
Abstract
Background:
Suicide attempt is a significant predictor of suicide and occurs more frequently than suicide. Each suicide attempt leaves a significant impact on the family as they take the primary role in providing care and bear the responsibility for supporting them. The prospect of future suicide attempts puts the family in distress and makes them prone to adverse psychosocial circumstances.
Methods:
The objective of this study is to understand the life experiences of caregivers of suicide attempt survivors after the suicide attempt of their relative. Using the purposive sampling method, we interviewed the primary caregivers (n = 6) from a tertiary care setting. The in-depth interviews explored their experiences, concerns, and needs. This study used Interpretive Phenomenological Analysis.
Results:
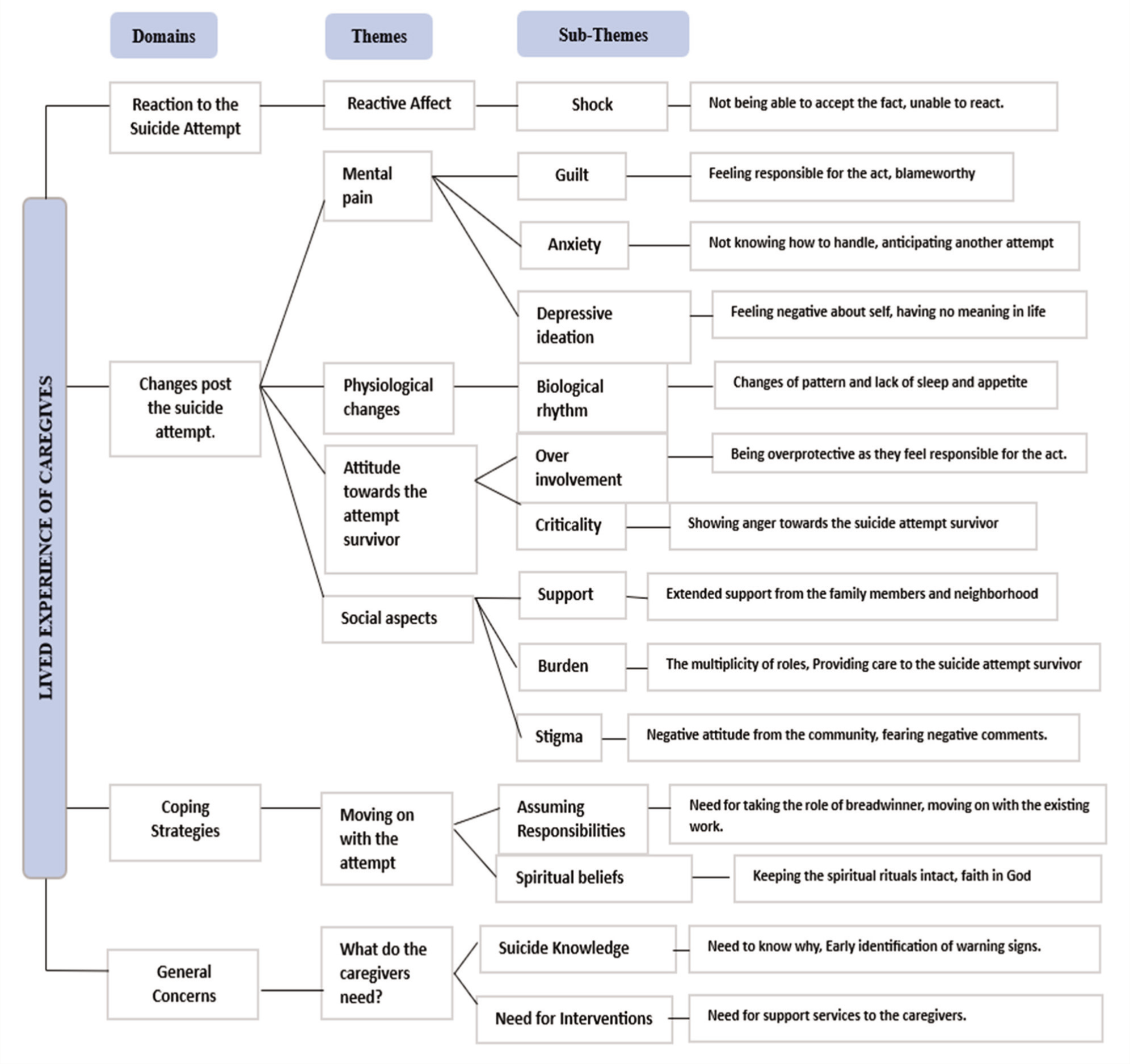
Four major themes emerged: the reactive affect, changes post the suicide attempt (mental pain, physiological changes, attitude toward the suicide attempt survivor, and social aspects), moving on with the attempt (assuming responsibilities and spiritual beliefs), and the caregivers’ needs.
Conclusion:
The impact of suicide attempts on families is primarily ignored and under-researched in the country. There is a growing need to recognize the roles and struggles of family members and support them.
This study underlines the need for developing socioculturally relevant family-focused interventions that will enhance the knowledge on suicide, regulate coping skills and self-care, and may help mitigate the aftereffects of suicide attempts such as burden and mental pain, and reduce future suicide attempts.Key Messages:
Suicide is a complex, multifaceted phenomenon that continues to be one of the significant public health issues and is highly stigmatized globally. 1 Suicide attempts can be more frequent than the death by suicide. The World Health Organization (2014) report states that for every death by suicide, there are 20 other suicide attempts likely to occur. However, the number of people attempting suicide globally every year is uncertain. 2 Governments officially publish the national statistics on suicide deaths in four Southeast Asian countries, counting out the data on suicide attempts, leaving a dearth of knowledge on attempted suicides.3,4 Suicide is a significant issue that concerns suicidal ideation, communication, and suicide attempts, which is a significant predictor of suicide. Edwin Shneidman in his ‘On the Nature of Suicide, 1969’ suggested that a suicide may intimately affect six other people and is an event with unforeseen severe effects affecting a multitude of people. 5
Nevertheless, a systematic estimation of how many survivors are left behind from a suicide informs that the number may vary depending on the type of relationship to the decedent, the age of the decedent, and the frequency of contact with the decedent. 6 While the suicide loss survivors are left to deal with their grief and trauma and restore the meaning of their lives, the families of suicide attempt survivors are pushed to face the long-term impact of the act while they provide care to the suicide attempt survivor. A suicide attempt is said to cause social injury to the family as it disturbs the family dynamics, such as interactions among the family members, leadership, decision-making, and relationships due to the social consequences of the act. 7 Family members try to find reasons for the suicidal behavior, 8 may feel blameworthy for the act, 9 anticipate future suicide attempts,10,11 experience pain following the suicide attempt, guilt for not preventing the act, and experience distress, making them vulnerable to long-term effects including depression, suicidal ideation and other forms of distress.5,12 The caregivers’ experiences include transitions (learning a new role, putting their life on hold), interfacing with health care professionals, living with uncertainty and fear, and changing relationships. 13 Moreover, the burden of providing care can be perpetuated by shame and stigma related to suicide, 14 and these factors collectively prevent the caregivers from attending to their own emotional, physical, and mental health needs.9,15 A recent meta-ethnographic study that aimed at the theoretical interpretation of relatives’ experience of providing care to persons with suicidal behavior came up with four stages: living abnormal lives as the normalcy is lost due to the suicidal act, relatives’ perceived capability to help their family members that is mediated by social interaction with professionals, being stuck in abnormality as there is no interaction in the surroundings, and moving from abnormal to normal in the process of re-positioning themselves in life. 16
In India, family is a critical resource in caregiving and essential for every individual’s growth and development. They prefer to be involved in the caregiving process due to their interdependence on each other 17 and the members being able to help each other in the family. Though the joint family systems disintegrate in Indian society, it promotes collectivism, interdependence, and cohesion. Suicidal acts are severely traumatic for the family members, which throws them into emotional turmoil. Most studies focus on suicide attempt survivors, and less focus is given to their families or immediate caregivers in the Indian context. The family members assume responsibility for providing support that extends across physical, psychological, spiritual, and emotional domains, but most often, the psychosocial factors that include the experiences and how families cope after an attempt are left unattended.7,18 The distress of families following the suicide attempt, however, may vary from one cultural setting to the other. 19
Emphasis should be placed on the caregivers’ experiences and needs to inform the practice. 13 There is little research examining the impact of suicide and the support needs of significant others,8,20 especially the literature concerning families of suicide attempt survivors in the Indian context is scarce. There is a considerable need to recognize the role of family members in supporting a person who attempted suicide, and there is a potential need for postvention for families that struggle to cope with the impact of suicide attempt.5,15 This study aimed to explore the life experiences of the caregivers, the changes in their lives, and how they coped after the suicide attempt of the relative. Exploring the carers’ needs and developing better support for them would help address vulnerability to adverse conditions and serve as an essential component in the area of suicide prevention and postvention, and would form a consultation for the development of socioculturally oriented support for the carer population.
Methods
As the first author, I must mention the influence of background and experiences on every aspect of the research process. During the study, the first author underwent clinical and academic training in psychiatric social work practice, which included the psychosocial aspects of mental health. Moreover, the cultural background and identity as an Indian researcher may influence the understanding of the social and cultural context surrounding suicides in India, as well as the interactions with the participants and interpretation of the narratives. By focusing on participants’ narratives and experiences, the aim is to elevate their voices and contribute to a more nuanced understanding of the experiences of the caregivers of suicide attempt survivors in India. During this process, the first author was constantly supervised by the second and third authors. By being transparent about the perspectives and reflexively examining the role of a researcher, the aim is to mitigate bias and enhance the validity and credibility of the study.
Study Design
This study was carried out using Interpretive Phenomenological Analysis and was conducted from September 2020 to May 2021 to develop insights from the perspectives of the caregivers of suicide attempt survivors, detailing their lived experience post the suicide attempt of their relative, how their lives changed, and how did they cope after the suicide attempt of their relative. This design allowed us to obtain experiences through first-person accounts during one-to-one interviews. 21
Participants
This study was conducted at a tertiary care center. The participants who were the primary caregivers of persons who attempted suicide were approached directly. A total of 17 caregivers were approached, and finally, 6 participants were recruited by purposive sampling from psychiatry in-patient wards, who were aged above 18 years and below 60 years. The suicide attempt was the first suicide attempt. Participants with severe mental illness or chronic medical conditions were excluded. Informed consent was obtained from all the participants. The reasons stated by others for not consenting to the study included not wanting to discuss the suicide attempt, unavailability of time, not being comfortable with recording the interview, and few without any reasons, which were not probed further respecting the autonomy of the respondents.
Materials and Procedures
The profiles of the respondents were gathered using the sociodemographic data sheet prepared by the research team. The first author developed the semi-structured interview guide based on reviewing previous studies on the impact of suicide attempts on family.5,10,19,20 It was validated by experts that included two psychiatric social workers and one psychiatrist. It was pilot tested with one interview with a respondent, made necessary changes, and approved by the experts.
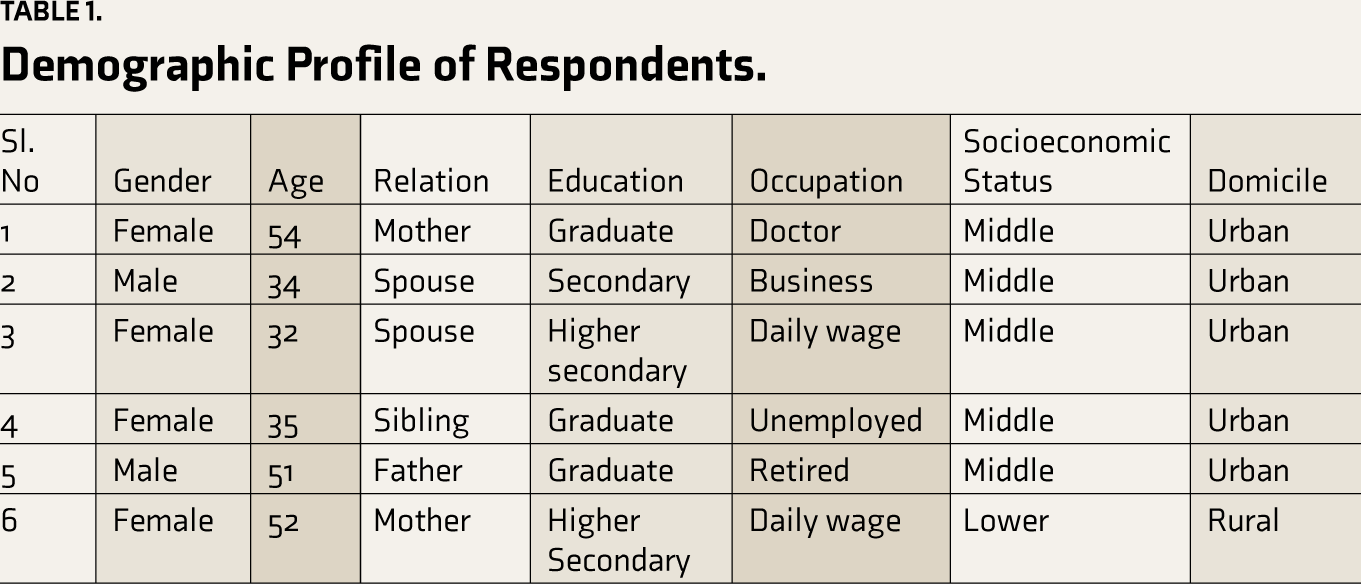
The interview began with a brief introduction about the research and providing information about the rights of the respondents. Once the respondents consented, the interviews were initiated with the demographic profile (Table 1) of the respondents, getting to know the context of the suicide attempt and moving on to the specific questions such as “What was your immediate reaction toward the suicide attempt? How did you respond to it? Could you please tell us how it feels to know a loved one had attempted suicide” to explore their experiences about the phenomena. The interviews were audio-recorded with the consent of the respondents. The interviews ranged from 60 to 90 minutes in duration. Five interviews were done initially. The researcher coded after each interview, but no new codes emerged during the fifth interview. One more interview was carried out to verify if any new themes emerged. Hence, data saturation was achieved with six interviews, supported by the literature stating that the sample size of phenomenological studies usually ranges from 3 to 25 participants.22–24
Demographic Profile of Respondents.
Data Analysis
The interviews were audio-recorded. Each interview was transcribed by the first author and anonymized; participants were assigned pseudonyms, and all identifying details were removed or altered. Audio and transcribed data were stored securely with participants’ IDs in password-protected, approved platforms. Transcribed data were matched with the audio recordings and checked for accuracy by the other authors. The first author independently coded data by reading and re-reading to get the global essence of the responses. The first author also maintained a reflexive journal from the beginning of the study. The sections with similar focuses were grouped and interpreted. These codes were discussed with other authors, and minor revisions were made. The transcripts were compared using an iterative approach to identify significant themes and sub-themes in the data, and the results were finalized (Figure 1). The researchers ensured that the study’s findings had adequate and accurate references in the raw data and were substantiated by concrete and detailed participant descriptions.
Mapping of Themes and Subthemes.
Ethical Considerations
The ethical approval for the study was obtained from the Institute Human Ethics Committee. Participants were provided with information regarding the purpose of the study, confidentiality, and data management. They were also informed that the study may involve some sensitive issues, and in case of distress, the option of pausing the interview or withdrawing from the study was emphasized. The option of facilitating professional help was also provided. Written informed consent was obtained from the participants.
Results
Central themes were reaction to the suicide attempt, mental pain, physiological changes, attitude toward the suicide attempt survivor, social aspects, moving on the attempt, and the caregiver’s needs. Following are the emerging themes and subthemes:
Reaction to the Suicide Attempt
Shock
These are an individual’s immediate emotional responses after they hear about the suicide attempt of their relative. The shock was the foremost and most common reaction of the respondents toward their relative who attempted suicide. Respondents reported that they were uncertain about what to do and how to react when they heard about the suicide attempt.
One of the respondents mentioned, “I was shocked as why did she go this way? I did not know how to react at her and to this situation” (34-year-old spouse).
“It was unbelievable. I could not take it. I could not believe that something has gone wrong with my son or that he has attempted suicide.” (54-year-old mother)
Changes Post the Suicide Attempt
Mental Pain
Physiological Changes
Attitude Toward the Suicide Attempt Survivor
The following were the expressed emotions of the caregivers toward the suicide attempt survivors.
Yeah. After that incident, I was doing things like checking on him. We were pampering him like a kid and feeding him food. Previously, he used to sleep alone. After that, we never left him alone. I used to check on him as to what he was doing, whether he was sleeping properly or not, whether he had food properly, and used to buy whatever he liked and things like that. (35-year-old sister)
Social Changes
I am a doctor, and I seriously tell you, when I get a case of suicide attempt, I never had any empathy. I used to be very disgusted. Why is this person so weak? Why does he want to do such an act? The same thing was done by my colleagues also when my son had attempted suicide.
There were also instances when the caregivers felt not being included in gatherings and observed changes in the communication pattern.
Moving on with the Attempt
What Do the Caregivers Need?
Suicide Knowledge
The caregivers reported the need to know why their relative chose to attempt suicide. They also mentioned having noticed a few changes in their relative prior to the suicide attempt, which were left unnoticed or ignored, thinking not to bother by probing on it. The guilt emerged as the signs were not identified and addressed at the right time as a 52-year-old mother said, “I know that he was upset over his separation from wife for a long time, which I did not take seriously. However, I did not expect my son to do this.”
Need for Intervention
The vast changes in respondents’ lives pose the need for a postvention program. A few participants also raised the need for a support group. A 51-year-old father said, “The parents who have experienced such situations should interact with other parents so they do not undergo similar situations or face any adverse circumstances. We are the burning examples of how we are suffering.”
Discussion
This study investigated the experiences of caregivers on their reactions and how their lives changed after the suicide attempt of a loved one. The themes that emerged were reactive affect, that is, shock, mental pain, changes in attitude toward the suicide attempt survivor, social changes, moving on with the suicide attempt, and the needs of caregivers. The aftermath of suicide attempts by family members is understudied in low- and middle-income countries, especially in India. To the best of our knowledge, this study is the first of its kind in India that focuses on the caregivers of suicide attempt survivors. The family systems perspective informs that a person identifies oneself as subject to the push and pull in the family system, which may include various factors such as emotional demands, role expectations, and others. 25 In line with the systems perspectives, the caregivers undergo enormous transitions after the suicide attempt of a relative, which have been discussed in this article. The immediate reaction of the caregivers when they came to know about the suicide attempt was shock as they did not expect the suicidal act to happen and were not able to find any reason for the suicide attempt that is in line with the existing literature globally.5,19 Blameworthiness was an important aspect to note in the Indian context, where every unit in the family is intertwined and holds themselves responsible for every act that takes place in the family. The respondents reported guilt of not being able to prevent the attempt, made them vigilant often, and they feared future suicide attempts. 26 They also reported guilt of not performing their duties as a family, which might have resulted in a suicide attempt. Furthermore, the present study reveals that, with hindsight, respondents felt there may have been warning signs, but they had not understood how serious they were. In that sense, participants conveyed guilt about not perceiving the sign or responding to the changes that they noted in their relative.27,28 The feeling of not being capable of caring, powerless, and less confident could be improved by the interface with the professionals. The professionals could involve the caregivers in the treatment, provide better information about the warning signs, and how to take care of them to prevent future attempts and better care for themselves. 16 The respondents reported feelings of distress in the process of caring. Few had suicidal ideations at some point in time post the suicide attempt of their relative, which is in line with literature that says that individuals who are exposed to suicide attempts or death by suicide in their lifetime have an increased risk of having suicidal ideations, suicide attempt, and death by suicide.29,30 In addition to the effect on mental health, respondents also noted changes in the quality of sleep and appetite. The respondents also reported a burden when the earning member of the family had attempted suicide. The subjective burden varied based on the type of family, whether the person who attempted suicide was an earning member and the social support system the respondents had. However, the study did not intend to measure the caregivers’ distress and burden level. The lack of social support hampers coping with the stress. As the roles were transferred and multiplied among the respondents, they started engaging in work as a form of problem-focused coping.26,27,31 Besides, coping included spiritual beliefs, which helped them build their emotional strength. 32 Studies highlighted the fact of acknowledging cultural needs when considering the carers, particularly due to the stigma that is attached to suicide in certain countries19,33 that will apply to the Indian sociocultural context, where suicide is still stigmatized despite the decriminalization of it. It was evident from the findings that there was a negative attitude toward respondents and a change in the interaction pattern with the neighbors. The results also indicated the presence of internalized stigma and reduced participation in social gatherings and social interactions. 34 There is also a need to understand suicide attempts clearly, immediate measures to sort the difficulties that arise out of suicide attempts, and needed information for the caregivers to know how to move forward and to avail appropriate social support services. 35 There is a potential need for suicide prevention and postvention programs for those who are struggling to cope with the impact of suicide attempts. Indigenous family-oriented psychosocial interventions such as psychoeducation focusing on debunking the myths, providing facts on suicide, identifying the early warning signs of suicide, communication skills, coping strategies, and self-care of the carer population must be developed. Studies also suggest that caregivers need practical information and education regarding mental health problems and suicide, strategies that will help manage at home, seeking help during a crisis, targeted interventions to address the emotional, relational, and mental health impact of caring, follow-up calls from healthcare staffs, complex supports such as respite services, clinician empathy, validation, and nonjudgement and interventions to develop coping strategies.8,13,20,28,36–39 The National Suicide Prevention Strategy of India, which was released in November 2022, also suggests the delivery of brief interventions for suicide attempt survivors and families. 40 Support for families of suicide attempt survivors is less studied in India. Hence, more focus on research should be taken to explore the experience of families in the Indian context and their support needs and develop interventions to address the distress of families of suicide attempt survivors for better implementation of the suicide prevention strategy.
Footnotes
Acknowledgements
The researchers would like to acknowledge all the respondents for their valuable time and for sharing their experiences.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.