
Abstract
Background:
The phenomenon of metacognition is instrumental in the conceptualization and management of obsessive compulsive disorder (OCD). Studies on the comparison between metacognitions in OCD patients and healthy controls or those with other clinical conditions have been conducted. We aimed to compare metacognitions among currently symptomatic OCD (S-OCD) patients, currently remitted OCD patients (R-OCD), and healthy controls (HC).
Method:
This cross-sectional research was conducted in the Department of Psychiatry of a tertiary care hospital in North India. Purposive sampling method was used to recruit 40 OCD patients, including an equal number of R-OCD and S-OCD patients, and 20 HC matched for age and education. Meta-Cognition Questionnaire and Thought Control Questionnaire were used to assess metacognitive functions.
Results:
The findings showed a gradient of highest maladaptive metacognitions in the S-OCD group and lowest in HC. In the OCD subgroups, specific metacognitive beliefs (negative beliefs F = 65.52; need to control thoughts F = 61.03) and strategies (worry F = 83.55; low distraction F = 105.61) remained significantly different (P ≤ 0.001) between S-OCD and R-OCD patients. Certain other metacognitions remained consistently more or less stable between S-OCD and R-OCD patients, that is, metacognitive beliefs (cognitive confidence F = 11.43; cognitive self-consciousness F = 37.12) and strategies (punishment F = 17.45; low social control F = 12.89). This finding is further corroborated by positive correlations of severity of OCD with need to control thoughts (r = 0.66, P < 0.001), negative beliefs (r = 0.63, P < 0.001), and worry (r = 0.76, P < 0.001), and negative correlations with distraction (r = – 0.79, P < 0.001).
Conclusion:
The study provides preliminary evidence for specific metacognitions distinguished as potential state and trait markers for OCD, which needs to be established on a larger sample using a longitudinal study design.
Keywords
Symptomatic OCD patients have higher maladaptive metacognitions compared to remitted OCD patients. There is preliminary evidence for specific metacognitions to be distinguished as potential state and trait markers. Identification of metacognitive markers for OCD is useful in planning subsequent therapeutic intervention.Key Messages:
Obsessive compulsive disorder (OCD) has a heterogeneous presentation of obsessive thoughts and compulsive acts. It is known to have a complex biopsychosocial etiology.1,2 The worldwide lifetime prevalence of OCD is around 2.3%, 3 and in India, prevalence studies found estimates varying between 1% and 3%.4, 5 This disorder causes substantial impairment for both the patient and family members.6,7
Recently, the construct of metacognition has gained interest in the conceptualization and management of OCD. Commonly described as “thinking about thinking,” metacognition refers to the knowledge (beliefs), cognitive processes, and strategies used to appraise, monitor, and control thoughts. Wells proposed8–10 the metacognitive theory for OCD, based on the self-regulatory executive function (S-REF) model. 11 This model suggests that beliefs about thinking comprise three metacognitive components: (a) beliefs about the significance of thoughts, (b) interpretation and experiential perspectives on those thoughts, and (c) beliefs about the need to control thoughts and cope with them. 12
The S-REF theory postulates that the processes of metacognition become maladaptive in psychological disorders. These maladaptive metacognitions result in “cognitive-attentional syndrome (CAS).” CAS is a crucial etiopathological and maintaining style of thinking for OCD.
The identification of cognitive markers of OCD has a significant preventive and therapeutic implication. A trait marker has a causal and predisposing role in a disorder and remains more or less stable across different phases of illness. In contrast, a state marker reflects dynamic changes in cognition in various stages of the disease. For instance, the neurocognitive deficits in OCD are shown to be stable trait markers as they remain relatively unchanged in different phases of OCD.13–17
Comparative studies on metacognition in OCD have been conducted with a healthy control group and other clinical conditions. These studies show that beliefs about the uncontrollability of thoughts, excessive focus on the awareness of thinking, low cognitive confidence, positive beliefs about worry, and negative beliefs about worry are elevated specifically in OCD.18–24 Also, OCD patients use punishment, worry, reappraisal, and social control more often as thought control strategies.25,26 The findings of these studies show the presence of diagnostic specificity of the metacognitive processes and strategies used in OCD vis-à-vis other anxiety conditions. Hence, there is an indication that they are state or trait markers of OCD.
Most studies showing maladaptive metacognitions in OCD have been conducted on symptomatic patients. It is not clear if maladaptive metacognitions are state dependent or state independent and if they persist in the remitted phase of OCD. In other words, just as neurocognitive deficits, are they stable and remain unchanged in the remitted phase of OCD and hence are suggestive of “traits markers,” or are they reversible and merely a reflection of a phase or severity of OCD as “state markers?” If metacognitive variables are “trait” characteristics, then the course of illness, that is, the remission phase, should not affect them significantly. The present study aimed to compare metacognitions (“metacognitive beliefs” and “thought control strategies”) among OCD patients who were symptomatic, OCD patients who were remitted, and healthy control subjects.
It was hypothesized that OCD patients (symptomatic and remitted) would have more maladaptive metacognitions than healthy controls. Furthermore, it was also hypothesized that there would be a significant difference among all metacognitions between symptomatic and remitted OCD patients.
Materials and Methods
Study Design and Subjects
The present cross-sectional study was carried out in a tertiary care hospital in North India. It was conducted between December 2015 and May 2016. The total sample comprised of 60 subjects, with 20 participants in each of the 3 arms, namely: Group 1—OCD patients currently symptomatic (S-OCD), Group 2—OCD patients currently remitted (R-OCD), and Group 3—healthy controls (HC). A priori it was planned to have at least 20 subjects in each arm based on a previous study by Bannon et al. 13 conducted on 20 S-OCD, 20 R-OCD, and 20 panic disorder subjects that confirmed the presence of specific executive function deficits in OCD, and indicated deficits to be trait-like in nature. The subjects were group matched for age and years of education; after recruitment of the patients, the group-matched controls were recruited in the study.
OCD patients were recruited from the outpatient services of the Department of Psychiatry by using the purposive sampling method. The inclusion criteria for patients were: age 180–50 years, a diagnosis of OCD as per DSM-5, receiving standard anti-obsessive pharmacotherapy under a consulting psychiatrist, with minimum education up to tenth standard, and having the ability to read and write in the Hindi language. Patients with neurological illnesses (seizures, traumatic brain injury, stroke, or tumor) or intellectual disability, as indicated by history and clinical impression, were excluded. Those with comorbid psychiatric disorders, undergoing any other therapy for OCD and having any medical condition requiring urgent intervention, were also excluded. Patients who met the remission criteria as defined by “International Expert Consensus” 27 as having a Yale-Brown Obsessive-Compulsive Scale (YBOCS) score of ≤ 12 for at least the last week were placed in the R-OCD group. HC who scored ≤ 3 on the General Health Questionnaire-12 (GHQ-12) 28 were purposively selected from community areas accessible to the investigator.
Measures
Procedure
Ethical clearance was obtained from the institutional ethics committee. The diagnosis of OCD was established as per DSM-5 by the treating consultant psychiatrist. GHQ-12 was used for recruiting HC. After seeking written informed consent, sociodemographic pro forma was completed for all subjects to collect information related to age, gender, education, history, family history, personal history, and medical history. The assessment was carried out at a mutually convenient time in the Department of Psychiatry. Patients were advised not to take benzodiazepine medication 12 h before assessment. MCQ-30 and TCQ were applied to all subjects. Besides, other assessment instruments, MINI, and Y-BOCS were used for the patients.
Data Analysis
Analysis was done using descriptive statistics and making comparisons among various groups. For the analysis of sociodemographic characteristics, discrete (categorical) data were summarized as proportions and percentages (%). Chi-square test was applied for the comparision of categorical variables. The quantitative data were represented as mean±SD, on which t-test was used. The normality was tested by the Shapiro–Wilk test, which is used for small samples. The results showed that for each parameter, at least one group had normality of data; therefore, parametric tests were applied as they are more potent.
Analysis of variance (ANOVA) and Tukey’s post hoc test were used for comparison of MCQ-30 and TCQ domains across the three groups. ANCOVA was used in the clinical groups to eliminate the effect of illness duration, by treating it as a covariate. Also, a partial correlation method was used to find an adjusted correlation between the scores on severity of OCD and metacognitions, after eliminating the effect of duration of OCD. The P value of <0.01 and <0.001 were taken as the significance level. The analysis was done by using IBM-SPSS (v21) and MS Excel.
Results
For this study, 61 OCD patients were screened. The most common reason for exclusion among OCD patients was a comorbid psychiatric illness (8) (depression [4], agoraphobia [2], and social anxiety disorder [2]). Other reasons for exclusion were age > 50 years (2), below the desired educational level (3), and undergoing other therapies (5). In total, 43 OCD subjects were taken for assessment, and 3 did not complete the assessment. In the control group, 25 subjects were screened, out of which 20 subjects were included. Three subjects were below the desired education level, and two subjects refused to give consent. Hence, 20 in each group were taken up for analysis.
Sociodemographic and Clinical Characteristics
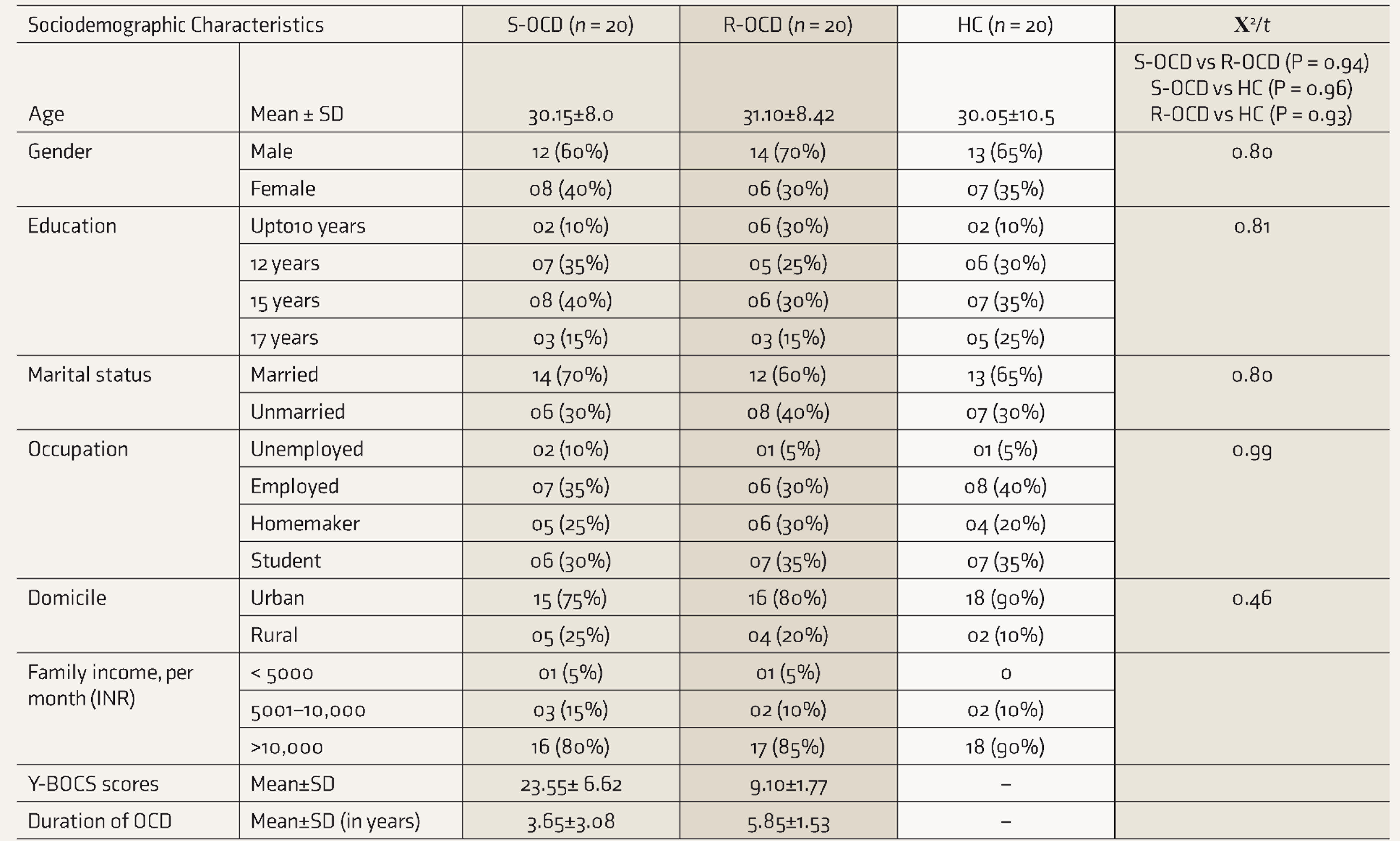
Sociodemographic characteristics were comparable across S-OCD, R-OCD, and HC (Table 1). Among clinical features, as expected, the R-OCD had significantly lower severity of OCD, with the mean±SD Y-BOCS score being 23.55±6.62 in S-OCD and 9.10±1.77 in R-OCD. R-OCD had a longer duration of illness than the S-OCD group, with the mean duration being 3.65±3.08 years in S-OCD and 5.85±1.53 years in R-OCD.
Sociodemographic Characteristics of Clinical Groups and Healthy Control Group
Differences Among the Study Groups
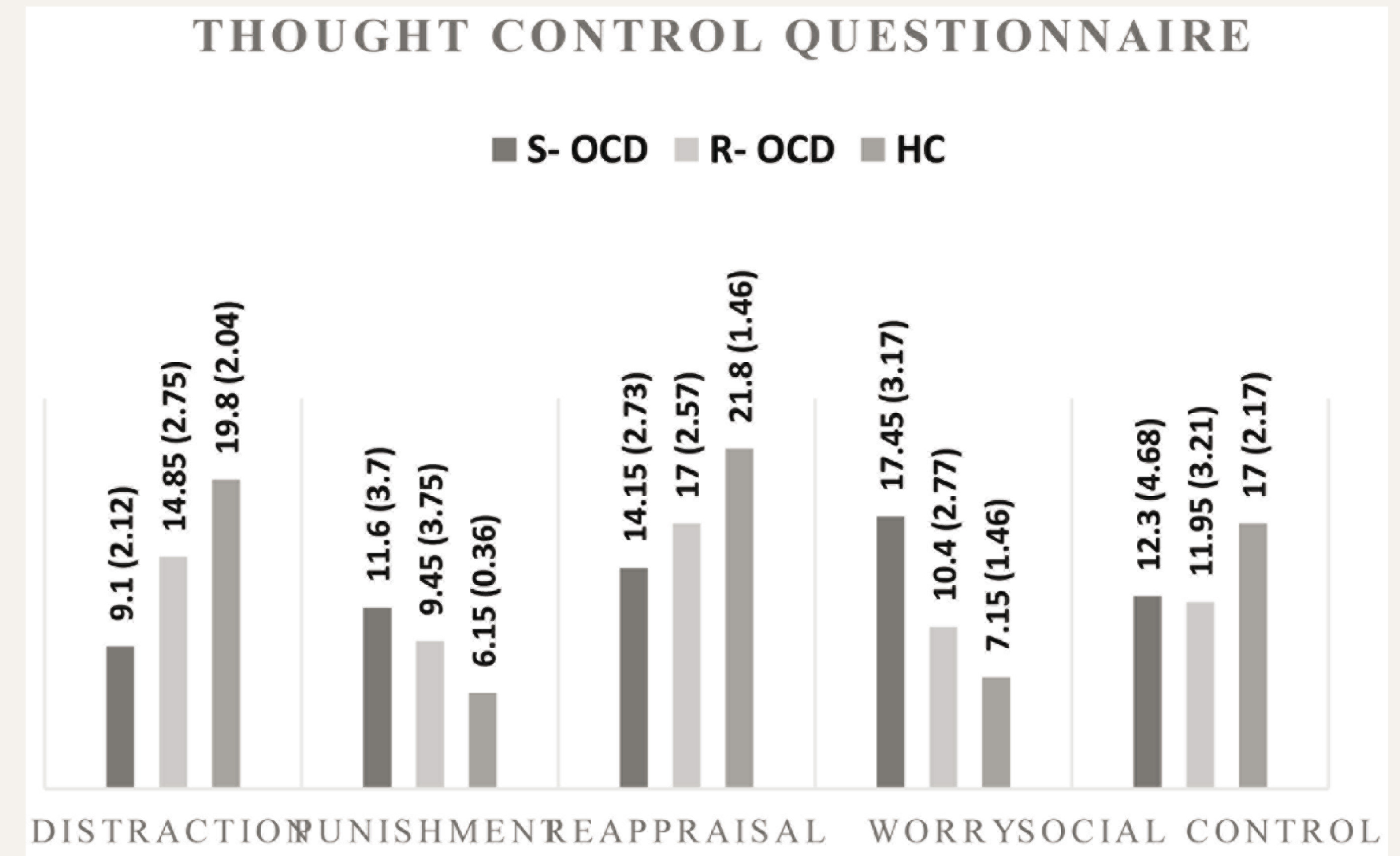
The differences among the three study groups on all domains of metacognitions (MCQ-30 and TCQ) are depicted by findings of ANOVA and post hoc analysis (Table 2, Figures 1 and 2). On MCQ-30, compared to HC, generally, both OCD groups scored higher on all domains. Mostly there was a gradient in these scores (S-OCD > R-OCD > HC), with S-OCD scoring significantly (P < 0.001) higher than R-OCD (high but not significant on CC and CSC), which scored significantly higher than HC (high but not significant on POS).
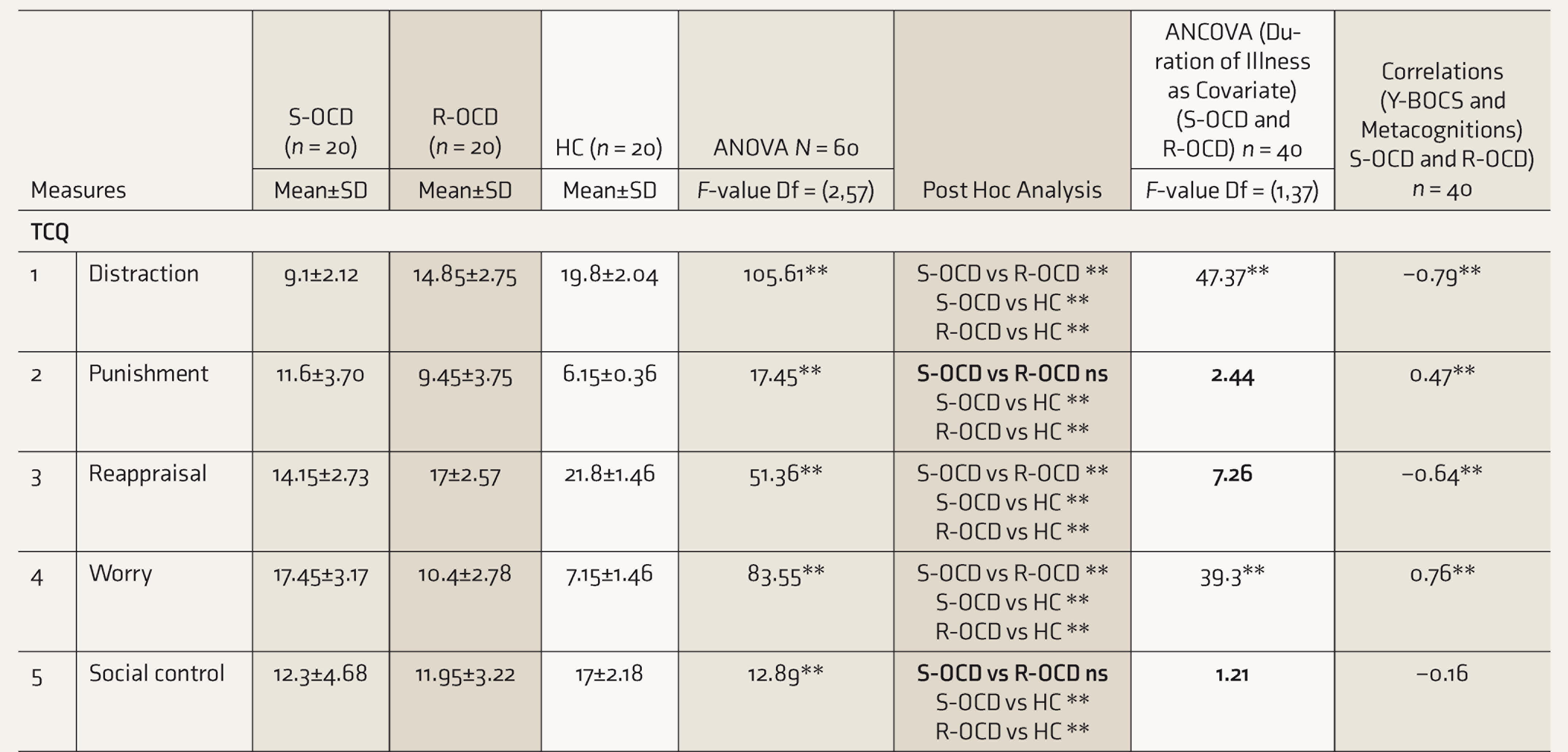
One-Way ANOVA and Post Hoc of Metacognitions (MCQ-30 and TCQ) by Clinical Groups and Control Group. ANCOVA (Duration of Illness as Covariate) and Correlations (Y- BOCS and Metacognitions) in the Clinical Groups
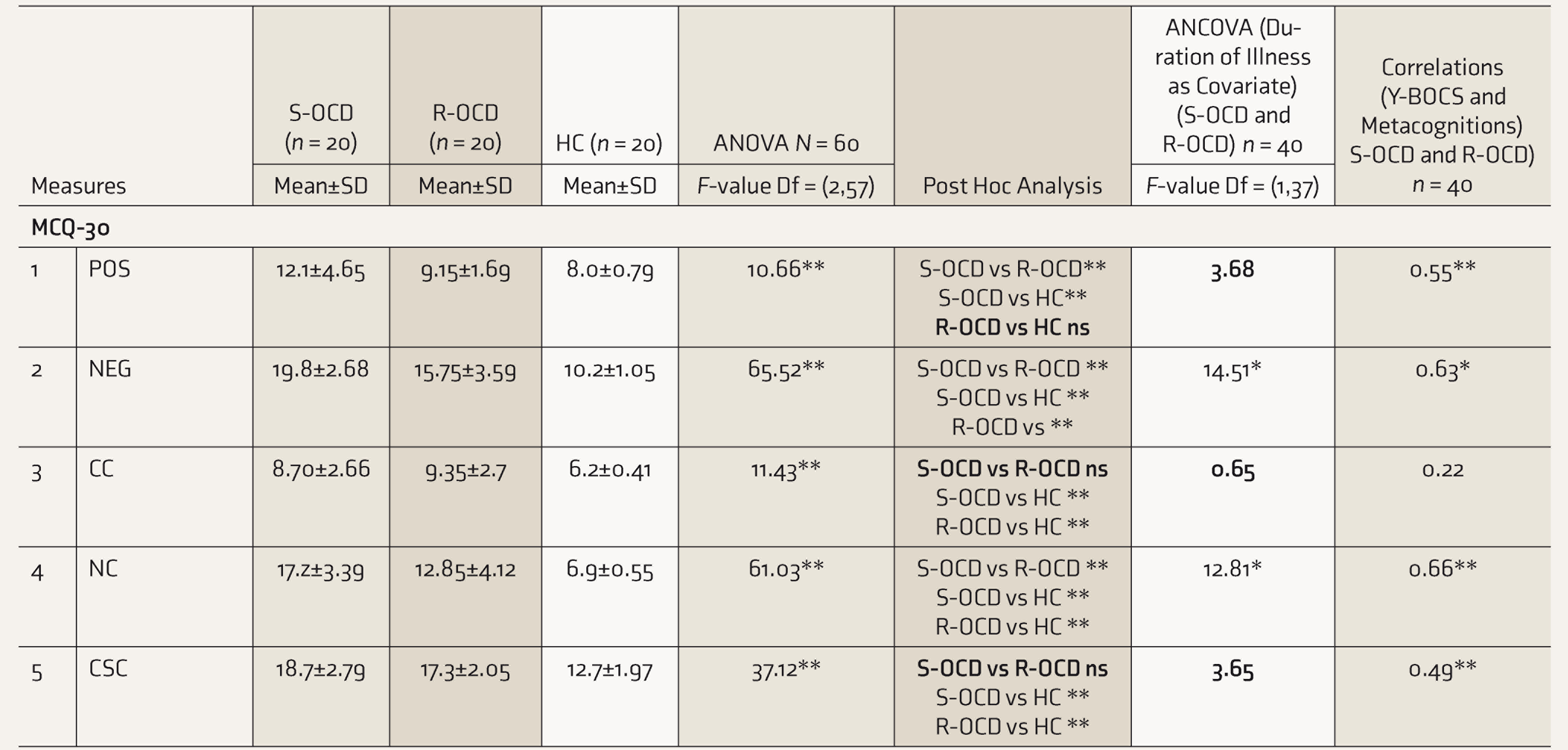
ns: not significant, S-OCD: symptomatic OCD patients, R-OCD: remitted OCD patients, HC: healthy controls, MCQ-30: Meta Cognition Questionnaire, TCQ: Thought Control Questionnaire, POS: positive belief, NEG: negative belief, CC: cognitive confidence, NC: thought control, CSC: cognitive self-consciousness.
**Significance at P < 0.001, *significance at P < 0.01.
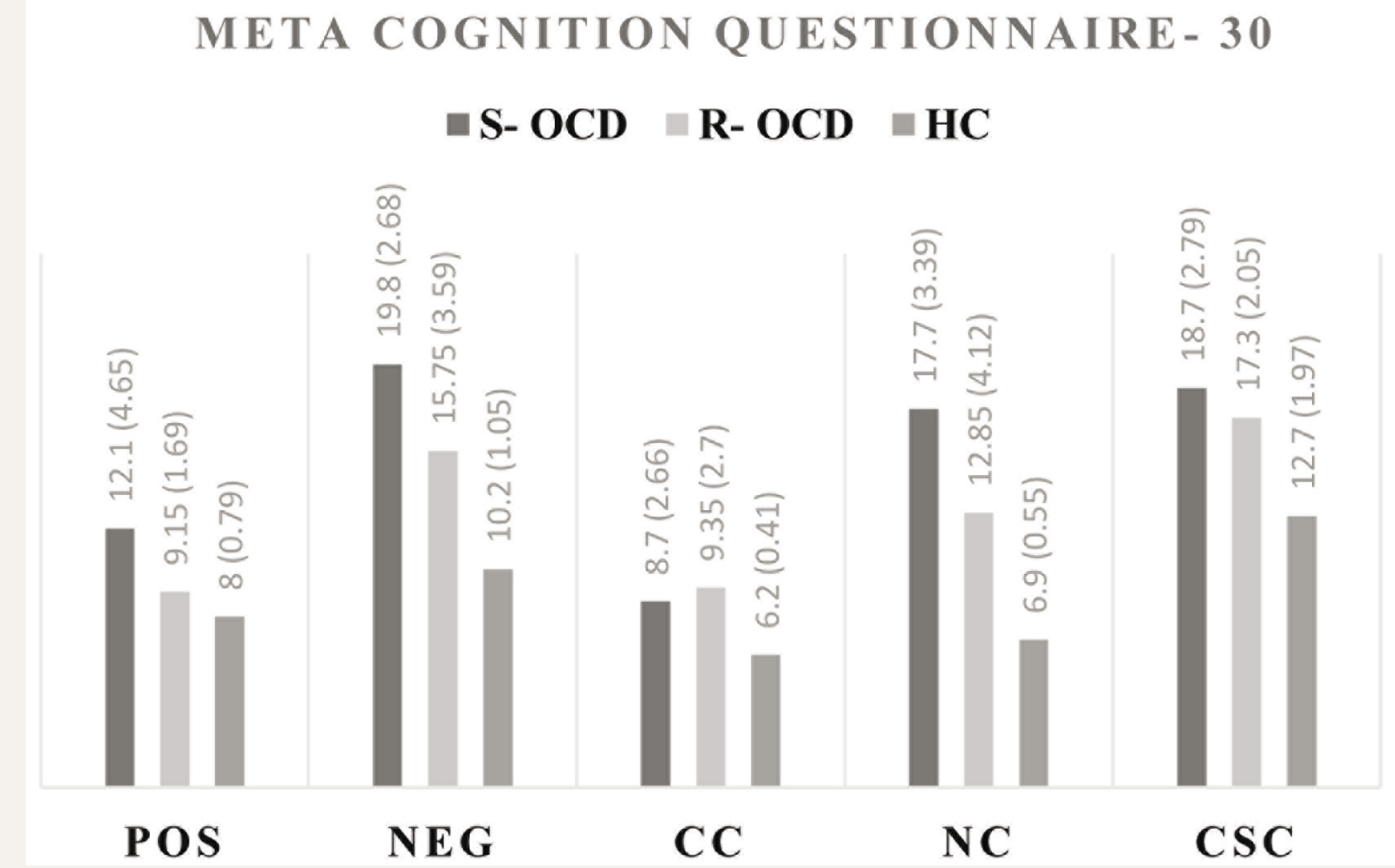
S-OCD: Symptomatic OCD Patients; R-OCD: Remitted OCD patients; HC: Healthy controls; POS: Positive Belief, NEG: Negative Belief, CC: (lack of) Cognitive Confidence; NC: Thought Control; CSC: Cognitive Self-Consciousness.
S-OCD: Symptomatic OCD patients; R-OCD: Remitted OCD patients; HC: Healthy controls.
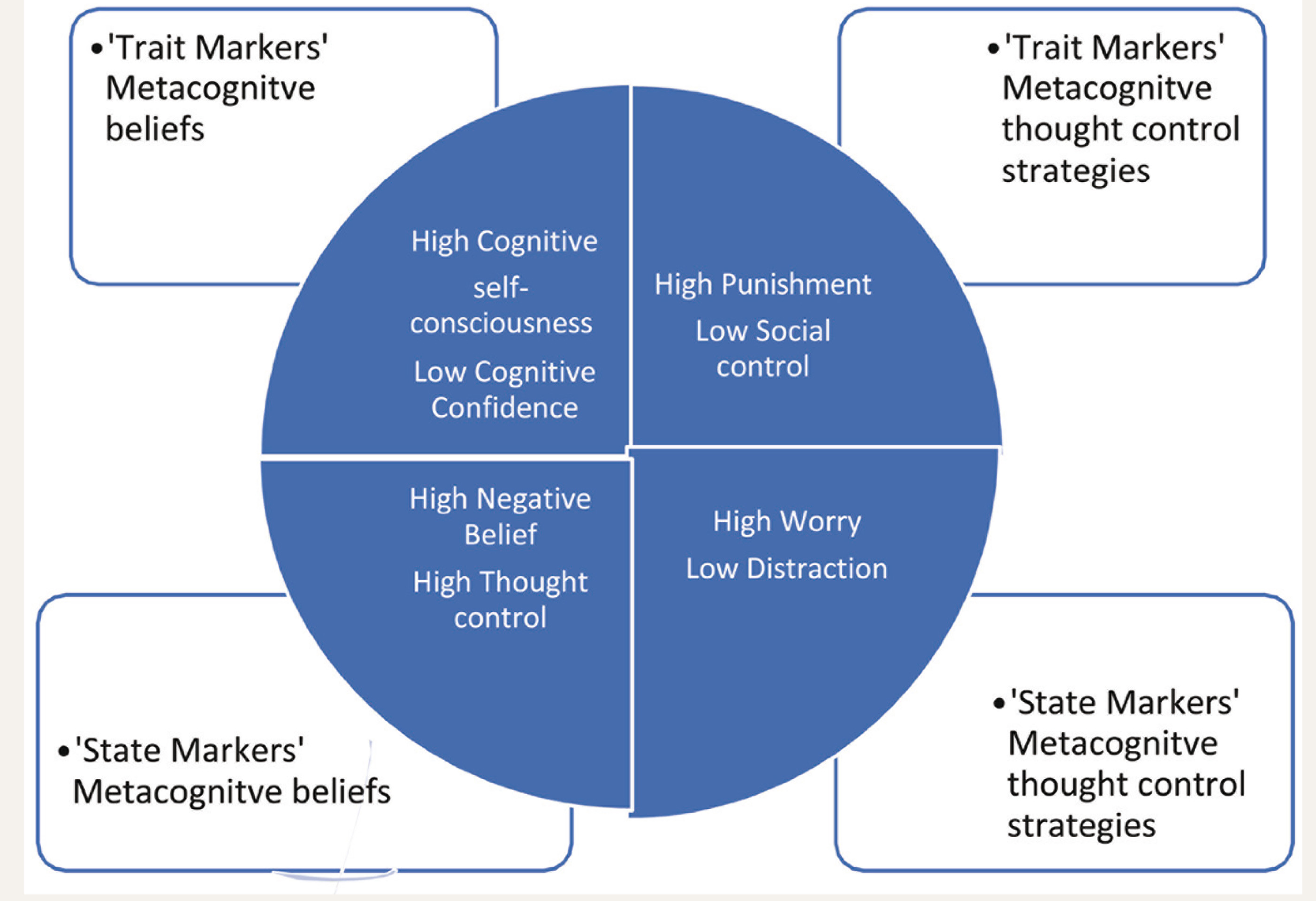
Explaining Trait and State Metacognitions in OCD (On the Basis of Preliminary Findings of Study)
On TCQ, OCD patients differed from HC on all domains. While distraction, reappraisal, and social control were significantly highest (P < 0.001) in HC and lowest in S-OCD (S- OCD < R-OCD < HC), a reverse order was found for punishment and worry (S-OCD > R-OCD > HC). However, here the differences within the subgroups of OCD were not significant in punishment and social control.
Differences Between OCD Subgroups
On conducting ANCOVA in S-OCD and (Table 2) to study duration of illness as a covariate and eliminate the effect of variation in course, results showed that the variables NEG, NC, distraction, and worry showed a significant difference between S-OCD and R-OCD. In contrast, no significant difference was found on POS, CC, CSC, punishment, reappraisal, and social control.
Association Between Severity of OCD and Metacognitions
After adjusting the effect of duration, in OCD subgroups, the correlations between severity of illness (Y-BOCS scores) and metacognition showed high positive correlation with NC (r = 0.66, P ≤ 0.001), NEG (r = 0.63, P ≤ 0.001), r = 0.76, P ≤ 0.001). High negative correlation was found with distraction (r = –0.79, P ≤ 0.001) and reappraisal (r = –0.64, P ≤ 0.001) (Table 2). Moderate positive correlations were found on POS (r = 0.55, P ≤ 0.001), CSC (r = 0.49, P ≤ 0.001), and punishment (r = 0.47, P ≤ 0.001). There were poor correlations with CC and social control.
Discussion
The present study looked at metacognitive beliefs across symptomatic and remitted OCD patients and healthy controls. The three groups in the study did not differ on any sociodemographic characteristics. Studies show that metacognitions are likely to be affected by sociodemographic characteristics.35–37 Majority of the participants in the present study belonged to the age group of 18–30 years, similar to most studies that report higher prevalence of OCD in young adults. 38
Differences Among the Study Groups
Our findings of ANOVA and post hoc (Table 2, Figures 1 and 2) of MCQ-30 and TCQ suggest that generally there were higher unhelpful metacognitions in both OCD subgroups. S-OCD scored higher than R-OCD who scored higher than HC (S-OCD > R-OCD > HC) in NEG “negative beliefs about worry concerning uncontrollability of thoughts and danger,” NC “need to control thoughts,” and “worry” and the reverse was found in “distraction” and “reappraisal” ( S-OCD < R-OCD < HC). This finding is consistent with Well’s S-REF model, which proposes that CAS, a pattern of thinking involving negative metacognitive beliefs regarding dangerousness and significance of intrusive thoughts, may be the causal and maintaining factor for OCD. 39 These findings are also supported by studies that have focused on the role of unhelpful metacognitions in distinguishing OCD patients from non-clinical controls.40,41 Consequently, our first hypothesis that OCD patients (symptomatic and remitted) will have more maladaptive metacognitive beliefs and thought control strategies than healthy controls was accepted.
Differences Between OCD Subgroups
While trying to explore differences between the S-OCD and R-OCD, we conducted ANCOVA to establish the extent to which the differences between the subgroups remain unchanged with changes in the duration of illness. This was done because the mean duration of OCD was different for the symptomatic and remitted groups. This observation agrees with a common reflection that patients take a longer time to reach the remitted phase.
A closer look at post hoc analysis and ANCOVA shows that differences between specific metacognitions (higher CSC, CC, punishment, and lower social control) remain “not significant” after post hoc and ANCOVA . On the other hand, certain other metacognitions (increased NEG, NC, worry, and lower distraction) were significantly different between the two OCD subgroups. This is further supported by our findings of the partial correlational analysis, which was used to assess the adjusted correlation between the severity of OCD and metacognitions. The correlations between severity of illness (YBOCS scores) and metacognition showed a high positive association with NC, NEG, and worry; a high negative correlation with distraction; and poor correlation with CC and social control; this further supports the above findings. Post hoc and ANCOVA findings are not consistent on POS and reappraisal, and hence, their role is questionable.
Trait and State Metacognitions and Phase of OCD
The role of trait and state metacognitions in OCD can be understood in terms of a vicious cycle (Figure 1). Our findings imply that persons with OCD have higher traits of “cognitive self-consciousness” (“I think a lot about my thoughts”), “lack of cognitive confidence” (“I have little confidence in my memory for words and names”), “punishment” (“I get angry at myself for having the thought”), and deficits in “social control” (“I talk to a friend about the thoughts”). These may impact other metacognitions that are state dependent in symptomatic phase, namely “negative beliefs about uncontrollability and danger of worry” (“my worry is dangerous for me”); “need for control,” “worry” (“I focus on different negative thoughts”), deficits in adaptive thought control strategies of “distraction” (“I think about something else”), and “reappraisal” (“I analyze the thought rationally”). These maladaptive strategies, such as worry and punishment, may result in biased perceptions of threatening stimuli and increase intrusive thoughts by an increased focus on threatening stimuli. An increase in the chances of detecting unwanted thoughts and triggering intrusions may lead to other unhelpful metacognitions. 11
Our findings are consistent with earlier studies that also found greater use of punishment and worry in patients with OCD when compared with HC.42–44 They found a reduction in the use of punishment post-treatment; we found no difference in punishment and social control between symptomatic and remitted patients, that is, at both stages of OCD, punishment was used more and social control less than by healthy controls.
The findings suggest that this tendency for state-level metacognitions is significantly exaggerated during the active phase of the illness. It is possible that these dysfunctional cognitions improve with time as there is an improvement in symptoms45,46 and hence contribute as state markers. Our study shows that with the progression in the state and phase, certain unhelpful metacognitions also decline. This suggests that treatment may have a significant effect on the severity of OCD and the state level metacognitions. Hence, this provides a preliminary evidence that certain metacognitions have a role of trait markers while certain other metacognitions have a role of state markers. Therefore, our second hypothesis that there will be a significant difference in all metacognitions between symptomatic and remitted OCD patients was rejected.
Small sample size and cross-sectional design may have impacted the findings of this study. Moreover, comparison to some other anxiety conditions, such as generalized anxiety disorder, may have given more information in terms of cognitive markers of OCD. Analysis in terms of symptom profile of OCD may have given further information about metacognitions in this disorder. Another limitation was that the translated scales were not validated. It is possible that other aspects of the illness type of treatment may have also impacted thought control strategies. However, studying these variables was not possible with our cross-sectional design. Future studies should look at these phenomena in a larger sample of patients, using a longitudinal or prospective design. Identifying these dimensions as markers in future studies may be useful in treatment decisions, such as the use of metacognition-focused interventions even in the remission phase, to moderate the risk of relapse.
The strength of this study is that it compares metacognitive beliefs and thought control strategies between OCD patients at two stages of the illness (namely, symptomatic and remitted phases) and healthy controls. We included only those OCD patients who did not have comorbid psychiatric disorders; therefore, findings were not affected by the presence of, say, depression or other anxiety disorders. Individuals with mood and anxiety disorders have been noted to be different in the pattern of metacognitive beliefs and thought control strategies.
Conclusion
The study highlights the differences in metacognitive beliefs and thought control strategies in individuals with OCD and healthy controls. We found that compared to healthy controls, OCD patients have significantly higher unhelpful metacognitive beliefs. These findings showed a gradient, being highest in the symptomatic OCD group and lowest in healthy controls, suggesting that the course of illness may impact metacognition and thought control strategies. However, certain metacognitive beliefs (cognitive confidence and cognitive self-consciousness) and thought control strategies (punishment and low social control) did not differ between the phases of symptomatic and remitted OCD. These small metacognitions may play a role in all stages of illness, that is, onset, recovery, and relapse. The study provides preliminary evidence for the possible role of certain metacognitions to be trait and state markers of cognitive and metacognitive therapy response.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.