
Abstract

Yoga and meditation are promising therapeutic interventions for physical and psychological conditions.1–3 The COVID-19 pandemic has greatly affected the mental health of both the general population and those with a history of mental illness. Amidst the pandemic, various agencies have recommended using meditational practices to cope with psychological problems and promote a healthy lifestyle; simultaneously, the literature has also cautioned against the untoward effects of the meditation if not practiced properly.4, 5 Meditation has been broadly categorized into (a) Focused attention (FA, concentrative type, where the practitioner voluntarily focuses one’s attention within [breath, thoughts, etc.] or outside [candlewick, etc.] to the exclusion of all other experiences); (b) Open monitoring (OM, where the attention is not directed toward a particular thing; rather, the practitioner attends in a nonjudgmental and nonreactive manner to whatever arises in one’s mental continuum); (c) Automatic self-transcendence (AST, transcending the practice of meditation and harnessing the natural tendency of the body to attain pure consciousness); and (d) Guided meditation (GM, where the content of meditation takes precedence over its other aspects, and the practitioners are guided through a set of images or chants to engage in a particular aspect of self [empathy, kindness, etc.] mindfully). 6
Despite the proven benefits of meditative practices for several psychological conditions, they (unsupervised and unregulated practices in particular) have been linked with unwanted effects or adverse effects (A/E) in the psychological (psychosis, dissociation, depersonalizations, etc.), physical (pain, epilepsy, etc.), and spiritual (conflicts between one’s religious beliefs or philosophy and one’s principles of meditation programs) domains.7, 8 Different meditation practices (or schools of practices) do provide a guideline about the right technique of practice (Patanjali Yoga Sutras mention that these practices must be done slowly and in a step-wise manner [Tasya Bhumishu Viniyogah] 9 ; similarly, chapter-VI of Gita mentions about the moderation in food and sleep [Atma-Samyama Yoga]), 10 flouting of which could result in A/Es.
The A/Es related to meditation are determined by various meditation-related (e.g., type, depth, duration of meditation, practice beyond prescribed format, etc.), practitioner-related (past or family history of psychiatric illness, psychological vulnerability, personality traits, etc.), and environment-related (sensory deprivation, fasting, practice in isolation, etc.) factors.3, 7, 8, 11 Despite this potential A/E, including severe ones like psychosis, the literature is scarce in this area and limited to a few case reports or reviews.7, 11–13 Even less literature is available about the important aspects of practice-related guidelines/recommendations to prevent A/E, including psychosis. Therefore, this paper aims to highlight issues pertaining to meditation-induced psychosis through a series of clinical cases; it also intends to provide recommendations on the prevention and early detection of psychosis associated with meditation.
Case Series
We present five cases (Table 1) of meditation-related psychosis (Schizophrenia/nonaffective psychosis or affective psychosis) belonging to different places (three different places from India and one from Nepal) and clinical settings (three were managed in outpatient and two in inpatient settings), and we discuss some of the critical aspects of it. The report has been prepared as per the case-report guideline (CARE-checklist; supplementary file). 14
Details of the Included Patients

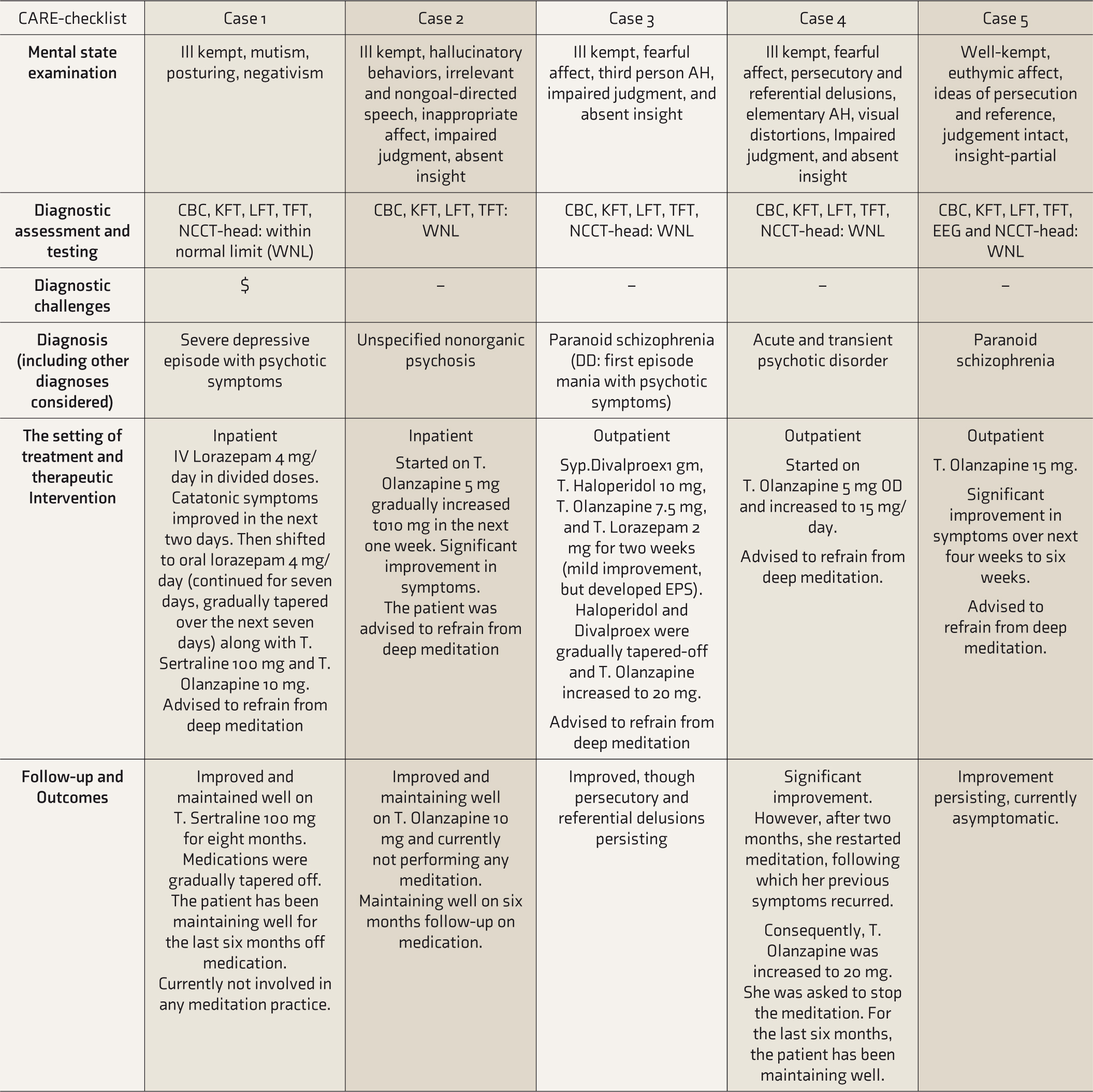
Note. #catatonic symptoms involve mutism, posturing, stupor, and negativism; $In the spiritual sect, some followers would label it as a part of a deep meditation experience while others would label it abnormal. Since there was severe socio- occupational-physical dysfunction, it was labelled as a disorder; AH: auditory hallucinations, ADR: adverse drug reaction, CBC: complete blood count, DD: differential diagnosis; KFT: kidney function test, LFT: liver function test, TFT: thyroid function test, NCCT: noncontrast computer tomography; EPS: extra-pyramidal symptoms, F/h+: positive family history, HIE: hypoxic-ischemic encephalopathy, PMT: premorbid temperament.
Risk Factors for Meditation-induced Psychosis#

Note. # developed by the authors based on the available literature on meditation and psychosis and not merely on the current case-series.
Discussion
This report highlights that inadequate participant screening and supervision, and unregulated meditation practice (depth and duration of practice), particularly in the novice, can precipitate/worsen psychosis, especially in the vulnerable population (Table 2). Some of the pertinent points have been discussed further and recommendations have been made based on the available literature on this area (Box 1).
Possible Measures to Prevent Meditation-Induced Psychosis#
Note: # developed by authors based on the review of literature.
Issues Related to Participants Selection
Two of the five cases had a positive family history of severe mental illness (e.g., schizophrenia). However, such useful information was not documented by the yoga instructor before inducting the participants into the meditation program. Those with a family history or history of psychiatric disorders are at higher risk of meditation-induced psychosis.7, 15 Hence, it would be prudent to take a brief psychiatric history of the potential enrollees before inducting them into the program. For them, the meditation program should be tailored accordingly; getting a psychiatric opinion would also be a welcome step.
Type of the Meditation Practices
All the cases were involved in either the FA or AST (e.g., transcendental meditations) type of meditation. FA meditation has been linked with a higher prevalence of psychosis than OM or GM. 7 The former is associated with greater structural changes and functional dysregulation at the prefrontal cortex and limbic system—the areas also implicated in schizophrenia.16, 17 It has been recommended that those with psychiatric vulnerabilities should preferably be enrolled in OM or guided forms of meditation. 15
Duration of the Meditation Sessions
Before the onset of illness, four patients were involved in deep meditation, that too for prolonged duration (retreat courses) and during odds hours (late night and early morning). One patient was involved in Buddhist enchantment meditation practices for a prolonged duration. These findings are similar to another report from Japan where the participant had psychotic experiences following a prolonged practice of Buddhist enchantment meditation. 18 The literature also suggests that unsupervised deep meditation for a prolonged period, coupled with sensory deprivation, is associated with the onset of psychosis.7, 19 Therefore, it’s mandatory that the practitioners, especially the novice practitioners, should be encouraged to meditate for a brief period and maintain hydration, and should be supervised periodically.
The Setting of Meditation
All the patients were involved in deep meditation without being in touch with their instructor (unsupervised meditation). Moreover, they did not contact their trainer despite having abnormal psychic experiences. The literature suggests that as high as 50% of the meditation practitioners experienced some form of AEs following meditation. 7 However, these effects were brief and improved with changes in their meditation practices on the advice of their trainer or with treatment. Hence, it is recommended that the instructors must regularly seek feedback from their trainees and encourage them to periodically participate in group sessions. This would facilitate the early identification of any emergent psychopathologies.
Other Risk Factors for Meditation-induced Psychosis
Retreat courses or prolonged duration of intense meditation are often coupled with practices of sensory deprivation, prolonged fasting, sleep deprivation, social withdrawal, and intense efforts to achieve inner consciousness; these can act as the contributory factors for meditation-induced psychosis.7, 15 Hence, such intense practices should be discouraged, especially for the novice. Notably, in one of our patients, the meditation was undertaken to improve one’s attention and concentration for better academic performance, while the principle of the concerned meditation program was to attain a deeper state of consciousness. This mismatch in the expectation (of the participants) and purported goals of a given meditation and the inadequate assessment and education of the participants, including assessment of their level of preparedness for a given meditative practice, might have contributed to the onset of the psychosis.
Causality in Meditation- Induced Psychosis
None of the cases had a history of any psychiatric illness. Three out of five patients were involved in prolonged duration of meditation practice, ranging from one to five years, but their meditation practices got acutely increased just a few weeks before the onset of illness. Another two cases developed psychotic symptoms within ten days of starting meditation practices. Although an unequivocal temporality between the two, particularly among those cases with a history of meditation practice for a significant period, could not be firmly established, a marked change in their pattern of meditation was observed. This points toward an association between a sudden increase in the duration of meditation practice, including inducting in deep meditation practice, and the onset of psychosis—a finding that has also been reported in the literature.7, 13, 19 One should explore the shared biological vulnerabilities (e.g., neurobiological research), genetic studies (involving meditation practicing/nonpracticing family members), and if meditation has been a form of coping for managing psychotic experiences, to better understand the relationship between the two conditions.
Course and Prognosis of Meditation-Induced Psychosis
Almost all of our patients showed improvement in their symptoms over one to four weeks of treatment and cessation of meditation—an observation that is in concordance with previous literature. Notably, we found a relapse of psychotic symptoms in one case following the reinstatement of the meditation practices. This is a practical challenge in the clinical practice as, often, such patients seek advice on restarting meditation after attaining remission or insist on restarting some form of meditation as a way of maintaining a healthy lifestyle. Meditation is to be discouraged in individuals with a history of meditation-induced psychosis,7, 15 however, if one still wants to continue it, it should be guided or OM type (vs. FA or transcendental), that too for a brief period, preferably in a group setting and under supervision. The treatment should be continued, especially if there are biological or psychological risk factors present.
The current case series has certain noteworthy limitations. First, the temporality between meditation with psychosis cannot be proven without doubt. Second, corroborative information from the meditation trainer/expert was not available; hence, the information presented is solely based on the patients’ and caregivers’ versions. Third, the role of the contributory factors (starvation, dehydration, and abnormal experiences related to them) was not to be assessed. Lastly, only the short- to medium-term course of the illness is available; the long-term impact of the medications and the cessation of the meditation is yet to be assessed.
Conclusion
Various bio-psycho-social and meditation-related factors determine the development of meditation-induced psychosis. The temporality between the two conditions, however, is often difficult to establish. Meditation-induced psychosis often responds well to treatment and cessation of the implicated meditation practice. There is a need for a structured protocol for screening the participants before they are inducted into the meditation, particularly because meditation has been increasingly promoted for psychological well-being following the COVID-19 pandemic, and for monitoring participants subsequent meditation practices. Yoga professionals could liaise with mental health professionals to prevent the emergence of such A/E; moreover, this would also ensure early identification of and prompt intervention for such cases. Also, more longitudinal and neurobiological research is required to explore this phenomenon. Further, future research must endeavor to develop a culture- and meditation-specific questionnaire to screen the at-risk population for the possibility of developing meditation-induced psychosis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
A written informed consent for patient information to be published was provided by the patient(s) or a legally authorized representative.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.