
Abstract
Background:
The apathy evaluation scale (AES) measures apathy, but its usefulness as a screening tool in diverse populations is limited without translation into more languages. To date, there is no reported translation of the AES into Malayalam, a language spoken by over 32 million people in the southern Indian state of Kerala. In the present study, we aimed to validate the Malayalam version of the AES.
Methods:
Six hundred sixty-one community-dwelling older adults without dementia participating in the Kerala Einstein study completed the Malayalam AES. We assessed the internal consistency and the validity of the Malayalam AES, using another measure of apathy, as well as measures of depression and anxiety. We also used principal component analysis (PCA) to determine the dimensionality of the Malayalam AES. Finally, we assessed possible sex differences in apathy.
Results:
The Malayalam AES demonstrated high internal consistency and good validity, and the results of our PCA indicate that it has a three-component structure, as in the original English version and other translated versions. We found that while overall apathy scores were similar, the relationship with other neuropsychiatric symptoms differed by sex, with stronger relationships found in male participants compared to female participants.
Conclusion:
Our study provides another tool to screen for apathy in non-English-speaking populations, an important early risk factor for cognitive and functional decline, and enables future research across diverse cultures.
This is the first reported psychometric validation of the Malayalam version of the Apathy Evaluation Scale. The Malayalam AES has high internal consistency, good validity, and a three-dimensional structure, as reported in other versions. This study adds to the availability of tools to assess apathy in diverse populations, contributing to a better understanding of apathy globally.Key Message:
Apathy is a psychological syndrome that refers to decreased motivation, lack of interest, diminished emotional expression, and loss of energy. 1 Apathy is commonly seen in a number of neurological disorders, such as Alzheimer’s disease, traumatic brain injury, and Parkinson’s disease. 2 For example, apathy is the most common neuropsychiatric subsyndrome of Alzheimer’s disease, with 65% of patients meeting the criteria for clinically relevant apathy. 3 Recent research has suggested that apathy is an early risk factor for dementia and pre-dementia syndromes,4–7 and apathy has been linked to cognitive and functional decline.7–9 Dysfunction of frontal-subcortical circuits, particularly those linking prefrontal and basal ganglia regions, may contribute to apathy symptoms. 10 Still, many clinicians are underinformed about the detection, diagnosis, and management of apathy, and no gold-standard diagnostic criteria exist. 2 These findings underscore a need for appropriate screening tools to identify individuals with apathy and consequently at an increased risk of cognitive decline and dementia.
The apathy evaluation scale (AES) was developed to screen for apathy in clinical populations. 11 The original version of the AES demonstrated high levels of internal consistency, test-retest reliability, and construct validity. The AES aimed to characterize the behavioral, cognitive, and emotional aspects of apathy. The AES has been used in English-speaking samples and translated into several other languages, including Spanish, 12 Swedish, 13 Japanese, 14 Chinese, 15 Italian, 16 and German, 17 indicating interest in understanding apathy in different populations.
India recently became the most populous country in the world, 18 with an increasingly large older adult population. Given this demographic shift, understanding brain disorders in older Indian adults is of particular importance. However, studies investigating apathy in older adults in India are limited. One study investigated the clinical profile of older adults with mild cognitive impairment (MCI) in Bangalore, finding that 19.5% of participants with MCI reported experiencing apathy more often than depression or anxiety. 19 Another study asked Indian older adults with frontotemporal dementia and their caregivers to complete an assessment of the frequency of behaviors related to apathy, finding greater levels of apathy than healthy controls and that increased apathy scores correlated with widespread reductions in gray matter volume. 19 Similar findings of increased rates of apathy were seen in studies assessing apathy symptoms of older adults with cognitive impairment from New Delhi, 20 as well as older adults with cognitive impairment and dementia in Kolkata.21–23 Older adults in the southern state of Kerala are of unique interest, as Kerala has both the largest population of older adults and the longest life expectancy in India.24–26 To our knowledge, there is no validated translation of the AES into Malayalam, the primary language spoken by over 32 million people in Kerala, 27 and few studies have explored apathy in Kerala specifically. None of the above studies have used the AES despite its clinical and research utility. In the present study, we aim to translate and validate a Malayalam version of the AES to support future research that explores apathy in diverse and understudied populations.
Materials and Methods
Participants
The Kerala Einstein Study (KES) is an ongoing study established in 2007 that recruits communitydwelling adults aged 60 and older 28 . Exclusion criteria included previous physician-diagnosed dementia, the presence of acute and/or terminal illnesses, and/or the presence of severe auditory or visual loss. Participants were recruited from urban (Baby Memorial Hospital, Parayancheri) rural (Kakkodi Community Health Center), and exurban (Meitra Hospital) sites in Kozhikode, a northern district of Kerala, India. We excluded participants who scored less than the locally established cut score for dementia of five out of eight on the Picture-Based Memory Impairment Screen (PMIS), a culture-fair picture-based cognitive screen designed to be used in populations with variable literacy rates. 29 Between April 2022 and December 2023, 661 participants without dementia (39% female, M age 68.6 ± 5.59 years) completed the Malayalam version of the AES. The institutional review boards of the Albert Einstein College of Medicine and Baby Memorial Hospital approved this study. All participants provided written informed consent.
Instruments
Apathy Evaluation Scale
The AES is a measure of apathy with high internal consistency (Cronbach’s α 0.86) and good test-retest reliability. 11 The scale includes 18 items, which characterize the behavior (e.g., “I get things done during the day.”), cognitive (e.g., “I am interested in learning new things.”). Furthermore, emotional (e.g., “When something happens, I get excited.”) aspects of apathy. The original AES included three versions: self-rated, informant-rated, and clinician-rated. In the self-rated version used in the present study, participants are asked to indicate how much each item describes how they have felt in the past 4 weeks (1 “not at all,” 2 “slightly,” 3 “somewhat,” or 4 “a lot”). All items, except for three (Items 6, 10, and 11), are reverse-scored. The final AES score represents the sum of the 18 items, ranging from 18 to 72, with higher scores indicating greater apathy.
For the present study, a bilingual translator first translated the English version of the AES into Malayalam. This Malayalam version was then back-translated to English by an independent bilingual translator to ensure accuracy. The research team reviewed the final version regarding format, wording, grammatical structure of the sentences, similarity in meaning, and relevance. The research team discussed any ambiguities regarding cultural meaning and colloquialisms or idioms in the instructions, the items, and the response format between the back-translation and the original instrument to derive a final version of the instrument (Appendix 1).
Geriatric Depression Scale (GDS-30)
The GDS-30 is a widely used tool that screens for depression in older adults. It consists of 30 items that ask participants to assess their mood over the past week. 30 Scores range from 0 to 30, with 0–9 considered “normal,” 10–19 considered “mild depression,” and ≥20 considered “severe depression.” The Malayalam version of the GDS-30 has been previously validated, 31 and the short-form GDS-15 has previously been used in the same sample. 32
The GDS3A is a 3-item apathy subscale of the GDS that has been previously validated and used in older adults.4,33 It consists of the following items from the GDS-30: “Have you dropped many of your activities and interests?” “Do you prefer to stay at home rather than going out and doing new things?” “Do you feel full of energy?” A score of two out of a possible 3 indicates clinically relevant clinically relevant apathy in older adults.
Generalized Anxiety Disorder
The Generalized Anxiety Disorder (GAD-7) is a brief clinical assessment for the screening of anxiety, 34 and the Malayalam version has been previously psychometrically validated. 35 The GAD-7 asks participants to indicate how often, in the last 2 weeks, they have been bothered by seven anxiety symptoms. Participants rate the frequency of each symptom on a 4-point scale: 0 (not at all), 1 (several days), 2 (more than half the days), and 3 (nearly every day). Total scores range from 0 to 21. A score of 0–4 indicates “no anxiety,” 5–9 indicates “mild anxiety,” 10–14 indicates “moderate anxiety,” and ≥15 indicates “severe anxiety.”
Medical Comorbidity Score
We calculated a medical comorbidity score (0–10) based on the presence of physician-diagnosed hypertension, diabetes, stroke, depression, Parkinson’s disease, arthritis, heart disease, myocardial infarction, angina, or chronic obstructive pulmonary disease. 36
Procedure
The questionnaires (in Malayalam) were completed as part of the larger battery. After receiving brief instructions about the Malayalam AES questionnaire, a research assistant read each item and asked participants to respond verbally. The research assistant provided clarification as necessary. A similar procedure was conducted for the GDS-30 and GAD-7 questionnaires.
Data Analysis
We calculated descriptive statistics (mean and standard deviation) for demographic characteristics, as well as for each item on the Malayalam AES and overall scores on the Malayalam AES, GDS3A, overall GDS-30, and GAD-7. We assessed the normality of the distribution of overall Malayalam AES scores using visual inspection and the Shapiro-Wilk test. To assess internal consistency, we calculated split-half reliability and Cronbach’s α. We also assessed test-retest reliability in a subset of participants (n = 16) who completed the Malayalam AES a second time on average 18 months after the first test. We analyzed the dimensionality of the Malayalam AES using principal component analysis (PCA) with oblimin rotation. To ensure that PCA was appropriate, we first checked the assumptions related to PCA. The Kaiser-Meyer-Olkin measure of sampling adequacy (KMO) 37 was 0.95 and Bartlett’s test of sphericity 38 was significant, P < .001, indicating acceptable sampling adequacy and sufficiently large correlations between the items for PCA. Evidence for validity was assessed by examining Pearson’s correlations between overall scores on the Malayalam AES and the GDS3A, overall GDS-30, GAD-7, and a medical comorbidity score (excluding depression). One participant was missing GAD-7 data and was excluded from the analysis of GAD-7 data. We conducted independent-sample t-tests to assess the differences in Malayalam AES scores across sexes (male and female). The statistical analysis was conducted using psych package 39 in R. 40
Results
Participant characteristics are presented in Table 1. The overall mean age was 68.6 (±5.59) years, and the mean years of education were 9.16 (±3.43) years. The mean PMIS score was 7.61 (±0.64), and the mean number of medical comorbidities was 1.56 (±1.32), indicating overall good cognitive and physical health in the sample. The mean overall score for the Malayalam AES was 33.8 (±10.1) out of a possible 72. Overall scores on the Malayalam AES were not normally distributed (P <.001) and were positively skewed. The mean score of the individual items ranged from 1.58 (±0.76) for Item 16 to 2.69 (±1.07) for Item 11. The average split-half reliability was 0.92, and the Cronbach’s α for the Malayalam version of the AES was 0.91 (Table 2). All items had corrected item-total correlations greater than 0.6, except for Items 6, 10, and 11 (data not presented). The inter-item correlations for the Malayalam AES are presented in Table 3. All items were positively correlated with each other (r > 0.4), again with the exception of Items 6, 10, and 11, which showed weak positive or no correlations (Item 10) or weak negative correlations (Items 6 and 11) with the other items. These items were weakly (r < 0.4) positively correlated with each other. When these items were dropped, the reliability of the scale increased slightly (average split-half reliability when all three items dropped: 0.96, Cronbach’s α when each item dropped: Item 6: 0.93, Item 10: 0.92, Item 11: 0.93). A subset of participants (n = 16) completed the Malayalam AES twice, with an average of 18 months between tests. The correlation between the overall apathy scores on the first and second tests was 0.55.
Characteristics of the Participants Overall and Stratified by Sex.
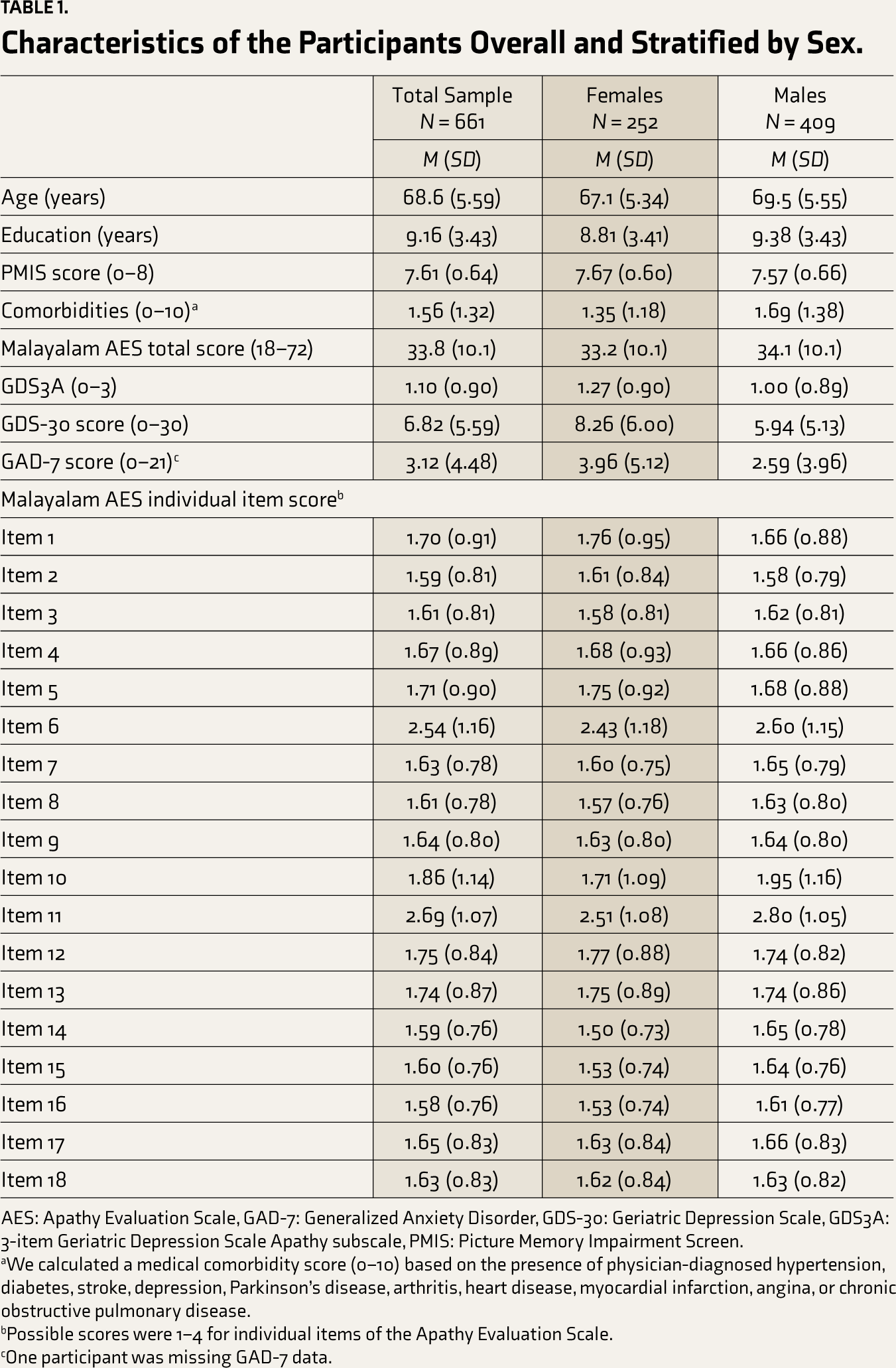
AES: Apathy Evaluation Scale, GAD-7: Generalized Anxiety Disorder, GDS-30: Geriatric Depression Scale, GDS3A: 3-item Geriatric Depression Scale Apathy subscale, PMIS: Picture Memory Impairment Screen.
aWe calculated a medical comorbidity score (0–10) based on the presence of physician-diagnosed hypertension, diabetes, stroke, depression, Parkinson’s disease, arthritis, heart disease, myocardial infarction, angina, or chronic obstructive pulmonary disease.
bPossible scores were 1–4 for individual items of the Apathy Evaluation Scale.
cOne participant was missing GAD-7 data.
Internal Consistency and Validity Assessment of the Malayalam Apathy Evaluation Scale.
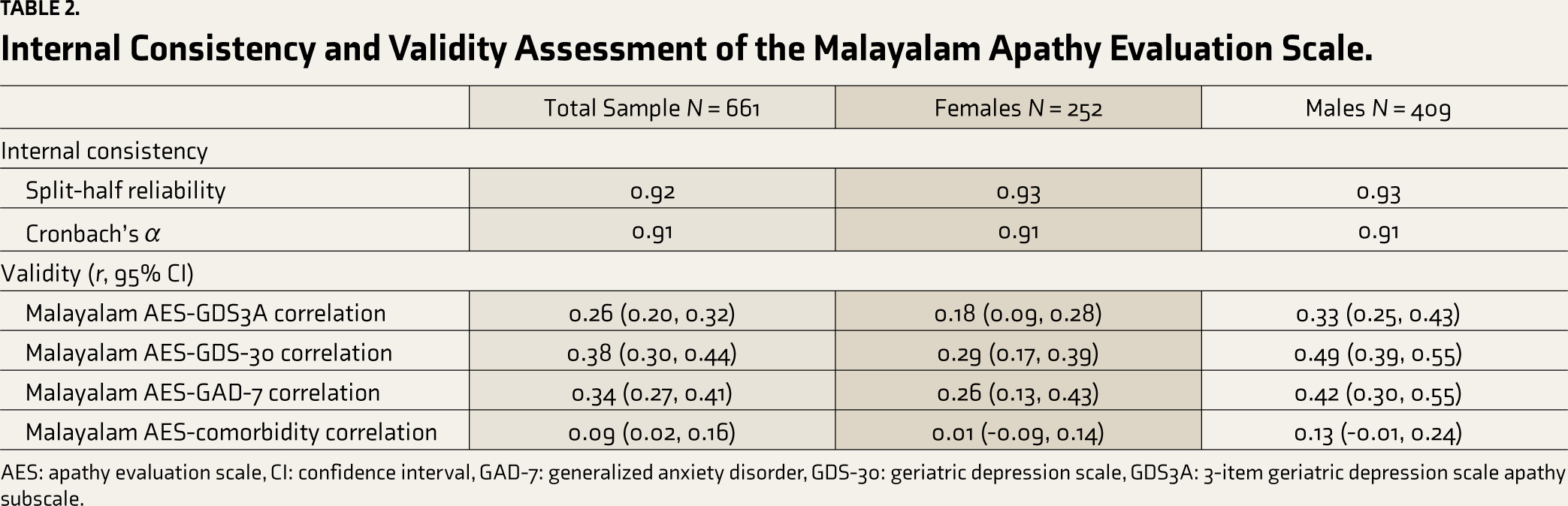
AES: apathy evaluation scale, CI: confidence interval, GAD-7: generalized anxiety disorder, GDS-30: geriatric depression scale, GDS3A: 3-item geriatric depression scale apathy subscale.
Inter-item Correlations (Pearson’s r) of the Malayalam Apathy Evaluation Scale.
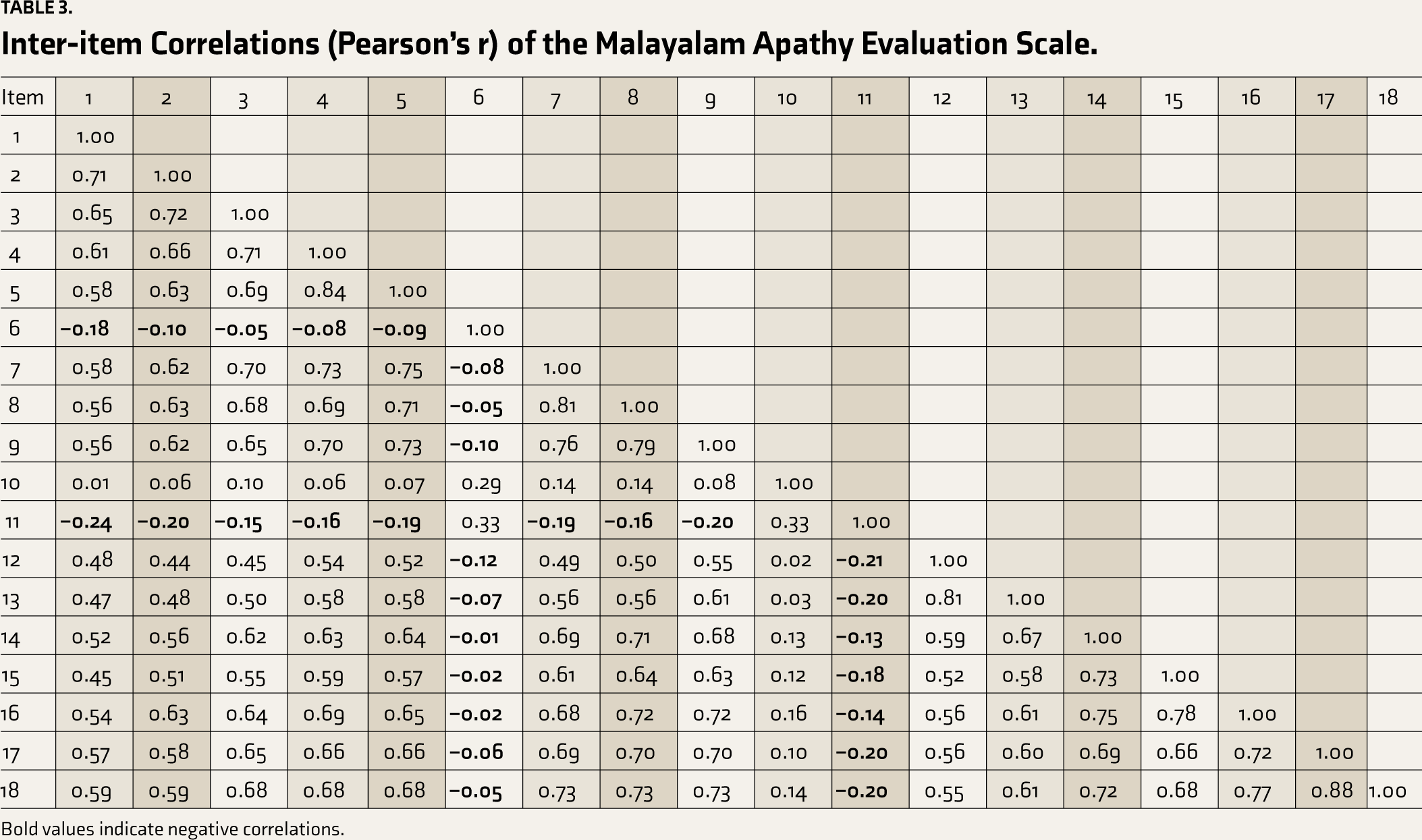
Bold values indicate negative correlations.
In our principal components analysis (PCA), Kaiser’s eigenvalue-greater-than-one criteria and inspection of the scree plot indicated three components, which accounted for 71% of the variance. Most items are loaded onto the first component (corresponding to motivation and purpose). However, four items (Items 12, 13, 14, and 15) loaded onto a second component (corresponding to insight and social and emotional experience), and three items (Items 6, 10, and 11) loaded onto the third component (corresponding to indifference). There was a weak correlation between these components (ranging from 0.01 to 0.64), supporting a three-factor structure. The results of our PCA are presented in Table 4.
Principal Components Analysis of the Malayalam Apathy Evaluation Scale.

Bold values the largest component loadings for each item.
We assessed construct validity by calculating the correlation between the apathy scores on the Malayalam AES and the GDS3A. In our sample, the mean score for GDS3A was 1.10 (±0.90) out of three. We found a weak positive correlation between scores on the Malayalam AES and the GDS3A (r = 0.26, 95% CI: 0.20–0.32). To assess the convergent validity of the Malayalam version of the AES, we calculated the correlation between apathy and two other negative mental health symptoms, depression, and anxiety. The mean overall score for the GDS-30 was 6.82 (±5.59) out of 30, and the mean score on the GAD-7 was 3.12 (±4.48) out of 21. Malayalam AES and overall depression scores were positively correlated (r = 0.38, 95% CI: 0.30–0.44), as were Malayalam AES and anxiety scores (r = 0.34, 95% CI: 0.27–0.41). We assessed the discriminant validity of the Malayalam AES by calculating the correlation between apathy and the medical comorbidity score. The mean number of medical comorbidities (excluding depression) was 1.53 (±1.30) out of nine. Malayalam AES and comorbidity scores were only very weakly correlated (r = 0.09, 95% CI: 0.02–0.16). These results are presented in Table 2.
We also assessed if there were sex differences in reported apathy in our sample. Sex differences are reported in Table 1. Overall, male participants reported similar levels of apathy (M 34.1 ± 10.1) as female participants (M 33.2 ± 10.1), t(659) = –1.19, P = .23. Internal consistency remained the same across sex (Cronbach’s α: male = 0.91, female = 0.91). The correlation between Malayalam AES and GDS3A scores was stronger in male participants (r = 0.33, 95% CI: 0.25–0.43) compared to female participants (r = 0.18, 95% CI: 0.09–0.28). A similar pattern was seen for the correlations between Malayalam AES and overall GDS-30 scores (r: male = 0.49, 95% CI: 0.39–0.55; female = 0.29, 95% CI: 0.17–0.39) and GAD-7 scores (r: male = 0.42, 95% CI: 0.30–0.55; female = 0.26, 95% CI: 0.13–0.43). Malayalam AES and medical comorbidity scores were not correlated in male (r = 0.12, 95% CI: –0.01–0.24) or female (r = 0.01, 95% CI: –0.09 to 0.14) participants. These results are summarized in Table 2.
To ensure that the missing GAD-7 data in one participant (0.15%) out of 661 did not bias our results, we also reran the Malayalam AES and GAD-7 correlation analyses, including an imputed value by replacing the single missing data point with the overall median GAD-7 score. All results remained the same.
Discussion
In the present study, we validated a Malayalam version of a widely used measure of apathy in a sample of 661 older adults (aged 60–88 years), largely in good physical and cognitive health. Our results indicate that our Malayalam translation of the AES is an appropriate tool to assess apathy among community-dwelling older adults in India. As India, and Kerala specifically, has a large and growing older adult population, systematically characterizing and measuring brain disorders such as apathy that contribute to emotional and cognitive health is critical. Measures like the Malayalam AES are essential for identifying individuals with apathy who are at risk for cognitive decline, as well as broadening our understanding of apathy across diverse populations.
We found that the Malayalam version of the AES had high internal consistency (Cronbach’s α = 0.91), in line with the original validation of the English self-rated AES (Cronbach’s α = 0.86), 11 and other translations, including the Spanish (Cronbach’s α = 0.91) 12 and Swedish (Cronbach’s α = 0.95) 13 versions. While most of the items in the Malayalam AES had high corrected item-total correlations and were positively correlated with the other items, we found three items (numbers 6, 10, and 11) to exhibit a different pattern, namely weak or no inter-item correlations (Item 10) or negative inter-item correlations (Items 6 and 11). A similar finding was also seen in the Spanish version of the AES. 12 The authors of the Spanish version recommend dropping Items 6 and 11, which were reported to have corrected item-total correlations < 0.3. Our analyses also found that Items 6 and 11, along with Item 10, had low corrected item-total correlations, and reliability improved (Cronbach’s α from 0.91 to 0.92–0.93) when these items were dropped. As such, we also recommend that researchers consider removing these items when using the Malayalam AES.
We also assessed test-retest reliability in a small subset of participants who completed the Malayalam AES twice. We found a correlation of 0.55 between overall scores at these two times, lower than reported for the original English AES (r = 0.76). However, the time between tests was much shorter (25 days) compared to our study, which was approximately 18 months. The lower reliability in the present study may reflect mental health or neurological changes rather than reliability issues with the Malayalam AES. Future research should assess test-retest reliability in a larger sample over a shorter period in order to clarify this question.
The results of our PCA indicated that the Malayalam AES consisted of three components, though most items were loaded onto a single component. The first component included items that largely relate to “motivation and purpose,” the second component included items related to “insight and social and emotional experience,” and the third component included items related to “indifference.” This is similar to the original validation of the study, which also found a three-component solution. 11 The original study described their factors as a “general apathy” component, a “curiosity or novelty-seeking” component, and an “impaired insight and dependency on others” component. Other studies have also assessed the dimensionality of translated versions of the self-rated AES. The Spanish version identified three components corresponding to “motivation, purpose, and emotion,” “indifference,” and “social and personal experience,” 12 similar to our study.
In contrast, the Swedish version reported a two-component structure, with most items loading onto the first component. 13 Notably, the items that loaded onto the second factor included Items 6, 10, and 11 (as well as Item 15), similar to the findings of our PCA. Differences between the two-component structure reported for the Swedish version and the three-component structure reported in the present study may be due to analytical choices or differences in sample characteristics, as the Swedish version included three groups of participants: healthy controls, people with MCI, and people with parkinsonian symptoms. Using clinician-rated versions, two studies also assessed the dimensionality of translated versions of the AES. The Chinese version of the AES found a three-factor structure, including a “general apathy” factor, a “having new experiences and learning new things” factor, and an “insight and social activity” factor. 15 However, the German version of the AES found a two-component structure, with the first component including items related to “problem awareness, the ability to complete tasks independently, structuring the day, interest in new learning experiences and perseverance” and the second component corresponding to the assessment of “the importance of friendships, general motivation, and personal initiative.” 17 These results indicate that the three-component structure reported in our study is largely in line with the original English AES, as well as, several other translations.
We also found that the Malayalam AES showed weak but positive correlations with another independent measure of apathy, as well as measures of depression and anxiety. First, we found that scores on the Malayalam AES were weakly correlated with scores on another apathy measure, the GDS3A (r = 0.26). When compared to the English AES, the GDS3A has been reported to have a sensitivity of 69% and a specificity of 85%. 41 However, a more recent validation study found the GDS3A to have a sensitivity of 29%–33% and a specificity of 89%–93% in two older adult cohorts. 33 These findings suggest that using the GDS3A may lead to an underestimate of apathy, which could have influenced our results and subsequent weak correlation. Second, we also found Malayalam AES scores to be positively correlated with GDS-30 (r = 0.38) and GAD-7 (r = 0.34) scores. The original English version found scores on the self-rated version of the AES to be similarly correlated with both depression (r = 0.42) and anxiety (r = 0.42) scores. The Swedish version of the self-rated AES also found positive correlations of AES scores with depression (r = 0.48) and anxiety (r = 0.35) scores. 13 As evidence of the discriminant validity of the scale, we found that scores on the Malayalam AES did not correlate strongly with a medical comorbidity score. Together, these results demonstrate that the Malayalam AES is a valid tool for assessing apathy. However, these results also underscore that apathy is a distinct syndrome from both depression and anxiety, an important reminder for the clinical interpretation of our results.
The results of our sex-stratified analyses are notable. While the overall apathy scores were similar and our reliability metric (Cronbach’s α = 0.91) remained the same across the sexes, our measures of validity were largely different. Specifically, we saw stronger correlations between the Malayalam AES and all three other measures (GDS3A, GDS-30, and GAD-7) in male participants compared to female participants. While this could be the result of a larger sample size of male participants, as our sample was 61% male, these findings could also reflect sex differences in the relationship between apathy and other neuropsychiatric symptoms. For example, previous studies have found that men with depression are more likely to endorse apathy symptoms compared to women.42,43 A recent meta-analysis reported that men with Alzheimer’s disease had more severe apathy. In contrast, women had more prevalent and severe depression symptoms, 44 underscoring that apathy and depression are overlapping but distinct neuropsychiatric disorders that may differ across sexes. Future research is needed to clarify these findings further.
Our study has strengths, including a large sample of community-dwelling adults from a population that has been largely understudied in the field of apathy research. We also were able to confirm our findings using validated Malayalam translations of another apathy scale, as well as depression and anxiety scales. However, the present study has several limitations. First, our sample may reflect selection bias, as we only recruited older adults from Kerala, and our sample had a larger number of male participants than female participants. While our results indicate that the Malayalam AES is an appropriate tool for older adults seen in clinical and community settings across rural and urban locations, younger adults or people from other regions outside of Kerala may require variations in the Malayalam AES, particularly as three items in the present scale had low reliability in our sample.
Additionally, although we found no difference in overall apathy scores, we did find differences in the relationship between apathy and other mental health symptoms. Future research should expand the sample recruitment location and demographics to increase the generalizability of the results and confirm our validation of the Malayalam AES in a broader sample. Second, we found some evidence of the validity of the Malayalam AES using the three-item GDS3A, but research is needed to validate these findings using other more comprehensive apathy assessments by qualified health professionals. Further, we were unable to assess the predictive validity of the Malayalam AES because of limited follow-up data. Future research should explore the predictive validity of the Malayalam AES, such as predicting future cognitive decline. Another limitation is our need for confirmed apathy diagnoses by a physician, the current gold standard for apathy assessment, due to the design of the KES. This may have resulted in measurement error, and future studies should include an in-depth physician assessment to confirm apathy diagnoses and further validate our results. Finally, as our main goal was to validate the Malayalam AES in the largest possible sample, we did not assess the impact of potential confounds, such as participation in social or physical activities, 45 chronic substance use, 46 or chronic fatigue/poor sleep. 47
The present study provides several avenues for future research. Longitudinal studies that assess the reliability of the Malayalam AES, as well as potential change in apathy symptoms over time, are critical to both the psychometric validation of the scale and improving our understanding of apathy in this population. Further, longitudinal studies could also assess other outcomes, such as cognitive or functional decline or changes in mental health symptoms over time, to better understand the role of the Malayalam AES in prediction and the impact of apathy on these outcomes. Our research also highlights the need for gold-standard diagnostic criteria for apathy, further exacerbated by the limited assessment tools available in different languages for use in diverse populations. Future research should develop such criteria to validate existing apathy measures better. Finally, future studies should continue to translate tools such as the AES into other languages in order to improve clinical treatment for apathy and broaden our understanding of apathy in understudied populations.
This study presents a Malayalam version of the AES, the first to our knowledge, and reports that this version has good levels of internal consistency and convergent validity. These results indicate that the Malayalam AES is a useful tool to measure apathy in Malayalam-speaking populations. As apathy has been identified as a risk factor for dementia and pre-dementia syndromes, expanding the diversity of available validated instruments is critical in better understanding apathy as a clinically identifiable feature across cultures. The development of simple, easy-to-administer scales in other languages will help clinicians identify and treat apathy in diverse social groups.
Footnotes
Acknowledgements
The authors wish to thank the KES research team and the participants, without whom this research would not be possible.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data,Materials,and/or Code Availability
The Malayalam version of the Apathy Evaluation Scale is available as online supplemental material. Data are available upon request and with completion of the data user agreement.
Declaration Regarding the Use of Generative AI
The authors assume full responsibility for the entire content of the manuscript. No part of the manuscript was generated using AI.
Ethics Approval
This study was approved by the institutional review boards of the Albert Einstein College of Medicine and Baby Memorial Hospital.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded by the National Institute on Aging (2R01AG039330-07).
Informed Consent
All participants provided written informed consent.