
Abstract
Adolescents with substance use disorders often have co-morbid disruptive behaviour disorders, due to shared aetiology or bidirectional feedback. Such patients require a more nuanced assessment, as discussed in this editorial. Limited studies exist on the management of the comorbidity. Psychosocial interventions, especially those involving the family, are the most important.
Keywords
The National Survey on Extent and Pattern of Substance Use in India revealed substantial current prevalence of adolescent substance use (opioids: 1.8%, alcohol: 1.3%, inhalants: 1.17%, cannabis: 0.9%). 1 Besides, across India, most people seeking addiction treatment had initiated the use in adolescence. 2 Globally, adolescent substance use is highly comorbid with disruptive behavioural disorders [DBDs, i.e., attention deficit hyperactivity disorder (ADHD), conduct disorder (CD), and oppositional defiant disorder (ODD)] (Table 1). In a meta-analysis, ADHD and ODD/CD increased the odds of subsequent addiction (OR = 2.27 and 3.18). 19 Moreover, substance use is common even in those with subclinical behaviour problems. 20 Conversely, those with less severe substance use also have higher odds of ADHD symptoms and CD. 19 The comorbidity is also associated with lower SUD treatment completion rates.10,14
Comorbidity Rates of SUDs in Individual Disruptive Behaviour Disorders (DBD).
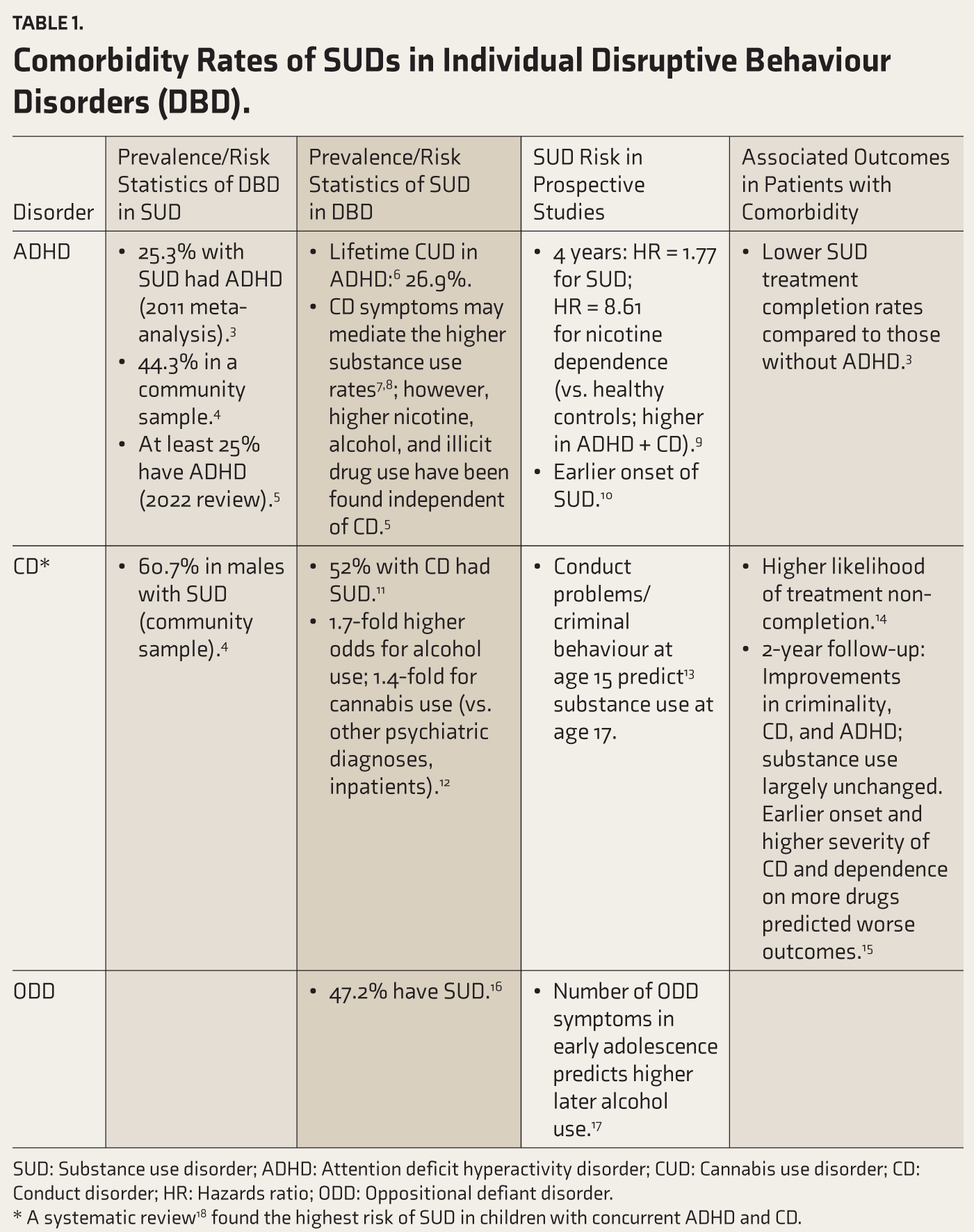
SUD: Substance use disorder; ADHD: Attention deficit hyperactivity disorder; CUD: Cannabis use disorder; CD: Conduct disorder; HR: Hazards ratio; ODD: Oppositional defiant disorder.
* A systematic review 18 found the highest risk of SUD in children with concurrent ADHD and CD.
Thus, understanding how these conditions interact is central to prevention, assessment, and management. This editorial synthesises current evidence while emphasising pragmatic assessment and management strategies relevant to low-resource and Indian clinical settings.
Discussion
Aetiology of the Comorbidity
Two major mechanisms have been proposed: 21
Shared Etiological Factors
A twin registry study found a shared genetic factor for childhood CD, alcohol/drug dependence, and adult antisocial behaviour. 22 A combination of smaller grey matter volume and lower white matter integrity is associated with an increase in both impulsivity and early substance use risk. Also, altered functional connectivity in the inhibitory control and reward processing networks elevates the risk of both impulsivity and substance use. 23 Family (e.g., poor parental supervision), peer (e.g., early involvement with deviant peer groups), and community risk factors may also contribute to comorbidity. 24
Bidirectional Feedback
Substance use can worsen the DBD (e.g., cannabis may exacerbate aggression and antisocial behaviour). 25 Conversely, those with DBDs can use substances due to the symptoms or as self-medication. For example, ADHD symptoms may encourage involvement with deviant peers 24 and risk- and drug-seeking behaviours. 5 While stimulants such as nicotine may temporarily ameliorate attentional deficits, alcohol and opiates may allay anxiety and excessive arousal. 26
Diagnostic Challenges
Diverse clinical problems and their consequences may be causing guilt, shame, stigma, and fear. Many patients have trauma histories with resultant trust issues. 21 Hence, assessment and diagnosis should be ongoing and evolve across multiple sessions. Clinicians should differentiate experimentation from problematic use (e.g., functional impairment) and identify the underlying risk factors (e.g., positive vs. negative reinforcement processes). 27 However, high dropout rates between screening and diagnostic assessments and possible unreliable history may jeopardise the process. 28
Attention Deficit Hyperactivity Disorder
Symptoms like inattention, impulsivity, and executive dysfunction may be common to both ADHD and SUD. 28 Hence, ADHD evaluation is best conducted after a period of abstinence (e.g., one month) or detoxification or stabilisation from SUD. 29 However, this may be difficult in outpatients, as ADHD symptoms may hamper involvement with SUD treatment. 28 Also, ongoing cannabis use confoundsthe assessment of ADHD medications’ effectiveness on hyperactivity and inattention. 30
Oppositional Defiant Disorder/ Conduct Disorder
Irritability and aggression, prevalent in intoxication and withdrawal states and indistinguishable from baseline oppositional features, may complicate both diagnostic and therapeutic-response assessments. 31 Illegal activities, such as stealing, may be aimed at procuring substances and not reflect a core CD symptom. 32
Rating Scales
Especially in busy, low-resource settings, nurses or counsellors may be trained to administer rating scales for a comprehensive assessment. 33 We 33 routinely use the Strengths and Difficulties Questionnaire, 34 Adverse Childhood Experiences-Questionnaire, 35 Teen Addiction Severity Index, 36 Adolescent Smoking Consequences Questionnaire, 37 and Parent/Teacher DBD Rating Scale. 38 Other tools for a multifaceted evaluation of substance use, mental health, strengths, and diverse life domains include Global Appraisal of Individual Needs Quick Version-4, 39 Problem Oriented Screening Instrument for Teenagers (POSIT), 40 and Comprehensive Adolescent Severity Inventory. 41
Evidence-based Treatment
A recent review
42
found only three randomised controlled trials (RCTs):
In adolescents with major depressive disorder, lifetime CD, and at least one non-tobacco SUD, fluoxetine + cognitive behaviour therapy (CBT) was not more effective on substance use or CD symptoms than placebo + CBT.
43
Osmotic-release methylphenidate + CBT was not more effective on ADHD or substance use than placebo + CBT.
44
Atomoxetine + motivational interviewing (MI)/CBT was not more effective than placebo + MI/CBT for ADHD or use of non-nicotine substances.
45
(Please remember that negative trials per se do not imply futility but may instead indicate the need for better-designed studies).
In secondary analysis of an RCT, in patients with a DBD and cannabis abuse/dependence receiving motivational enhancement therapy (MET), CBT, and abstinence contingency management, when family management training (FMT) or parent psychoeducation was additionally provided, the FMT group had fewer days of cannabis use; externalising behaviours did not change significantly. The FMT, 45 minutes long, included Parent Management Training (PMT) and the development and implementation of a substance-monitoring contract. 46
Nicotine patches and bupropion help ADHD symptoms, such as inattention. 47 However, in those with alcohol, cannabis, or opiate use disorder, ADHD medications have little impact on the SUD, despite improvement in ADHD symptoms. 30 Hence, a combination of both ADHD medications and SUD treatments is recommended for most patients with the comorbidity. 48 A systematic review found only four randomised trials of pharmacotherapy for co-morbid ADHD and SUD; none revealed a robust effect on either. No RCTs were found on the efficacy of psychosocial treatments in co-morbid ADHD and SUD. 18
Practical Guidance from Literature
A biopsychosocial–spiritual approach is essential. 21 Combined psychotherapeutic and pharmacological interventions are the most effective. 49 The spiritual component may emphasise wholeness, balance, and relationships with family, community, and the natural environment. 21 As the multitude of symptoms often leads to poor adjustment to or expulsion from school and association with peers having similar vulnerabilities, educational and crime-prevention services may need to be involved. 21
If the DBD diagnosis is uncertain, waiting for a period of sobriety before starting medication may provide a clearer picture. However, DBD medications may be introduced earlier in case of: (a) DBD symptoms clearly predating substance use; (b) past treatment failures and relapses; and (c) history of good medication response to DBD. 24
Attention Deficit Hyperactivity Disorder
As impulsivity may lead to early relapse, ADHD medication 30 and relapse-prevention strategies 50 may require quick initiation. Psychoeducation should emphasise the relative safety of ADHD medication even during ongoing substance use. 28 As ADHD patients may struggle in treatment settings due to their reduced ability to process new information (e.g., inattention or distractibility in a group setting), group leaders and participants should be sensitised to ADHD. 26 Likewise, role plays on specific skills that can be automatically applied, minimising cognitive load during real-life stressful situations, could be utilised. 28
Preventing Stimulant Misuse
A systematic review on misuse of prescribed stimulants among ADHD patients found no youth-specific studies; in studies that included both youth and adults, the prevalence ranged from 2% to 29%, with higher rates in those with a substance use history.
51
Recommendations for prevention include:
30
Close monitoring for signs of misuse, such as missing appointments or requesting higher doses or more prescriptions. Considering extended-release methyl-phenidate formulations, or non-stimulants such as atomoxetine or bupropion.
Conduct Disorder
The propensity for deviant social behaviour, which contributes heavily to overall dysfunction, should be addressed. Issues such as impulsivity, affective dysregulation, excessive anger, and poor social and problem-solving skills can be managed through behavioural interventions, including skills training and cognitive-behavioural methods. Promoting association with non-substance-using peers and adoption of prosocial activities and goals is essential, too. 24
Managing Individual Conditions
Given the limited evidence on management of the comorbidity, each disorder may be addressed with its most supported interventions:
Substance Use Disorder
Psychosocial interventions are the recommended primary modality; the most effective are family-based therapy, CBT, and multicomponent approaches that combine these interventions with MI and contingency management. Family-based therapies engage parents, caregivers, and siblings and are particularly effective in promoting therapeutic alliance and treatment attendance. 52
The only FDA-approved pharmacotherapy is buprenorphine for opioid use disorder (in those aged ≥16). 53 Digital therapies can complement other treatments to improve accountability and teach recovery-focused life skills. 54
‘Controlled use’ should never be an explicit treatment goal, though it can be an interim goal to help build skills to tackle substance use and improve self-efficacy. 55
Nicotine
Counselling received a strong recommendation, while varenicline and bupropion received conditional recommendations, both based on very low–certainty evidence. Nicotine replacement therapy has limited effectiveness. 56
Alcohol
Among psychosocial interventions, the highest effect sizes were noted for integrated MET-CBT in reducing the frequency, and for Common Elements Treatment Approaches in reducing the amount. 57
Cannabis
Contingent rewards, engaging the family, and brief motivational counselling that includes information on peer network 58 have shown promise. 59
Inhalants
Certain holistic, multifaceted residential programmes have the highest success rates. While small clinical trials support aripiprazole, case reports support baclofen, naltrexone, and lamotrigine. CBT-based brief interventions and family therapy have some supporting evidence. 60
Attention Deficit Hyperactivity Disorder
ADHD should be managed with an individualised multimodal approach incorporating psychoeducation, medication, and psychosocial interventions. In general, stimulants are recommended as first-line therapy and non-stimulants as second-line. 61 In a subgroup analysis within a meta-analysis, for parent-rated symptoms, meta-analyses did not find stimulants to be significantly superior to non-stimulants. However, for teacher ratings, stimulants had a higher effect size (SMD: 0.79 vs. 0.42). 62
A systematic review of recent trials revealed that the effects of cognitive/behavioural treatments (C/BTs) and medication were complementary rather than duplicative. It advised combining medication and C/BT in the beginning itself, to enhance adherence and response breadth (i.e., improve both ADHD symptoms/cognitive performance and coping skills/functional impairments). 63
Stimulants are the first-line treatment for aggression in ADHD. However, many patients would require additional interventions. Clonidine may provide some benefit for conduct-related behaviours in ADHD patients. 64
Conduct Disorder/Oppositional Defiant Disorder
Atypical antipsychotics are relevant in DBDs because most vulnerability alleles are related to dopaminergic and serotonergic systems. 65 Of all antipsychotics, risperidone seems effective in the short-term management. However, antipsychotics are associated with weight gain in this population. 66
Psychosocial interventions are considered the most effective, particularly when they have multiple components and involve both the patient and parents. 67 However, even in high-income countries, up to 70% of children and adolescents do not receive these interventions when needed. 68 Moreover, several familial and social risk factors of DBDs (e.g., economic backwardness, parental unemployment or substance use) can themselves hinder engagement in psychosocial interventions. 69
Aggression
Risperidone and divalproex have the most evidence, with promising but less robust data available for other atypical antipsychotics such as aripiprazole. Lithium and haloperidol have shown efficacy, primarily in inpatients. 64
Trauma
CBTs with a trauma focus are the first-line treatment. 70 Inpatients, in particular, should receive trauma-informed care that emphasises safety, minimises re-traumatisation, helps rebuild a sense of empowerment, and highlights strengths and resilience. 71
Prevention
Universal Prevention
Indian adolescents have poor knowledge of substance-related harms, 72 and friends and close acquaintances are the commonest introducers to substances. 73 Drug awareness alone is ineffective; training in social skills, problem solving, and anger management may help prevent SUDs and later DBDs. 24 Relationship skills should be part of the school curriculum. 32 As the usual age of starting tobacco use is about 12 years, interventions must be directed at younger age groups. 74 Using local images, incorporating cultural values, etc., can help culturally adapt the prevention efforts. 75
Educating teachers not only about substance use but also about issues such as conduct problems may be useful. 74 Supply reduction (e.g., a ban on the sale of legal substances to minors) should also be employed. 32
A review identified Functional Family Therapy, Positive Family Support, and Lifeskills Training as the programmes with the highest benefit-cost ratios in preventing adolescent substance use. 76
Selective Prevention
In high-risk adolescents, a programme with psychoeducational, MET, and CBT components reduced the substance use rates and related harms by about 50% and the likelihood of transitioning to psychological problems, including conduct problems, by 25%; effects lasted 2–3 years. 77 A group cognitive-behavioural intervention targeting impulsivity and sensation seeking reduced the growth in SUD rate for five years. 78
Unhealthy relationships augment the genetic influences on substance use. For example, lower parental monitoring increases the likelihood that genetic predispositions manifest. 79 Likewise, in adolescents with more peers who use alcohol, genetic predispositions had a greater expression. 80 These findings can inform tailored prevention for those with a family history. 81
School counsellors should reach out to those with family risk factors, substance-using peers, or a history of stressful events. As most treatment-seeking Indian adolescents are school dropouts, 74 and substance use and externalising problems are risk factors for school dropout, 82 vocational training centres and safe spaces should be made available to them. 74 Counselling services and interventions, such as life-skills-based education, should be provided in such places. 74
Indicated Prevention
Treatment of DBDs in childhood, including PMT, is crucial. 24 Family interventions should emphasise the importance of parental monitoring (i.e., knowing the child’s peers and whereabouts after school). 83 For those with DBDs, SUD prevention interventions should be of sufficient duration and intensity to promote durable change. Including booster or follow-up sessions may increase the likelihood of sustained change, foster resilience to SUD, and improve later DBD outcomes. 24 In children with ADHD, stimulants may prevent SUD in adolescence. 18 Besides, ADHD interventions may make substance problems more treatment-responsive. 27
Mentorship programmes, effective in selective and indicated prevention of substance use and externalising problems independently, 84 need evaluation in co-morbid populations.
Indian Scenario
Research on comorbidity in India is sparse. Among 49 patients of addictive disorders at our centre (including 11 with gaming disorder), conduct-dissocial disorder, ADHD, and ODD were present in 22, 14, and 11, respectively. 33
Specialised substance treatment services for children or adolescents are restricted to a few centres. Many lack infrastructure and staff and function suboptimally. 74 Though the National Action Plan for Drug Demand Reduction funds one centre for adolescent boys in each state, 85 currently, only Delhi and Manipur run them. Even where services are available, treatment-seeking is poor, probably due to lack of motivation, stigma, or deficient understanding about the nature of SUDs. 74
The Mental Healthcare Act (MHCA) 2017 mandates that minors be admitted only with the nominated representative (NR) or an attendant appointed by the NR. 86 This poses practical challenges, especially when a short-term rehabilitation is required to manage both SUDs and DBDs. Besides, adolescents with addictive disorders often come from broken families87,88 (57.6% in our study of 59 patients, of whom 79.7% had a DBD), 89 limiting bystander availability.
We developed a care model that low-resource settings can adopt for assessment and management of SUDs and DBDs. It included training social work postgraduates and nurses in the use of assessment tools and workbooks. The model was found to be feasible and acceptable to patients. 33
Conclusions
This critical area remains under-researched. Cultural validation of assessment tools and efficacy studies of interventions are urgently needed. Amendments to MHCA, with provision to admit at least patients from broken families or the street without a bystander, would ease rehabilitation efforts. Timely diagnosis and deployment of culturally appropriate, cost-effective, and empirically validated therapeutic and preventive interventions, alongside ongoing research and policy measures, can keep many dreams from ever needing a requiem.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
During the preparation of this manuscript, the author used Grok 4.1, ChatGPT 5.2, and Perplexity Pro to assist with literature search and to improve the language and structure. ChatGPT 5.2 was also used to format the references, which the author subsequently reviewed and verified. No part of this article was written by a generative AI tool. The author takes full responsibility for the content of the published article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.