
Abstract
Background:
Persons with schizophrenia (PwS) are vulnerable to developing disordered eating behaviors. However, standardized tools to assess disordered eating patterns are unavailable in the regional language, Tamil. Different versions of the Three-Factor Eating Questionnaire (TFEQ) have been used to measure disordered eating patterns among PwS worldwide. This study aimed to assess the factor structure and reliability of the Tamil version of TFEQ-R18V2 among Tamil-speaking PwS.
Methods:
Over three months, 135 PwS, aged 18–65 years, who attended the outpatient department of a tertiary mental health service provider in Chennai, completed the Tamil version of TFEQ-R18V2. Thirty PwS completed the tool after two weeks to assess its test–retest reliability. The factor structure of the tool was explored using principal component analysis.
Results:
The sample included 75 (55.6%) males and 60 (44.4%) females with a mean (±SD) age of 40.1 (±9.8) years and a mean duration of illness of 11.99 (± 8.72) years. Internal consistency and test–retest reliability of the Tamil version were 0.84 and 0.532, respectively. A five-factor structure emerged from the factor analysis, with 65.67% of the variance.
Conclusion:
The Tamil version of TFEQ-R18V2 emerged as a reliable tool to assess disordered eating patterns among Tamil-speaking PwS.
The Tamil version of the Three-Factor Eating Questionnaire R18-V2 is reliable for assessing disordered eating patterns among Tamil-speaking persons with schizophrenia.Key Message:
Background
Disordered eating behaviors (DEBs) include unhealthy behaviors, such as purging, binging, and restrained eating, which cannot be diagnosed as full-blown eating disorders because of the lower frequency or severity of the symptoms. 1 DEB lies on a continuum with eating disorders that warrants regular monitoring among the vulnerable population to ensure timely management and intervention. 2 In persons with schizophrenia (PwS), the risk of developing DEB is higher owing to comorbid conditions such as diabetes, cardiovascular diseases, and obesity. 1 Antipsychotic medication compounds their vulnerability further as it can alter their satiety signals, thereby worsening DEB. 3 Literature shows that the association between psychotic symptoms of schizophrenia and DEB is not uniform. Some cases have been reported where a period of disordered eating patterns preceded the onset of psychotic symptoms. At the same time, in some, the DEB emerged or worsened in the long course of chronic schizophrenia. 4
The global prevalence of different types of disordered eating reported among PwS varies from 4.4% 5 for binge eating to 60.6% 6 for food cravings. Most studies on PwS across the globe have used standardized instruments that measure disordered eating, such as the Dutch Eating Behavior Questionnaire, the Eating Attitudes Test-26, the Eating Behavior Assessment, and the Three-Factor Eating Questionnaire (TFEQ). 1
There is a shortage of research on disordered eating in India, with almost no published work exploring DEB among PwS in more than 10 years. 7 There are no standardized questionnaires in Indian languages to assess disordered eating among persons with psychosis. 8 The current study ventured to bridge this gap by validating the Tamil-translated version of the Three-Factor Eating Questionnaire-R18V2 (TFEQ-R18V2) for use among PwS in Tamil Nadu, one of the states with the highest prevalence of schizophrenia compounding to a crude disability-adjusted life year rate of 183 (124–207) per 1,00,000 population. 9
The TEFQ was initially designed by Stunkard and Messick in 1985 as a 51-item dichotomous self-report. This questionnaire could assess cognitive restraint of eating, disinhibition, and hunger. 10 This scale was refined to form an 18-item questionnaire, TFEQ-R18, with a 4-point Likert scale to enhance its internal consistency and discriminant capacity. 11 It assessed the cognitive and behavioral aspects of eating in three domains: Cognitive Restraint, Emotional Eating, and Uncontrolled Eating. The TFEQ-R18 was further revised to improve its construct validity by adding three more items to the Emotional Eating domain. This resulted in TFEQ-R21. 12 However, a confirmatory factor analysis (CFA) indicated a refinement to this 21-item questionnaire. Accordingly, the TEFQ revised 18-item version 2 (TFEQ-R18V2) was formulated in 2009 by removing three items on the Cognitive Restraint domain of TFEQ-R21, identified as weak items with low loadings. 13 This latest version retained the three domains of Cognitive Restraint, Emotional Eating, and Uncontrolled Eating, and had a robust factor structure and good reliability. 13
Across the globe, different versions of the TFEQ have been used to describe disordered eating patterns among PwS. 1 However, translations in Indian languages, including Tamil, have not been validated. In this study, an initial CFA was performed to evaluate the existing three-factor structure of TFEQ-R18V2 in our population, as CFA can give valuable information regarding the fit of the data to the specific, theory-derived measurement model. The strength of CFA lies in its disconfirmatory nature, wherein models or theories might be rejected in a specific population. Still, results might also indicate potential modifications to be investigated in subsequent exploratory factor analyses (EFAs). 14 Hence, this study aimed to assess the factor structure and reliability of the Tamil-translated version of the TFEQ-R18V2 among Tamil-speaking PwS.
Materials and Methods
Study Setting
The study was conducted at the Schizophrenia Research Foundation, Chennai, India, a tertiary mental health service center with outpatient and inpatient services. Tamil-speaking persons from urban and rural areas comprise most service users who primarily access the services for treating severe mental illnesses. This study was carried out after receiving approval from the Institutional Ethics Committee.
Sample Size Calculation
A sample size of 90 was required to carry out the factor analysis of TFEQ-R18V2 as there are 18 items in the questionnaire, and at least 5 responses per item are recommended. 15
Participants
Participants were recruited through consecutive sampling after checking their eligibility criteria. Persons attending the outpatient service of the study setting who were 18–65 years old and diagnosed with schizophrenia according to International Classification of Diseases, Tenth Revision (ICD-10) were included after obtaining their written informed consent.
Persons who reported having gastrointestinal pathology, like oral or liver pathology, or had undergone abdominal surgery were excluded. PwS with a comorbid diagnosis of intellectual disability disorder or stroke were also excluded.
Measures
Sociodemographic and Anthropometrics Scales
A semi-structured form was used to gather sociodemographic and clinical information, namely age, sex, place of residence, education, employment status, and duration of illness. The severity of schizophrenia at the time of recruitment was assessed using the Scale for the Assessment of Positive Symptoms (SAPS) and the Scale for the Assessment of Negative Symptoms (SANS).16,17 SAPS and SANS scores were reported as the sum of global scores of each domain of the respective severity measures. The height (in cm) and weight (in kg) of the participants were recorded following the standard WHO measurement protocol, 18 and their body mass index (BMI) (in kg/m2) was calculated.
Three-Factor Eating Questionnaire-R18V2 (TFEQ-R18V2)
TFEQ-R18V2 13 assesses patterns of disordered eating using 18 items spread across three subscales. Of the three subscales, the Uncontrolled Eating subscale assesses the tendency to lose control over eating when feeling hungry or exposed to external stimuli. The Cognitive Restraint subscale assesses the tendency to control food intake to influence body weight and shape. The Emotional Eating subscale measures the propensity to overeat owing to negative mood states, for example, feeling lonely, anxious, or depressed.
The 18 items of the tool are scored on a 4-point response format. The responses for the first 16 questions range from 1 to 4, where 1 = Definitely True, 2 = Mostly True, 3 = Mostly False, and 4 = Definitely False. Items 17 and 18 were also scored on a 4-point scale where the ratings measure the frequency of DEB. Before calculating the sum of scores, the responses to questions 1–16 are reverse coded so that higher scores in a domain mean a higher disordered eating pattern. The total score for the 18 items ranges from 18 to 72.
The Tamil Version of TFEQ-R18V2
The research team obtained the Tamil-translated version of TFEQ-R18V2 from the original author, who certified that the translation followed the linguistic validation process recommended by the MAPI Research Institute. 19 The linguistic validation process undertaken by the original author included forward translation of the TFEQ-R18V2 tool from English into Tamil by two qualified translators, reconciliation of the two Tamil-translated versions, back translation from Tamil to English by a qualified translator, cognitive interview with five patients with obesity, and proofreading of the final version.
Procedure
The Tamil-translated version of TFEQ-R18V2 was circulated to four experts in the field of eating disorders and schizophrenia, who assured the linguistic equivalence of the 18-item tool.
Subsequently, the final translated version of the tool was used to collect data from the study participants. Data were collected for three months (January–April 2022). After providing written informed consent, 135 participants shared their sociodemographic details and completed the Tamil version of the TFEQ-R18V2. Trained research staff was available to address participants’ queries and ensure the questionnaire’s completeness. Thirty willing participants completed the tool after two weeks to test the temporal stability of TFEQ-R18V2.
Participants’ identifiable information was removed from their responses and replaced with study IDs to preserve privacy and anonymity.
Data Analysis
The data were analyzed using STATA version 16.1. The sample was described using sociodemographic variables, symptom severity, duration of illness, and BMI. Internal consistency and temporal stability of TFEQ-R18V2 were determined through Cronbach’s α measure and the intraclass correlation coefficient (ICC). Test–retest analysis was performed. A two-way mixed effects model was used to calculate the ICC where raters/participants’ effects are random and measure effects are fixed.
CFA of the original 18-item tool was performed. Fit indixes calculated included the root mean square error of approximation (RMSEA) with a goal of 0.05 for a good model fit, comparative fit index (CFI), and Tucker–Lewis index (TLI). Initial CFA was followed by an EFA using the principal component analysis method with Varimax rotation to test the loading strength of items on factors. Factors that had eigenvalue > 1 and items that had loading > 0.5 were retained. The correlations between the factors were studied using Spearman’s rho.
Results
Sample Characteristics
Table 1 describes the sociodemographic and clinical details of the sample in terms of their mean (± standard deviation [SD]) and number (%).
Sociodemographic and Clinical Details (N = 135).
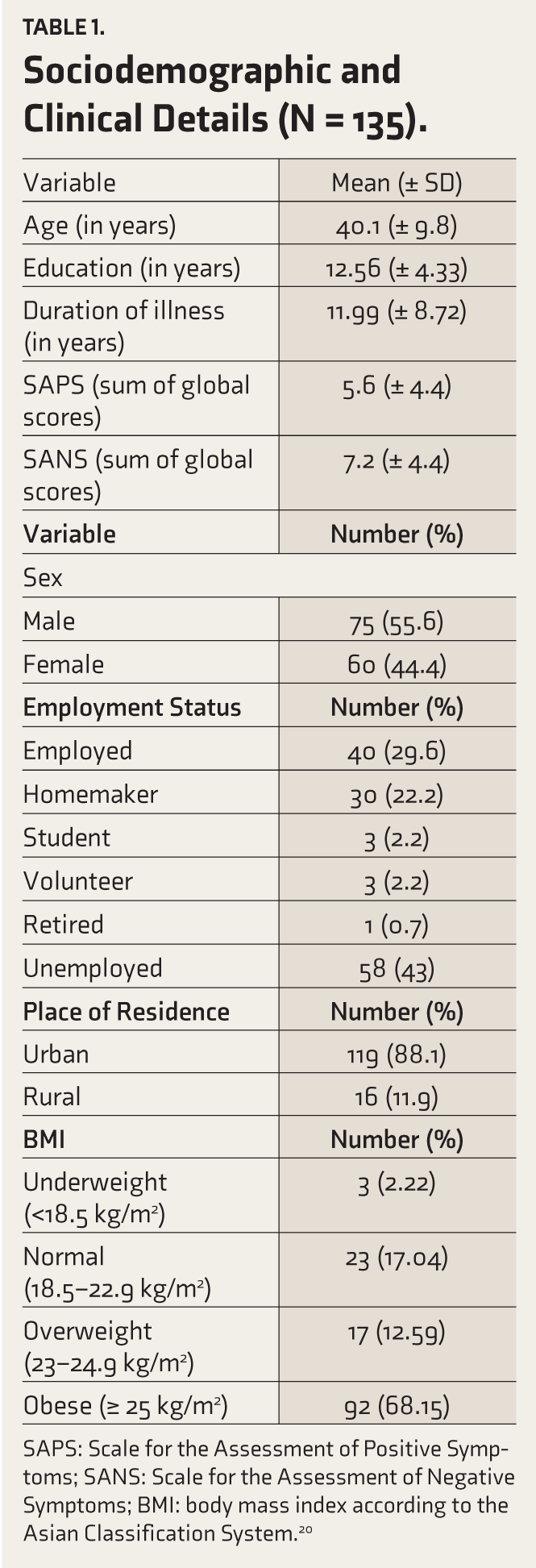
SAPS: Scale for the Assessment of Positive Symptoms; SANS: Scale for the Assessment of Negative Symptoms; BMI: body mass index according to the Asian Classification System. 20
The sample had relatively more males, and most were from urban areas. The mean BMI of the sample was 27.72 (± 5.46) kg/m,2 and more than 80% fell under the overweight and obese categories.
Reliability of TFEQ-R18V2
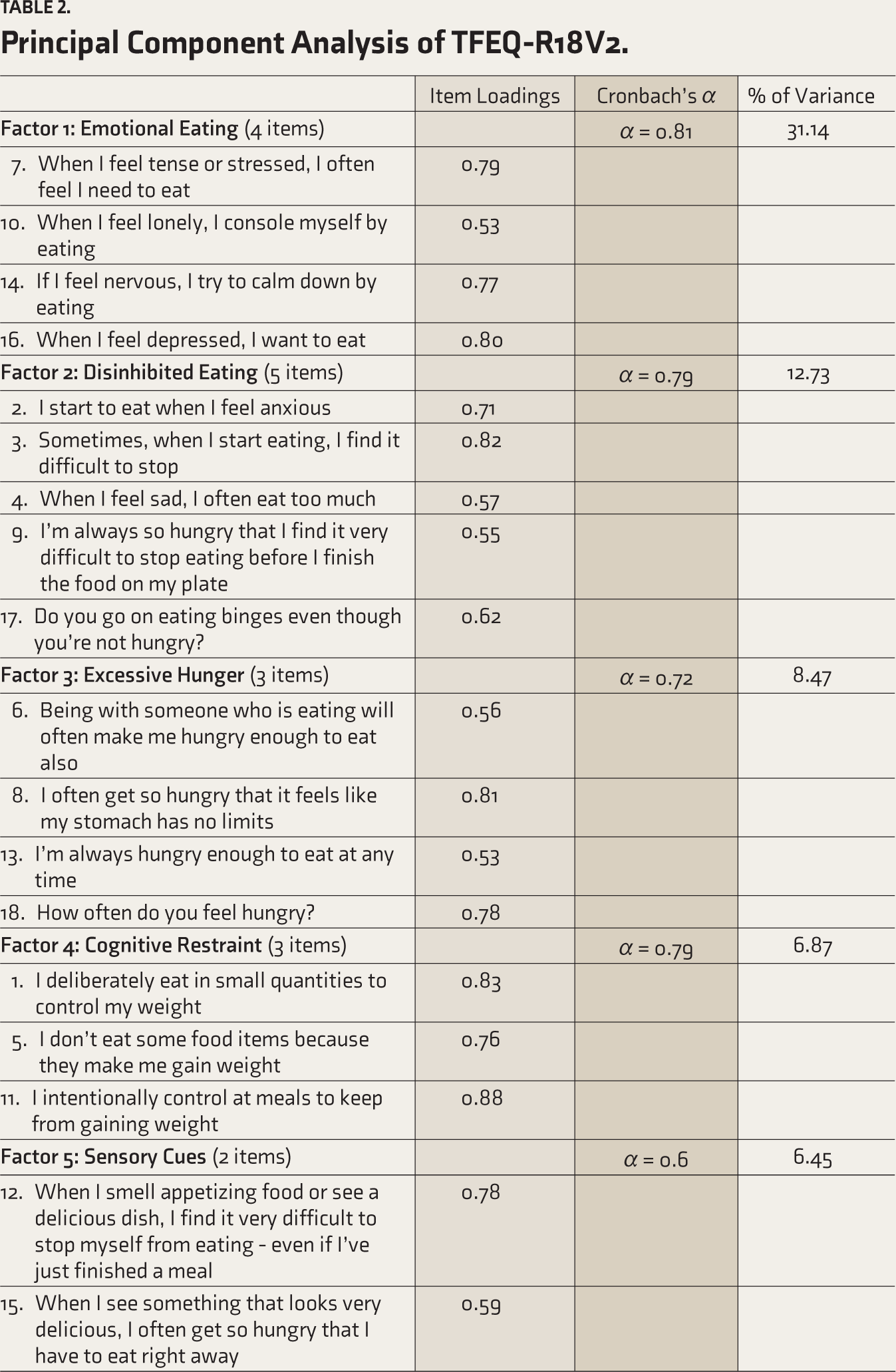
The internal consistency of TFEQ-R18V2 demonstrated by Cronbach’s α was 0.84. The internal consistency of the factors that emerged from EFA ranged between 0.6 and 0.81 (Table 2).
Principal Component Analysis of TFEQ-R18V2.
The test–retest reliability of TFEQ-R18V2 calculated using the ICC gave a statistically significant score of 0.53 (95% CI, 0.17–0.78, p < .05).
Factor Structure of TFEQ-R18V2
Confirmatory Factor Analysis
The CFA gave an RMSEA value of 0.10, the CFI was 0.79, and the TLI was 0.76, suggesting a poor fit.
Exploratory Factor Analysis
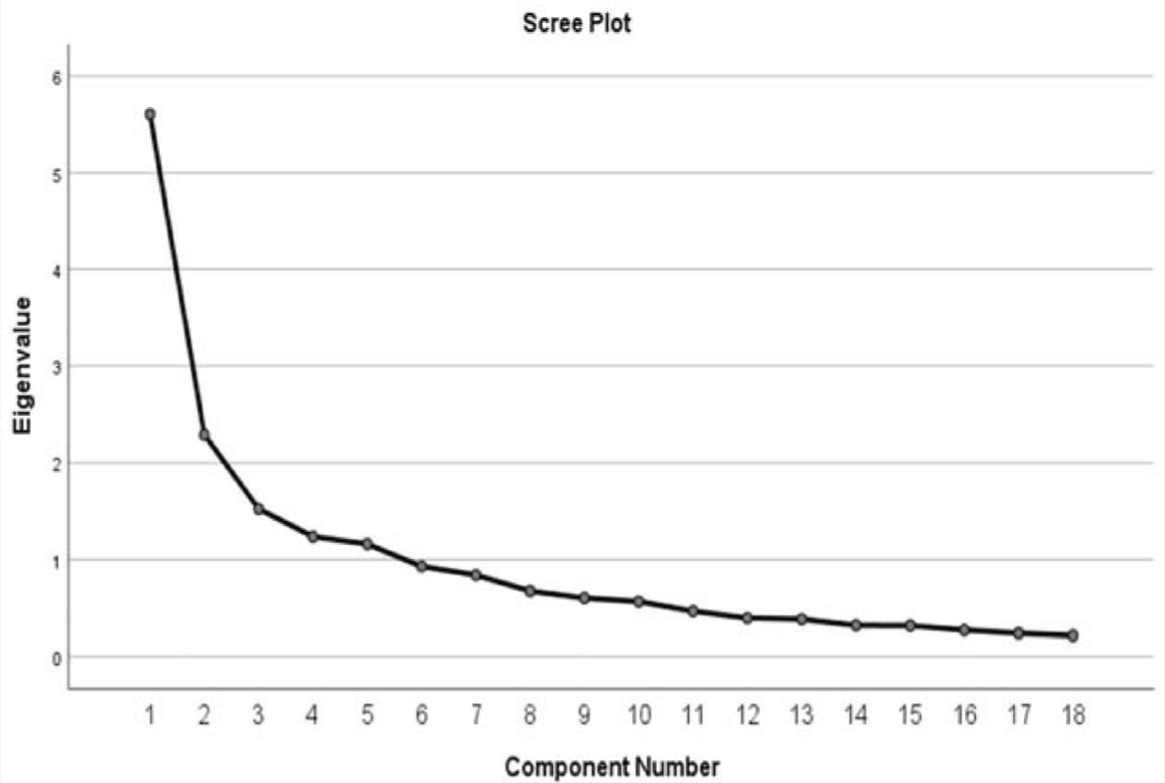
The 18 items of TFEQ-R18V2 converged over five factors. These five factors could explain a variance of 65.67%, and factors beyond the first five accounted for lesser variability, as shown in the scree plot (Figure 1). Kaiser–Meyer–Olkin measure of sampling adequacy came to be 0.804, and Bartlett’s test of sphericity was significant with p < 0.001. The item loadings, internal consistency (Cronbach’s α value), and the percentage of variance of each factor are presented in Table 2.
Scree Plot with Eigenvalues of Items on TFEQ-R18V2.
The research team labeled each of the five factors to capture the significance of the items in the most appropriate manner. Item loadings ranged from 0.53 to 0.88. Table 2 shows the variance explained by each factor and the individual item loading.
The correlations between the five factors of TFEQ-R18V2 are shown in Table 3. A moderate correlation was seen between Emotional Eating, Disinhibited Eating, Excessive Hunger, and Sensory Cues. Disinhibited Eating showed a weak correlation with Cognitive Restraint.
Correlations Between the Five Factors of TFEQ-R18V2
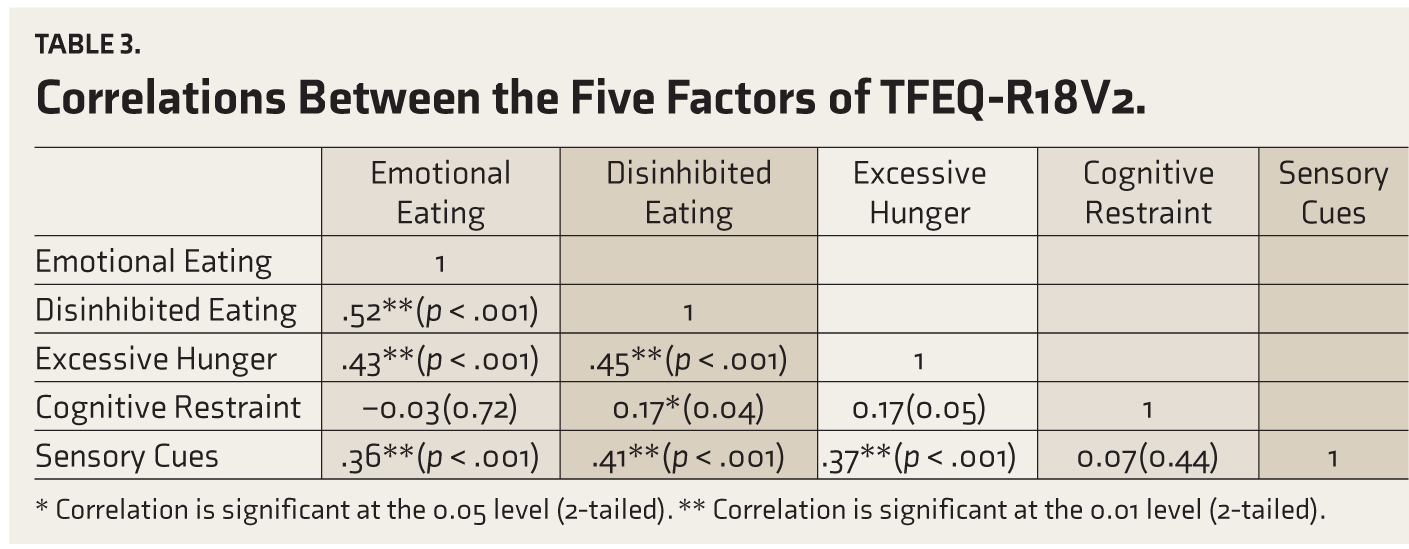
* Correlation is significant at the 0.05 level (2-tailed). ** Correlation is significant at the 0.01 level (2-tailed).
Discussion
To the best of the authors’ knowledge, this is the first study to investigate the reliability and factor structure of the Tamil version of the TFEQ-R18V2 among Tamil-speaking PwS. This validation exercise was part of a larger study to determine the proportion of disordered eating among PwS in a tertiary mental health service provider in Chennai. Since standardized tools to assess disordered eating were unavailable in Tamil, a popular tool, TFEQ-R18V2, was used for validation in Tamil.
The face and content validity of the Tamil version of TFEQ-R18V2 was ascertained by four mental health professionals who assured that the items in Tamil were appropriate and understandable. The Tamil version of TFEQ-R18V2 demonstrated good internal consistency, similar to the findings of another study. 21 The test–retest reliability of the tool revealed that it had moderate temporal stability.
EFA of the Tamil version of TFEQ-R18V2 gave a five-factor structure for this sample in contrast to the original three-factor structure. 13 Although the factors that emerged in the EFA differed from the original, some themes from the original subscales were preserved, and no items were excluded.
The Emotional Eating factor of the five-factor structure retained four of the six items from the homonymous subscale of the English TFEQ-R18V2. These items outlined the desire to eat to assuage negative emotional states such as loneliness and depression. 22
The Disinhibited Eating factor contained two items from the Emotional Eating subscale and three from the Uncontrolled Eating subscale of the English version. 13 Together, the five items reflected a sense of losing control over eating due to internal or external factors. Literature has outlined that negative emotions cause a lack of self-control, leading to overeating, while individuals attempt to restrain themselves from eating. Suppressed hunger might take over and lead to disinhibition in the grip of emotions. 23
Items comprising the Excessive Hunger factor in the five-factor structure explained the subjective feeling of hunger as a response to a sense of loss of control. These items were listed under the Uncontrolled Eating factor in the English version. 13 Previous studies have shown increased hunger on TFEQ-18 in overweight or obese individuals.24,25 Our sample included individuals with higher BMI values who were predominantly overweight/obese. This could explain the emergence of Excessive Hunger as a separate factor in the current study.
The Cognitive Restraint factor retained all the items in the same name’s subscale in the English version. The construct of a conscious effort to restrain oneself from eating captured by the Cognitive Restraint factor is a robust construct captured by other scales that assess disordered eating patterns. 26
Two items focusing on taste and smell and visual cues converged into the factor Sensory Cues. These items encapsulated participants’ hunger triggered by environmental cues. These correlated with each other, and the original latent factor of Uncontrolled Eating did not sufficiently explain them, similar to the findings of a previous study. 21 Traditionally, Indians emphasize appreciating the eating process with the maximum number of senses; thus, sensory cues are an important cultural aspect of the Indian way of eating. 27 These “appetitive traits” or characteristics, such as food-associated cues and appetite, influence eating behaviors. The observed differences in factors may be a manifestation of prevailing cultural practices, choices, and belief systems, including attitudes toward food, which influence eating behaviors.28,29
The correlation between the four factors of Disinhibited Eating, Excessive Hunger, Emotional Eating, and Sensory Cues observed in our study may be explained by the overlap of items across the original factors of Uncontrolled Eating and Emotional Eating. Disinhibition is a tendency for overeating and eating opportunistically in an obesogenic environment, typically in response to negative affect or excess hunger. 30 While our sample perceived the loss of control in eating, emotion, and sensation-triggered eating tendencies, and excessive perception of hunger as separate constructs, previous studies have explained the role of craving as an underlying mechanism to understand the correlation between the factors as seen in our study. 31 However, Cognitive Restraint was poorly correlated to Disinhibited Eating and was perceived as a stand-alone construct not associated with environmental or internal triggers.
Based on the findings, the Tamil version of TFEQ-R18V2 is a useful tool to assess the disordered eating patterns among Tamil-speaking PwS. As a short 18-item self-report tool, the Tamil version of TFEQ-R18V2 is an ideal tool to assess the patterns of disordered eating in PwS attending a clinical setting. Timely identification of disordered eating patterns among PwS can ensure better care and management of DEB and prevent it from developing into an eating disorder. Screening PwS using the Tamil version of TFEQ-R18V2 can be the first step to achieving that.
Since the current study focused on PwS, the findings of this study may not be generalizable to the Tamil-speaking population without schizophrenia. Although the content validity index of the Tamil version of TFEQ-R18V2 was not evaluated, four Tamil-speaking mental health professionals with expertise in schizophrenia and eating disorders assured the linguistic equivalence and the content validity of the Tamil version. Though a wide range of recommendations regarding sample size in factor analysis have been made, and this study could have used a bigger sample size, Gorsuch (1983) recommended five subjects per item, with a minimum of 100 subjects, regardless of the number of items. 32
In conclusion, this study identifies that the Tamil version of TFEQ-R18V2 emerges with five factors to screen PwS for disordered eating patterns. Future studies need to focus on confirming its factor structure using CFA in a similar population with a larger sample size.
Footnotes
Acknowledgements
We thank the original author, Dr. Jan Karlsson, for providing us with the Tamil-translated version of the TFEQ-R18V2 for validation and further usage.
Author Contributions
PA, LV, AS, and PR were responsible for the concept and design of the study. whilst SG, NH, VM, and JD were involved in data acquisition, analysis, and interpretation. All authors were involved in the drafting of the manuscript. The final manuscript was approved by all the authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Statement
This study was reviewed and approved by the Institutional Ethics Committee of Schizophrenia Research Foundation, Chennai, India.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.