
Abstract
Background:
Mental Healthcare Act 2017 (MHCA) came into force on 29 May 2018. Goa State Mental Health Authority (GSMHA) notified the Mental Health Review Board on 8 February 2022, completing the important process of implementation of the act. The transition comes with challenges.
Methods:
A qualitative study was conducted with 18 practicing psychiatrists who had worked under Mental Health Act 1987 as well as MHCA 2017 through purposive sampling across Goa. Data was collected through individual interviews; analysis was done by Braune and Clarke’s framework of Thematic Analysis.
Results:
Eighteen psychiatrists participated: 4 private, 3 secondary and 11 from tertiary levels. The themes extracted were work during MHA 1987, transition, and after the implementation of MHCA 2017. Some participants reported difficulties, felt an increase in workload, and had negative emotions, while a few were neutral, indicating mixed perceptions.
Conclusion:
This study highlights the administrative struggles and moral dilemmas faced by psychiatrists in handling the new legislation. It’s imperative that the implementation of new act should be carried out with sufficient resource allocation and monitoring mechanisms.
Psychiatrists faced increased workload due to exhaustive documentation processes. Most psychiatrists had a positive experience with the concept of nominated representative.Key Messages:
Implementing the Mental Healthcare Act (MHCA) 2017 has turned out to be a Gordian knot. There is a popular Chinese fable where there is “A Chinese farmer whose horse runs away. Then all the villagers come to his home to say, ‘It’s unfortunate that your horse has ran away,’ and he replies, ‘Maybe’. The next day the horse returns with other horses, and villagers return to say, ‘Lucky you, it’s a great turn of events’, and he replies, ‘Maybe’. The same day his son tries to train a horse and breaks his leg; villagers return to say, ‘Oh, that’s bad,’ and the farmer replies, ‘Maybe’. The next day army officers come to recruit his son for war, and his son is rejected due to a fractured leg. Villagers return to say, ‘Isn’t it great’ and the farmer replies ‘maybe’.” This indicates that it is impossible to know when something happens, whether it is for good or bad. Similar is the situation since the introduction of MHCA 2017 in the country where many parts of the Act during the implementation process have turned out to be a fortune at times and misfortune at some other times.
MHCA 2017 came into force on 29 May 2018, as notified by the Ministry of Health and Family Welfare, Government of India. 1 The Member Secretary, Goa State Mental Health Authority (GSMHA), which was established under the old Mental Health Act (MHA), 1987, initiated the process of implementation of the new Act in consultation with the Chairperson of the GSMHA, that is, the Health Secretary. The Chief Executive Officer (CEO) of the Joint Secretary level was appointed to overlook the functioning of the GSMHA under the new Act as per provisions of section 121 of Mental Health Care Act, 2017, following which the charge of the State Mental Health Authority was handed over by the Member Secretary to the CEO, who in turn constituted the new state authority after consultation with the state government.2,3
Then, under the guidance of the Ex-Member Secretary, the CEO formed Mental Health Review Board (MHRB) as per section 73 of the MHCA 2017. GSMHA notified the MHRB on 8 February 2022. Goa is a relatively smaller state with an area of 3702 km 2 and two districts, north and south Goa, with a population of 14.59 lakhs as per the 2011census. GSMHA notified that the current requirement is one MHRB as per demographics. 2 There are approximately 40 practicing psychiatrists, with 22 in the government sector and 18 in private. Registration of mental health establishments and mental health professionals is yet to begin with GSMHA.
The National Mental Health Survey 2014–2016 found that the lifetime prevalence of any mental illness was 13.7%. To combat this, the Government of India came up with the strategy of the National Mental Health Policy, 2014 and MHCA 2017 to improve access to mental health services. However, the implementation of the Act has hit a roadblock due to the lack of infrastructure to meet the needs of the growing population. 4
The whole onus of responsibility is on the government to make community mental health establishments available. However, the mental health workforce is less, and the budget allocated to providing mental health services is low. 5 The new Act has been criticized to be driven by Western ideology and focusing on patient-centric treatments. The lack of adequate resources is causing hindrance to psychiatrists in delivery of mental health services. 4
Certain sections of the Act, like the formation of the MHRB, have put incredible pressure on psychiatrists by putting a microscope on involuntary admissions and supervising the protection of patients’ rights by advocating community-based care without providing adequate infrastructure. Similarly, psychiatrists are duty-bound to follow advance directives without having any access to online directory of directives 6
Due to the above mentioned reasons, the current study aimed to understand the experiences of psychiatrists working under MHCA 2017 and appraise the differences between working under MHA 1987 and MHCA 2017.
Methods
This study was done by interviewing 18 psychiatrists across Goa from July to September 2022. The participants were selected by purposive sampling. Informed consent was taken. Psychiatrists with an experience of working under the MHA 1987 for at least one year and under the MHCA 2017 for at least six months were included. Goa has one tertiary care psychiatric hospital and two district hospitals. Hence, the sample was deliberately chosen to represent all the three centers, along with a few private practitioners, with a focus on maximum variation. Participants were contacted over the phone and explained the details of the study. After that, detailed interviews were conducted at their clinic and workplace using an interview guide, taking 30–40 min.
The study was approved by the Institutional Ethics Committee. Confidentiality was maintained by assigning alphanumeric codes, instead of personal details, to evaluate the transcripts. No compensation was offered for participating in the study. They were also offered the choice to opt out of the study at any time. An extensive interview guideline was prepared, and modifications were made after conducting a pilot interview for validation by administering it to three participants who were not included as part of the analysis in the main study. The researcher who conducted interviews was excluded from participating in coding and analysis. All the participants’ age, sex, designation, years of experience, and sector of practice were obtained at the start of the interview. Interviews were conducted in English. Transcripts were not returned to participants for corrections. There were no repeat interviews conducted. The interviews were transcribed from speech to printed form. The data is stored as encrypted files on the laptop of the researchers. Two broad questions were used to initiate the interview:
“How/What were your experiences working under Mental Health Act 1987?” “How has been your experience working under the Mental Health Care Act, 2017?”
Follow-up questions were open-ended to procure details. Further questions were asked to probe and extract information with respect to functioning under relevant sections of the MHCA 2017.
Data Analysis
Qualitative data analysis was carried out by Braune and Clarke framework of Thematic Analysis, which included six steps: (1) familiarizing with the data by reading the transcripts, (2) generating codes based on the framework, (3) searching for themes by analyzing statements and categorizing them based on their ability to reflect the phenomenon of interest, (4) reviewing themes with separate headings, (5) defining sub-themes under thematic headings, and (6) writing it up. 7
The researchers analyzed and classified the interview transcripts into themes through specified codes. The coding was done manually using Microsoft Word macros. Codes were established from the extracted data. The research team did not analyze the data with predetermined codes, but the codes were allowed to flow from the transcripts to represent participants’ thoughts. The key points were summarized into themes and sub-themes for the topic. The data obtained was analyzed by two data coders independently so that the extracted themes were checked for consistency with coded extracts amongst the datasets. The themes and sub-themes obtained were debated amongst the authors for their relevance until a consensus was reached.
Results
Amongst 18 participants, 11 worked in tertiary care hospitals, four in secondary care hospitals, and three in private practice. There were seven male and 11 female psychiatrists. Ten psychiatrists had 1–5 years of practice experience, three had 5–10 years, four had 10–15 years, and one had 15–20 years.
We summarized the results into broad themes (Table 1) as follows:
Experiences during MHA 1987 Experiences during the transition from MHA 1987 to MHCA 2017 Experiences of working under MHCA 2017.
Summary of Themes and Subthemes Extracted from Coding.
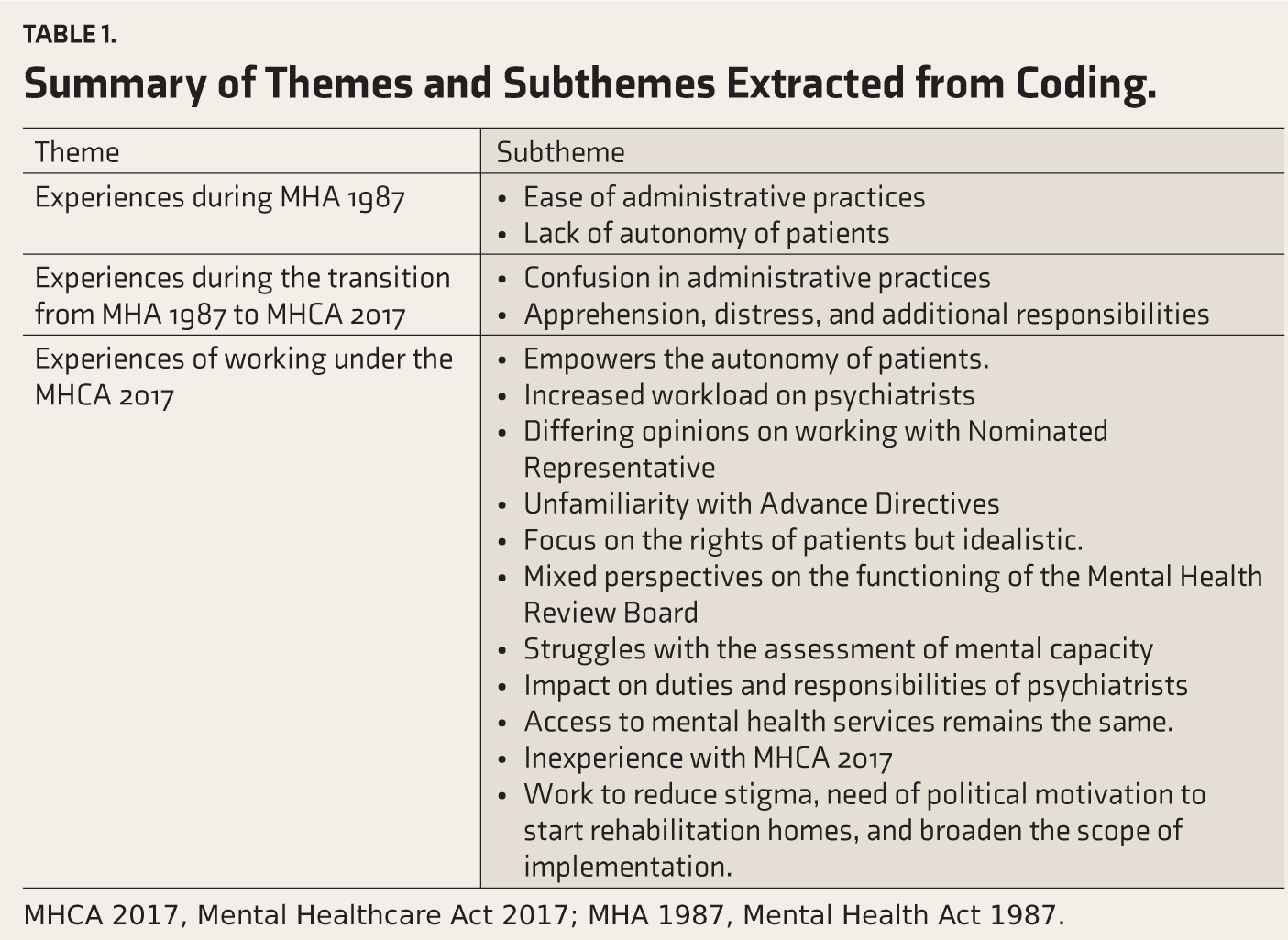
MHCA 2017, Mental Healthcare Act 2017; MHA 1987, Mental Health Act 1987.
Experiences During MHA 1987
Ease of Administrative Practices
Most responses indicated the flexibility of working under the Act, which did not require the difficult capacity assessments, involved less paperwork/documentation, and made decision-making easier.
Line 23 – It was comfortable to handle administration
Line 3 – Admissions and discharge criteria were fixed, and there was flexibility in administration
Line 2 – It was comfortable, it needed less documentation, and decision-making was easier
Line 4 – It has been better in terms of the need for documentation and paperwork
Line 5 - Special Circumstances admissions were allowed, which did not necessitate a detailed capacity assessment of clients, which is a tedious process
Lack of Autonomy of Patients
Some of the responses indicated with respect to Mental Health Act, 1987 were that patients with mental illness had minimal involvement with decision-making.
Line 1 – Patients with mental illness had minimal involvement with respect to decisions regarding admission and treatment
However, most participants reported a positive experience under the Mental Health Act, 1987.
Experiences During the Transition from MHA 1987 to MHCA 2017
Confusion in Administrative Practices
Responses received about the transition included administrative diffi-culties, complexities in the assessment of mental capacity as well as the struggle for capacity assessments in personality disorders.
Line 10 – During the initial days of transition, there was difficulty in understanding the procedure, documentation, implications and in expressing to patient about same
Line 7 – As a resident there was a need to learn and understand about capacity assessment and how to correctly do the same as well as learn about the provisions of the Act and their implications
Line 3 – …specially with respect to patients with personality disorder and under intoxication of substances. It is difficult to explain aspects of the mental health care act, 2017 and assess mental capacity in them.
Line 22 – …I was not very well versed with doing capacity assessments and was unaware regarding the functioning of the Mental health review board.
Line 14 – I believe mental capacity is a dynamic concept and not a simple yes or no assessment
Apprehensions, Distress, and Additional Responsibilities
Some participants even reported emotions such as apprehensions about mental capacity assessments, distress about documentation procedures and additional legal responsibilities, and confusion about functioning during the transition.
Line 11 – Apprehensions about capacity assessments and conversion of various admissions under MHCA, 2017
Line 8 – I was apprehensive about availability of social workers, rehabilitation units and difficulties that would be faced while working with Mental health review board
Line 17 – …in the initial days it was confusing as to understand the procedures, especially in the emergency settings.
Line 20 – I was worried about legal implications on psychiatrist
Line 13 – I was apprehensive about doing involuntary admissions and using physical restraints and was worried about availability of nominated representative
Participants reported increased workload due to changes in the working system.
Line 12 – the work hour has increased due to frequent capacity and restraints documentations
Line 24 – …getting used to new forms requiring documentation for almost every act carried out for patients like capacity, restraints etc. increases time spent on administrative work
Experiences of Working Under MHCA 2017
Empowers the Autonomy of the Patient
Participants reported mixed responses with a few reporting that it was empowering patients and promoting more independent admissions.
Line 21 – It promotes more independent admissions and number of independent admissions have increased
Line 9 – I feel it is empowering to patient to make decisions
Line 6 – Because of inclusion of rights, patients feel more responsible and can exercise control over treatment outcomes and be more compliant with treatment. They exhibit more trust towards their psychiatrists
Line 16 – Discharges happen faster, and autonomy of patient is respected
Increased Workload on Psychiatrists
Others reported negative responses such as increased workload on psychiatrists due to frequent capacity assessments and increased work hours.
Line 30 – Psychiatrists need to review the patients more frequently as according to capacity, section of admission needs to be reviewed
Line 26 – I feel the workload has increased with respect to documentation, and frequent capacity assessments adds on almost weekly increasing hospital work hours
Differing Opinions on Working with Nominated Representative
Responses with reference to the concept of nominated representative under the MHCA 2017 were that it reduces decision-making responsibilities and includes family members as part of treatment.
Line 32 – I feel the nominated representative is a good concept. The responsibility of decision making on psychiatrists has reduced because of nominated representative and makes relatives more involved in the care of the patient.
Some reported inaccessibility to nominated representatives during important treatment-related decisions.
Line 18 – work is affected as sometimes nominated representative admits the patient, leaves the patient in psychiatric ward, and does not report back for treatment-related decisions and discharge, making work difficult
Unfamiliarity with Advance Directives
Most of the participants had a neutral response stating that they are yet to come across any advance directives.
Line 14 – Have not encountered any patients with advance directives
Focus on the Rights of Patients but Idealistic
Most respondents felt that it was a positive step to emphasize the rights of the patients under MHCA 2017.
Line 28 – I feel that patients are empowered with their rights in the current Act
However, a few reported that the clauses are idealistic in the Indian scenario.
Line 23 – They are idealistic and difficult to implement. Patients are noted to misuse the same
Mixed Perspectives on the Functioning of the MHRB
Responses received with respect to functioning under the MHRB were mixed with a few indicating that legal procedures such as obtaining reception orders, handling issues related to mentally ill prisoners was easier, and the onus of responsibility to resolve ethical dilemmas was on the board.
Line 25 – MHRB has made discharges and legal procedures easier for the treating psychiatrist
Line 29 – it is good for patient care, reduces ethical dilemmas, and has a humanistic approach
However, some reported there would be more scrutiny over the working of psychiatrists and that due to the inclusion of non-medical members in the board, there are conflicts and delay in decision making.
Line 27 – I feel there will be more scrutiny over functioning of psychiatrists
Line 34 – However, involvement of non-medical members may lead to conflicts and increased time taken at times for decision-making processes
Struggles with the Assessment of Mental Capacity
Most participants reported difficulty and need for training in assessing mental capacity due to the complexity of the Indian socio-cultural setting and that it is an arbitrary concept.
Line 36 – However, patients, due to their cognitive, socio-cultural and educational levels, have difficulty comprehending nature of capacity assessment
Line 40 – I feel that mental capacity is arbitrary concept; it being a subjective assessment leads to confusion among treating doctors
Impact on Duties and Responsibilities of Psychiatrists
Most participants reported negative effects on the duties and responsibilities of psychiatrists.
Line 37 – I feel that psychiatrists are more accountable and have to maintain systematic documentation
Line 33 – I feel that work and burden on psychiatrists has increased
Access to Mental Health Care Services remains the same
The majority of responses were neutral, stating that no change has been noted in patients’ access to mental health services.
Line 39 – No change in access to mental health care
Inexperience with MHCA 2017
Some of the responses indicated that MHCA 2017 has not been followed or completely implemented in private practice
Line 42 – I am yet to start operations as per MHCA, 2017 for admissions. I’m in private. I provide mostly OPD services
Line 47 – I cannot comment much as I have not done any admissions apart from voluntary admissions, and I am yet to understand nuances of other admission processes
Decreasing Stigma, Need for Political will, and Rehabilitation Homes to Broaden the Scope of Implementation
Some of the suggestions made about MHCA 2017 were to enhance awareness, community-targeted education regarding the Act, availability of provisions of mental health insurance, and use of political power to make mental health services available to communities.
Line 50 – At an individual level, enhancing awareness, decreasing stigma, and increasing the conversation around mental health remain important
Line 53 – Education of communities regarding implementation of the Act
Line 57 – Mental health curriculum as part of education and insurance for mentally ill patients
Line 64 – Requires political will to ensure all services are made available
A few suggestions were made to the State Mental Health Authority that non-medical members of the MHRB and State Mental Health Authority be sensitized through psychiatric training. Some suggested making halfway and rehabilitation homes available.
Line 60 – To make MHCA, 2017 better applicable, formation of rehabilitation units and sensitization about the act amongst public is a must. Need of training regarding legal issues in Psychiatry for non-medical members of MHRB and SMHA
Line 65 – Making availability of rehabilitation homes, halfway homes
Discussion
Our study methodology was directed at individual interviews of psychiatrists to extract information to understand the dynamic experiences that came with implementing the new MHCA 2017. The responses received about experiences regarding functioning under the old MHA 1987 were markedly positive, reporting easier administration, less documentation, and easy decision-making with involuntary admissions mostly because the old Act provided psychiatrists from an administrative perspective, an implied authority to treat patients involuntarily, and had provisions largely focusing on custodial management. 8
This study captured a range of experiences during the transition between two important mental health legislations meant to govern the mental health of one of the highest populated democracies in the world with psychiatrists as its pillars. With the requirement of capacity assessment, the administration was bound to be stretched too thin for providing services. Our study found that several psychiatrists felt difficulty in capacity assessments during the admission of patients with substance use or personality disorders. Many reported difficulties in explaining the concept of capacity assessments to relatives of patients with personality disorder and substance use disorder requiring admission. Responses reflected alienness towards the functioning of the MHRB, which required psychiatrists to maintain meticulous documentation and to send regular updates to it. Our study elicited apprehensions of legal implications on psychiatrists and even about decisions to use physical restraints in agitated patients. 9 The challenges in functioning with change in legislation resulted in increased work burden due to detailed repeated documentation for capacity assessments, and the need to revise admissions under relevant sections of the Act regularly has pushed psychiatrists to their wit’s end.
The present study found mixed responses concerning working under the provisions of MHCA 2017. It was welcomed due to its right-based approach towards patients as the participants found it empowering, preserving autonomy, and making patients more compliant with the treatment. Some experienced increased work hours due to increased documentation and frequent reviews of involuntarily admitted patients. The opinion was divided among psychiatrists while functioning under the new Act, possibly because they are split between protecting the rights of patients with mental illness and being mindful of the proper delivery of mental health services. The current study found that most psychiatrists had a positive experience with the concept of nominated representative as they felt that decision-making responsibility with respect to admissions and choice of administration of medications is reduced. They felt the inclusion of relatives in decision-making processes to be productive. But some psychiatrists faced delays in treatment- and discharge-related decisions when the nominated representatives refused to turn up at the hospital. 10 Although all psychiatrists knew of the concept of Advance Directives, they had no experience treating patients with one.
The current study found that most psychiatrists emphasized that upholding patients’ rights was principal during care delivery. They were pragmatic towards a rights-based approach as per their experiences during involuntary admissions. They also recognized the vulnerability of persons with mental illness and their inability to access basic amenities, and hence needing protection under the Act. But, some felt that the idea of a rights-based approach was far-fetched with the current availability of infrastructure and that having judicial oversight to put rights above all might delay patients from getting treatment at the right time. 11 It is a precarious situation for psychiatrists who already struggle with ethical dilemmas of whether to put patients’ rights above all despite being aware of the harm it causes longitudinally in patients with substance use or personality disorders.
There were mixed responses with respect to functioning under the MHRB that it has reduced ethical dilemmas such as the difficulty of continuing inpatient care or discharge of abandoned patients into rehabilitation homes. The legal procedures are comparatively easier. They also felt they were under undue scrutiny from the Board and that the involvement of non-medical members in the board has led to unnecessary conflicts. However, one way to tackle this problem would be to encourage involvement of patients’ and carers’ experiences with mental health services to discharge their roles as MHRB representatives and to conduct short-term courses informing the functioning of MHRB, thereby reducing friction between the psychiatrists and the Board. 12
The current study found that many psychiatrists experienced significant difficulties during capacity assessments and encountered a lot of confusion. Mental capacity is the cornerstone of the Act; hence, a mandatory training program must be planned for all mental health professionals. According to the MHCA 2017, if the patient has mental capacity as per the psychiatrist’s assessment, the patient’s preferences and choices have to be respected during all treatment decisions. India being a diverse nation makes mental capacity assessment complex, which is further compounded by subjectivity. 13
The present study also found that psychiatrists felt an increased sense of responsibility for maintaining documentation, thereby increasing the burden of work. We found that psychiatrists did not experience any increase or decrease in patients’ access to mental health care services, indicating that stigma is still enduring. However, it is too early to conclude as the Act is still in the early stages of implementation.
We also found that the MHCA 2017 is yet to be followed in private settings, and many are in the process of unravelling sections of the Act for implementation, despite workshops having been conducted on the administrative practices and use of forms needed to document the administrative process. This reflects either the psychiatric practitioners’ lack of faith in the new Act or a lack of confidence in functioning under it. However, there is a need to train professionals who have interface with mental health care services in the execution of the new Act, such as police, judges, and staff of government bodies.
Psychiatrists put forth numerous suggestions such as community-focused education, keeping conversations of the MHCA 2017 open with the public to create awareness, and that political will is needed to implement the Act.
The suggestions put forth to improve the scope of implementation of the Act included the government’s active role in creating awareness of the new Act and making infrastructures such as community-based mental health services (halfway homes and rehabilitation homes) available. 14
Most nations have amended their mental health legislation according to the United Nations Convention for the Rights of Persons with Disabilities. Interestingly, even developed countries such as the United Kingdom have struggled with interpreting legislation among its mental health professionals, especially involving adults lacking mental capacity. Their studies even suggest that there is no charm in an act that solely focuses on the legal framework without considering a budget allocation to mental health services, which further adds bureaucratic work and stigmatizes mental health. Considering that most of the legislation is borrowed from the United Kingdom, we are right on track to encounter similar issues.15,16
A similar study done in India to understand the views of psychiatrists on Electroconvulsive therapy (ECT) under MHCA 2017 found that the ability to make medical decisions by psychiatrists have been swiped away by the new legislation. Concerns were voiced by psychiatrists as they were forced to adopt the newer non-medical model. The study also highlighted that the financial expenditure towards the Indian mental health services is bare minimum with less than 1% of the national budget. The Indian mental health services, crippled with resource allocation, are pushed to brink with the implementation of new legislation. 17
Conclusion
This study was designed to understand the challenges psychiatrists face during the transition and determine the gaps in the implementation of the Act in clinical practice.
It reflects the actuality of MHCA 2017 and provides insights through the lens of psychiatrists. The Act, which was thought to be over-ambitious, has done significantly well in protecting patients’ autonomy compared to its predecessor. Newer jargons, such as Nominated Representative and Advance Directives, are yet to be acquainted. With the unavailability of many facilities mandated by the law, such as halfway homes, review boards, and rehabilitation homes, psychiatrists are left to handle the legislation with one hand tied to the back. Psychiatrists are obligated to follow the law and have no choice but to evolve as per the regulations of the new Act or be held accountable by the regulatory bodies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.