
Abstract
Background:
India uses the Indian Disability Evaluation and Assessment Scale (IDEAS) for quantifying disability due to mental illness. The cutoff score for benchmark disability is 7. India has adopted International Classification of Functioning and Health (ICF) and thereby is a signatory to use World Health Organization Disability Assessment Schedule (WHODAS). Cutoff for benchmark disability in WHODAS in a community-based sample is lacking.
Methods:
The study was conducted in Jagaluru Taluk, Davanagere District, Karnataka. It is a part of an ongoing research funded by Indian Council of Medical Research. Frequency, percentages, mean, standard deviations, mode, median, Receiver Operating Characteristic Curve were used in analyzing the data.
Results:
The study included 184 persons with severe mental illness with mean age of 47 and average duration of illness (DOI) of 11 years. They had mild disability (5.99) in IDEAS. The corresponding cutoff score in WHODAS, as compared to IDEAS, when the influence of DOI is removed was 24.
Conclusions:
A shift from IDEAS to WHODAS is feasible. With the undue influence of DOI removed, both hospital and community-based samples show the score of 24 as cutoff.
Indian Disability Evaluation and Assessment Scale (IDEAS) is used to measure disability due to mental illness in India. India is signatory to use International Classification of Functioning and Health (ICF) and World Health Organization Disability Assessment Schedule (WHODAS). There is no cutoff for benchmark disability in WHODAS as evaluated in a community-based sample. Duration of Illness (DOI) influences disability scores in IDEAS to a large extent. Cutoff score for benchmark disability in WHODAS when the influence of DOI is removed is 24. A comprehensive measure including WHODAS and duration of disability taking into account disability during all phases of illness would be ideal.Key messages:
Society must empower individuals having physical and mental disabilities with the help of social measures, to provide equal opportunities and ensure equal participation. In India, the Rights of Persons with Disabilities (RPwD) Act 2016 was implemented to uphold the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD). It calls for providing fundamental rights and equal opportunities and preventing discrimination based on disability for individuals suffering from 21 disabilities, including intellectual disabilities, mental illnesses, autism spectrum disorders, and specific learning disorders. 1
Every country has unique standards for measuring and quantifying disability for individuals to avail of disability benefits. The RPwD Act mentions individuals with ‘Benchmark Disability’ as those who have not less than 40% of a specified disability. 1 While some countries rely on clinical judgment alone as the standard, countries like India have adopted the International Classification of Functioning and Health (ICF) as the Healthcare Information Technology standard for reporting functioning, disability, and health-related data. 2 Despite India adopting the ICF, due to the existing government guidelines, the Indian Disability Evaluation and Assessment Scale (IDEAS) is used to measure disability due to mental illness in India. 3 The score corresponding to 40% benchmark disability in the IDEAS is 7. 3 As a signatory to the ICF, India implies an eventual shift to the World Health Organization Disability Assessment Schedule (WHODAS 2.0), 4 a generic measure of health and disability due to medical, mental, and substance use disorders. This scale would serve to standardize disability profiling and is applicable cross-culturally.
Studies done by the authors have compared the implications of using IDEAS vs. WHODAS 2.0.5, 6 WHODAS 2.0 assesses disability over the past one month, and there is no such time frame for comparison in IDEAS. The duration of illness (DOI) accounts for 20% of the disability scoring in IDEAS, whereas WHODAS 2.0 does not take the DOI into account. The domains of measuring disability are also more comprehensive in WHODAS 2.0. The maximum score in IDEAS is 20, which translates to 100% disability. A disability of 40% would translate to a score of 8 [20X(40/100)]. But the cutoff score of disability in IDEAS is 7. This is a mathematical incongruity and poses difficulty in converting IDEAS scores into disability percentage. Besides, IDEAS is a tool used in the Indian setting only. By using the WHODAS 2.0, India will adapt to a globally acceptable and comparable standard of measuring and profiling disability in its citizens.
WHODAS 2.0 has no identified cutoff score corresponding to benchmark disability. Previous studies to ascertain the corresponding WHODAS 2.0 cutoff scores were done in hospital samples and had found that a score of 23 corresponds to the IDEAS scoring of 7 for benchmark disability. 5 Previous studies have also found that if DOI was not considered, the cutoff score of IDEAS for benchmark disability would shift from 7 to 6 and the corresponding scores in WHODAS 2.0 would become 24. 6 As per our knowledge, no community-based studies have assessed the cutoff scoring for WHODAS 2.0. The authors undertook this study to identify the cutoff score corresponding to benchmark disability in WHODAS 2.0 compared to IDEAS and fill the dearth in literature in India on the same.
Materials and Methods
Study Sample
The universe of the study consisted of persons with severe mental illness, including schizophrenia and other psychotic disorders, and bipolar affective disorders (BPAD) identified in Jagaluru Taluk, Davanagere District, Karnataka State, aged 18–99 years. This study is a part of an ongoing project funded by the Indian Council of Medical Research (ICMR) titled “Effectiveness of Community-Based Rehabilitation delivered by ASHAs for Persons with Severe Mental Illness in a Rural Community in Karnataka: A Randomized Controlled Comparison with Specialist Delivered Care”. 7 The study was conducted between October 2019 and September 2020. The Institute Ethics Committee of National Institute of Mental Health and Neuro Sciences (NIMHANS) approved the study.
Assessment Tools
Sociodemographic pro forma: Semistructured pro forma containing information on age, sex, years of education, marital status, DOI, and average income per annum (p.a.).
IDEAS: It measures disability in self-care, interpersonal activities, communication and understanding, work, and DOI. It has good internal consistency and construct validity. 8
WHODAS 2.0 12-item interviewer-administered version: A scale developed to reflect ICF, it covers the ICF domains fully and applies to mental, physical, and substance use disorders as well. It is a general measu re cutting across cultures, disorders, and settings. It has 12-item, 36-item interviewer-administered, proxy, and self-reported versions. The 12-item interviewer-administered version is simple, can be employed in five minutes, and has good face, construct, and concurrent validities. It places mental health on equal grounds with general health conditions. 4 The Diagnostic and Statistical Manual of Mental Disorders (DSM) 5 also has included WHODAS 2.0 36-item self-administered version for assessing functioning and disability. 9 The 12-item version accounts for 81% variance of the 36-item version, is adequate for brief assessments, and was used in this study.Clinical Global Impression-Schizophrenia Scale and Bipolar Version (CGI-SCH and CGI-BP): These are simple, reliable, and validated instruments to evaluate the severity of illness in schizophrenia and BPAD.10, 11
Statistical Analysis
The data was analyzed using PSPP (not an acronym, a free software for statistical analyses). 12 Frequency, percentages, mean, standard deviations (SD), mode, median, interquartile range with first quartile (Q1—lower bound at 25%) and third quartile (Q3—upper bound at 75%), and Receiver Operating Characteristic (ROC) Curve were used.
In the ROC curve, the area under the curve (AUC) and Youden’s J Static were used to determine the accuracy and the cutoff, respectively.13–17
Accuracy of the Test
It is quantified by the AUC. AUC of 0.5–0.6 is fail, 0.6–0.7 is poor, 0.7–0.8 is fair, 0.8–0.9 is good, and 0.9–1 is excellent.
Cutoff in WHODAS to Determine the “Benchmark Disability”
IDEAS was taken as the gold standard. The cutoff considered for categorizing as “benchmark disability” was 7, based on the RPWD Act, 2016.1, 3 The number of people with and without disability was used as the “state variable” in the analysis of ROC. The “test variables” were the total WHODAS scores. The ROC curve uses true positive rate (TPR), that is, sensitivity, and plots it against false positive rate (FPR), that is, 1 – specificity, for different possible cutoffs of WHODAS. Youden’s J Static, which is the best method to find the optimal cutoff, is TPR – FPR. The value of J can range from 0 to 1, 0 meaning the test is useless and 1 meaning the test is perfect. The values nearer to 1 predict a better cutoff.
When the influence of DOI was removed, the IDEAS cutoff was 6, as determined in the previous papers by the authors.5, 6 Again, total WHODAS was used as test variables against the IDEAS score state variable to determine the cutoff of WHODAS when the IDEAS score was 6.
Results
Sociodemographic Profile
The study included 184 persons with severe mental illness: 138 had a diagnosis of schizophrenia and other psychotic disorders, and 46 had BPAD. The mean age was 47 years. Most were females (58%) and married (61%) (Table 1).
Sociodemographic Details
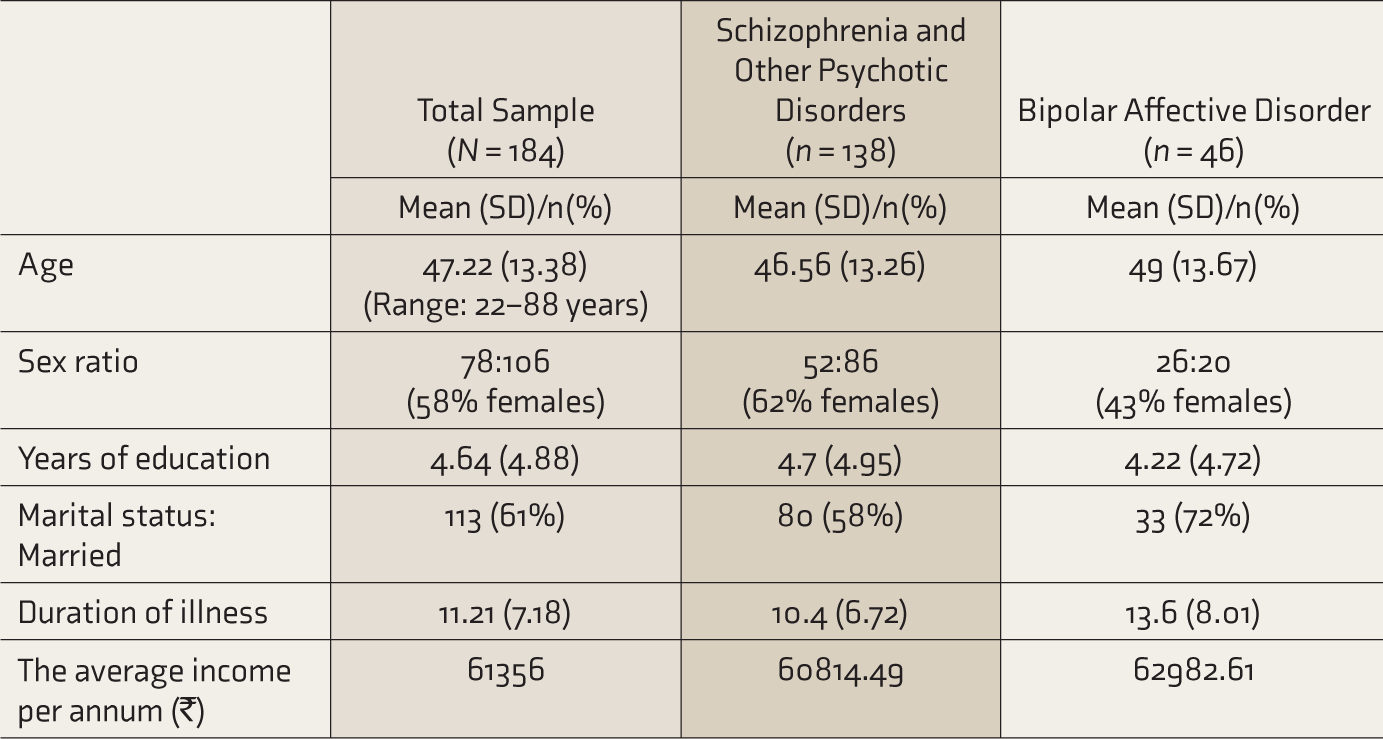
SD: standard deviation, INR: Indian rupees.
IDEAS and WHODAS Scores
In IDEAS, most patients scored 0, that is, no disability in self-care, interpersonal activities, communication and understanding, and work. The mean was <1, except for work (mean = 1.23). The majority scored 4 (mean = 3.15), that is, more than 10 years of illness, in the DOI, and had a total score of 4, that is, mild disability. For the total sample, the scores of self-care, interpersonal activities, communication and understanding, and the total were positively skewed. This may have happened as the majority had no disability in these areas. The scores of DOI were negatively skewed as the majority had higher DOI. The scores of work were not skewed (Table 2, Figure S1 and S2).
IDEAS and WHODAS Individual Domain and Total Scoring
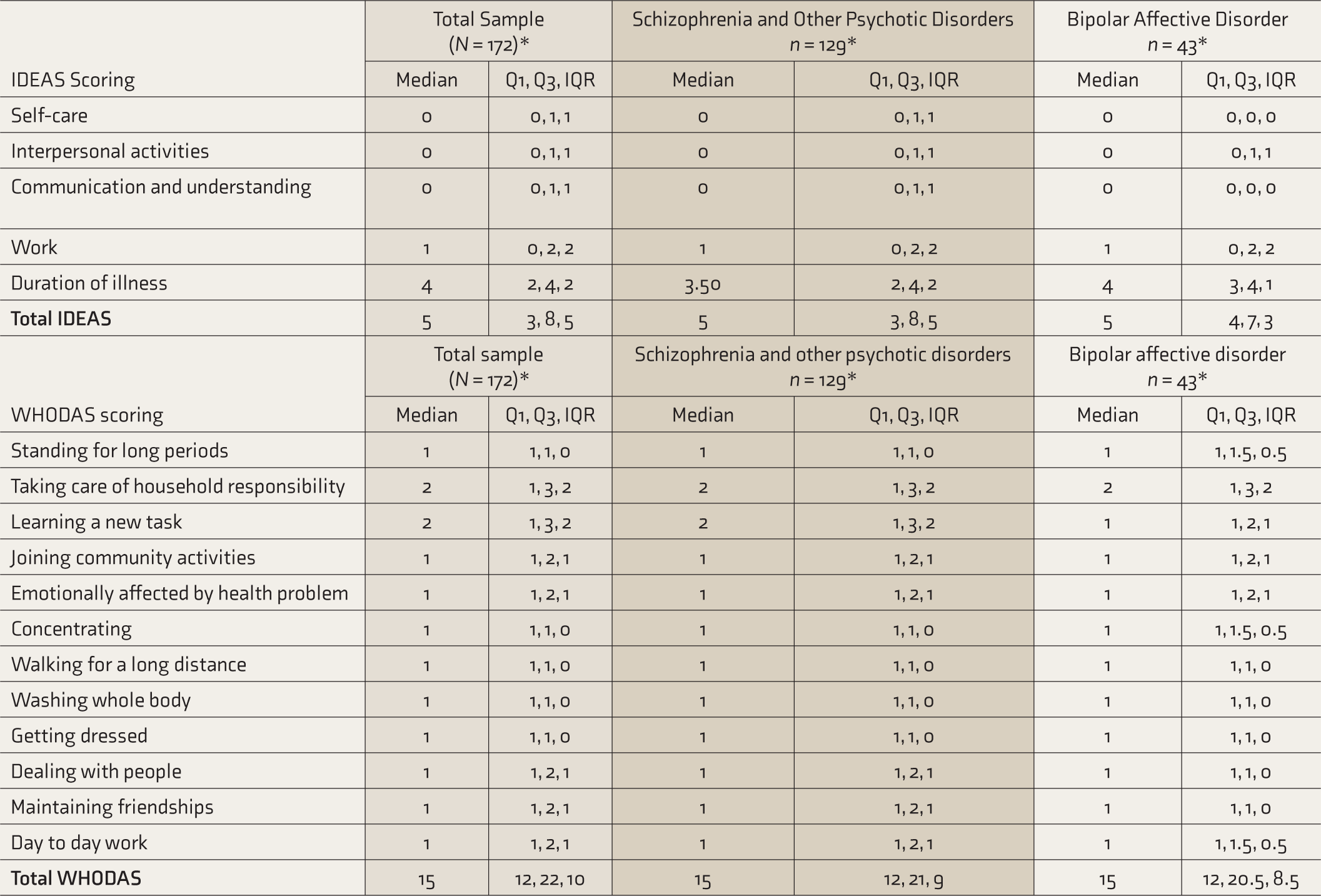
IDEAS: Indian Disability Evaluation and Assessment Scale, WHODAS: World Health Organization Disability Assessment Schedule, Q1: lower bound at 25%, Q3: upper bound at 75%), IQR: interquartile range. *N and n are less as data was missing in 12 subjects.
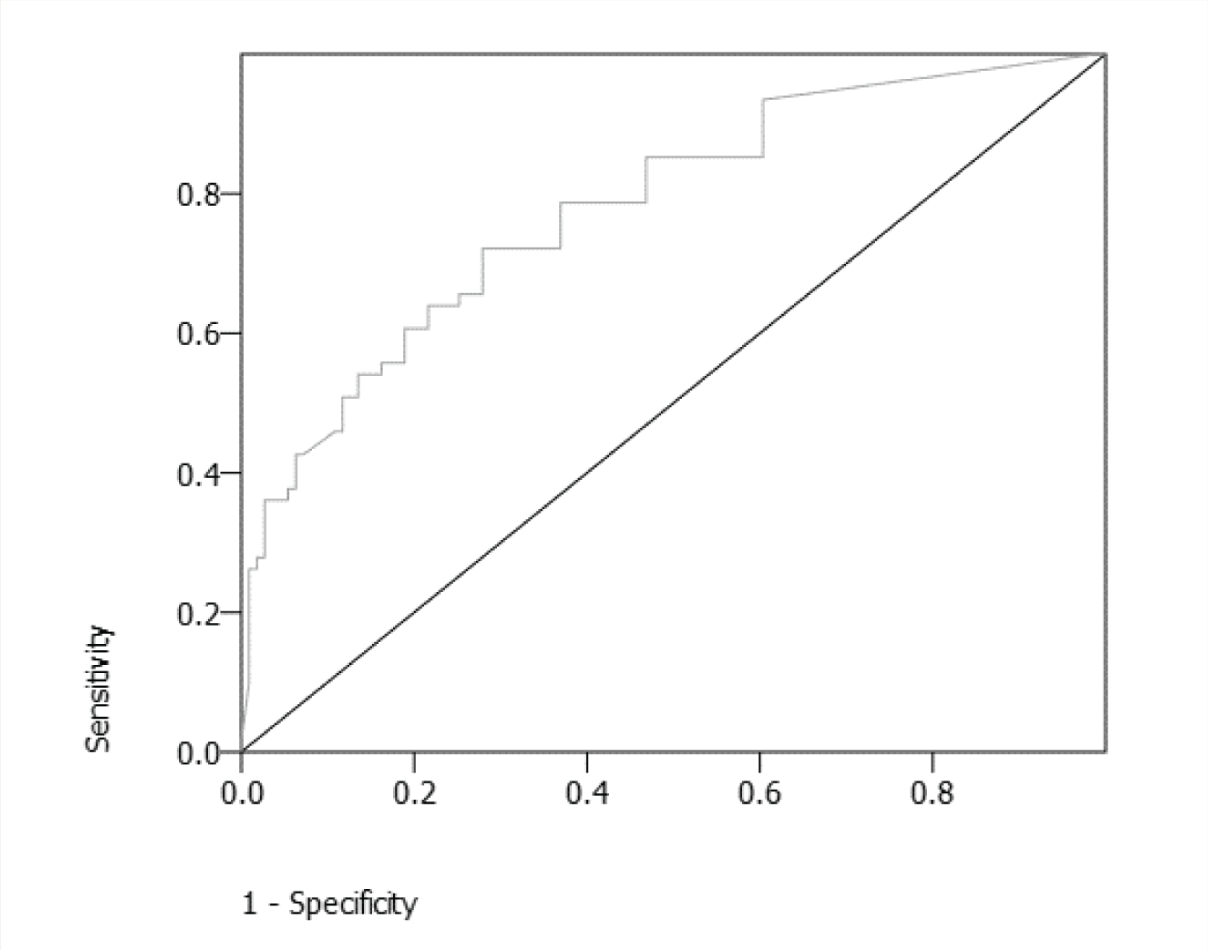
Area Under the Curve: 0.80
In WHODAS, most patients scored 1, that is, no disability, in all the domains. The mean was < 2 in all the domains except taking care of household responsibility (mean = 2.13) and learning a new task (mean = 2.01). For the total sample, there was no variability in the middle 50% of the data for the scores of standing for long periods, concentration, walking a long distance, washing the whole body, and getting dressed. The scores of joining community activities, emotionally being affected, dealing with people, maintaining friendships, work, and the total were positively skewed. Zero variability and positive skewing may have been due to the majority not having disability in these areas. The scores for taking care of household responsibilities and learning a new task were not skewed (Table 2, Figures S3 and S4).
Severity of Illness and Disability
Patients were normal to minimally ill in both schizophrenia (with a CGI score of 1.91 [SD: 1.37]) and BPAD (with a CGI score of 1.63 [SD: 1.50]) groups. They overall had a mild disability in IDEAS (5.99) and WHODAS (18.22).
The Cutoff for WHODAS as Compared with IDEAS
The corresponding score in WHODAS for 7 (the cutoff for benchmark disability) was 17 (Figure 1, Table 3a). The total WHODAS scores were in the range of 12–55. TPR, FPR, and J were calculated for each of these WHODAS total scores (Table 3a). The Youden’s J static for scores of 17 and 18 was the nearest to 1 and was 0.39. We considered WHODAS score 17 for the calculations as the average of 16 and 17 (0.385) was more than that of 18 and 19 (0.38).
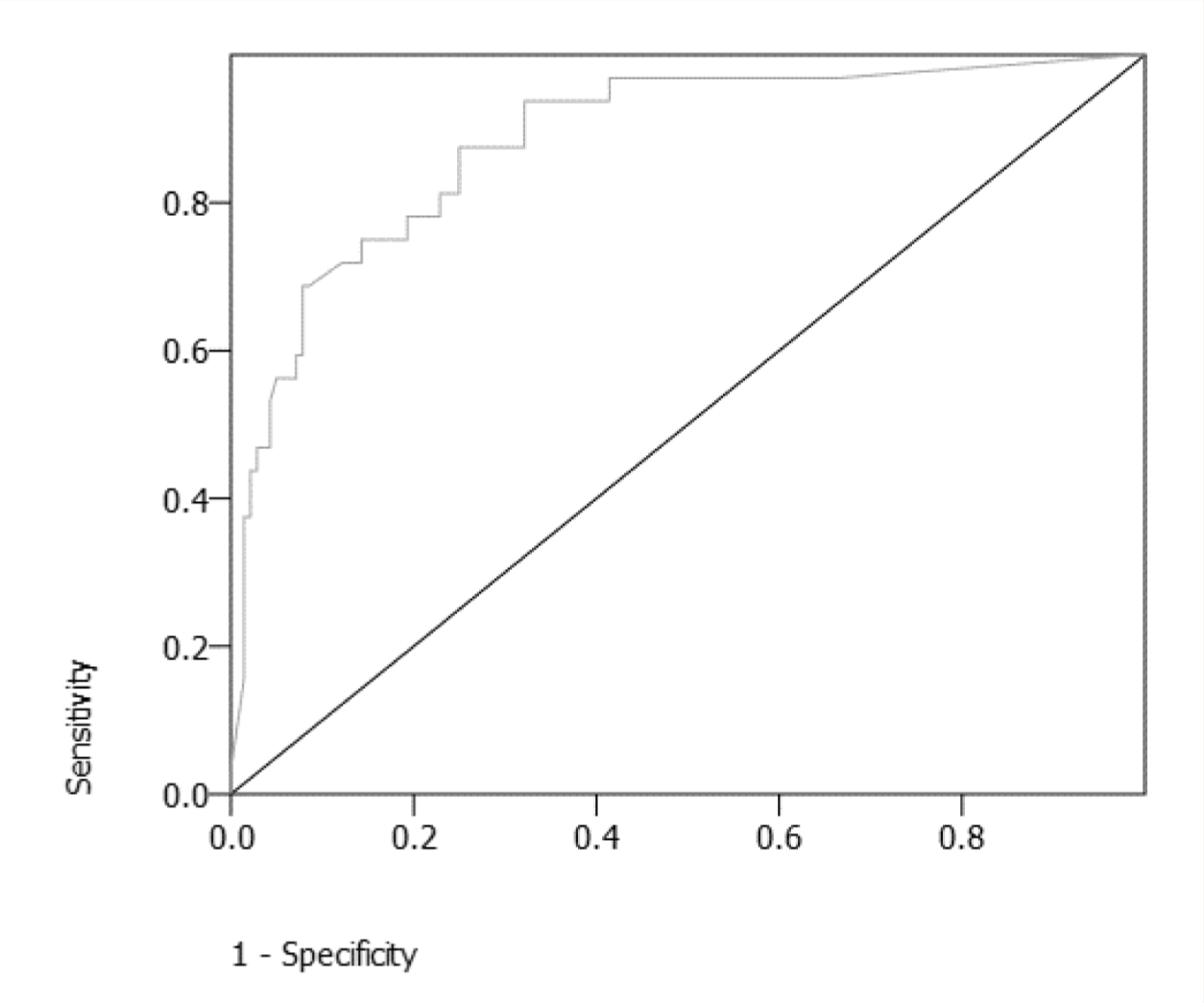
Area Under the Curve: 0.89
When the influence of DOI was removed, the corresponding score was 24 in WHODAS (for the IDEAS score of 6) (Figure 2 and Table 3b). Again, the total WHODAS scores were computed against the IDEAS score of 6 as the state variable. TPR, FPR, and J were calculated. The Youden’s J static for the score of 24 was 0.6 (nearest to 1). A previous paper by the authors had measured the impact of DOI on the disability scores.
6
We performed similar calculations in the present study and made the following observations:
The ROC curve was more accurate (AUC: 0.89 vs. 0.80; i.e., fair vs good). The cutoff in WHODAS was 24.
Youden’s J Static
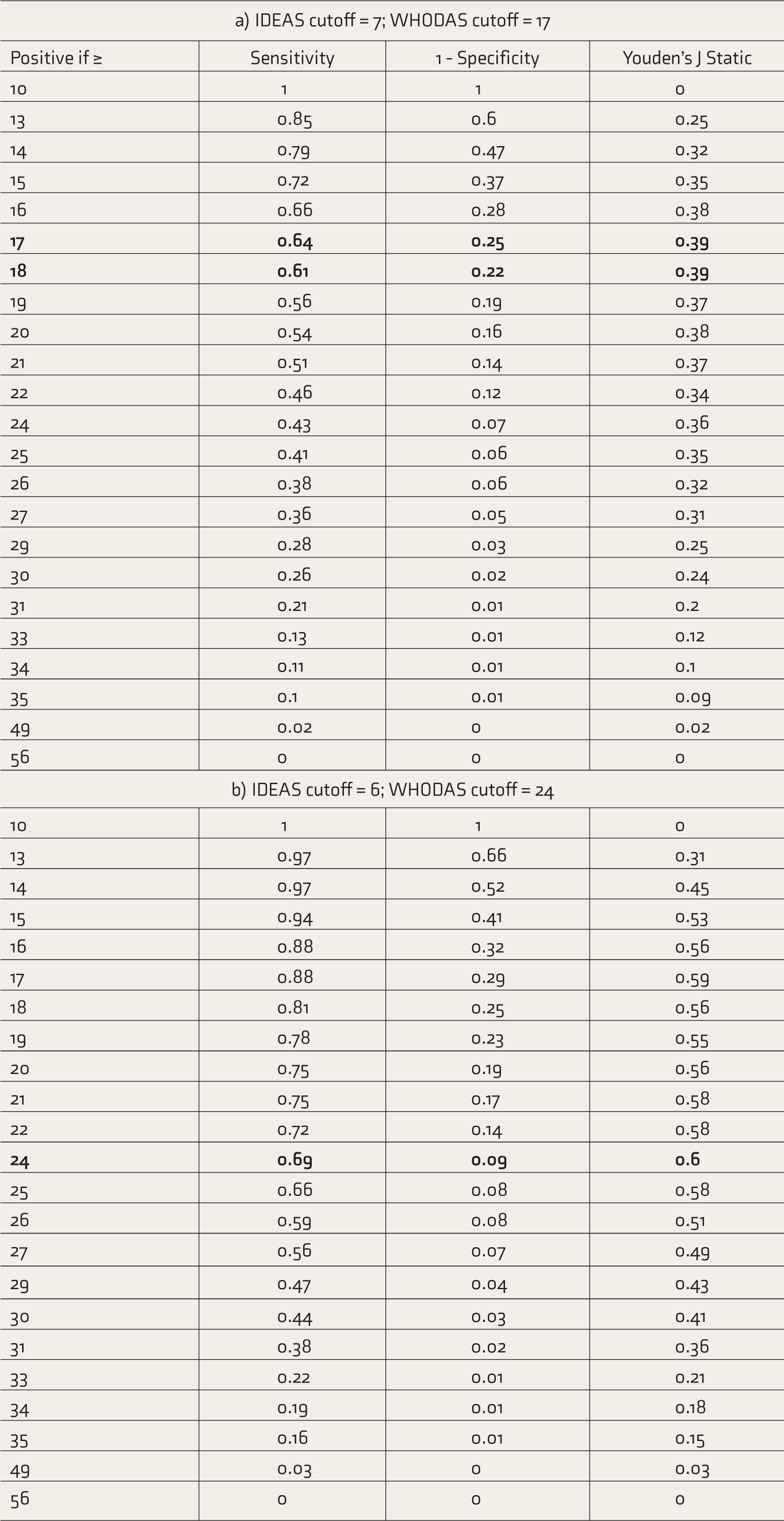
IDEAS: Indian Disability Evaluation and Assessment Scale, WHODAS: World Health Organization Disability Assessment Schedule. The bold values are the values that are significant (J nearest to 1).
The N was 172 (as opposed to the total N of 184 of the study) as data was missing in the 12 entries. We handled the missing data by case/record deletion, one of the most commonly employed methods to handle missing data in ROC studies. 18
Table 4 a shows the classification functions of the current measurement of IDEAS. Sixty-one persons had disability and 111 did not have disability as per IDEAS. Twenty-eight persons (16%) would be certified as having disability as per WHODAS, though they would not have disability as per IDEAS (false positives; cell B). Twenty-one patients (12%) would not be certified as having disability as per WHODAS but had disability as per IDEAS (false negatives; cell C).
The classification function is shown in Table 4b, with 6 as the cutoff for IDEAS and 24 as the cutoff for WHODAS. Thirty-two persons had disability and 140 persons did not have disability as per IDEAS. Twelve (7%) would be false positives (cell F), and 9 (5%) would be false negatives (cell G). Twenty-nine patients (17%) who were certified as having disability when the IDEAS cutoff was 7 would not be certified so if DOI is not considered.
Classification Functions.
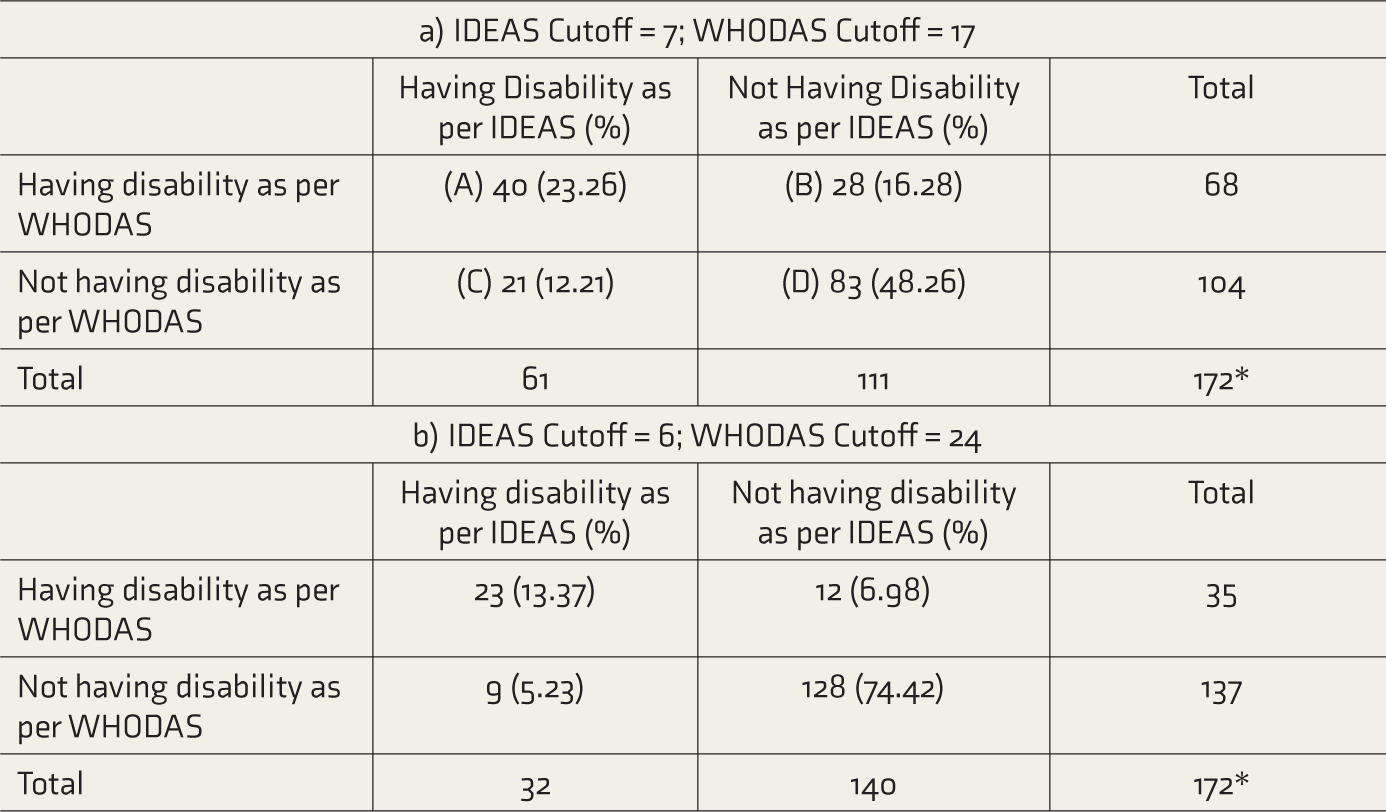
IDEAS: Indian Disability Evaluation and Assessment Scale, WHODAS: World Health Organization Disability Assessment Schedule. *N is less than 184 as data was missing in 12 subjects.
A shift from DOI-influenced IDEAS (Table 4a, A + C) to WHODAS (Table 4b, E + F) reduced the number of persons classified as disabled from 61 to 35 (a reduction of 15%). This shift will better identify patients whose disability status is influenced by the degree of actual disability rather than by DOI. Twenty-eight (16%) patients will be labeled as “not disabled” as per IDEAS, even when their disability was above the cutoff as per WHODAS (cell B). With the use of WHODAS, these also would get certified. This shift would deny benefits to patients whose disability status is influenced more by DOI rather than by the degree of disability. Twenty-one (12%) patients will be labeled as “disabled” as per IDEAS, even when their disability was below the cutoff as per WHODAS (cell C). With WHODAS, these would lose their disability status, as this shift would remove the undue influence of DOI on certification.
Discussion
This study of a community-based sample of persons with schizophrenia and other psychotic disorders, and BPAD, with minimal illness and mild disability in both IDEAS and WHODAS, showed the cutoff of WHODAS for benchmark disability as 17. With the influence of DOI removed, the cutoff was 24. When the influence of DOI is removed, a reduction of 15% in the number of persons classified as having disability will ensue. A shift to WHODAS would benefit an almost equal number (16%) to be classified as having disability.
Mental illnesses cause a significant burden of disability. In the current study, 35% of the study sample was found to have a disability, that too mild. The previous hospital-based study found that about 54% had disability, comparable to the National Mental Health Survey (NMHS), 2016. 19 The NMHS had revealed significantly higher disability in persons with severe mental illness—about 60%. In contrast, the Census of India conducted in 2011 had shown that a meager 0.03% of the population had a disability due to mental illness (0.08% if mental retardation is also included). 20 The huge discrepancy may be due to the method of collection of data in the census. The low level of disability in our sample may be due to the low severity of illness and the availability of accessible and affordable treatment.7, 21, 22 Our sample was not restricted to clinically stable patients. We have been providing treatment and rehabilitation inputs in the study universe since 2014. The low severity of illness may be due to these efforts from the team as well as the District Mental Health Program, which has a dedicated psychiatrist providing treatment at the district and taluk levels. The difference in the disabilities in NMHS vs our study may also be due to the different tools used (modified Sheehan’s Scale vs IDEAS/WHODAS).
Our earlier study had shown that the cutoff for WHODAS in the hospital-based sample, including DOI, was 23. The current study shows it as 17. This difference may be due to the fact that the hospitalized persons would have more disability compared to community-based persons. However, the cutoff remains the same when DOI is excluded, that is, 24 in both hospital- and community-based samples. This further shows that one of the main differences between IDEAS and WHODAS is DOI, which is somewhat responsible for skewing the disability scores. In the previous study, the shift from IDEAS to WHODAS resulted in a 10% reduction in the number of persons with disability and 6% would qualify as having disability as per WHODAS. The current study showed 15% and 16%, respectively, in the same parameters.
The classification and measurement of disabilities have undergone many modifications as the concept of disability has evolved from charity to medical to rights-based models. DSM-5 has embraced WHODAS 2.0. International Classification of Diseases (ICD-11) and ICF complement each other, and a unified platform provides holistic information about illness and its impact on a person’s functioning. 23 These point to a gradual and steady shift towards uniformity across diagnostic manuals, favoring WHODAS as a measure to assess disability. The other measures of disability are Activities of Daily Living-based surveys; Global Assessment of Functioning; International Classification of Impairment, Disabilities and Handicap, WHODAS, ICF, WHODAS 2.0, etc.
Currently, as per the authors’ knowledge, no country uses solely WHODAS to quantify disability. A few countries use either ICF or WHODAS partially. Taiwan uses ICF24–26 along with the Functioning Scale of Disability Evaluation System (FUNDES). Oman uses disability measures based on ICF, and other Arab countries are on a path to changing their guidelines related to disability. 27 The WHODAS has been used in more than 47 languages in 94 countries, mainly in research. 28
Needless to say, being a signatory to use ICF, India also may include WHODAS to measure disabilities across the illnesses causing disability, as opposed to measuring impairment alone as done currently (except for mental illness, which measures disability rather than impairment). Using WHODAS for quantifying disabilities has many advantages: An international comparison of disability data can be used on multiple disabilities simultaneously, and it is not related to illness/impairments alone. There are also a few disadvantages of using WHODAS: It does not consider the entire duration of disability and considers only the past month. The participation restriction extends to far more time than the past month. Since the disability certificate is at times given as a permanent disability, using WHODAS, which measures disability only for the past month, may be erroneous. Neither IDEAS nor WHODAS measures the impact of treatment. The disability, in the long run, may be different for treatment responders vs treatment-resistant persons.
This study and the previous studies by the authors provide a cutoff for the WHODAS for benchmark disability when this shift happens.
Strengths, Limitations, and Future Directions
This is the first community-based study comparing IDEAS and WHODAS to establish norms for WHODAS. The limitations are that the same rater usually applied both IDEAS and WHODAS, which may have led to observer bias. Blinded raters would be ideal. The study sample included persons with schizophrenia, other psychotic disorders, and BPAD only. A study including common mental illnesses would be beneficial, as all mental illnesses are eligible for disability assessment and benefits. The sensitivity and specificity are low for the cutoff 7 of IDEAS (sensitivity + specificity = 1.39). But the J static at this sensitivity and specificity is the highest among the other scores and hence the scores were considered for calculation and interpretation.
Although both IDEAS and WHODAS are simple yet comprehensive measures of quantifying disability, they both are riddled with their own issues, as elaborated earlier. Since WHODAS does not take DOI into account, a more comprehensive measure including WHODAS and duration of disability (instead of DOI), taking into account disability during all phases of illness (acute, recovery, remission, chronic illness, etc.), would be ideal.
Conclusion
A shift from IDEAS to WHODAS is feasible. Without the undue influence of DOI, both hospital- and community-based samples show a cutoff score of 24.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The researchers would like to thank the patients and their respective families, District Health Officer (Davangere), District Leprosy officer (Davangere), District Mental health program (Davangere), Taluk Health Officer (Jagaluru), all the heath staff in Jagaluru taluk, The Association for People with Disability (APD), Chittasanjeevani Charitable Trust, The Live Love Laugh Foundation, and Department of Psychiatry, National Institute of Mental Health and Neurosciences (NIMHANS) for their contribution in the effective implementation of the trial.
This work is supported by the Indian Council Medical Research (ICMR) under Capacity Building Projects for National Mental Health Program, ICMR-NMHP. We thank Dr Soumya Swaminathan (the then Secretary, Department of Health Research, DHR), Dr Balram Bhargav (the current Secretary D.H.R.), Professor V. L. Nimgaonkar, Professor Smita N. Deshpande, Dr Ravinder Singh, and Dr Harpreet Singh. We thank the faculty of “Cross-Fertilized Research Training for New Investigators in India and Egypt” (D43 TW009114, HMSC File No. Indo-Foreign/35/M/2012-NCD-1, funded by Fogarty International Centre, NIH). We are also thankful to the National Coordinating Unit of ICMR for NMHP Projects for their constant support and guidance. We thank the Data Management Unit of ICMR for designing the database. This manuscript’s content is solely the authors’ responsibility and does not necessarily represent the official views of NIH or ICMR. NIH and ICMR had no role in the study’s design and conduct; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Indian Council of Medical Research vide file number 5/4-4/151/M/2017/NCD-1.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.