
Abstract
Background:
Training the old-age home staff is essential in raising geriatric mental health care standards in India. Inadequate knowledge on ageing and psychosocial interventions is a significant issue in old-age homes. Old-age home staff must know how to provide individualized psychosocial care and support for older adults. Hence this study aimed to test the feasibility of the psychosocial care training program for the staff working in old-age homes.
Methods:
A quasi-experimental research design (pre-post without a control group) was used. Forty-two staff members participated. Mary Starke Harper Aging Knowledge Exam (MSHAKE) and structured checklist to measure the staff’s knowledge on ageing, psychosocial interventions, welfare legislations, schemes, and support services were administered before, immediately after, and two months after the program and the self-efficacy checklist was administered immediately and two months after the program, to examine the efficacy of the program.
Results:
Significant improvement was found in the ageing knowledge and the knowledge of psychosocial intervention and psychosocial care. These improvements continued for two months (p < .001). Similarly, their self-efficacy in managing such problems was also sustained across two post-measurements (p = .045).
Conclusions:
Face-to-face training programs would enhance the knowledge of the old age home staff. This Psychosocial Care Training module can be used for training old age home staff to address various psychosocial needs, concerns and other psychosocial problems of the residents.
A training intervention program improved the knowledge, skills, and practice among staff working in the old age homes. The same may be replicated for all the stakeholders, including nurses, maintenance staff and old age home managers.Key Message:
The population estimates indicate that India’s 60-plus age group will rise to 17.3 crores in 2026. The increase in life expectancy in India has contributed to the rapid growth of the population of older adults. In this context, merely increasing life expectancy is insufficient; policymakers must plan for a secure, dignified, and productive life for older adults. 1 Symptoms of depression, anxiety, insomnia, somatization, mild cognitive impairment and late-onset psychosis are seen more in Old Age Home residents, which need mental health treatment services to address their psychosocial issues. 2
Lack of trained staff is a major challenge in addressing mental health issues in OAHs.3–5 A study among OAHs residents found a major relationship of loneliness with depression and sociability. 6 A cross-sectional study in India about the prevalence of loneliness and its relationship with social connectedness and depression in the older adults living in OAHs revealed depression, loneliness and poor social support among them. 7 In India, the involvement of key stakeholders becomes mandatory, which throws light on the need for multi-sectoral collaborative services. 8 In India, there is a shortage of mental health professionals to provide mental health services to older adults.9, 10
To succeed, an OAH should have knowledgeable and skilled staff. Another major concern is the poor staff ratio to take care of residents, according to the various experts working in this sector, to ensure the quality of caregiving.11, 12 Studies from India on psychiatric morbidity in the geriatric population in OAHs underlined the need to provide comprehensive community-based geriatric healthcare programs and psychosocial care to the older adult population living in older adult care institutions.13–15 The studies suggested that comprehensive community-based geriatric healthcare programs must be formulated with vital health education components.16, 17 Many studies from abroad and India highlighted the need to provide psychosocial care services to older adults living in communities or OAHs. Training OAHs staff on geriatric mental health and associated psychosocial care services should enable them to provide comprehensive care in OAHs. Hence, this study assessed the efficacy of a psychosocial care training program for the staff working in OAHs.
Materials and Methods
The objectives of the study were to profile the staff working in OAHs and assess the efficacy of a psychosocial care training program for them. A quasi-experimental pre-post design study without a control group was adopted to study the staff of five OAHs in Bengaluru. These OAHs were selected from the list given by the Department for the Empowerment of Differently Abled and Senior Citizens, Karnataka Government. 18 The study protocol was approved by the Institutional Ethics Committee. Staff fluent in English or Kannada were included. All the participants were recruited after obtaining written informed consent. Purposive sampling was used. A total of 42 staff OAH participated in the training program. The data were collected from October 2020 to February 2021. A three-day training program was organized for the selected staff to enhance their knowledge of geriatric mental health and psychosocial interventions. On the day of training program the baseline assessment, post-assessment one was carried out, using the pre-assessment tools, and after two months of the training program, post-assessment two was carried out. Self-efficacy of the staff too was assessed at the same two time points.
The Mary Starke Harper Aging Knowledge Exam (MSHAKE), 19 was used to measure the staff’s knowledge of geriatric mental health, after translating it to Kannada. The 25 items were developed by a team of North American geriatric and mental health experts to assess aged-care workers’ basic mental health knowledge, including about normal ageing, dementia, and mental illness. There are true or false responses to the scale items, with a score of “1” for the response of “true” and “2” for “false.” The scores for all the items are summed, with a possible range of 25–50. This tool was used for measuring the knowledge of the staff on geriatric mental health. The reliability of this scale from the standardized alpha of the pre-test is 0.72 and the post-test is 0.71. This scale is available in the public domain.
We prepared a structured checklist to measure the staff’s knowledge on ageing, psychosocial interventions, welfare legislation, schemes, and support services. It was translated to Kannada and validated by five experts (two psychiatric social workers, one psychiatrist, one psychologist, and one psychiatric nurse, who had experience in working with geriatric mental health and community). The 30 items were there with yes or no responses, with a score of one for the response of “yes” and a 0 for “no.” The reliability of this checklist from the Kuder-Richardson 20 coefficient of the pre-test was 0.92 and the post-test was 0.88.
We prepared another checklist, which was translated into Kannada and validated by five experts, to check the self-efficacy of staff. The checklist was used only during the two post-assessments, to assess the self-efficacy of staff OAH in providing psychosocial care services. They responded to ten statements on a five-point scale: strongly disagree-1, disagree-2, neither agree nor disagree-3, agree-4, and strongly agree-5. The reliability of this checklist from the Cronbach’s alpha of the post-test immediately after the intervention was 0.85 and the post-test after two months of the training program was 0.67.
Development of Psychosocial Care Training Program Module
The training module for the psychosocial care training program OAH adopted the following phases:
Need assessment through interviewing OAH residents. The researchers prepared the module through the need assessment and findings from the literature. The module was validated by five experts in the fields of geriatric and community mental health.
In the study’s first phase, a purposive sampling technique was used to select the residents of OAHs. A total of 20 residents from four OAHs situated in Bengaluru were interviewed using an interview guide. The primary focus of the interviews was to understand the psychosocial care needs of the residents and the extent to which OAHs addressed those issues. A single interview session with each of the participants was done for approximately 30 minutes. The interviews were digitally recorded and transcribed. Data were analysed using content analysis. 20
In phase 2, the psychosocial care training program module was developed based on findings from interviews and a review of the literature. The module included five chapters: ageing; Health Care Needs of the older adult; common mental health and social problems of the older population; psychosocial interventions; and orientation on welfare legislation, schemes, and support centers.
In phase 3, the module was initially sent to five experts (two psychiatric social workers, one psychiatrist, one psychologist, and one psychiatric nurse who had experience in working with geriatric mental health and community) for validation. As per their suggestions and feedback, the physical health problems and mental illness were described using case vignettes from the need assessment. The methodologies adopted in the training program were lecture method, brainstorming, games, role play, storytelling, etc. MS played the role of trainer. The module was tested in one small group to check feasibility. The sample size for the pilot study was all the staff working in the selected OAH. Totally eight staff participated in the pilot study in one OAH. The majority of the staff (n = 5) were females. The job designation of the pilot study staff was distributed as nurse (n = 1), female attender (n = 3), manager (n = 2), male attender (n = 1), and cook (n = 1). Based on the pilot study, the sample size was estimated, and five OAHs with all the staff members were included in the study.
Statistical Method
Descriptive statistics such as mean, standard deviation, frequency and percentage are used to summarize the data. Repeated measure ANOVA (RM ANOVA) was used to find significant differences in the mean MSHAKE scores and checklist scores to assess staff’s knowledge on ageing, psychosocial interventions, welfare legislations, schemes, and support services. Pairwise comparisons were done with the RM ANOVA test and Bonferroni post-hoc analysis. Paired t-test was used to find significant differences in the mean self-efficacy score between two-time points. SPSS was used for analysis.
Results
The study sample consisted of 42 staff members working in five different OAHs. Four OAHs were run by charitable societies, while one OAH was managed by a private agency. Most participants (n = 24) were female. The mean age of staff score was 35.38 years and SD 14.13. The majority of (n = 35) of the staff followed the Hindu religion. Kannada was the mother tongue for majority (n = 34). Most (n = 39) were from Bengaluru city and the rest were from other parts of Karnataka. Most had studied up to under graduation (n = 22), and the remaining had studied up to secondary level (Class 8th to Class 10th). The job designations were nurse: (n = 11), female attender (n = 10), manager (n = 7), male attender (n = 6), counsellors (n = 4), and cook (n = 4).
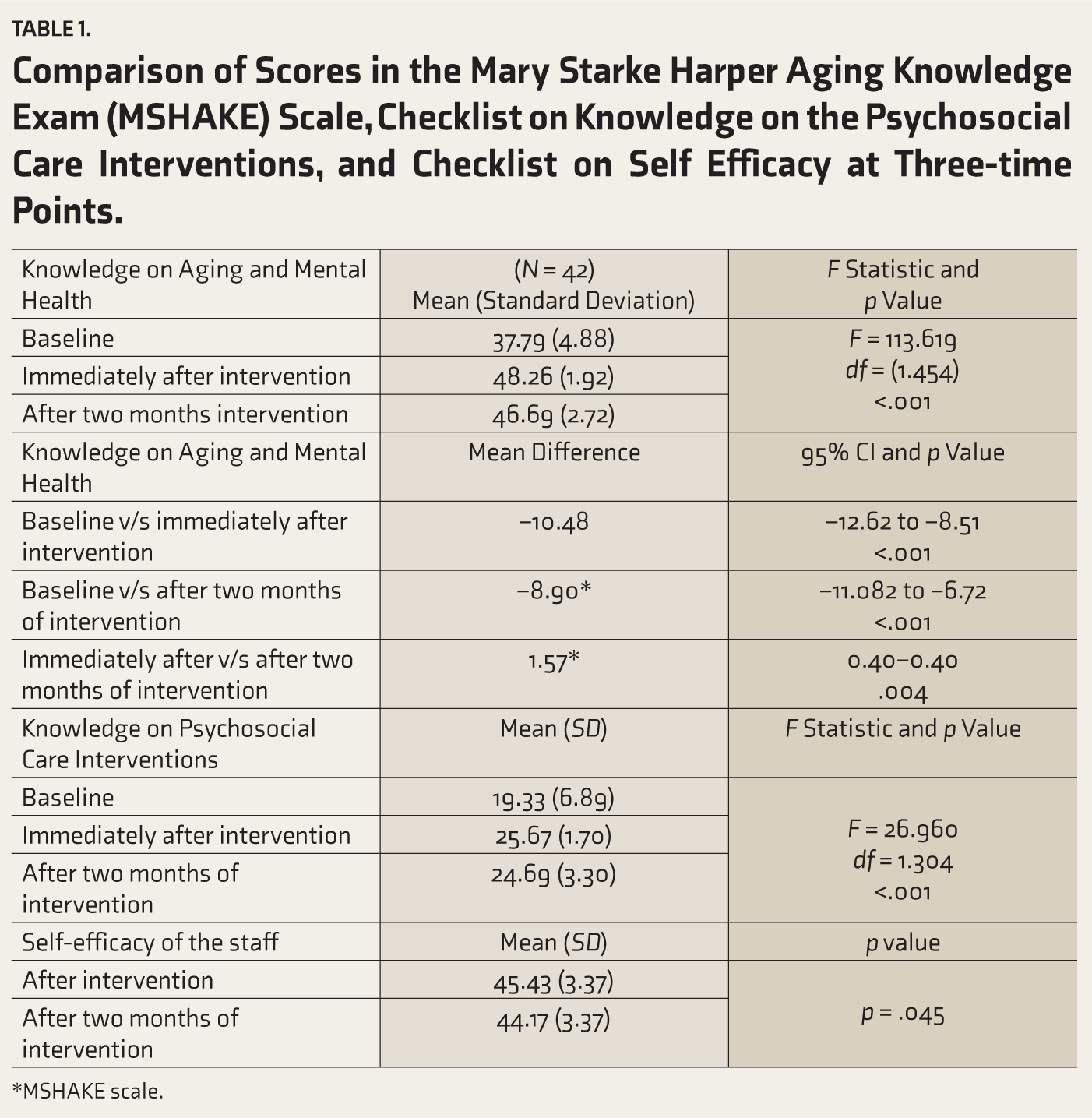
Table 1 compares the knowledge on ageing and mental health among OAH staff who attended the training program, across the three-time points. The observed mean score was highest immediately after intervention (M = 48.26, SD = 1.92) compared to baseline (M = 37.79, SD = 4.88) and after two months of the intervention (M = 46.69, SD = 2.72). RMANOVA revealed that the observed change was statistically significant (p < .001).
Comparison of Scores in the Mary Starke Harper Aging Knowledge Exam (MSHAKE) Scale, Checklist on Knowledge on the Psychosocial Care Interventions, and Checklist on Self Efficacy at Three-time Points.
*MSHAKE scale.
Pretest and posttest using the checklists of knowledge on the psychosocial care interventions were completed by 42 participants. Pretest and posttest on the checklist on self-efficacy of staff were also completed by 42 participants.
A pairwise comparison of the score of knowledge on ageing and mental health between baseline and immediately after intervention was carried out using Bonferroni post-hoc analysis (Table 1). Results indicated a significant change (Mean difference = –10.48, CI = –12.62 to –8.51, p <. 001). Another pairwise comparison of scores at baseline and after two months of the intervention also showed a statistically significant difference (Mean difference = –8.90, CI = –11.082 to –6.72, p <. 001). Final pairwise comparison of scores immediately after intervention and after two months of intervention showed statistically significant change (Mean difference = 1.57, CI = 0.40–2.74, p < .01); the knowledge decreased at the follow-up after increasing at immediate assessment.
Table 1 also shows the comparison of the knowledge on the psychosocial care interventions across the three-time points. The observed mean score was highest immediately after the intervention (M = 25.67, SD = 1.70) compared to baseline (M = 19.33, SD = 6.89) and after two months of intervention (M = 24.69, SD = 3.30). RMANOVA revealed that the observed change was statistically significant (p < .001).
Mean score (M = 45.43) at first post-assessment indicated a high level of self-efficacy (Table 1). At two months follow-up, the mean score (M = 44.17) decreased slightly, though the difference between the two mean scores was statistically significant (p = .045) in the paired t-test.
Exploratory analysis of the change in the score of knowledge on the psychosocial care interventions OAH showed no statistically significant difference across three-time points between males and females. The change in the score of knowledge on ageing and mental health was statistically significant across three-time points between staff with secondary education and under graduation (p < .001). As observed at baseline assessment, staff with low education level had low level of knowledge on geriatric mental health; after the training, they could benefit more and their knowledge reached to equal level of knowledge compared to staff with high education qualification at two post-assessments. Hence the pattern of change became statistically significant across the three time points between two groups.
Discussion
Most staff were women. Previous studies also revealed that most of the staff working in OAHs were women.21, 22
Our findings indicate that the program has enhanced the knowledge on ageing, geriatric mental health and brief psychosocial interventions among the staff working in OAHs. Similarly, the self-efficacy of the staff was found to be satisfactory after the training program and even after two months. A similar program has shown significant change in the self-efficacy of staff working in ten residential care homes for older adults in the Netherlands; the training programs for the staff and collaborative evaluation by staff increased identification of depression among residents. 23 Another study in residential care settings also reported the benefits of similar training program in increasing the carers’ knowledge of depression and self-efficacy in detecting depression and reducing the barriers to seek appropriate care at both posttest and six-months follow-up. 24 Yet another study showed that level of training or education influences long-term-care staff’s knowledge and beliefs about depression and that administrators and owners of residential care centers need to actively initiate an educational program for the welfare of staff and residents. 25
In this study, participants improved their knowledge on ageing and associated mental health conditions. However, this study has not assessed the rate of identification and referrals by the staff after the training. Likewise, a mixed-method study was carried out in York city, United Kingdom, to evaluate the effects of a training program, which included theoretical training system of mentoring the care staff to reinforce the training and a care planning intervention for the management of depression, which combined psychosocial and medical approaches. The training program was positively evaluated by the recipients, the trainers, and the researcher. The ability of the care staff to detect depression improved significantly over time and their self-efficacy in managing such problems also sustained across two post-measurements. 26
Major limitations of this study are the small sample size, selection of staff from OAHs situated in an urban area, not having a follow-up assessment to check referral rates, and the use of a quasi-experimental design of a pre-post study without a control group. MSHAKE tool has not been validated in India and it may not have precisely estimated the efficacy of the intervention.
Conclusion
The study was an attempt to develop a module and training, which was found to be beneficial for staff working in the OAHs. The face-to-face training program enhanced the knowledge on ageing, mental health and psychosocial interventions among the OAH staff. Increased knowledge on psychosocial intervention OAH sustained self-efficacy in managing such problems across the time points support the relevance of this training program. Considering the benefits of this training program, such training programs should be organized for the staff working in the other OAHs to empower them to address the gap in geriatric mental health care services in OAHs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.