
Abstract
Background:
The brain-derived neurotrophic factor (BDNF) has an important role in the growth of neurons and synaptic transmission. The BDNF gene Val66Met polymorphism (G/A) is associated with depression, but findings have not been consistently replicated. This study adopts a case-control design with an aim to investigate the association of Val66Met polymorphism and peripheral BDNF (serum) levels in patients of major depressive disorder (MDD) and healthy individuals (controls).
Materials and Method:
This study adopts an observational, case-control design with a total of 174 participants. Cases (n = 87) were currently depressed, having Diagnostic and Statistical Manual of Mental Disorders (DSM-5) MDD, without psychiatric comorbidity. Controls (n = 87) comprised healthy individuals with no family history of psychiatric illness. The cases were evaluated using the NIMH-Life Chart Method, Hamilton Depression Rating Scale (HAM-D), Clinically Useful Depression Outcome Scale (CUDOS), and Clinical Global Impression (CGI). TaqMan assay was used for genotyping, and serum BDNF was measured using Enzyme-linked immunosorbent assay (ELISA).
Results:
The case mean age was 35.32 ± 11.69 years (52% females) and comparable to controls. Allelic distribution was 33% (Met), and genotypic distribution was 17% (Met/Met), 32% (Val/Met), and 51% (Val/Val) for cases. The genotypic distribution did not differ across study groups. Serum BDNF was significantly lower in MDD cases as compared to controls (p < .001). The serum BDNF levels were comparable across the genotypic groups among cases.
Conclusion:
The Val66Met polymorphism has not been associated with a risk for MDD and, interestingly, did not influence the BDNF levels (serum). Significantly low BDNF levels were found in MDD cases. The study findings show that factors other than Val66Met gene polymorphism have a role in modulating serum BDNF levels.
The current study adds to limited reports on allelic and genotypic distribution of Val66Met in a sample from India. The Val66Met polymorphism is not associated with a risk for MDD and did not influence serum BDNF in depressed patients. Cases had significantly low BDNF levels as compared to controls, irrespective of Met carrier status.Key Messages
Major depressive disorder (MDD) clinical symptoms include discrete episode/s lasting two weeks or more, with changes in affect, energy, psychomotor activity, cognition, and neurovegetative functions accompanied by significant distress or impairment in functioning.1–4 Its lifetime prevalence varies from 10-20% and is among the leading causes of disability globally as well as in India.5–7
Studies reported an association of Val66Met polymorphism present along the brain-derived neurotrophic factor (BDNF) gene with MDD8–10; however, several other studies report negative findings as well.11,12 Few recent reports point to a moderating effect of Val66Met polymorphism on the clinical characteristics of major depression, like age of onset and lifetime episodes of depression. 13 Research indicates a blunted gene expression in the carriers of Val66Met gene polymorphism and low peripheral BDNF values among depressed cases. 14
The BDNF has a vital role in the growth of neurons and synaptic transmission14,15 and is encoded by the BDNF gene present on chromosome 11. A single nucleotide polymorphism (SNP) (rs6265) at nucleotide 196 (G/A) of the BDNF gene causes the replacement of Valine by Methionine on position 66 of the 5’pro BDNF sequence. Mechanistically, the Val66Met polymorphism has been linked to a decreased activity-dependent secretion of hippocampal BDNF. 5 As the activity-dependent synaptic secretion of the BDNF is critical for neuronal plasticity, this polymorphism is linked with several other neuropsychiatric disorders. As BDNF crosses the blood-brain barrier, 16 therefore its peripheral concentrations can reflect the brain concentrations. The BDNF levels (serum) are significantly low in cases with major depression compared with the healthy controls. 17 Further, low levels of BDNF have been linked to both recurrence as well as severity of depressive episodes. 18
Limited information is available on Val66Met in MDD patients from India. Three prior studies have assessed Val66Met polymorphism in Indian patients with MDD, of which two included a healthy control group.19–21 Other Indian studies of BDNF levels among MDD cases have not assessed Val66Met polymorphism.22,23 This study adopts a case-control design with the aim of investigating the association of Val66Met polymorphism of the BDNF gene and serum BDNF in major depression cases and healthy controls.
Materials and Method
This was an observational case-control study carried out at a tertiary care hospital in India. The Institute Ethics Committee (IEC) approved the study. Informed consent (written) was obtained from study participants. The STROBE case-control checklist has been used while writing the article. 24
The estimated sample size of the current study was as per the reference study. 13 A sample size of 44 was required in each group (wild and mutant) to achieve 80% power and 95% confidence level. As per the feasibility, a total of 87 cases were included. Adult (18–60 years) patients visiting the out-patient or in-patient facility at the Department of Psychiatry were enrolled between March 2021 and December 2021 in the study as per the selection criteria. Patients diagnosed with MDD as per Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria, 3 depressed with a score > 7 on the Hamilton Rating Scale for Depression (HAM-D) 24 were enrolled in the study. The diagnosis was made by a qualified psychiatrist of the department of psychiatry of our institute. Patients with comorbid psychiatric or substance use disorder, apart from nicotine dependence or any significant medical or neurological illness, were excluded. Patients were also excluded if they had biological relatedness within the study sample or had undergone electroconvulsive or other neuromodulatory treatment in the past six months. The control group comprised an equal number of biologically unrelated healthy individuals enrolled from the same setting, with no known medical or psychiatric disorder in self apart from nicotine use and no known psychiatric disorder up to second-degree relatives.
Study Tools
A semi-structured clinical form was prepared to gather details from cases and controls. Cases were also assessed using the 17-item HAM-D, 25 the Clinically Useful Depression Outcome Scale (CUDOS), 26 and the Clinical Global Impression (CGI). 27 The NIMH-Life Chart Method 28 was used to gather details of lifetime episodes in cases.
A total of 5 ml of venous blood sample was collected, of which an aliquot (2 ml) was collected in EDTA tubes for genotyping, while a 3 ml blood sample (plain vial) was used for serum separation to estimate BDNF levels. The samples were stored at –20°C until further analysis, as discussed below.
Val66Met Polymorphism
Extraction of Deoxyribonucleic acid (DNA) from blood was carried out using a DNA extraction kit, QIAamp from Qiagen GmbH (Germany). The Val66Met polymorphism for SNP rs6265 was carried out using TaqMan 5’ nuclease assay (C__11592758_10, Thermofisher Life Sciences, India). A 20 µl volume reaction mixture was used for Polymerase chain reaction (PCR). The mixture consisted of 20 ng/µl DNA, TaqMan super mix, and primers and probes (0.1–1 µM). The PCR reaction was carried out in a Real-Time PCR machine QS12K Flex (Thermofisher, India Pvt Ltd). The genotyping was done using the allelic discrimination assay with QuantStudio 12K flex optical system software. The researchers performing the assay were blinded about the clinical details of the participants.
Serum BDNF Estimation
The measurement of BDNF levels (serum) was done using a Human BDNF Enzyme-linked immunosorbent assay (ELISA) kit by BIOCODON (Kansas, USA). All the steps were performed according to the manufacturer’s instructions. Serum BDNF measurement was carried out using an ELISA Reader (M200 PRO, Multimode ELISA Reader, TECAN, Austria). Finally, according to the standards’ optical density values, the serum BDNF levels (ng/ml) of the samples were calculated.
Statistical Analysis
The analysis was done with Statistical Package for Social Sciences (SPSS) version 26. No missing data was detected. Descriptive statistics are used for clinical variables in the study sample. Shapiro Wilk was used to assess the normality of the data.
Allelic and genotypic distribution across the cases and controls was assessed using the Chi-square test. Association between genotype, serum BDNF, and clinical variables was assessed using Spearman-Rho, Chi-square, and Mann-Whitney U test as applicable. A significant p value (two-tailed) of <.05.
Results
Overall, the investigator approached 90 MDD cases meeting DSM-5 criteria, of which two did not meet selection criteria and one did not consent to be sampled. A total of 93 individuals were approached for participation as controls, of which six did not meet the selection criteria.
Finally, the study included 174 participants, with 87 cases and 87 healthy controls.
Demographic and Illness Profile
The age (mean) of the MDD cases was 35.32 ± 11.69 years (48% males, 52% females). Age and gender distribution were comparable across cases and controls (Table 1).
Clinical Profile of Cases and Controls.
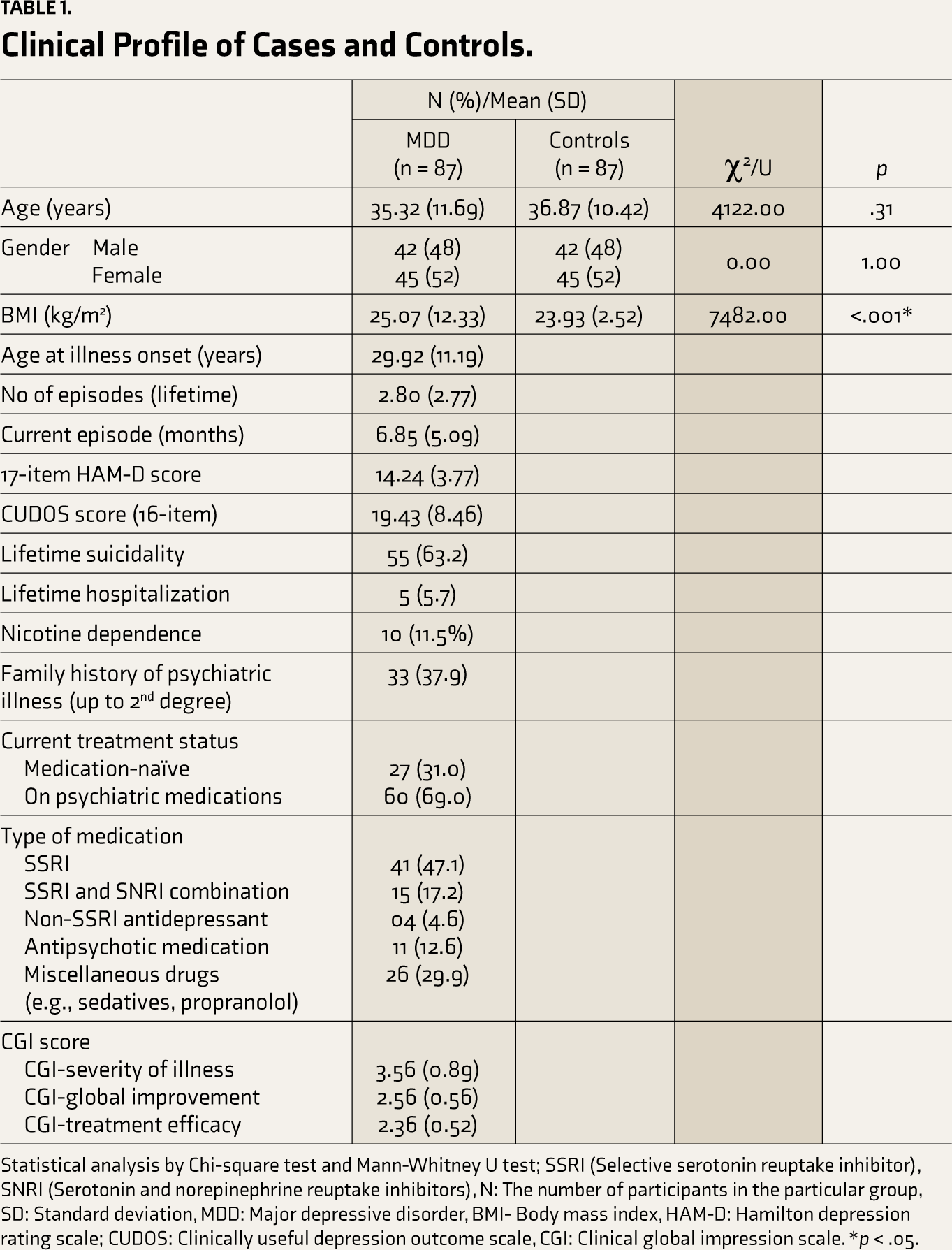
Statistical analysis by Chi-square test and Mann-Whitney U test; SSRI (Selective serotonin reuptake inhibitor), SNRI (Serotonin and norepinephrine reuptake inhibitors), N: The number of participants in the particular group, SD: Standard deviation, MDD: Major depressive disorder, BMI- Body mass index, HAM-D: Hamilton depression rating scale; CUDOS: Clinically useful depression outcome scale, CGI: Clinical global impression scale. *p < .05.
Cases had a mean of 2.80 ± 2.77 depressive episodes (median-2.0 & IQR-Q1: 1.0, Q3: 3.0, range: 1–20) over a lifetime. Nearly two-thirds (63.2%) reported suicidality. More than one-third (n = 33; 37.9%) had a positive family history, indicative of depressive disorders in 27, bipolar disorder in five, and schizophrenia in one case. Nearly one-third (31.0%) were treatment-naïve at study intake. The HAM-D score was 14.24 ± 3.77, and the CGI severity of illness was 3.56 (0.89).
Val66Met Polymorphism in Cases and Controls
The genotypic distribution of the Val66Met gene polymorphism followed Hardy-Weinberg equilibrium in cases and controls. The current study found no significant difference in genotypic distribution across cases and controls (χ 2 = 2.24; p = .33) (Table 2). Allelic frequency for Val/Met among cases and controls was 0.67/0.33 and 0.75/0.25 (χ 2 = 2.72; p = .09), respectively. The three genotype models (dominant, recessive, over-dominant) were tested to assess their association with risk of MDD, as shown in. The Val66Met polymorphism was not found to be associated with MDD (Table 3).
Genotypic and Allelic Distribution in Cases and Controls.
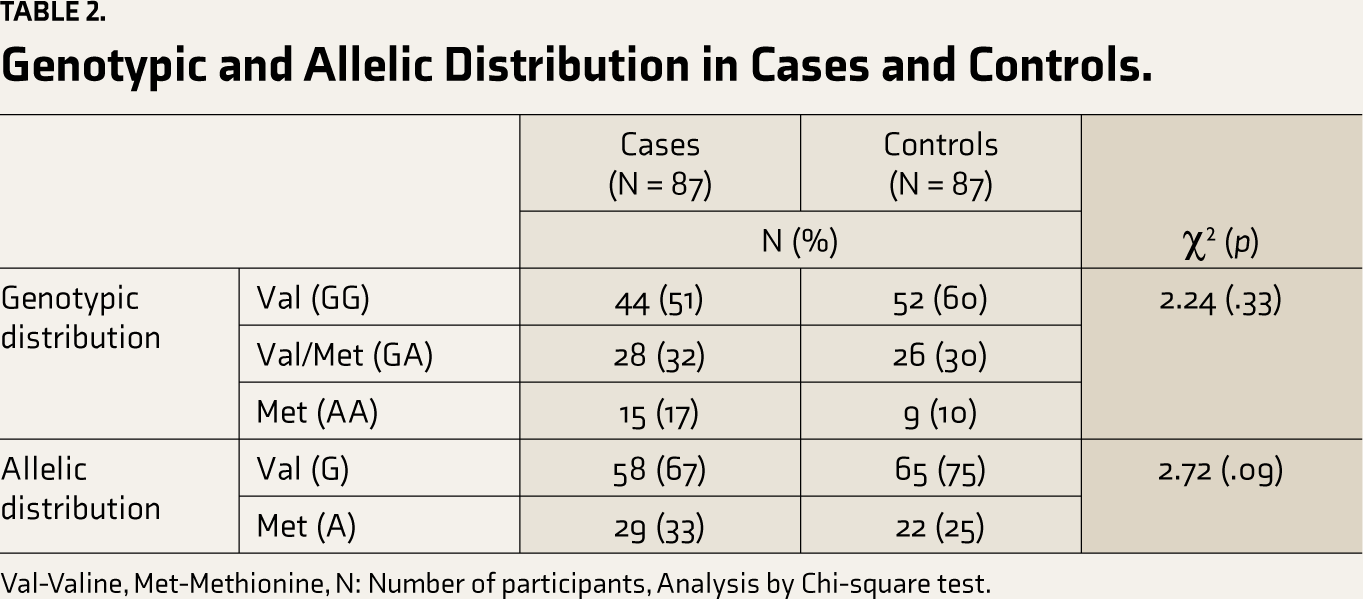
Val-Valine, Met-Methionine, N: Number of participants, Analysis by Chi-square test.
Val66 Met Polymorphism in Cases and Controls.
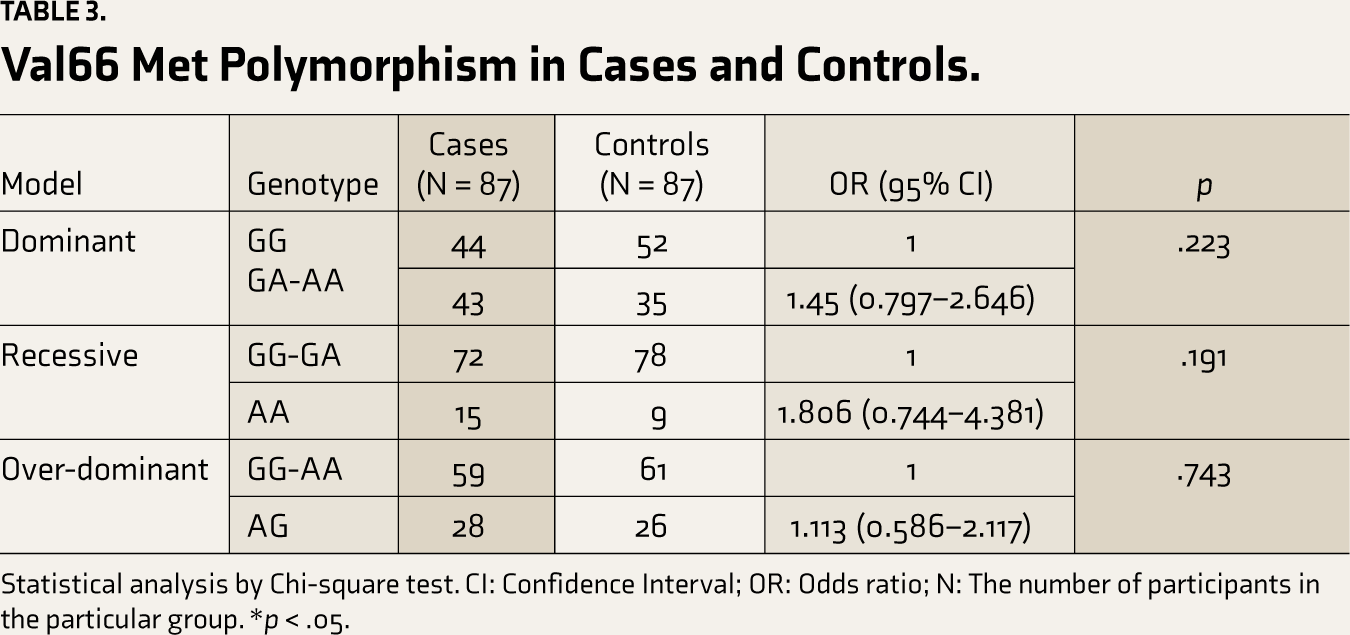
Statistical analysis by Chi-square test. CI: Confidence Interval; OR: Odds ratio; N: The number of participants in the particular group. *p < .05.
Serum BDNF in Cases and Controls
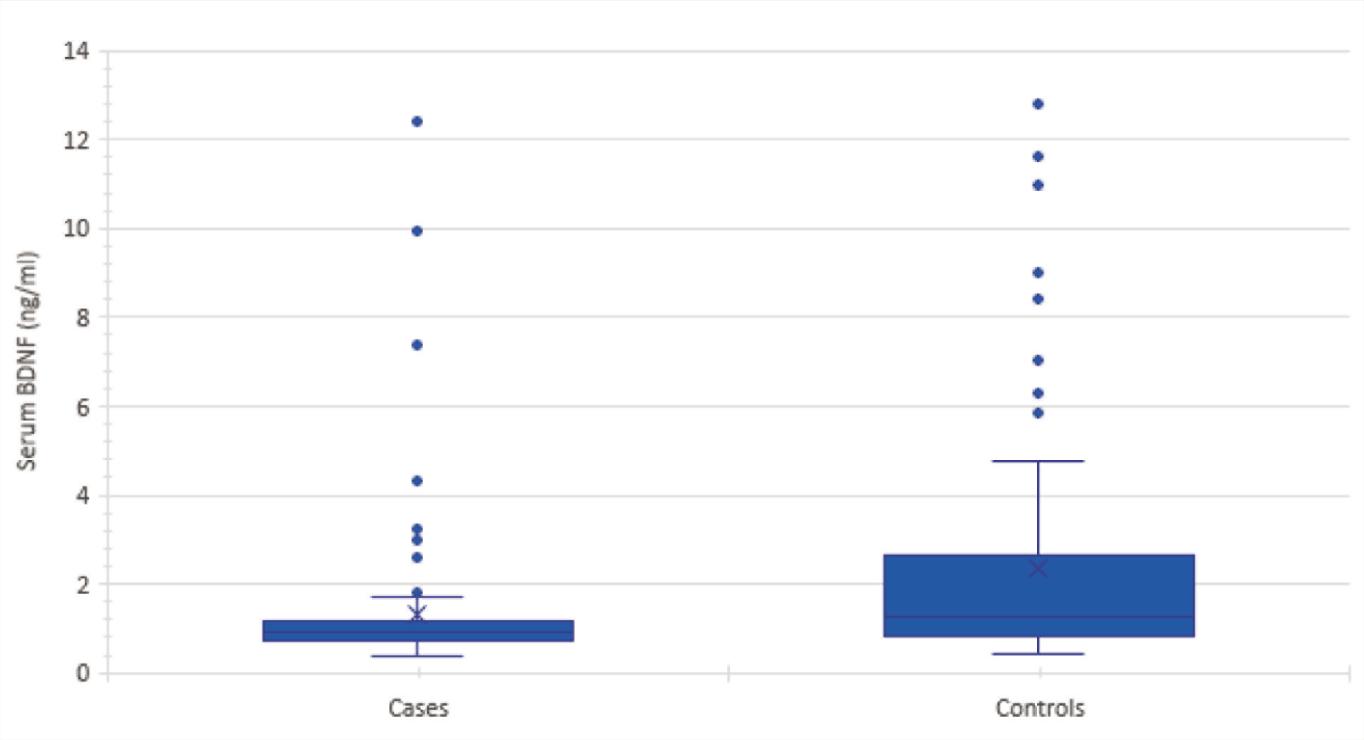
Serum BDNF levels among cases and controls were 1.33 (±1.77) Nanograms per milliliter (ng/ml) and 2.33 (±2.59) ng/ml, respectively. The mean BDNF (serum) was significantly low in MDD cases in comparison to healthy participants (U = 2598.50; p < .001). The boxplots of BDNF levels are shown in Figure 1.
Boxplots Showing Serum BDNF in Cases and Controls.
Association of Val66Met Polymorphism with Serum BDNF
For subjects with the Val/Val genotype, mean BDNF levels (serum) in cases (1.49 ± 2.06 ng/ml) were significantly lower (p = .009) compared to healthy controls (2.40 ± 2.70 ng/ml). A similar finding was observed for cases and controls with Val/Met genotype (0.97 ± 0.30 vs. 2.45 ± 2.66 ng/ml; p = .01) but not for Met/Met genotype (p = .46) (Table 4).
Val66Met Polymorphism and BDNF (Serum) in Cases and Controls.
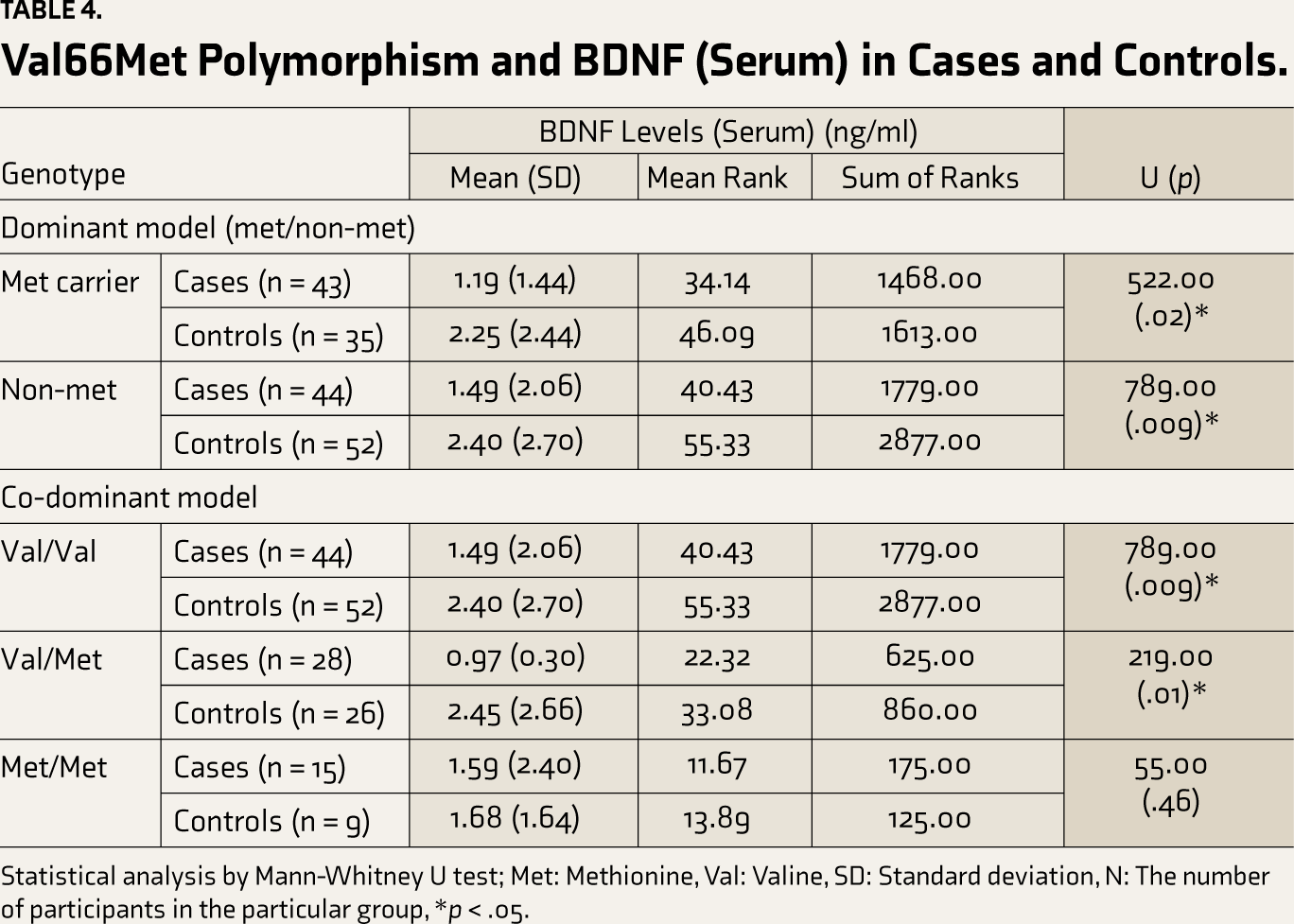
Statistical analysis by Mann-Whitney U test; Met: Methionine, Val: Valine, SD: Standard deviation, N: The number of participants in the particular group, *p < .05.
The serum BDNF was compared across Met carriers (Met/Met and Met/Val) and non-Met carriers (Val/Val) in MDD cases and controls. Compared to the respective healthy controls, serum BDNF was significantly lower among the cases, irrespective of the absence (p = .009) or presence (p = .02) of Met carrier status.
Within the MDD group, the serum BDNF levels across the three genotypic groups Val/Val (1.49 ± 2.06 ng/ml), Val/Met (0.97 ± 0.30 ng/ml), and Met/Met (1.59 ± 2.40 ng/ml) did not differ significantly (p = .69). The serum BDNF was not found to differ across Met carriers and non-Met carriers as well (p = .61).
Relationship Between Val66Met Gene Polymorphism and Serum BDNF to Clinical Variables of MDD
Interestingly, our study also observed significantly higher BDNF levels among nicotine users (1.83 ± 2.01 ng/ml) than non-users (1.27 ± 1.75 ng/ml) (U = 543.00, p = .035) (Table 5). Apart from that, no association was observed with any clinical variable. No association with illness variables was observed for BDNF gene polymorphism using the Met-dominant model (Table 5).
Relationship of BDNF Levels (Serum) and Val66Met Gene Polymorphism to Clinical Variables (N = 87).
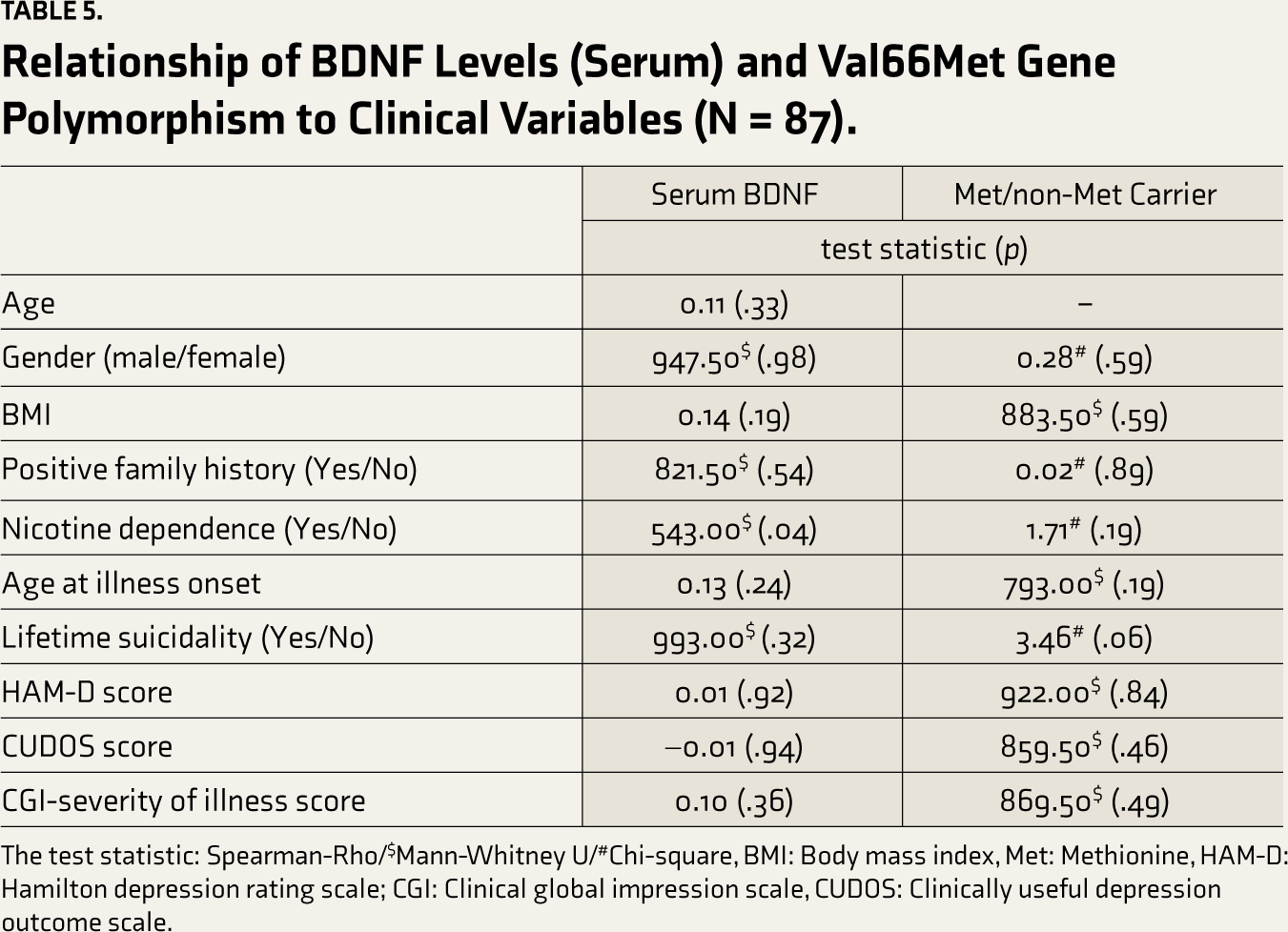
The test statistic: Spearman-Rho/$Mann-Whitney U/#Chi-square, BMI: Body mass index, Met: Methionine, HAM-D: Hamilton depression rating scale; CGI: Clinical global impression scale, CUDOS: Clinically useful depression outcome scale.
Serum BDNF in Medication-naive Patients
Analysis was repeated for serum BDNF levels in medication-naïve cases (n = 27). The mean serum BDNF level in medication-naïve cases (0.96 ± 0.47 ng/ml) was not significantly different (U = 722.50, p = .42) from cases on psychotropic medication (1.5 ± 2.09 ng/ml; n = 60), and was significantly different (U = 723.00, p = .003) from that of healthy controls (2.33 ± 2.59 ng/ml; n = 87).
Discussion
This case-control study reports the BDNF (Val66Met) polymorphism in MDD and its association with serum levels of BDNF and clinical variables in a sample of patients from Northern India. The Met allele frequency observed among MDD cases was 33%, which concurs with a prior study from South India. 19 The Met allele frequency among cases did not differ significantly from healthy controls, indicating little or no effect on the risk of MDD. The article adds to the limited available literature on BDNF Val66Met gene polymorphism in an Indian sample.
Findings from our study are also consistent with meta-analytic evidence by Li et al. 29 that did not find the risk of MDD with Val66Met polymorphism in either European (odds ratio): 1.00; 95% CI: 0.93–1.09) or Asian samples from China, Japan and Korea (OR: 0.97; 95% CI: 0.89–1.06). Among studies from India, Pathak et al. 20 observed a higher occurrence of Val66Met in MDD subjects compared to healthy individuals. In contrast, the study done by Haldar et al. 21 did not show a higher prevalence of Val66Met SNP of BDNF gene in the cases, similar to the results from our study.
The study observed significantly low BDNF (serum) levels in MDD cases in comparison to healthy controls (p < .001). This finding remained significant when the treatment-naïve subsample was compared with the healthy controls (p = .003). Available literature suggests decreased peripheral BDNF levels in cases with depression.9,12,30 A recent meta-analysis of case-control studies also found lower serum BDNF values in individuals with depression. 17 An Indian study done by Jeenger et al. 23 reported a low serum concentration of serum BDNF in MDD patients in comparison to healthy controls, which is consistent with the findings of the current study.
Some studies have reported an association of Val66Met with illness variables such as the age of onset of MDD, 13 HAM-D score,22,31 and suicide attempts. 32 The study done by Dell’Osso et al. 18 found a significant association of the BDNF values (serum) with the severity and recurrence of depression, which was contrary to observations from our study. Findings from our study, however, concur with several other studies,33,34 including those from India.21,23 Interestingly, authors found that BDNF level (serum) was significantly higher among the nicotine-dependent cases (p = .035), in line with a few previous studies that also found raised serum BDNF levels among smokers.13,35 However, our study had only a small subset of nicotine users. Future studies may explore a similar association in the Indian population about BDNF levels with nicotine dependence.
The present study has not found a significant association between BDNF levels (serum) and Val66Met gene polymorphism. This finding is in agreement with several prior studies,34–36 though few have also reported either higher13,37 or lower31,38 BDNF (serum) levels in the Met carriers. The recent study by Aldoghachi et al. 9 with 206 cases and 206 matched controls from Malaysia failed to find evidence for the effect of Val66Met gene (rs6265) polymorphism on the peripheral BDNF levels (serum).
The study’s limitations include samples collected from a single hospital, which limits the generalisability of findings. The study sample size was constrained by feasibility considerations, and a large sample would have enhanced the power of our study. The current study was not designed to assess prospective response to treatment, though that has also been linked to polymorphism. 38 Nonetheless, the study adds some useful information about Val66Met polymorphism in MDD among Indian subjects.
Conclusion
The Val66Met gene polymorphism may not have an association with a risk for MDD and, interestingly, did not influence the BDNF levels. Significantly lower BDNF levels (serum) were found in depressed cases in comparison to healthy participants (controls), which is consistent with the literature. The study points to components other than Val66Met polymorphism that may play a role in modulating BDNF serum levels. Given that India is a large country, we recommend conducting multicentric studies in the future to assess the Val66Met polymorphism in MDD patients.
Footnotes
Data Availability Statement
Anonymized data can be requested from the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Details of Ethics Approval
The study protocol was cleared by the Institute Ethics Committee at the AIIMS Delhi (Ref No: IECPG-91/27.02.2020, RT-11/24.06.2020) prior to start of the data collection.
Declaration Regarding the Use of Generative AI
No generative AI tools were used for this manuscript to collect or gather data, produce images or graphs, or write the manuscript. Authors assume full responsibility for the entire content of the manuscript.
Disclosure
Findings from the study were presented as oral presentations at ANCIPS, 2023 and ANCIPS 2024.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The written informed consent was taken from all the study participants.