
Abstract
Background:
Metabolic syndrome (MetS) is a concern in psychiatric patients. We aimed to study the influence of the modifiable lifestyle factors on MetS in adult psychiatric patients along with associated clinical factors and quality of life.
Methods:
Factors such as diet (Healthy Eating Index), exercise, substance use, cardiovascular risk (QRISK), illness severity (Clinical Global Impression), medications, adverse events (Systematic Monitoring of Adverse Events Related to Treatments), and quality of life (Recovering Quality of Life Scale) were assessed along with clinical components for MetS in 323 psychiatric patients receiving routine care and monitoring in a Community Mental Health Team.
Results:
MetS was present in 50.5% (95% CI: 45.0–55.9). It was significantly associated with higher age, duration of mental illness, body mass index (BMI), QTc, QRISK, and antipsychotic drugs. In logistic regression, age, QTc, QRISK, and BMI remained significantly linked to MetS. Patients with or without MetS were comparable in their lifestyle factors such as diet, exercise, and substance use, along with the family history of metabolic disorders, age at onset of mental illness, duration of antipsychotic medication, side effects, psychiatric diagnoses, and quality of life. However, many patients with or without MetS had poorer diet and physical inactivity, indicating scope for interventions.
Conclusions:
Around half of the psychiatric patients had MetS, and modifiable lifestyle factors did not differentiate individuals with or without MetS. The need for further research on the prevention and management of MetS in psychiatric patients is highlighted.
Around half of the psychiatric patients under the community mental health team had metabolic syndrome. Age, BMI, QTc, and QRISK were significant factors linked to MetS. Modifiable lifestyle factors were not different in patients with or without MetS.Key Messages
Patients with severe mental illness have lower life expectancy than the general population. 1 The reported figures for average years of life lost in patients with schizophrenia are around 10–15 years,2,3 which could be potentially much more. 4 There is a significant increase in death due to diabetes and cardio-cerebrovascular causes, in schizophrenia. 1 Those with severe mental illnesses, in general, have an increased prevalence of multimorbidity. 5 Co-occurrence of diabetes, hypertension, dyslipidaemia, and obesity refers to metabolic syndrome (MetS), which is associated with increased morbidity and mortality. 6 These cardiometabolic diseases are common causes of early death in psychiatric patients, considerably decreasing the life expectancy of patients with severe mental illnesses.3,4
There are many studies on MetS in patients with schizophrenia,7–9 bipolar disorder,10,11 depressive disorders, and intellectual disabilities. 12 Reported prevalence rates of MetS vary among studies, 8 and meta-analyses have suggested that around a third of patients with schizophrenia and related disorders have MetS.9,13 Information on MetS prevalence in patients with other diagnoses is comparatively scant.
There are reports of an association between MetS and drug-naïve patients with schizophrenia; 14 however, it is more commonly associated with antipsychotic drugs.15,16 Its reported prevalence figures in antipsychotic-naïve and antipsychotic-treated patients range between 3.3%–26.0% and 32.0%–68.0%, respec-tively.17–21 Common side effects of anti-psychotics include hyperglycaemia, weight gain, and obesity, 22 suggestive of metabolic dysregulation,16,23 and many patients with metabolic side effects meet the criteria for the MetS.15,24 There are differences in the metabolic side-effect profile of the antipsychotic drugs. 16 In addition to antipsychotics, antidepressants, and mood stabilizers have also been associated with an increased cardio-metabolic risk and many other physical diseases in patients with serious mental illnesses.25,26
Besides psychiatric medications, metabolic concerns have been con-sidered secondary to an unhealthy lifestyle, including poor diet and sedentary behaviour,26,27 which could be related to mental illness. Excess mortality in patients with severe mental illness is also due to these modifiable factors, lifestyle behaviours, reduced access to physical care, and frequent comorbid illnesses. 1 Lifestyle modifications are reported to help manage components of MetS,28,29 and have been a constant feature of guidelines for the intervention of meta-bolic side effects,30,31 besides cardiovascular monitoring and intervention.
Despite an increased understanding of MetS and the existing guidelines for screening and intervention,22,30,32 metabolic abnormalities are common in psychiatric patients, and alarmingly, these are often missed. Although many studies report MetS in specific diagnoses and medications, information on its prevalence in general psychiatric patients is scarce. In addition, the influence of various underlying factors, some of which are modifiable, for example, diet, physical exercise, and substance abuse, are not robustly clear in the community psychiatric clinic settings, although clinical advice related to these such as increased activity and attention to diet is commonly provided during routine care. In this context, we hypothesized that lifestyle factors are associated with the MetS in patients with mental illness in community psychiatric clinic settings.
We intended to study the influence of lifestyle factors such as diet, exercise, and substance use in relation to MetS, in a community mental health setting, to explore any modifiable, preventable factors that may be useful for individual patients. We also checked the association with diagnoses, severity of psychiatric illness, psychiatric drugs, side effects, and relationship with quality of life (QOL).
Method
Criteria for MetS
MetS involves obesity, insulin resistance, impaired glucose tolerance, dyslipidaemia, and hypertension. There are various definitions from different professional bodies.33,34 The definition of MetS for this study was taken from the International Diabetes Federation (IDF) Task Force. 35 It suggests that any three out of five criteria need to be present to qualify for MetS, which are elevated ethnicity-specific waist circumference (WC), elevated triglyceride (≥150 mg/dL or 1.7 mmol/L), reduced high-density lipoprotein (HDL) (<40 mg/dL or 1.0 mmol/L in males; <50 mg/dL or 1.3 mmol/L in females), elevated blood pressure (systolic: ≥ 130 mmHg or diastolic: ≥ 85 mmHg), and elevated fasting glucose (fasting plasma glucose ≥ 5.6 mmol/L or 100 mg/dL; or previously diagnosed Type 2 diabetes). It also suggests using alternative criteria of drug treatment for elevated triglyceride, reduced HDL, elevated glucose, and antihypertensive drug treatment with a history of hypertension. In addition to this, in the line of WHO criteria,34,36 IDF definition specifies that if body mass index (BMI) is> 30 kg/m2, central obesity can be assumed and WC need not be measured. 33
Site
This cross-sectional study was conducted at a secondary-level adult mental health service in a city in England with a population of around 250,000. The clinical setting has a clozapine monitoring clinic and an established physical health monitoring clinic. These clinics investigate for metabolic side effects and arrange for any necessary interventions. Information from these clinics is shared with general practitioners (primary care physicians) and treating psychiatrists in secondary care in a pathway to arrange appropriate treatment.
Sample
Inclusion Criteria
Both male and female patients aged between 18 and 65 in adult mental health services were eligible to be included in the study. This included patients from all ethnic groups and diagnoses. The sample included patients taking antipsychotic drugs and those who were not. Patients on two or more antipsychotic medications (polypharmacy) were also included but excluded from the analysis for any medication-specific analyses.
Exclusion Criteria
Patients who did not agree to participate, who did not attend the outpatient or physical health monitoring clinic appointments, and who could not be contacted even after two reminders were excluded, as there was no information available about their physical parameters and blood investigations. Patients who were pregnant or had delivered in the last six weeks were also excluded.
Sampling
The sample was recruited consecutively from the existing list of patients attending outpatient appointments, the clozapine clinic, and the depot clinic.
Sample Size
Based on the reported prevalence level of 32.5%, 9 with a margin of error of 5%, at 95% confidence level, with a population size of 5000 (approximate number of patients in the psychiatric services in the city), we calculated the sample size to be 316, based on the formula: n = Z2 PQ/d2; where, n = required sample size, Z = the value of standard normal variant at 95% level of confidence, P = prevalence of MetS, Q = 1-P, d = allowable error.
Data Collection
Data was collected by consultant psychiatrists, postgraduate trainees in psychiatry, and psychiatric nurses. They received training for the study and on the instruments, which included conducting an initial few assessments with the two authors, and later, a few more assessments were supervised. Interrater reliability was established following the initial assessments. Following this, there were random checks for data quality monitoring.
Details of sociodemographic (gender, age, and ethnicity) and clinical variables (diagnosis and treatment), and lifestyle factors (diet, exercise, smoking, alcohol or drug use) were collected. Patients were given appointments at physical health monitoring clinics where the physical examination and investigation-related information, for example, height, weight, waist circumference (WC), BMI, blood pressure (BP), glucose, HbA1c, lipid profile and electrocardiogram (ECG) for corrected QT interval (QTc) were collected. Laboratory blood tests were done at the local general hospital.
Specific clinical history indicative of cardiovascular concerns, for example, smoking, diabetes, hypertension or on medication for hypertension, high cholesterol, and use of statins were collected, along with family history of diabetes, obesity, hypertension, and angina/heart attack. The risk of developing a heart attack or stroke over the next ten years (QRISK) was calculated using QRISK-3 [
The severity of illness was assessed with Clinical Global Impression – Severity scale (CGI-S), which is a 7-point scale, 39 where the points suggest –0: not assessed, 1: normal, not at all ill, 2: borderline mentally ill, 3: mildly ill, 4: moderately ill, 5: markedly ill, 6: severely ill, 7: among the most extremely ill patients.
Side effects to medications were evaluated through self-report and an assessment based on systematic monitoring of adverse events related to treatments (SMARTS) checklist, which is a 12-item questionnaire that covers a range of side effects for antipsychotics. 40
Healthy Eating Index (HEI) was used to explore how healthy the diets were. 41 It is a validated self-reported diet-quality assessing instrument using a single-item measure that asks: ‘In general,how healthy is your overall diet? Would you say excellent, very good, good, fair, or poor?’ The responses were scored on a 5-point Likert scale (5: excellent, 4: very good, 3: good, 2: fair, 1: poor).
The method of exercise and levels were enquired about and categorized as inactive (little or no exercise), low (a maximum of 2.5 hours of exercise a week), and moderate (at least 2.5 hours of exercise each week). This was based on National Health Service guidelines for adults in the UK. 42
Following the clinical history, smoking status was categorized as non-smoker, ex-smoker, current use - light smoker (less than 10), moderate (10–19), and heavy (≥20 cigarettes). Similarly, alcohol use was categorized as non-drinking, ex-drinker, current use - occasional drinking, harmful use, and dependence. Illicit drug use status was categorised as never used, ex-use, current use – occasional, harmful use, and dependence.
We assessed the QOL using Recovering Quality of Life (ReQoL). 43 It is a 10-item scale that has been validated in the UK for patients with mental illness. The responses are scored on a Likert scale of 0 to 4, with higher scores indicating better QOL. A ReQoL score of ≤24 is categorized as within the clinical range, and ≥25 as the non-clinical range. It has an eleventh item on physical health (problems with pain, mobility, difficulties caring for self, or feeling physically unwell). We also asked about their overall QOL on a scale of 0 to 10 where a score of 0 is the worst and a score of 10 is the best QOL.
Ethics
Detailed information about the project was provided to the patients verbally and in written format. Anonymity and the option to withdraw at any time were explained. Written informed consent was obtained. The project was ethically approved by the Health Research Authority [IRAS project ID: 229330, REC reference 17/NI/0126]. In the process of the study, patients were psycho-educated and provided with an information leaflet regarding psychiatric disorders, medications, side effects, and physical monitoring needs. General practitioners were informed regarding any physical health concerns identified during the process. The results were also shared with treating psychiatrists in secondary care.
Analysis
Data were entered in Microsoft Excel and analysed using SPSS version 28 (Armonk, NY: IBM Corp). Missing data were not included in the analysis. The specific outcome of this study was the percentage of patients having MetS. The association of sociodemographic and clinical factors with MetS was studied using chi-square tests for categorical variables, and considering multiple comparisons, Fisher’s exact test (FET) was used when indicated. The means were compared with t-tests and ANOVA. We studied the relations between numerical variables using Pearson’s correlation. The associated factors were further analysed through logistic regression. The significance level was kept at standard 0.05.
Results
Demographic Characteristics
Patients were recruited for the study from June 2018 to October 2020. Out of 373 patients recruited, 50 were excluded (17 were aged >65, and 33 had inadequate data due to non-attendance for physical examination and investigation following initial assessment), leading to a final sample of 323, with a mean ± SD age of 44.4 ± 12.1 years. There were 186 (57.6%) male and 137 (42.4%) female patients with a mean age of 44.43 ± 12.3 and 44.37 ± 11.9 years, respectively (not significant, NS). The ethnic backgrounds of the patients were: White Caucasian (209, 64.7%), Asian (62, 19.2%), African/Caribbean (39, 12.1%), and other (13, 4.0%).
Clinical Characteristics
Major diagnoses in the sample were schizophrenia (134, 41.5%); other psychoses (47, 14.6%); bipolar disorder (41, 12.7%); depressive disorders (40, 12.4%), anxiety disorders (29, 9.0%); personality disorders, (23, 7.1%) and others (9, 2.8%). The mean age at onset of mental illness was 24.7 ± 10.3 years; the duration of mental illness: 19.7 ± 12.2 years. duration of taking psychiatric medications: 16.3 ± 11.6 years, and duration of taking antipsychotic medications: 14.8 ± 11.4 years. There were 35 (10.8%) patients not on antipsychotic drugs; all others (n = 288) were taking antipsychotics.
162 (50.2%) patients had high BP or were on antihypertensive treatment, 71 (22.0%) had high blood sugar or were on antidiabetic medicine, 177 (54.8%) had high triglyceride or on statins, and 139 (43.0%) had low HDL. Considering the IDF criteria, 33 242 (74.9%) patients had WC above the cut-off point based on ethnicity or had a BMI >30. The mean BMI in the sample was 31.6 ± 7.6, which correlated significantly with the WC (r: 0.72, p < .001). The average HEI score was 2.6 ± 1.1, midpoint being 3 on the 1 to 5 Likert scale. The mean QTc was 423.7 ± 25.9 msec, which was within the limit for both genders. 44 Considering QOL, the overall QOL was 5.5 ± 2.5; the ReQoL score was 21.6 ± 9.1 which was in the clinical range, and the mean physical health item score of ReQoL was 2.7 ± 1.2.
Prevalence of MetS
A little over half (n-163, 50.5%, 95% CI: 45.0–55.9) of all the patients had MetS, consisting of 91 (48.9%) male and 72 (52.6%) female patients (NS). Considering ethnicity, 54.8% (34/62) of Asian, 57.7% (30/52) of Black, and other minority group in contrast to 47.4% (99/209) of Caucasian White had MetS (NS). Prevalence rates of MetS in different diagnostic groups were as follows: schizophrenia, 51.5% (69/134); other psychoses, 55.3% (26/47); bipolar disorder, 53.7% (22/41); depressive disorders, 55.0% (22/40), anxiety disorders, 41.4% (12/29); and personality disorders, 47.8% (11/23) (NS).
Comparison of Patients with or without MetS
Comparisons of various demographic and clinical variables are given in Table 1. Patients with MetS had significantly higher age, longer duration of mental illness, longer QTc, and higher QRISK. As expected, patients with MetS had more number of criteria for MetS met (3.6 ± 0.7 vs. 1.3 ± 0.7, t: 27. 8, p < .001) compared with those with-out, and the individual components of MetS were also significantly more frequent in those with MetS. The duration of taking medication for mental illness was high in patients with MetS; however, it was not statistically significant.
Comparing Demographic and Clinical Variables of Patients with or without MetS.
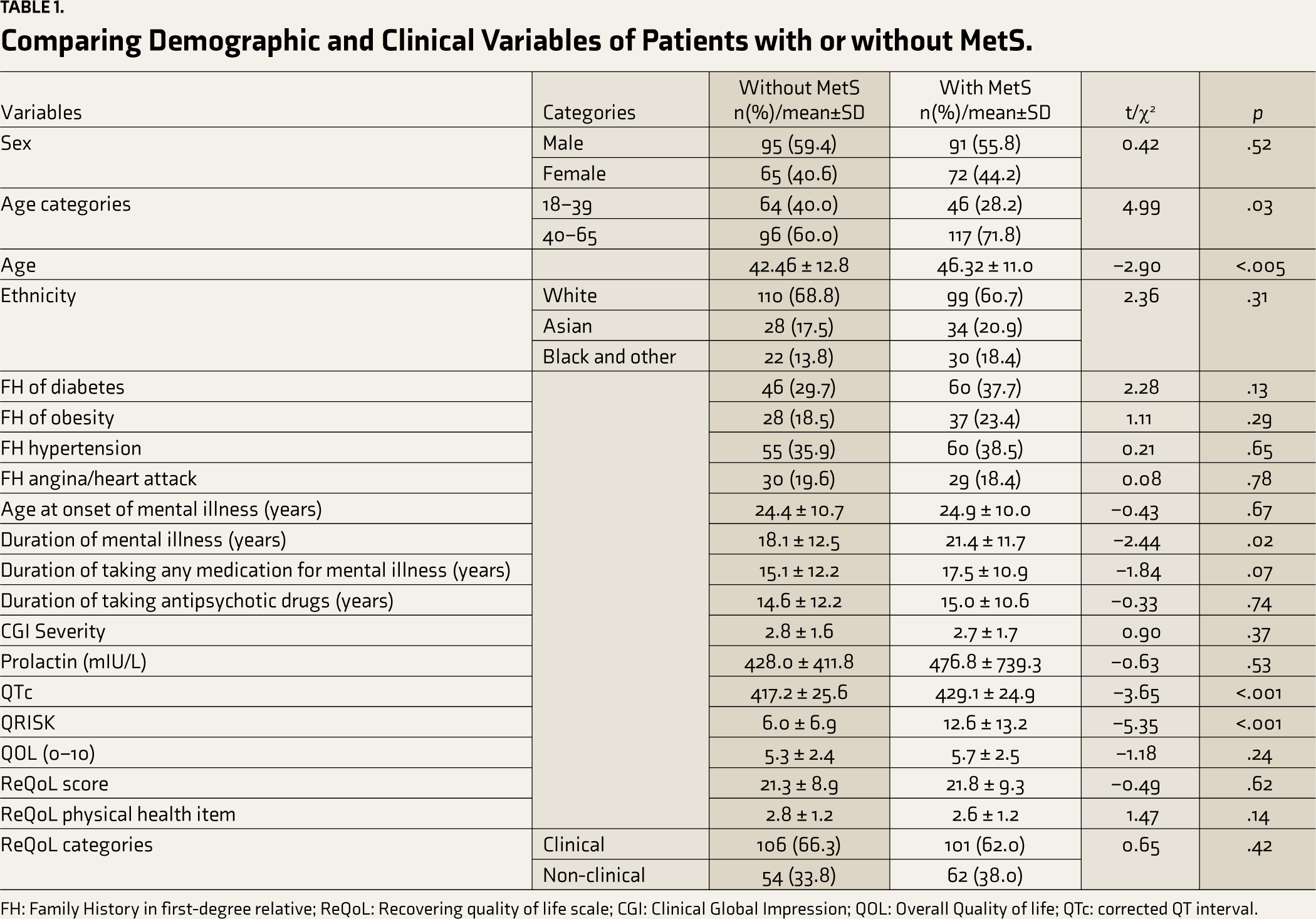
FH: Family History in first-degree relative; ReQoL: Recovering quality of life scale; CGI: Clinical Global Impression; QOL: Overall Quality of life; QTc: corrected QT interval.
Modifiable Factors
Information regarding possible modifiable factors is given in Table 2. Patients with or without MetS were comparable in their reported side effect profile. Although HEI response categories were comparable, 45.5% (140/308) of patients in the whole sample described their diet as poor or fair. Similarly, there was no difference in exercise levels in the two groups, but 36.9% (114/309) were physically inactive and 39.2% (121/309) had low levels (up to a maximum 2.5 hours a week) of physical activity.
Comparing the Modifiable Factors in Patients with or without MetS.
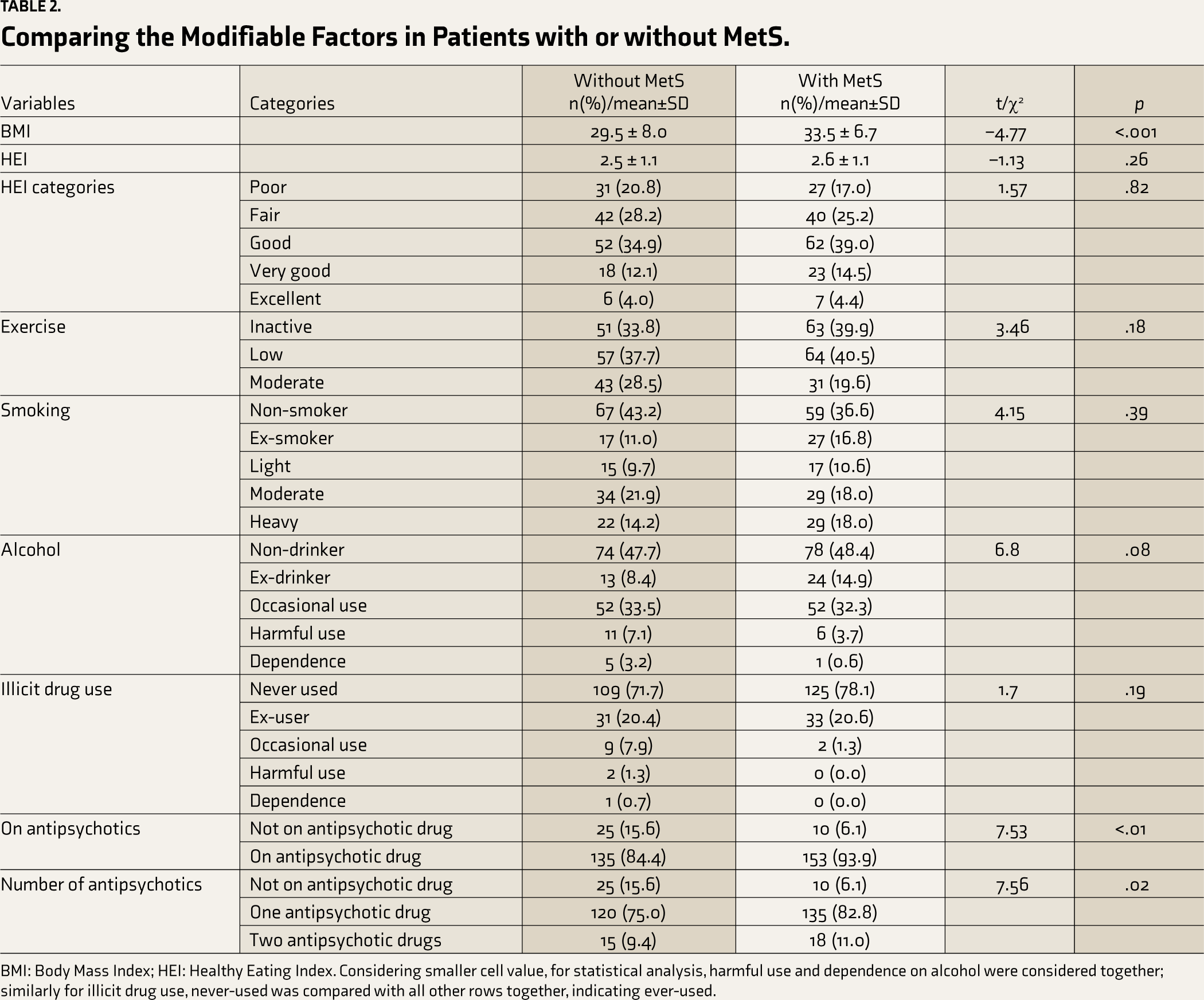
BMI: Body Mass Index; HEI: Healthy Eating Index. Considering smaller cell value, for statistical analysis, harmful use and dependence on alcohol were considered together; similarly for illicit drug use, never-used was compared with all other rows together, indicating ever-used.
Considering current smoking, 10.1% (32/316) reported light, 19.9% (63/316) moderate, and 16.1% (51/316) heavy smoking. Around one-third, 32.9% (104/316), of patients, reported occasional drinking, 5.4% (17/316) had harmful use, and 1.9% (6/316) had alcohol dependence. A minority (4.5%, 14/312) of patients reported current use of illicit drugs. The smoking, alcohol, and illicit drug use status was not significantly different between patients with or without MetS (Table 2). However, only two (1.3%) patients with MetS had current illicit drug use, compared to 12 (7.9%) without it (FET, p < .01).
Psychiatric Drugs and MetS
More than half (53.1%, 153/288) of patients on antipsychotic drugs had MetS, compared to 28.6% (10/35) taking other drugs (Table 2). Amongst the patients on antipsychotics, 33 (11.5%) were on two antipsychotics. The proportion of patients with MetS taking one antipsychotic drug (52.9%, 135/255) was comparable to that (54.5%, 18/33) of those on two.
Considering antipsychotic groups of currently prescribed drugs, without including those with polypharmacy, the prevalence of MetS was 59.5% (25/42) in the atypical depot, 41.1% (23/56) in the typical depot, 54.0% (87/161) in atypical oral, and 59.3% (35/59) in clozapine groups; there were only three patients on typical oral and only one of them had MetS. Proportions of patients on mood stabilizers who had MetS were 65.2% (15/23) for lithium and 58.8% (30/51) for antiepileptic drugs (valproate and carbamazepine).
Factors Contributing to MetS
We used logistic regression analysis to explore the associated factors for MetS (Table 3). The variables found significantly associated with MetS in the bivariate analysis, for example, age, BMI, QRISK, QTc, the duration of mental illness, and being on antipsychotics were entered. While age, BMI, QRISK, and QTc contributed significantly, the duration of mental illness and being on antipsychotics did not.
Logistic Regression Analysis of Associated Variables for MetS.
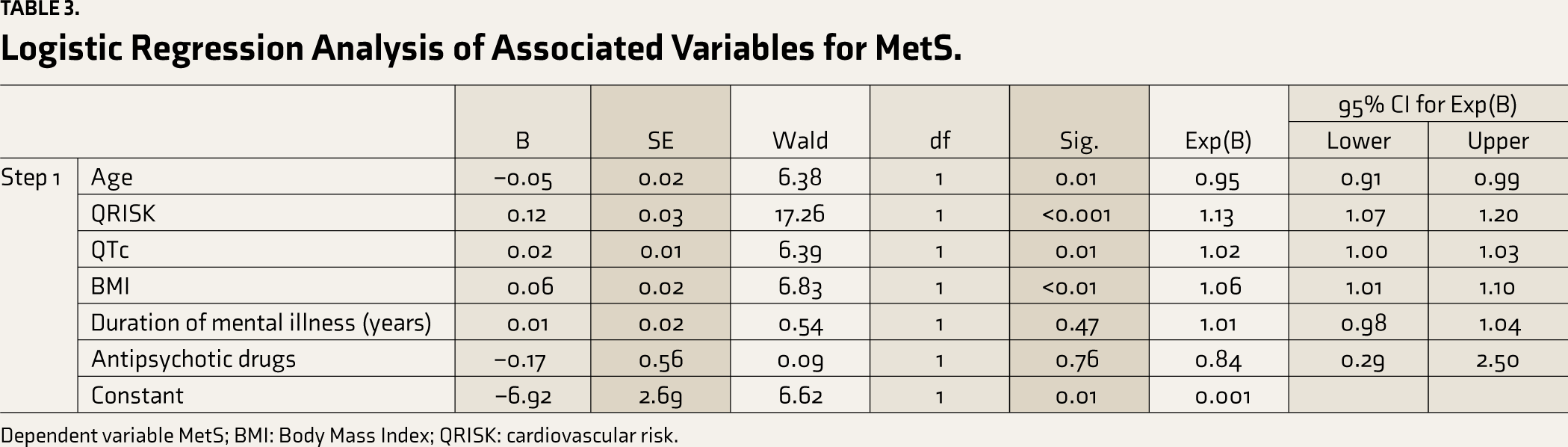
Dependent variable MetS; BMI: Body Mass Index; QRISK: cardiovascular risk.
Discussion
The study evaluated the association of MetS with clinical and modifiable lifestyle factors in adult psychiatric patients in a usual care setting of a Community Mental Health Team, including all diagnoses and treatment. It was observed that MetS is highly prevalent, being present in around half of the patients.
Although the reported rates have been quite variable,8,9,13,17,19,21 observed prevalence in this study is on the higher side, possibly due to various factors. Prevalence of MetS in the UK general population is comparatively higher, with around a quarter of adults to one-third of older adults being affected by this;45,46 in contrast to around 12.5% to 31.4% prevalence in other regions in the world.47,48 Besides the population background, the mean age of the studied sample was over 40, and higher age has been reported as a contributing factor for MetS in psychiatric patients.9,13,21,49 In addition, the average BMI of the sample was in the obesity range for all the ethnic groups, 50 which correlated significantly with WC and is known to be associated with MetS. 21 Other factors known to influence the prevalence of MetS are the side effects of associated psychiatric medications and lifestyle factors discussed below. Various interactive mechanisms such as chronic inflammation, genetics, 51 and biological factors 52 have been reported for MetS; however, it is beyond the scope of this study to reflect on these factors.
Diagnostic Groups
In our study, the proportions of MetS in different diagnostic groups, such as schizophrenia, other psychoses, bipolar disorder, and depressive disorders, were slightly higher than that in anxiety and personality disorders. The reported prevalence figures in different diagnostic groups have been variable.9,10,13 Observations of higher rates in this study are probably because most of our patients received antipsychotic drugs across the diagnoses, and some received mood stabilizers, which are known to be associated with MetS.15,16,52
In the case of mood disorders, our findings are comparatively higher than a report of around a third to half of patients with depressive disorders and a quarter of patients with bipolar disorder having MetS. 52 Interestingly, MetS has been associated with an increased prevalence of depressive disorder, and there may be other common factors in mood disorders, such as antidepressant drugs and mood stabilizers contributing to weight gain. Similarly, the prevalence figures of MetS in patients with anxiety and personality disorders in our sample were comparatively higher than the reported figures.52–54 This may be due to the range of psychiatric drugs prescribed in these patient groups, which included antipsychotics and mood stabilizers that can contribute to weight gain as a side effect.
Modifiable Lifestyle Factors
The study found that a considerable proportion of patients had concerns about the modifiable lifestyle factors; however, these did not significantly impact the prevalence of MetS (Table 2). This could be due to the inability of lifestyle activities to influence in the context of the long duration of mental illnesses and exposure to various psychiatric medications with metabolic side effects. However, as lifestyle intervention may be effective for dealing with MetS,28,29 more focused action may be needed beyond the routine clinical care, cardio-metabolic screening, and intervention system based on the existing guidelines.30,32
Diet
A considerable proportion of patients reported poor or fair diet; however, the HEI index and categories were comparable between those with or without MetS. Poor diet may be a common observation in psychiatric patients for various reasons, including self-neglect and economic constraints. Disordered eating behaviours are also commonly reported in schizophrenia patients. 55 Although statistically not significant, the findings of this study suggest a possible scope for intervention for a proportion of patients, which might decrease the diet-related factors.
Exercise
In this study, exercise levels did not differentiate the groups with or without MetS; however, most patients were inactive or low on exercise. This is not an uncommon observation with psychiatric patients, especially those having chronic disorders with negative symptoms. Although it has been reported that exercise can reduce mental health burden and improve QOL,56,57 a meta-analysis found no change in mental health symptoms, BMI, and body weight in adults with serious mental illness. 58 Nonetheless, as regular physical exercise may be beneficial, some patients may need additional practical multidisciplinary support, 59 beyond the usual clinical advice.
Substance Use
Although many patients had past or current use of tobacco, alcohol, or illicit drugs, these did not differentiate patients in relation to MetS. Interestingly, current drug use, in general, was significantly less in patients with MetS. However, the sample size is inadequate to draw any firm conclusion. In contrast to our findings, alcohol use disorders have been reported to be associated with MetS. 60 Based on these findings, a few general observations can be made regarding substance use. As smoking is linked to cardiovascular risks61,62 and a considerable proportion of patients in this study were current smokers, interventions to decrease and stop smoking may benefit many psychiatric patients, reducing their cardiovascular risk. Bespoke smoking cessation intervention has been reported to be helpful, 63 so also psychological interventions; 64 however, their availability and motivation of patients may be a challenge. In summary, measures to deal with MetS in psychiatric patients should include the management of substance use disorders.
Clinical Factors
A large proportion of our patients had components of MetS, and patients with MetS had significantly higher BMI, QTc, and QRISK. However, in the logistic regression, the associations were not robust considering the odds ratios, and the duration of mental illness or being on antipsychotics did not contribute. Increased age is a well-known contributor for MetS.9,13,21,49 Higher BMI and increased QRISK are well-reported in schizophrenia-spectrum disorders. 65 Considering the findings, the clinical importance of monitoring QRISK, QTc, and BMI and the intervention regarding these cardiovascular risk indicators is reemphasized. As the likelihood of MetS is increased with the presence of any of its components, it suggests a need for greater clinical focus while prescribing for psychiatric patients with any cardio-metabolic diseases. This also suggests the need for pro-active intervention related to metabolic side effects associated with antipsychotics.3,4
Psychiatric Medications
A higher proportion of patients on antipsychotic drugs in our study had MetS. This is within the reported ranges of 32.0%–68.0% of antipsychotic-treated patients17–21 but higher than the rates of around one-third as suggested in the meta-analyses.9,13 The association of antipsychotics with MetS has been well reported.66,67 Patients with MetS in our study had a significantly longer duration of mental illness, which has been reported as an associated factor.9,11,21 A combination of factors is probably linked to chronic mental illness, including exposure to psychiatric drugs such as antipsychotics and mood stabilizers, physical inactivity, and poor dietary habits. However, in the logistic regression, being on antipsychotics was not significantly contributing. This might be due to the possibility of other psychiatric medications, such as mood stabilisers, contributing as well to weight gain and obesity, which has links with other metabolic disorders. Despite higher metabolic side effects, antipsychotics are protective against all-cause mortality in psychiatric patients, 1 so the approaches to contain MetS need to look for additional measures.
While the association of MetS with antipsychotics was reemphasized, the study could not comment on the causal relationships with specific drugs or class as most patients had a history of many years of exposure to various antipsychotics and other drugs. It is known that the MetS prevalence increases as the period of exposure to antipsychotics increases;7,20,68 this cross-sectional study could not reflect the changes over the years of exposure.
Considering current typical and atypical antipsychotic drugs, the proportions of MetS were highest in the atypical depot and lowest in the typical depot. MetS in patients with clozapine, atypical oral agents, and polypharmacy were comparable. Similar findings have been reported in previous studies, for example, the prevalence of metabolic abnormalities was higher in patients receiving atypical antipsychotics compared to the typical ones. 17
MetS prevalence rates on one or two antipsychotic drugs were comparable in our study; however, the number of patients receiving two antipsychotics was low. In contrast, previous studies have reported that polypharmacy was associated with elevated rates of MetS compared to monotherapy, 66 where it has ranged from 18.8% to 44.7% in one study. 67 Antipsychotic polypharmacy is known to increase the risk of side effects, including metabolic ones,66,69 and warrants caution related to MetS.
QOL
Interestingly, the QOL was not different between these groups with or without MetS (Table 1). It is known that physical illnesses, including cardio-metabolic diseases, are associated with lower QOL, especially when associated with psychiatric illnesses.65,70–73 It is possible that the QOL of the studied groups was not significantly different as they were being influenced by various factors, including both mental and physical illnesses.
Clinical Implications
The study highlighted that in community clinical setups with treatment as usual, many psychiatric patients had MetS, and lifestyle factors did not influence its prevalence. This was despite having established cardio-metabolic monitoring and intervention systems within the psychiatric setup based on guidelines,22,30,32,74 To compound the problem, it is known that many psychiatric units in the UK and elsewhere have inadequate monitoring for metabolic parameters and many cases of hypertension, diabetes, dyslipidaemia, and obesity are missed.20,24 Considering this, based on this study’s findings, it appears that there is a need for monitoring for all psychiatric patients, irrespective of diagnoses and medications. In addition, the monitoring process should be robust where there are specific concerns regarding medications,22,30,32,74 cardiovascular side effects, or the existence of components of MetS. 75 While monitoring needs to have specific objectives to detect and manage components of MetS, there should be focused efforts to prevent these as a part of the overall intervention. Attention must be paid to QRISK, BMI, and QTc, along with increasing age.
Although the modifiable lifestyle factors did not influence MetS prevalence through usual care, there was scope for further improvement as many patients had poor diet, physical inactivity, and substance use. There should be a specific effort to evaluate and actively support lifestyle factors routinely beyond usual clinical advice. 21 Practical measures may be specifically incorporated into the intervention plan. In addition, there is a need to explore measures that can effectively prevent and manage MetS.
Strength and Limitations
This study was conducted in a general psychiatric unit in the community, and the results may be generalizable to similar clinical setups. Most previous studies have focused on schizophrenia and severe mental illnesses; however, this study has included patients irrespective of diagnoses and drug treatment. The study looked into the association of various lifestyle factors holistically, such as exercise, diet, smoking, alcohol and drug use, QRISK, and QOL with MetS.
There are a few limitations of this study. Most of the sample was taking antipsychotic drugs, reflecting the current scenario of patients attending secondary mental health services. Future studies may consider a larger group of patients with other psychiatric medications and patients without mental illness for comparison. Similarly, the number of patients with polypharmacy with antipsychotic drugs was small in the sample, which may not be adequate for comparison.
Comparable MetS rates in different diagnoses could be secondary to multiple factors such as most patients having antipsychotic drugs across diagnoses, mood stabilizers with an increased rate of obesity, and long duration of illnesses with exposure to various psychotropic drugs. Although it may be challenging in a usual care setting with comorbidities and multiple medications over different periods, studies with larger sample sizes may look into MetS in different diagnoses, comparing drug-naïve states with those following specific drug treatment.
A small proportion of patients did not feel comfortable providing WC for whom BMI criterion was used as per guideline.33,34 It was realized that measuring WC may be a concern in patients who are sensitive about central obesity, which needs to be considered. Probably, the categorization methods of diet, exercise, and substance use could not highlight any existing differences if present between patients with or without MetS; future studies may consider more in-depth assessments for these variables.
Conclusions
Almost half of the psychiatric patients attending the outpatient clinics had MetS, across psychiatric diagnoses. Patients with MetS had a significantly longer duration of mental illness, and a higher proportion had antipsychotic drugs. Age, QRISK, BMI, and QTc contributed significantly to the risk of MetS. Many patients had poor diet and substance use and were physically inactive, but these did not differentiate patients with or without MetS. However, the findings suggest the scope of intervention regarding these and indicate the need for focused monitoring and interventions specific to MetS. Future studies should look more widely for the factors contributing to MetS, the methods of interventions that may prevent or decrease the prevalence of MetS in psychiatric patients, and the effectiveness of those interventions.
Footnotes
Acknowledgements
We thank Debbie Lester, Jenny Horne, Dr Faiz Masood, Dr Mahum Kiani, Dr Amy Boswell, Dr Helen Wheeldon, Dr Zaib Nisa, Dr Jasmin Mahil, Dr Tulika Prasad, Dr Sayyid Ahmed, Dr Sadia Zahid, Dr Susmit Roy, Dr Shreyan Kar, Dr Faiz Masood, Dr Thanuja Vidyaratne, Dr Amina Rashid, Dr Brajaballav Kar, Dr Nitish Mathur, Alison Grant, Andrew Chapani, Jo Whitehouse, Gaye Johnson, for support related to data collection and data quality management. We are also thankful to Research and Innovation Department of the Black Country Healthcare NHS Foundation Trust and The Institute of Insight, United Kingdom.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research was supported by General Adult Faculty Small Project Funding – 2019, Royal College of Psychiatrists, London, United Kingdom. Funding or supporting organizations had no influence on study design, analysis or report.