
Abstract
Background:
Many laws and acts related to mental health play a vital role in delivery of mental health services for persons with mental illness (PMI). In India, the Mental Health Act of 1987 (MHA, 1987) was replaced with the Mental Healthcare Act, 2017 (MHCA, 2017). However, there were numerous barriers and challenges in the proper implementation of the Act, and there is a paucity of research on the extent of implementation of the new Act. This study assessed the admission patterns of PMI admitted during the transition phase from MHA, 1987 to MHCA, 2017.
Methods:
A retrospective chart review was done on admissions through the Hon’ble Magistrate’s orders and mentally ill prisoners at a tertiary care psychiatric hospital in first four years (2018–2022) after MHCA enactment. Details regarding the admission, legal variables, and clinical variables were taken from case records.
Results:
Our study included 354 patients, including 222 (62.7%) admissions through the Hon’ble Magistrate’s orders and 132 (37.3%) mentally ill prisoners. Paranoid schizophrenia (n = 162, 52.9%) was the most common diagnosis and modified electroconvulsive therapy was given to 36% (n = 120) of patients. Total 115 (52%) patients were admitted under MHA, 1987, and 38 (17%) were admitted under MHCA, 2017, and no Act was mentioned in the case of 68 patients (30.6%).
Conclusions:
This study highlights the extent of change in admissions of PMI after MHCA, 2017 enactment and sheds light on probable barriers for delay in the proper implementation of the Act. Our study emphasized the need for awareness about MHCA for all stakeholders as adherence to the proper procedure is necessary while admitting patients in closed wards and prison wards of the psychiatric facility.
This study reviews admissions ordered by Hon’ble Magistrates and the Superintendent of Prisons. We found more admissions under the MHA, 1987 Act than under the MHCA, 2017 Act, with other cases lacking specific legal references. Our findings highlight the incomplete implementation of the MHCA, 2017, in its first five years and emphasize the need for improved awareness and coordination among stakeholders.Key Messages:
The provision of early and safe treatment for people with mental illnesses (PMI) is essential for reducing long-term morbidity and regaining socio-occupational functioning. However, facilitating treatment for PMI has abundant challenges. Apart from well-known obstacles, mental health legislation and regulations play a crucial role in facilitating the delivery of mental health services across nations. 1 In India, many mental health laws pertaining to the treatment, care, isolation, and detention of PMI have been passed over the years. Among these, the Mental Health Act (MHA), 1987 was implemented to treat and care for PMI, who primarily lack mental health capacity. Under this Act, a reception order from the Hon’ble Magistrate is required for the admission of mentally ill, homeless, wandering, and mistreated patients into a psychiatric facility. 2 In addition, the MHA, 1987 allows the admission of prisoners when the mental capacity of the prisoner to understand the legal proceedings is questioned. However, MHA, 1987 has several setbacks, such as perceived coercion among PMI, involuntary admission, a threat to rights, and autonomy of treatment choices for PMI.
To overcome the limitations of MHA,1987, the Mental Health Care Act, 2017 (MHCA, 2017) was passed in India, and it came into effect in May 2018. The new Act empowers PMIs of their rights, upholds their autonomy, and mandates them to seek informed consent during all mental healthcare procedures. This Act has brought several amendments and new changes to MHA,1987, with significant ones including the removal of involuntary admission and the introduction of advanced directive, nominated representative (NR), and mental health review boards (MHRB). Independent admission (Section 86), supported admission (Section 89), and emergency admission (Section 94) are the provisions for the admission of PMI with impaired mental health capacity as per the MHCA, 2017 Act. Section 102 deals with the admission of PMI to a mental health establishment (MHE) by the Hon’ble Magistrate for the assessment and treatment for not more than 10 days, and a mental health professional (MHP) must submit a report to the Hon’ble Magistrate by the end of this period. Section 103 deals with the admission of prisoners for the treatment of mental illness through orders of the Superintendent of prison or Judicial Magistrate. Under this Section, any PMI must be transferred to a psychiatric ward in the medical wing of the prison or an MHE with prior permission of the Board. The medical officer of the prison is required to send a report to the MHRB certifying that there are no PMI in prison once every three months. 3–5
Though it has been a half decade since the implementation of MHCA in 2017, many MHEs are still in the early stages of translating the Act into practice. 6 Hence, it is worthwhile to assess the admission patterns and the extent of change in service delivery in the early years of the implementation of MHCA, 2017. Research on the current admission trends and management of PMI will help in allocating human resources, planning adequate facilities, and involvement of all stakeholders. Previous studies on MHCA, 2017 highlighted the scope, legal aspects, challenges, liabilities, and cost estimation in implementing new Acts.7–11 However, there is a paucity of research about the extent of MHCA’s implementation. The objective of the current study was to assess the admission patterns of PMI admitted during the transition phase from MHA, 1987 to MHCA, 2017.
Methods
The current study was a retrospective chart review of PMI admitted through the Hon’ble Magistrate’s orders and mentally ill prisoners at a government tertiary care psychiatric hospital. The study was approved by the ethics committee of the institute, and permission was taken from the hospital authority. Case records of persons admitted between June 1, 2018, and May 31, 2022, were retrieved and reviewed using a semi-structured proforma for details about sociodemographic, admission procedure, Hon’ble Magistrate’s orders, duration of admission, clinical diagnosis, and primary methods of treatment. The Hon’ble Magistrate referred the PMI on an outpatient basis regarding their psychiatric or psychological assessment and those who had not received any inpatient care were excluded.
Statistical Analysis
Data were tabulated and analyzed using the Statistical Package for the Social Sciences, version 25 (SPSS-25). Mean and standard deviation were computed for the continuous variables, whereas frequency and percentages were calculated for the categorical variables.
Results
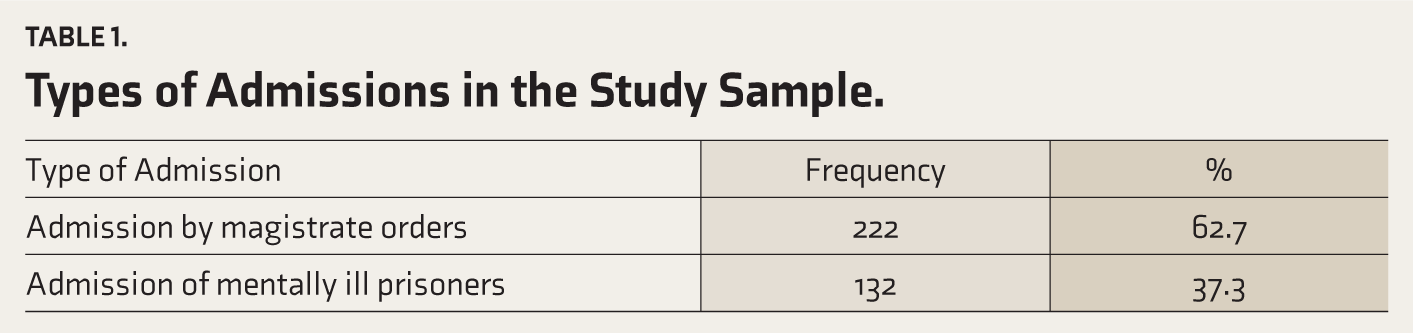
During the study period, 354 patients were admitted through the Hon’ble Magistrate’s orders and prisoners with mental illness. Among these, 222 admissions were made through the Hon’ble Magistrate’s orders, which included 178 (80.2%) males and 44 (19.8%) females. The remaining 132 admissions were of Prisoners with mental illness, which included 123 (93.2%) males and 9 (6.8%) females. Among prisoners, 88 (66.7%) were remand prisoners, and 44 (33.3%) were convict prisoners, as shown in Table 1. In both admission procedures, the majority were males compared to females. The age group of patients ranges from 17–75 years, with a mean age of 33.8 (SD ± 9.7) years. In terms of annual admissions, there were 46 admissions from June to December 2018, 67 admissions in 2019, 82 admissions in 2020, 117 admissions in 2021, and 42 admissions in the last six months of the study period, that is, January to May 2022. It was noted that the number of admissions increased annually.
Types of Admissions in the Study Sample.
Paranoid schizophrenia (n = 162) was the most common diagnosis, followed by bipolar affective disorder (n = 54), mental retardation with comorbidities (n = 26), and substance use disorders (n = 24). Twenty-one patients admitted were found to have no primary psychiatric disorder on diagnostic evaluation, and these were the patients admitted by the Hon’ble Magistrate’s order, who were either referred for evaluation or those pledging insanity defense for their alleged Indian Penal Code (IPC) charges. Modified electroconvulsive therapy (mECT) was given to 33.8% (n = 120) of the total patients in our study. A combination of mECT and antipsychotics (n = 77, 21.7%) was the more commonly used treatment method, followed by a combination of antipsychotics and mood stabilizers (n = 43, 12.1%). The admission period in our study ranges from one month to more than six months, with a mean duration of 2.76 (SD ± 2.2) months. The majority of patients had admission for one-month duration (n = 104), and only three patients had an admission duration of six months. Out of the total sample, 31 (7.1%) patients were rereadmitted during the study period. There were seven deaths during the study period (three due to suicides and four due to severe medical illnesses).
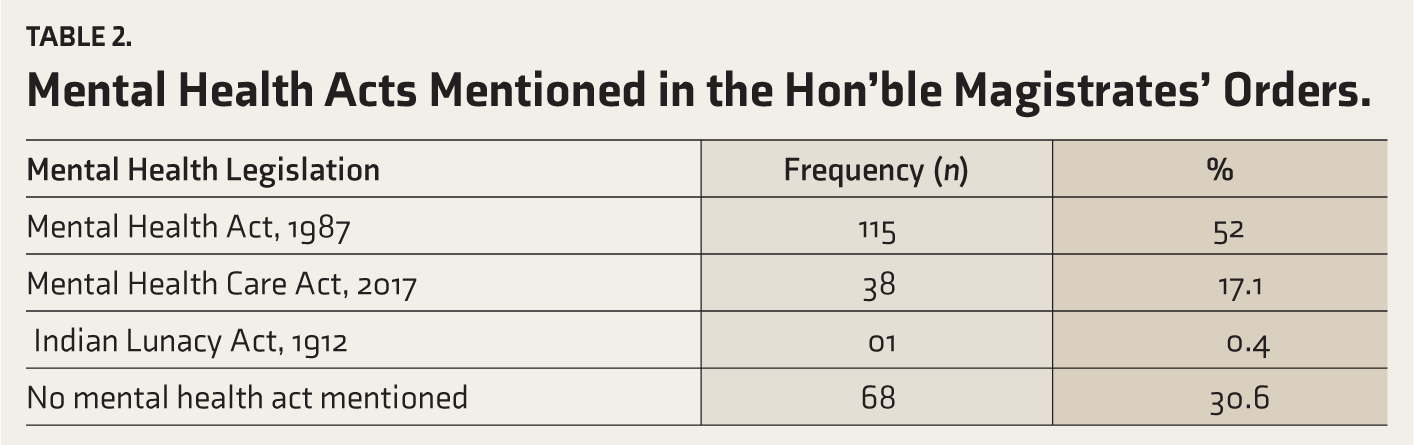
A higher number of PMI were admitted under the MHA, 1987 (n = 115) (52%), followed by the MHCA, 2017 (n = 38) (17%) (Table 2). In 68 cases (30.6%), no Act was mentioned. In the case of admissions as per MHCA, 2017, Sections 100–104 and 115 were mentioned in the Hon’ble Magistrate’s orders. Similarly, Sections 20, 22–25, 28, 34, and 40 were mentioned in the Hon’ble Magistrate’s orders issued as per MHA,1987. In the admission of mentally ill prisoners, the Prison Superintendent referred 80% of patients, and the Hon’ble Judicial Magistrate referred 20% of patients. Among them, the majority were charged under the IPC Section 302 (n = 43), followed by Section 307 (n = 9), Section 304 (n = 7), Section 20 of the Narcotic Drugs and Psychotropic Substances Act (n = 7), Section 7 of the Protection of Children from Sexual Offences Act (n = 4), and Section 3 of the Prevention of Damage to Public Property Act (n = 3). It was noted that the reasons for transferring prisoners to psychiatric hospitals include the need for the treatment of behavioral problems such as violence, suicidality, and substance use, certification regarding fitness to stand trial, acute exacerbation of existing psychiatric illness, review of psychiatric medications, and insanity defense.
Mental Health Acts Mentioned in the Hon’ble Magistrates’ Orders.
Discussion
This study comprised PMI admitted through various channels, among which two-thirds of patients were admitted through the Hon’ble Magistrate’s orders. Such a large number of admissions can be explained by the fact that our hospital serves as a tertiary care center for mental health and offers custodial care. Most of the patients were in the age group of 20–40 years, consistent with previous Indian studies.13–15 In our study, the majority of patients were brought by police escort alone, and only a few were accompanied by family members at the time of admission. Many of the patients were wandering mentally ill persons who were brought by police or private NGOs through the Hon’ble Magistrate’s orders. 16 The admissions of mentally ill prisoners were smaller in proportion than those of the Hon’ble Magistrate Order’s admissions in our study, which might be due to the referral of PMI to nearby government general hospitals for psychiatric care, and only those who require custodial care would be referred to a tertiary care hospital.
Our study showed an upward trend in admission rates from 2018 to 2021. This could also be due to the COVID-19 pandemic, which affected every aspect of life, especially mental health. During the pandemic, the high psychological stress altogether with barriers to mental healthcare access could have resulted in poor medication compliance and high relapse rates among PMI or may have increased the severity of mental illness. 17 All these factors may have accounted for a higher admission rate during this period. The majority of patients in our study had psychosis as a diagnosis, with a significant number of readmissions, which might be due to a lack of insight, poor social support, and poor treatment adherence. 18 Nearly one-third of all patients received mECT, demonstrating the severity, chronicity, and treatment resistance of mental illness. The longer mean duration of treatment of 2.76 months signifies the severity of mental illness in our study, and these findings are consistent with the previous study. 13
Our study found that despite mentioning mental health Acts in some Hon’ble Magistrate’s orders, appropriate sections were not mentioned, which is consistent with findings of earlier research in terms of mentioning pertinent legislation and sections.19,20 Even though the Mental Health Act of 1987 forbids the use of derogatory and offensive terms like “insane,” “lunatic,” and “asylum,” these terms were used in referral letters and the Hon’ble Magistrate’s orders, and the use of such terminologies should preferably be avoided in the future while issuing the Hon’ble Magistrate’s orders. Over 87% of admitted prisoners received a psychiatric diagnosis, demonstrating the high rate of psychiatric morbidity in prisons. Assault and murder were the most frequent charges in the profile of alleged offenses, and these findings are consistent with the previous studies.13,15,21
The MHRB, which is an essential part of MHCA, 2017, has a role in the registration and review of advance directives, the appointment of NRs, resolution of MHP and MHEs’ objections, prison visits, and human rights protection.9,22 When someone was brought without caregivers, MHRB designates an NR. The MHRB has a crucial role to play when there is a conflict with the consent-related issue in mental healthcare and treatment decisions. Unfortunately, the MHRB is still in the developmental phase at the time of the study, which could have delayed the proper enactment of MHCA, 2017.9,22,23
In our study, the majority of admissions were done as per the old MHA, 1987, even after five years of the enactment of the new MHCA, 2017. This finding points to the new Act’s incomplete implementation, which might be due to several factors, such as the MHRB’s unavailability, lack of awareness among stakeholders like police officers and Hon’ble Magistrates, as well as lack of strict practical guidelines and appropriate training to comply with the new mental healthcare Act. A similar situation occurred in the early years of the implementation of MHA, 1987 when many were adhering to the Indian Lunacy Act of 1912 instead of MHA, 1987. Then the honorable state High Court intervention hastened the enactment of MHA, 1987. Meanwhile, there is a need to increase awareness and understanding among the stakeholders regarding the new Act. The implementation of MHCA, 2017 across southern India is at different stages, with three out of five states proceeding with the formation of MHRBs. 9 In the state of Andhra Pradesh, initial steps to form the MHRB were taken. However, they were not completely operational at the time of conducting our study. Another factor leading to the delayed implementation of MHCA of 2017 could be a lack of financial preparedness and resolution to execute the new Act, as the expected yearly investment in mental healthcare is far higher than the allocated funds. 10
Strengths of the Study
To the best of our knowledge, our study is the first of its kind in published literature to assess admission patterns with a large study sample and a long study period. Our study highlighted the probable barriers to delay in implementing MHCA, 2017 and brought out the necessary measures for effective implementation.
Limitations
Our study was retrospective, whereas a longitudinal, prospective study would have been more effective and accurate. We did not assess the extent of awareness among the stakeholders about the new MHCA Act.
Conclusion
Our study assessed the extent to which the admission procedure for PMI changed after MHCA, 2017 came into effect. The majority of admissions were done under MHA,1987, rather than MHCA, 2017, indicating the need for all stakeholders to be aware of the new mental health legislation. MHRBs also need to be fully operational to facilitate adherence to the proper procedure for admitting patients in closed wards and prison wards of psychiatric facilities.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Ethics Committee of Andhra Medical College with the approval number 46/IEC AMC/SEP 2022.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Informed Consent
All participants involved in study provided informed consent for their participation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.