour F and colleagues evaluated the efficacy and safety of memantine as an adjunct to standard antipsychotic treatment on psychotic symptoms and cognitive function in individuals with chronic schizophrenia over 8 weeks. The study demonstrated that adjunctive memantine improved verbal memory, learning, verbal letter fluency, and working memory, although it did not produce significant changes in psychotic symptoms. 35 The present study is consistent with previous findings, 35 in demonstrating good tolerability and minimal adverse effects of adjunctive memantine, supporting its favorable safety profile. Additionally, while both this and earlier studies, 35 reported cognitive improvements that vary across studies, with specific domains showing benefit, which may reflect differences in assessment instruments, treatment duration, baseline cognitive functioning, or symptom profiles of the recruited participants.
A few studies contradict the current study’s results.36,37 In a randomized placebo-controlled study conducted by Leiberman and colleagues, who focused on both residual psychopathology and impaired cognition, memantine demonstrated no therapeutic efficacy as an adjunctive treatment in patients with schizophrenia. It was associated with a higher incidence of adverse effects than placebo. 36 A placebo-controlled pilot study by Lee and colleagues found that adjunctive memantine treatment did not yield improvements in cognitive functioning or psychopathology among patients with chronic schizophrenia. However, memantine was well tolerated and did not worsen positive symptoms. 37 Similarly, a systematic review by Di Iorio and colleagues concluded that memantine predominantly improves negative symptoms, whereas cognitive and positive symptoms show no significant improvement. 20 These discrepancies may reflect differences in study populations (residual vs. chronic stable patients), sample size, illness phase, concomitant antipsychotic regimens, and treatment duration. Moreover, the use of broad global measures in earlier studies and pooled analyses in systematic reviews may have obscured subtle domain-specific improvements. In contrast, the present study employed targeted cognitive assessments focusing on attention, concentration, and visual-perceptual skills, which may have been more sensitive to detecting change. Taken together, these variations suggest that memantine’s cognitive effects may be context-dependent, emerging more clearly in selected domains and patient subgroups under specific methodological conditions.
With respect to safety, memantine has already been established as a treatment for AD, demonstrating benefits in slowing disease progression as well as a favorable safety profile. 38 However, evidence regarding its safety in the treatment of schizophrenia remains limited and inconsistent. In the present study, our findings, consistent with those of most other trials, indicated good tolerability of memantine at 10 mg/day in patients with chronic schizophrenia, with no worsening or emergence of positive symptoms, agitation, or hallucinations. A few patients reported mild nausea and headache in the initial days, which reduced over continued use. In the trial of Lieberman and colleagues, adverse events, dropouts, anxiety, and hallucinations were reported more frequently in the memantine group compared to placebo (5.8% vs. 0%). 36
To minimize potential practice effects, the order of test administration was varied across participants, and assessments were spaced 8 weeks apart. An 8-week interval in our study aligns with established clinical research practices,39,40 and provides a scientifically grounded rationale to assess the impact of adjunctive memantine on cognitive symptoms in chronic schizophrenia. These findings align with existing evidence suggesting that NMDA receptor modulators with neuroprotective properties may benefit cognitive symptoms in schizophrenia. 41 Memantine, in particular, has demonstrated strong neuroprotective effects in excitotoxin-induced neurotoxicity models by preventing the pathological opening of NMDA receptor-gated calcium channels. 42 Thus, the present findings support the growing body of evidence for memantine’s potential role in improving cognition in schizophrenia.
This study suggests that adding memantine to antipsychotic treatment improves cognitive performance, as assessed by the ACE-R. It should be noted that the ACE-R has not been formally validated for assessing cognitive change in schizophrenia. This limitation warrants caution when interpreting the findings, as it may affect both the validity of the measured cognitive outcomes and the generalizability of the results to broader schizophrenia populations. Future studies should consider using cognitive assessment tools that are specifically validated for this patient group to strengthen the reliability of the conclusions. Attrition (resulting in a 40% loss to follow-up) and the use of a convenience sample may have introduced selection bias. Although baseline comparisons suggested no major differences between completers and dropouts, the lack of effect sizes and confidence intervals limits the strength of this conclusion. The other limitations were a small, uncalculated sample size and the absence of a control group. The non- randomized design limits generalizability, underscoring the need for future placebo-controlled trials with larger sample sizes and extended follow-up. Although efforts were made to minimize practice effects, they could not be eliminated; it remains a potential limitation. Even though participants were clinically stable and taking consistent doses of antipsychotics, detailed symptom characterization was not conducted as the Positive and Negative Syndrome Scale (PANSS) was not administered. This remains a limitation of the present study, and future research should incorporate more standardized measures for more detailed symptom profiling.
Future Directions
The Pharmacological profile of memantine can be studied more deeply and extensively to understand its role in the improvement and prevention of cognitive symptoms, not only in schizophrenia but also in conditions such as bipolar disorder, where cognitive impairments emerge during the chronic phase.
Conclusions
The findings of this study suggest that adding memantine to an antipsychotic treatment regimen may provide beneficial effects on cognitive symptoms in chronic schizophrenia, with good tolerability and minimal adverse effects. However, further research is required to confirm these findings.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Data Sharing Statement
All de-identified participant data underlying the results, including the study protocol, master chart (which includes demographic details and ACE-R scores before and after adding memantine), and statistical analysis, will be made available to the researchers who provide a methodologically sound proposal. Data will be made available upon request through email to
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
The study was approved by the Institutional Ethical Committee (IEC) KIMS RF-20/30.09.2024. This study was registered under the Clinical Trials Registry in India (
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Patients were included in the study after obtaining written informed consent. No consent is required for the use or publication of any information provided in the paper.
Presentation
Paper presentation was done at the IPS South Zone Conference (IPSOCON - SZB)-Guntur 2023.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.