
Abstract
Purpose of the Review:
This narrative review evaluates the effectiveness of interpersonal psychotherapy (IPT) among individuals at risk of suicide, with a focus on the quality of randomized controlled studies.
Collection and Analysis of Data:
The available literature was systematically searched on PubMed, the Cochrane Library, Hinari-Research4Life, and ResearchGate to identify RCTs in which participants at risk of suicide received IPT compared to other forms of treatment. Extracted study data were organized into a table of evidence using Microsoft Excel and Word. The Risk of Bias 2 Excel tool was used to evaluate the possibility of bias. Out of 158 identified studies, six met the inclusion criteria for review and analysis, encompassing 1,275 participants, of whom 53.1% were randomized to IPT conditions. Among these studies, two demonstrated that IPT was effective in significantly reducing suicidal ideation and behaviors over time compared to treatment-as-usual or waitlist conditions. However, most studies did not report clinically significant outcomes, such as risk ratios, effect sizes, and confidence intervals (CIs) with p values. A significant risk of bias was observed across the majority of studies, particularly in randomization (83.30%), deviation from the intended intervention (66.70%), missing outcomes (66.70%), measurement of outcomes (66.70%), and selection of the reported results (100%), with an overall high risk of bias across all assessed domains.
Conclusions:
The effectiveness of IPT in reducing suicidal risk was found to be imprecise due to incomplete reporting of results, indicating the need for further conclusive and evident research.
Globally, suicidal behavior is a significant public health concern, as per the World Health Organization. Around 40 countries have national suicide prevention strategies (NSPSs). 1 India also introduced its NSPSs on November 21, 2022. 2 The latest systematic review suggested that the prevalence of suicidal ideation among adolescents was found to be 11%, while suicidal plans and attempts were each 3%. 3 Numerous contributory factors, such as previous suicidal thoughts and attempts, psychiatric diagnoses (including depression, schizophrenia, alcohol use, anxiety, borderline personality disorder, post-traumatic stress disorder, and adjustment disorders), previous in-patient admissions, and recent biopsychosocial stressors have also been known to be associated with suicidal behaviors.4,5 Among them, studies have suggested a connection between interpersonal issues and the risk of suicide, with interpersonal psychotherapy (IPT) emerging as an evidence-based treatment for depression.6–8 Previous systematic reviews,9,10 and meta-analyses,11–13 have established IPT as an effective monotherapy for treating depression in adolescents/adults, and have highlighted its adaptability across various clinical populations. 14
Rationale for the Study
The current body of literature provides insufficient evidence regarding the effectiveness of IPT in reducing the risk of suicide or suicidal behaviors. The limited number of randomized controlled trials (RCTs) further restricts our understanding of the efficacy of available therapies, including IPT, in addressing suicide risk. 15 This review provides an insightful explanation of the effectiveness of IPT on the risk of suicide by focusing on RCTs, which may have been unanswered in previous studies and reviews. This narrative review addresses the gap by (a) analyzing RCTs to evaluate the effectiveness of IPT in reducing suicide risk; (b) examining the components and working hypotheses of IPT in reducing suicidal risk; (c) assessing the quality of these studies; and (d) proposing recommendations to guide future randomized controlled research in this area.
Initially, the following research question was formulated: Is IPT more effective than other standardized treatments in managing individuals at risk of suicide?
Methods
This review is reported according to the Scale for the Assessment of Narrative Review Articles guideline. 16 The literature search was conducted to screen published records evaluating the effectiveness of IPT in individuals at risk of suicide. An advanced search strategy was implemented across the following databases: PubMed, Cochrane Library, Hinari-Research4Life, and ResearchGate. Search terms included combinations of “Interpersonal Psychotherapy,” “Brief Interpersonal Psychotherapy,” “IPT,” “IPT-A,” and “Suicidal Risk,” with a filter applied for RCTs. The search string for PubMed was: ((((Interpersonal psychotherapy) OR (Brief Interpersonal Psychotherapy)) OR (IPT)) OR (IPT-A)) AND (Suicidal risk); Filter: Randomized controlled trials. Similarly, searches in the Cochrane Library, Research4Life, and ResearchGate utilized equivalent terms. The last search for published records was completed on October 18, 2024. Studies meeting the inclusion criteria were further analyzed.
To ensure relevance and methodological rigor, studies were included if they met the following criteria: (a) participants had a documented suicidal risk characterized by a history of suicide attempts within 1 month or frequent expression of suicidal ideation or death wishes; (b) the intervention involved the application of IPT with a minimum of five weekly sessions; (c) the study design employed an RCT framework; and (d) outcomes investigated included measures of suicidal risk, such as suicidal ideation and behaviors.
The studies included after screening were systematically assessed. All records were managed using Zotero (version 6.0.36) and Microsoft Excel (version 2019). These tools were used to identify and exclude duplicate entries. Extracted data from eligible studies were organized into a table of evidence in Microsoft Excel and Microsoft Word, providing a clear and structured overview of study characteristics and findings (Supplementary Files 1 and 2). Although the Risk of Bias 2 Excel tool was used to assess the risk of bias across included studies, all analyses were cross-verified by co-authors, who checked and scrutinized the extracted data to ensure accuracy and consistency.
Results
The database search yielded 158 records. A systematic screening process was followed for study selection, such as initially screening title, followed by the abstract followed, and then the full text. The flow diagram (Figure 1) summarizes the study selection process, including reasons for exclusion: (a) 37 studies were excluded because they did not employ IPT or RCT designs; (b) 21 studies were excluded as they neither utilized RCT designs nor focused on suicide risk outcomes; (c) 31 records were reviews or meta-analyses that did not address suicide risk outcomes; and (d) 23 records were excluded as they consisted of book sections, protocols, posters, or publications in other languages. Additionally, 36 full-text articles were reviewed for eligibility, of which 30 were excluded because they did not specifically assess suicide risk outcomes. Ultimately, 152 studies were excluded and six studies were included in the final review (see Supplementary Excel File 1 for details on inclusion/exclusion criteria and remarks).
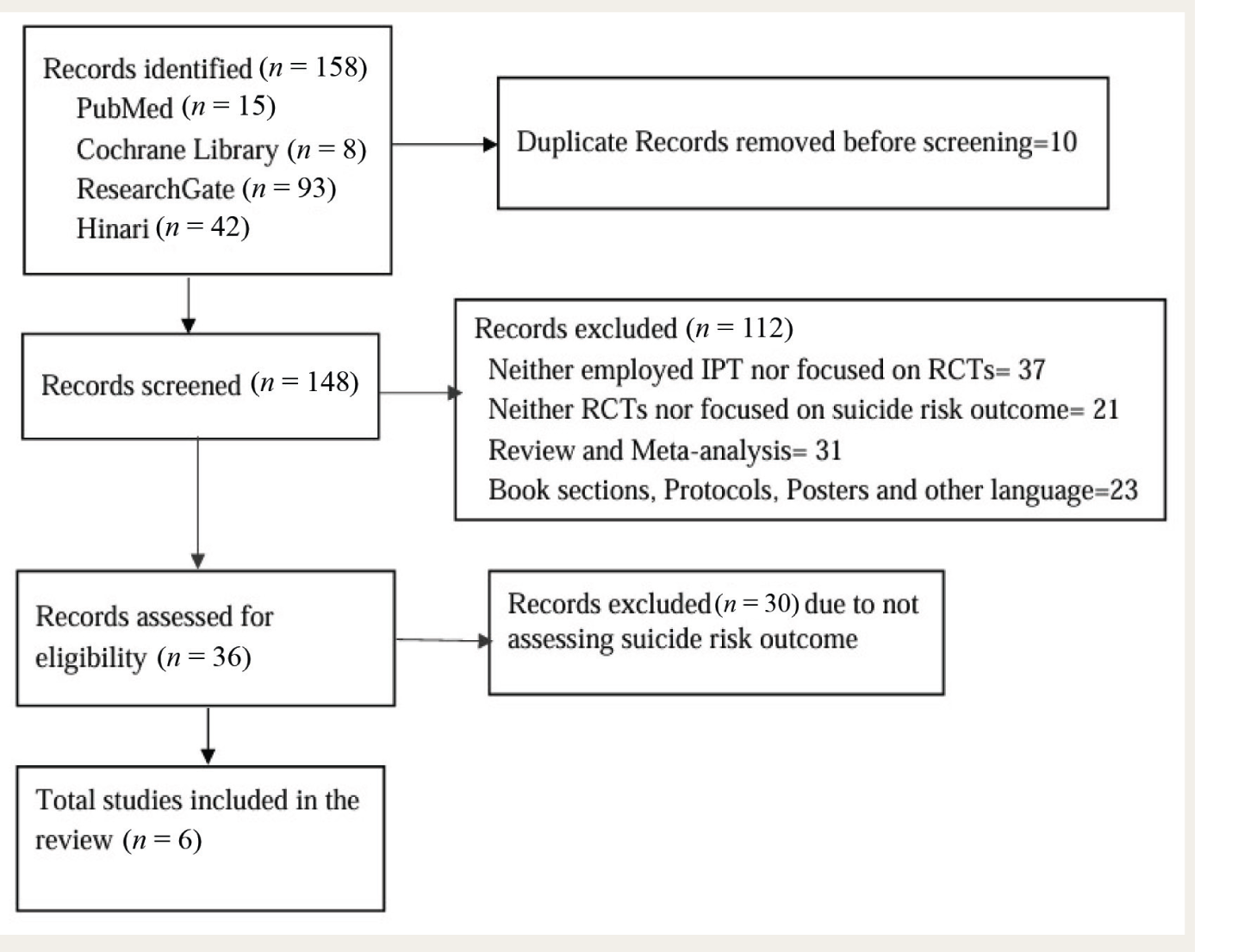
IPT, interpersonal psychotherapy; RCT, randomized controlled trial.
Descriptive Summary of Studies.
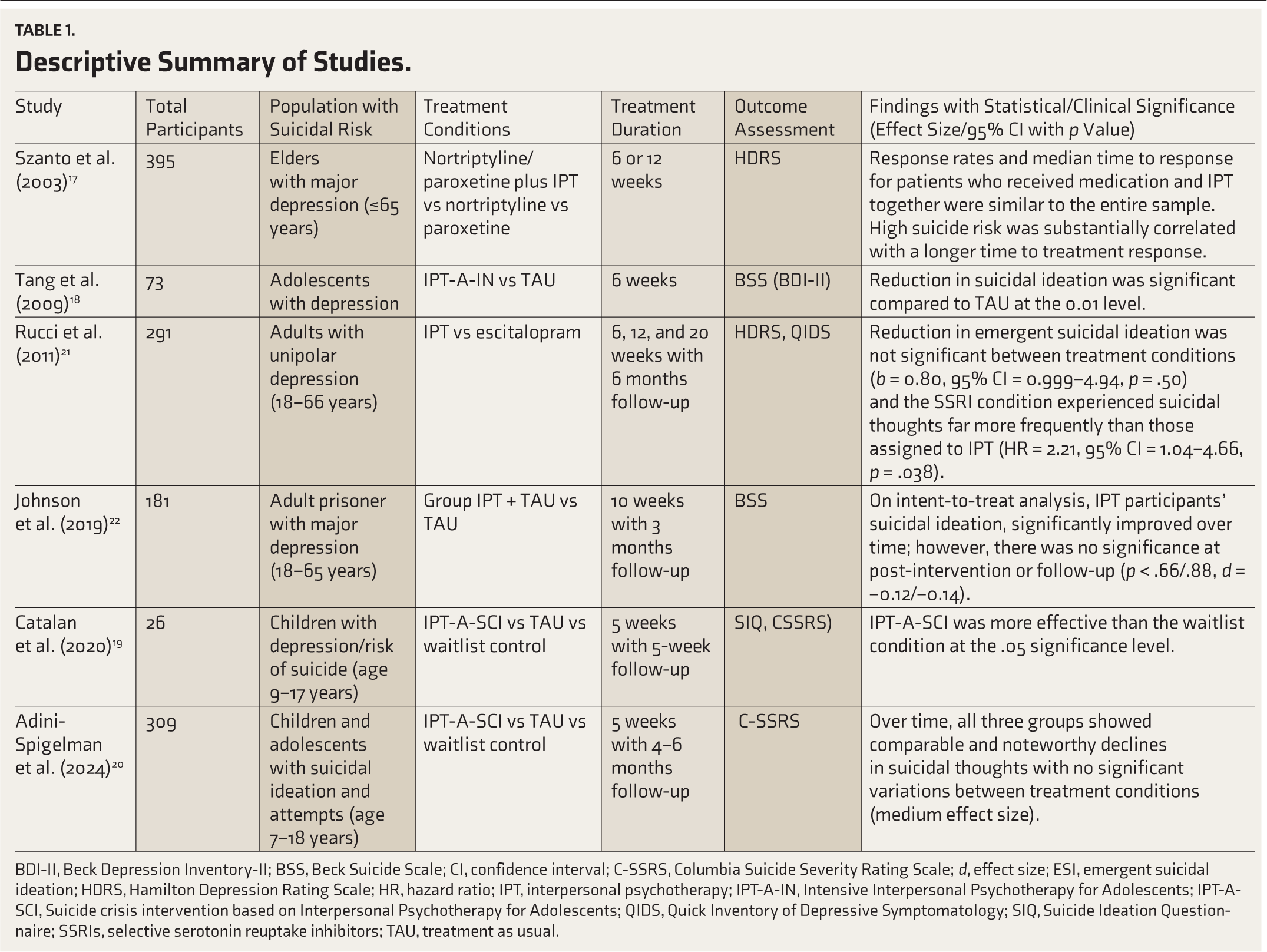
BDI-II, Beck Depression Inventory-II; BSS, Beck Suicide Scale; CI, confidence interval; C-SSRS, Columbia Suicide Severity Rating Scale; d, effect size; ESI, emergent suicidal ideation; HDRS, Hamilton Depression Rating Scale; HR, hazard ratio; IPT, interpersonal psychotherapy; IPT-A-IN, Intensive Interpersonal Psychotherapy for Adolescents; IPT-A-SCI, Suicide crisis intervention based on Interpersonal Psychotherapy for Adolescents; QIDS, Quick Inventory of Depressive Symptomatology; SIQ, Suicide Ideation Questionnaire; SSRIs, selective serotonin reuptake inhibitors; TAU, treatment as usual.
Component and Working Hypothesis of IPT Across Included Studies
In the included studies, IPT was introduced to reduce depressive symptoms with a specific focus on evaluating suicidal risk outcomes. Traditional IPT typically consisted of 12–16 sessions encompassing four interpersonal areas: grief, role transition, interpersonal dispute, and deficit. However, its quality of modifiability has extended to ultra-brief IPT (or IPT-A-SCI), which consists of five sessions addressing the safety plan, interpersonal circle, interpersonal, emotional, and behavioral coping strategies, and relapse prevention focusing on the identified interpersonal problem area. The authors attempted to indicate the working hypotheses or causal pathways of ultra-brief IPT. Szanto et al. and Tang et al. briefly described the foci of the intervention.17,18 Tang et al. precisely described the focus components and working hypothesis of IPT, as well as the techniques used to reduce suicidal risk. Catalan et al. and Adini-Spigelman et al. provided precise details about the IPT techniques used to address those interpersonal areas.19,20 Please refer to Table 2.
Components of Interpersonal Psychotherapy Across Six Studies.

IPT, Interpersonal Psychotherapy; IPT-A-IN, Intensive Interpersonal Psychotherapy for Adolescents; IPT-A-SCI, Suicide crisis intervention based on Interpersonal Psychotherapy for Adolescents.
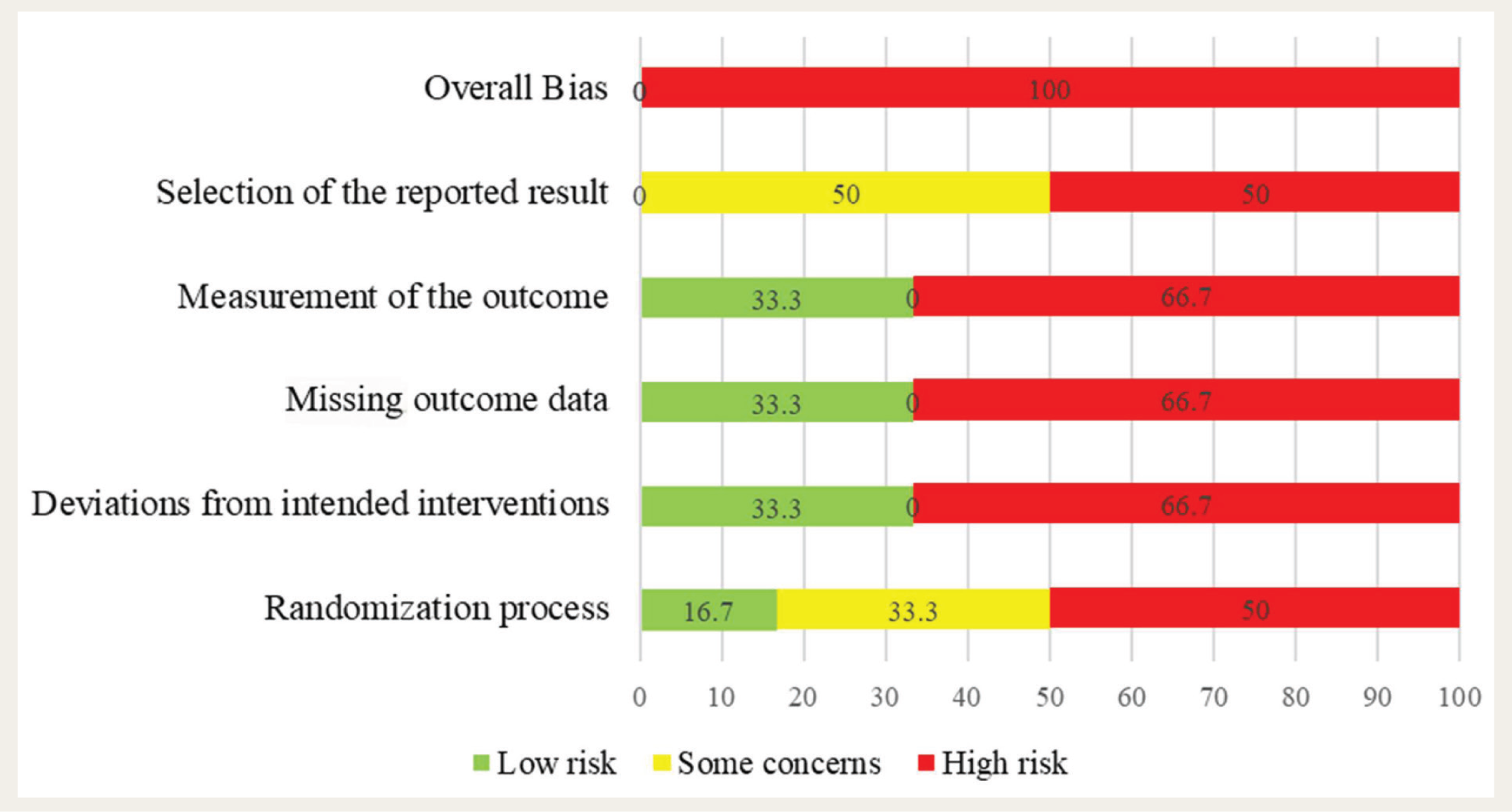
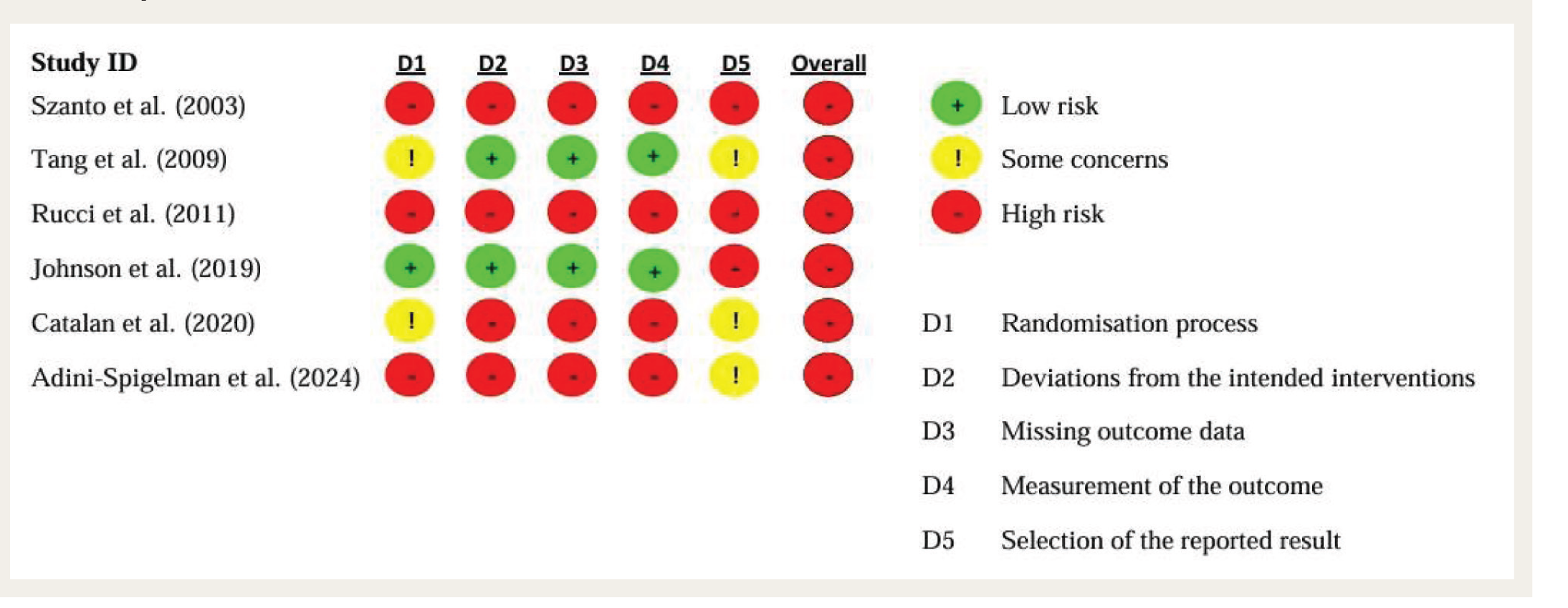
Figures 2 and 3 illustrate the risk of bias summary and graph across the included studies. The following observations can be drawn: Some concerns of bias were shown in the randomization process (33.30%) and selection of reported results (50%). Similarly, a high risk of bias (50%) was found in both the randomization process and selection of reported results, due to insufficient detail about the randomization, concealment, imbalanced baseline characteristics, and missing multiple appropriate analyses. A significant high risk of bias (66.67%) in each domain was observed, including deviations from the intended intervention, missing outcome data, and measurement of outcome data. This was due to insufficient details about imbalanced baseline characteristics, lack of awareness of the intended intervention, missing appropriate analysis of randomized participants, missing follow-up data, and absence of appropriate analyses.17,20,21 Only a few studies had a low risk of bias in deviation from the intended intervention, missing outcome data, and measurement of outcome, due to adherence to rigorous methodological standards.18,22 Overall, the included studies demonstrated a high risk of bias across multiple domains.
Graph Across Included Studies.
Summary for Each Risk of Bias Area Across Studies.
Discussion
The results of this review revealed mixed findings across the included studies. As summarized in Table 1, most studies assessed outcomes using the Hamilton Depression Rating Scale, Beck Suicide Scale, and Columbia Suicide Severity Rating Scale (C-SSRS). While these studies suggest an overall decrease in suicidal ideation over time, no significant differences were observed between treatment conditions in several studies.17,20–22 In this condition, subgroup analysis may determine whether any differences exist in patient interventions for specific subgroups, as many factors influence the outcome. In a related pioneering study, IPT was found to be more effective compared to another comparator for more severely depressed patients. 23 Another subgroup analysis of a meta-analysis suggests that IPT is found to be more effective in adolescent depression compared to adult depression in improving social functioning. 24 Two studies reported post-intervention outcomes, showing a significant difference in the reduction of suicidal ideation between treatment conditions. However, neither study reported actual treatment effects with a 95% CI, limiting the interpretation of clinical significance for IPT18,19 in this population. Two studies compared IPT with selective serotonin reuptake inhibitors (SSRIs) and suggested comparable effectiveness.17,21 This represents a minimal number of studies. However, an interesting finding was that longer periods of suicidal ideation in the SSRI sequence were associated with twofold times more increased risk of emergent suicidal ideation compared to the IPT sequence. 21 However, no other studies reported harms that could reveal the unintended effects of the intervention. Conversely, Tang et al. suggested that IPT was significantly more effective than treatment as usual (TAU) in reducing suicidal ideation among adolescents. However, this study was conducted on school-going adolescents in a community setting. 18 Catalan et al. suggested the effectiveness of five sessions of IPT-A-SCI with 5 weeks of follow-up, indicating better outcomes than the waitlist control. 19 However, follow-up outcome analyses were missing in their reporting. Adini-Spigelman et al. randomized individuals with a high risk of suicide into experimental conditions and indicated that there was no significant difference in suicidal ideation and behavior compared to TAU and waitlist control after the intervention.19,20 However, using enhanced usual care in the control group or adaptive randomization could reduce the selection bias. Both Catalan et al. and Adini-Spigelman et al. overlooked the scoring and analysis of C-SSRS, as per the guidelines of the Food and Drug Administration Advisory Committee, which suggested 11 categories of the C-SSRS (five subtypes of suicidal ideation, five subtypes of suicidal behaviors, and one subtype of self-injurious behaviors without suicidal intent). These categories were not displayed in the results, such as the proportion of different suicidal behavior and their lethality, which are important clinically and for risk analysis purposes. 25 High dropout rates were observed, suggesting that patients with suicidal risk have a higher chance of dropping out during treatment.17,19,20 Therefore, researchers should focus on intention-to-treat analysis, 26 which compares the randomized groups without bias to avoid misleading interpretations about the effectiveness of given interventions. Two studies reported a moderate effect size (Cohen’s d) for the effectiveness of IPT but lacked accompanying 95% CIs, making it unclear whether IPT had a significantly greater treatment effect compared to other conditions.20,22
Tang et al. precisely described the components and working hypothesis of intensive interpersonal psychotherapy for adolescents in their procedure, as well as the foci of intervention in which 90% of adolescents at risk of suicide had interpersonal conflicts. This may be one of the primary components of IPT during intervention among individuals with suicidal risk, 18 and could be helpful in generalizing the most important foci of intervention in individuals at risk of suicide if other studies also described these foci of intervention. This is recommended by the extended Consolidated Standards of Reporting Trials (CONSORT) guidelines for social and psychological interventions, which advise providing precise details about intervention.27,28 However, most of the studies were published before these guidelines. Catalan et al. and Adini-Spigelman et al. briefly described the causal pathways and techniques used in IPT-A-SCI intervention.19,20 Most included studies also exhibited a high risk of bias, with inadequate reporting of randomization methods, allocation sequences, and other key methodological details.17–21
Due to incomplete reporting in terms of statistical significance between treatment conditions and misleading interpretation of the effectiveness of IPT—by presenting results only by p values without focusing on 95% CIs and receiver-operating characteristic (ROC) curves, it is most important to promote the reporting of clinically interpretable effect sizes and associated 95% CIs, either in addition to or instead of statistically significant p values.27,29–31 No studies assessed the risk ratio, such as the relative risk, which could determine the percentage reduction in suicide risk due to the intervention compared to other treatment conditions. This could suggest minimal clinical significance for mental healthcare professionals, who could then decide on the importance of IPT. Many studies did not report effect sizes or perform subgroup or adjusted analyses that could express the effectiveness of IPT in terms of clinical relevance compared to TAU and other comparators. The effectiveness of IPT was found to be compromised due to a lack of adherence to standard guidelines such as Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) and CONSORT,25,28,29,32 resulting in incomplete reporting of results, which limits the generalizability of IPT’s effectiveness among individuals at risk of suicide (refer to Table 1 and Supplementary File 2). Given the variability in outcomes, it is important to consider patient preferences when selecting a treatment course, as individual factors may influence therapeutic results. Future studies should prioritize robust methodologies, including reporting effect sizes with 95% CIs and performing subgroup analyses to better evaluate the clinical significance of IPT compared to TAU and other treatment modalities.
Limitations
Participant selection was restricted to individuals with non-psychotic depressive disorders who were motivated to engage in treatment, limiting generalizability to broader clinical populations. The review did not account for variations in depression severity or the spectrum of suicidal risk—such as ideation with or without intent, actual attempts, or aborted and interrupted attempts—which contribute to clinical heterogeneity and interpretive uncertainty. Methodological shortcomings were common, including insufficient reporting of randomization procedures, lack of blinding, omission of intent-to-treat analyses, and unclear allocation concealment, resulting in a high or unclear risk of bias in most studies. Additionally, few studies specified the therapeutic focus or components of IPT, such as grief, role transitions, interpersonal disputes, or deficits. Clinical outcomes were often reported solely as p values, without effect sizes, CIs, or ROC metrics, limiting their interpretability. The absence of subgroup analyses precluded examination of IPT’s differential efficacy across demographic or clinical subgroups. High dropout rates, particularly among individuals with elevated suicide risk, introduce attrition bias and compromise the reliability of findings. Moreover, most studies lacked long-term follow-up data, restricting conclusions about the durability of treatment effects. Lastly, the review was constrained by a limited database search conducted by a single author, increasing the risk of selection bias and precluding a comprehensive systematic review or meta-analysis.
This review identifies several priorities for future research on IPT for individuals at risk of suicide. First, studies should rigorously follow established methodological guidelines, such as SPIRIT and CONSORT, as well as current good clinical practice standards, to ensure transparency, replicability, and comprehensive reporting. Second, outcomes should be presented using clinically meaningful metrics—such as effect sizes and 95% CIs—to convey the practical significance of IPT beyond p values. Third, the standard of usual care must be enhanced, particularly for individuals at acute risk; this includes integrating structured psychological support, such as professional crisis counseling and suicide prevention helplines, during the study period to safeguard participant welfare. Fourth, incorporating personality assessments—especially for individuals with self-injurious or impulsive traits—may allow for more tailored interventions and improved treatment outcomes. Fifth, researchers should clearly articulate the theoretical framework and components of IPT, including its interpersonal focus areas and delivery strategies, to strengthen the conceptual fidelity of the intervention. Sixth, future trials should incorporate subgroup and adjusted analyses to explore differential treatment effects by severity, age, or other relevant variables, facilitating personalized therapeutic approaches. Seventh, high dropout rates and missing data should be addressed using intention-to-treat analyses, which also support the estimation of clinically significant outcomes such as relative risk. Lastly, future reviews should employ rigorous systematic methods and consider advanced approaches—such as network meta-analyses and stratified analyses to comprehensively evaluate IPT’s comparative and population-specific efficacy.
Conclusions
The findings of this review highlight the limited evidence regarding the clinical significance of IPT in reducing suicidal risk. While some studies suggest potential benefits, the lack of consistent reporting on clinically interpretable metrics such as risk ratios, effect sizes, and CIs makes it challenging to determine the effectiveness of IPT in this context, indicating the need for further conclusive and evident research.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
The author thanks the faculty members (Dr Kumari Sandhya, Professor of Anatomy; Dr S. B. Singh, Additional Professor of Preventive and Social Medicine; Amit Kumar, Associate Professor of Laboratory Medicine; Dr Ganesh Chauhan, Associate Professor of Genetics and Genomics) of Rajendra Institute of Medical Sciences (RIMS), Ranchi, who always encouraged the preparation of review articles during the PhD coursework and also provided training in systematic review and meta-analysis. The author also thanks Adini-Spigelman et al. for sending the link to their full-text article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Prior Presentations
This review has not been presented at any conference or scientific event.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.