
Abstract
Background:
There is a decline in cognitive and functional skills in older adults. The objective of this study was to compare the effects of cognitive and mind-motor training (MMT) on cognition and functional skills in a community-dwelling sample of older adults.
Methods:
In this observer-blinded randomized clinical trial, 40 older adults with medical stability, ability to comprehend and respond to simple verbal instructions, no diagnosed psychological disorders, absence of severe visual and hearing problems, the capacity to walk independently, and a score of more than 46 in Berg Balance Scale were included. They were randomly allocated into cognitive or MMT groups. Cognitive training (CT) was practiced with activities for memory and attention, using paper–pencil tasks. MMT was practiced using a simple, indoor based square-stepping exercise. They practiced one-hour of training per day, three days a week, for eight weeks.
Results:
General linear model analysis showed that the time by groups was not statistically significant. The mean (standard deviation) scores in General Practitioner Assessment of Cognition Scale and Hindi Mental State Examination improved significantly (P < 0.001) following MMT [1.75 (1.29); 2.4 (1.34)] and CT [1.5 (1.36); 2.7 (0.99)]. The functional skills measured using Lawton Instrumental Activities of Daily Living Scale revealed beneficial changes for both the groups. None of the outcomes were statistically significant between the groups (P > 0.05).
Conclusion:
Both cognitive and MMTs showed similar practice effects on cognition and functional skills in community-dwelling older adults.
Cognitive decline and restricted daily functioning are common among community-dwelling older adults. CT and MMT benefit cognition and functional skills of older adults.Key Message:
Both the cognitive training (CT) and physical exercises benefit cognition and brain plasticity in older adults. Each type of training impact the structural and functional connectivity of brain and improve different cognitive functions. 7 Physical exercise strategies improve the physical capacity, quality of life, and some domains of cognitive function. 8 The CT targets cognitive functioning directly or indirectly as opposed to the interventions focusing on behavioral, emotional, and physical function. 9 It might alter the structural connectivity and intrinsic activity of the brain through increased cerebral blood flow in prefrontal and posterior cingulate cortices. 10 It can be given individually or in groups, using repetitive exercises designed to improve single or multiple cognitive abilities. 5 Hill et al., 11 in their systematic review, concluded that computer-based CT is beneficial on global and domains of cognitive function and psychosocial performance of older adults with mild cognitive issues.
A systematic review concluded that CT and physical exercise strategies were beneficial in improving the cognitive function in older adults over the usual therapy care. Simultaneous inclusion of physical and cognitive dual-task practice is benefiting various aspects of cognitive function in healthy older adults over single-task training. 12
A novel strategy, MMT is a feasible mode of dual-task strategy to influence the cognitive functioning in older adults. The MMT, a square-stepping exercise, is a cognitive-based memory-motor task that enhances the metabolic activity of hippocampus. 13 It is a simple, low cost, indoor, group-based exercise program practiced in older adults. 6 It is a visuospatial working memory task that requires physical exertion, focused attention, memory, and execution. The participants are asked to memorize and execute the foot placement patterns involving forward, backward, lateral, and diagonal steps, using a gridded floor mat. 14
Boa Sorte Silva et al. found that extra 15 minutes of MMT, compared to multiple-modality exercises, did not show superior changes in global cognitive functioning or walking speed among older adults. However, they found trends of more cognitive improvement, particularly in memory, warranting future studies with increased exercise duration of MMT.15, 16 The evidence on the benefits of MMT on the memory, attention, and executive function of the older adults remains unclear. We hypothesized that in the older adults, MMT that simultaneously engages cognitively and physically (i.e., dual-task performances) would cause therapeutic benefits similar to those of well-established CT on cognition and functional skills. The objective of the study was to compare the effects between the MMT and CT on cognition and functional skills in community-dwelling older adults.
Materials and Methods
Study Design
This observer-blinded, randomized clinical trial was approved by the institutional research committee of Chitkara University. Ethics approval was obtained from the ethics committee of Fortis hospital, Punjab, India, and the study was registered in the Clinical Trial Registry of India (CTRI/2018/01/011334).
Participants
The community-dwelling healthy older adults were contacted in a senior citizen library, Mohali, through purposive sampling, from January 2017 to April 2018. Written informed consent was obtained from them before the study, seeking their voluntary contribution and active participation. Healthy older adults aged above 65 years, able to comprehend and respond to simple verbal instructions, able to speak and read Hindi language, and with a history of forgetting the conversation and names of friends and relatives in the past two years, who scored above 46 in the Berg Balance Scale were included. People were excluded if they were diagnosed with severe mental illness, Alzheimer’s disease, or schizophrenia; had issues in vision, hearing, or communicating; had an inability to walk independently; or scored more than 4 points in the 2-items’ Patient Health Questionnaire (PHQ-2). 17
Procedure
Older adults meeting the eligibility criteria were randomly assigned either into CT or MMT by an observer who was not involved in collecting the outcome measurements or conducting the training. The method of allocation was block randomization. The block size was eight. From every block, four chits were assigned to CT and MMT groups each and were concealed in thick envelopes. The training was administered by two qualified physical therapists having four years of clinical experience working with the geriatric population. All the outcome measurements were collected at baseline and eight weeks after the training by an independent assessor blind to the treatment groups.
Sample Size Estimation
After MMT, a mean change of one point in the General Practitioner Assessment of Cognition Scale (GPCOG) or Lawton Instrumental Activities of Daily Living (IADL) Scale was considered clinically relevant, with a 5% significance level (α = 0.05) and 80% power (1 – β) of the study. We estimated a sample size of 20 for the MMT group, expecting a 10%–15% dropout. Having a comparative group, that is, CT, we needed a total sample size of 40.
Interventions
Cognitive Training
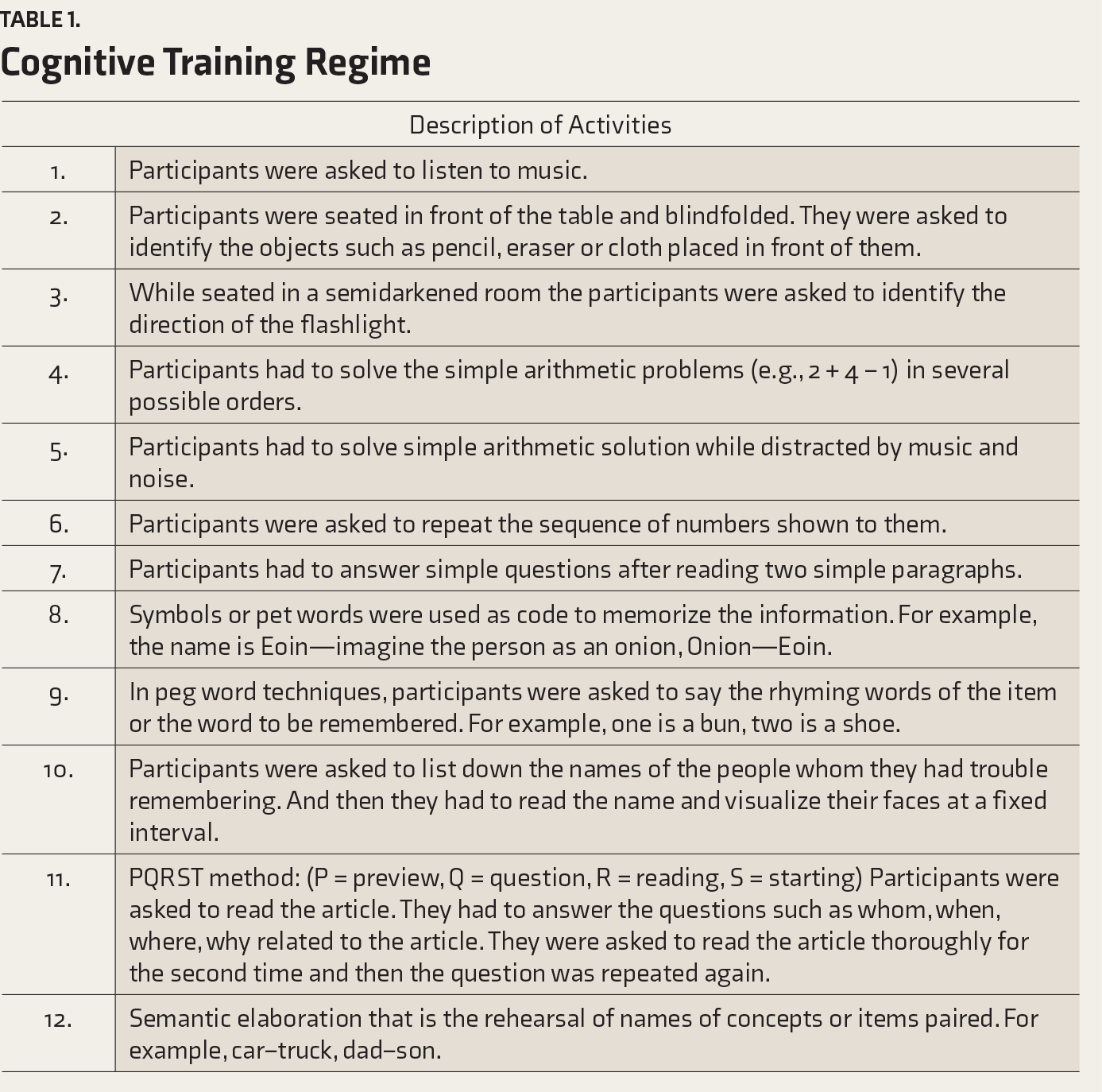
In CT, the therapy session commenced with activities for memory and attention, with paper–pencil tasks. The attention training mainly focused on the ability to solve problems with or without distractions and the ability to concentrate on specific tasks such as reading and listening to music or story. The memory training was focused on the verbal episodic memory. Participants were taught mnemonic strategies for remembering word lists and sequences of items and recall strategies. A detailed description of the activities of CT is given in
Cognitive Training Regime
Mind Motor Training
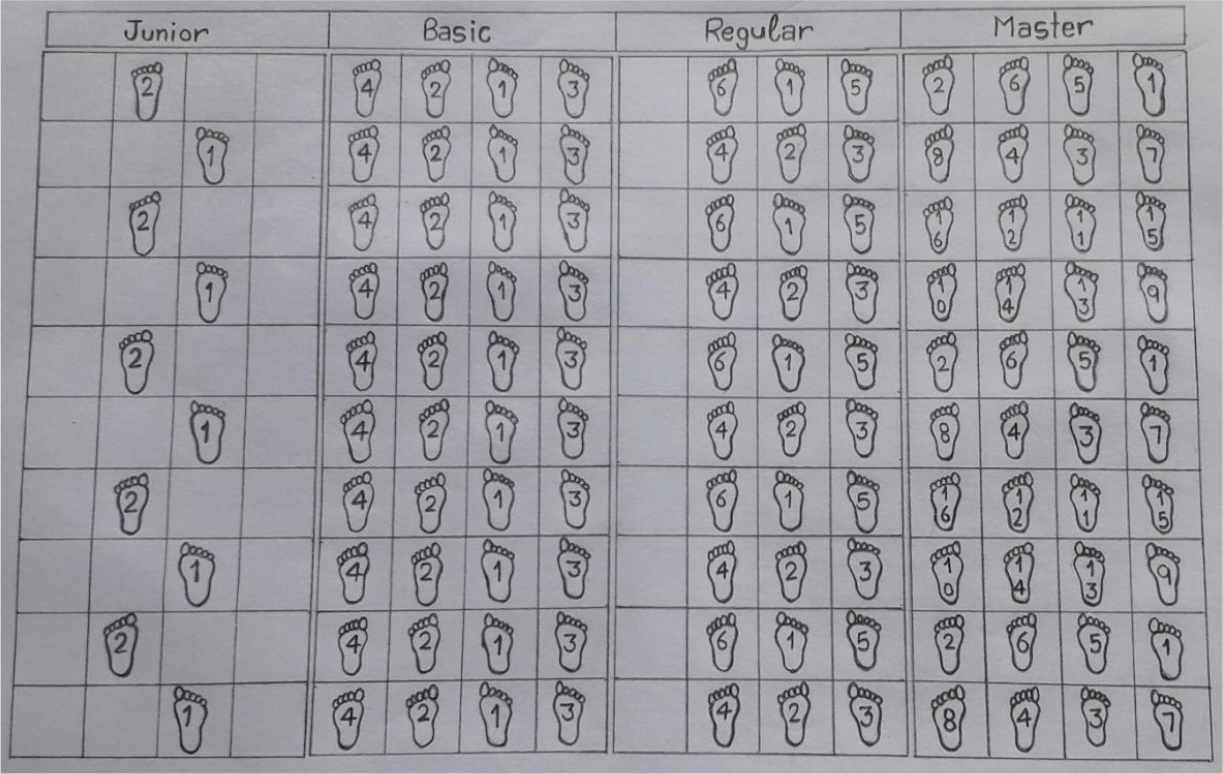
The MMT commenced by setting up a square, nonslippery, stepping mat, with dimensions of 100 × 250 cm
2
. The mat had 40 squares, in 4 rows and 10 columns. Each side of a square had a dimension of 25 cm. The exercise consisted of different levels of stepping patterns, named junior, basic, regular, and master. The junior-level pattern was initially demonstrated to the participants, and they were asked to memorize the pattern and perform it. They had to repeat the correct pattern three times and then progress to the next stepping pattern (
Different Levels of Mind Motor Training Exercises
The participants from both the MMT and CT groups received the therapist’s supervised individual training sessions. They practiced a 1-hour training session in a day, 3-days a week, for 8-weeks.
Outcome Measures
The GPCOG was the primary outcome measure. The Hindi version of the Mini-Mental State Examination (HMSE) and the Lawton IADL Scale were the secondary outcome measures.
GPCOG is a cognitive screening instrument that measures time orientation, memory, and information. It has two domains: patient assessment and informant interviews. The patient assessment score ranges from 0 to 9, impaired to normal. If an older adult score 5–8 points in the feature of patient assessment, he/she was required to have an informant interview, which is scored from 0 to 6. A higher score in the informant assessment indicates less cognitive impairment, and a score of 4–6 suggests the absence of significant cognitive impairment.18, 19 This tool was reported to have a sensitivity of 0.85, specificity of 0.86, and inter-rater reliability of 0.75. 20
The Mini-Mental State Examination has been proven for its diagnostic accuracy (sensitivity of 0.85) and specificity (0.90).21, 22 Its cross-culturally adopted Hindi version, HMSE, was administered to test the cognition of the older adults.23, 24 The HMSE is a paper-based cognitive screening tool that measures orientation, immediate memory, remote memory, language, and visuospatial memory. The HMSE has a maximum possible score of 30. Lower scores indicate severe cognitive dysfunction, and a score above the cut-off point of 24 refers to normal cognitive function.23, 24
The Lawton IADL measurement identifies how an individual meets daily functioning at the current moment and over a while. In contrast to measures of activities of daily living, the Lawton IADL assesses the complex process of independent living skills. This tool measures eight domains of functional skills, such as the ability to use a telephone; do shopping, housekeeping, and laundry; prepare food; use modes of transportation; take responsibility for own medications, and handle finances. A summary score of zero indicates the person is completely dependent on others for activities of daily living (low functioning), and the score of 8 reflects complete independence in functional skills. The inter-rater reliability of Lawton IADL was 0.85, and it has been validated with the clinical measures of functional status. 25
Statistical Analysis
Data were analyzed using SPSS version 16 (TEAM EQX). Baseline demographic variables of continuous and dichotomous measures were evaluated by student’s paired t-test and the chi-square test, respectively. Levene’s test evaluated the equality of variance for the continuous variables. We observed that the data of 40 older adults were normally distributed; therefore, repeated-measures ANOVA was performed. The general linear model analysis was performed to determine the change in the outcome measurements over time (from baseline to post-training) and between the groups (CT and MMT). The tests of within-subjects’ effects were observed in Greenhouse–Geisser analysis after assuming the sphericity from Mauchly’s test. Intention to treat analysis was performed to handle the missing values of post-training measures. The within-group analysis was conducted using a paired t-test. A P value < 0.05 was considered statistically significant.
Results
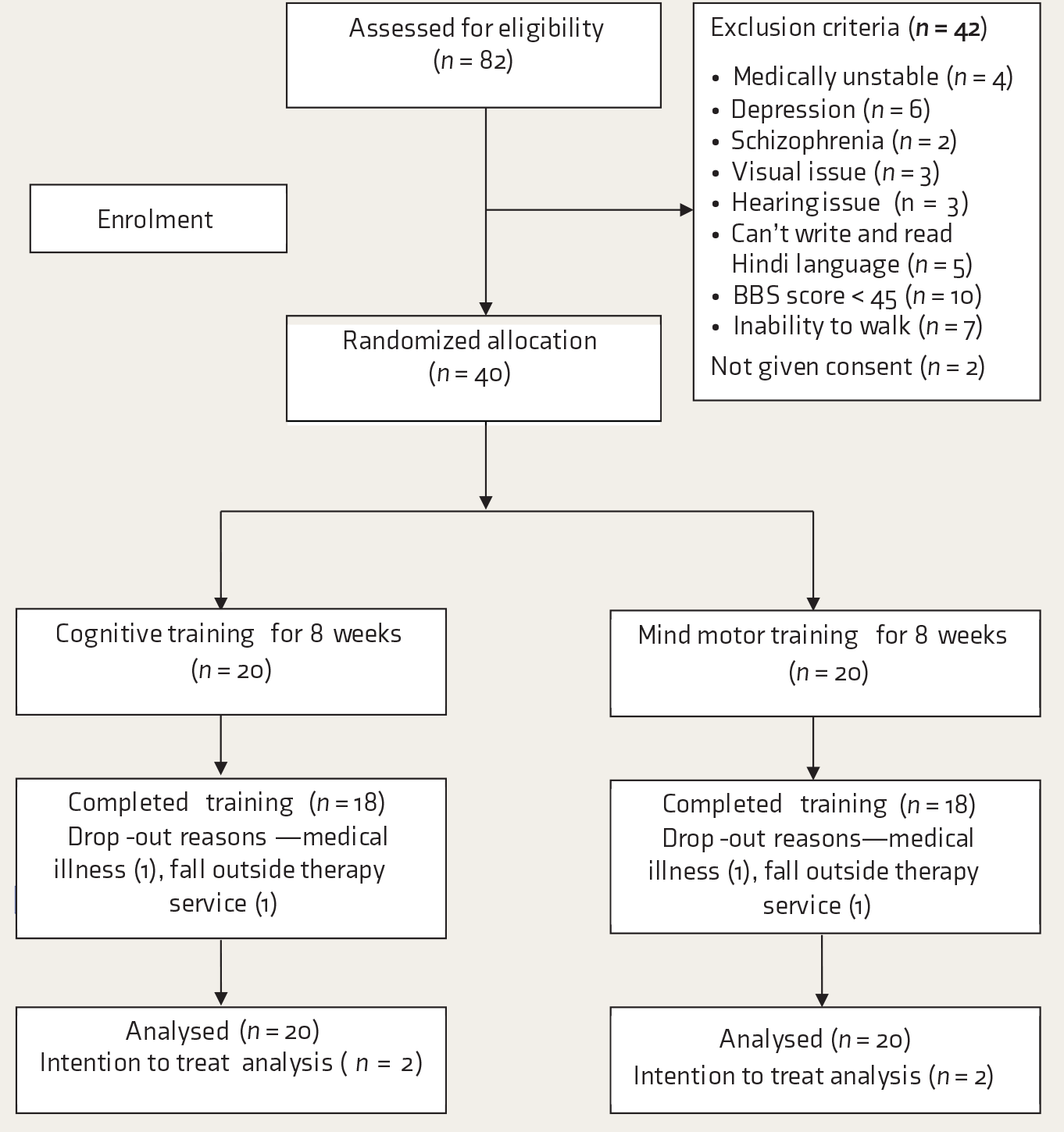
The study organization is shown in a CONSORT flowchart (
Baseline Characteristics (N = 40)
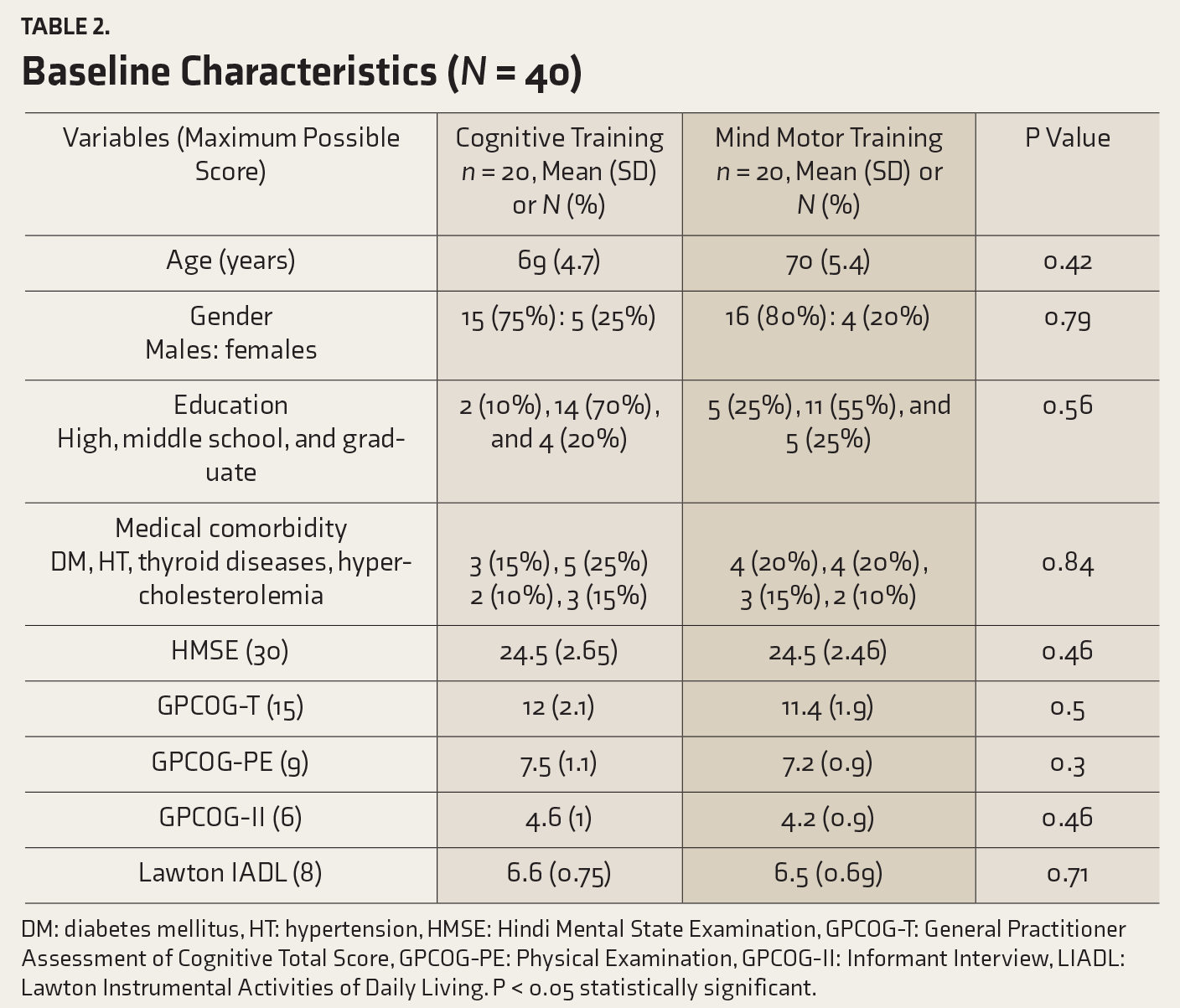
DM: diabetes mellitus, HT: hypertension, HMSE: Hindi Mental State Examination, GPCOG-T: General Practitioner Assessment of Cognitive Total Score, GPCOG-PE: Physical Examination, GPCOG-II: Informant Interview, LIADL: Lawton Instrumental Activities of Daily Living. P < 0.05 statistically significant.
CONSORT Flowchart
At baseline measurement, only five participants had the maximum score of 15 in the GPCOG. Under the patient examination subset of GPCOG, 12, 14, and 8 participants scored 8, 7, and 6 points, respectively. Likewise, 13 participants each scored 5 and 4 points in the informant interview. Nine participants who scored 3 in the informant interview were considered to have definite cognitive dysfunction. In the HMSE, 13 participants scored below 24 points. Four participants were functionally independent, scoring 8 points on the Lawton IADL, whereas 35 were found to be functionally dependent. Of them, 20 scored 6 points and 15 scored 7 points in the IADL measurement.
There was a statistically significant difference (P < 0.001) in the mean scores of all the outcome measurements across time. There was no significant differences in the mean scores of outcome measures between the groups, implying that the change is similar for both CT and MMT groups. For within-group comparison, all the outcome measures were statistically significant post-training (P < 0.001) in both the CT and MMT groups. There was a statistically significant improvement in the combined mean (standard deviation) score of GPCOG following MMT (1.75 (1.29), P < 0.001) and CT (1.5 (1.36), P < 0.001). After eight weeks of practice, there was a similar improvement in the HMSE for the MMT [2.4 (1.34)] and CT [2.7 (0.99)] groups. The Lawton IADL measures nearly changed by one point for both groups, post-training. The change in the outcome measures within- and between-groups is shown in
Within-Group and Between-Group Comparison of the Outcome Measures
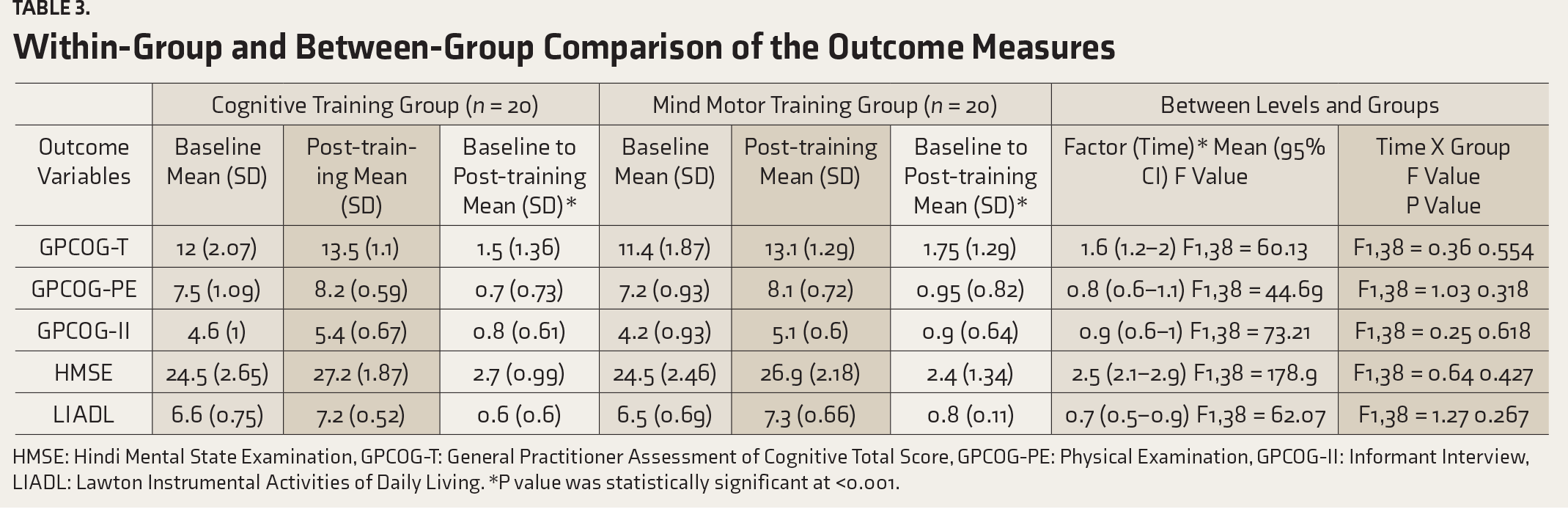
HMSE: Hindi Mental State Examination, GPCOG-T: General Practitioner Assessment of Cognitive Total Score, GPCOG-PE: Physical Examination, GPCOG-II: Informant Interview, LIADL: Lawton Instrumental Activities of Daily Living. *P value was statistically significant at <0.001.
Discussion
To the best of our knowledge, this is the first study comparing the MMT and CT in community-dwelling healthy older adults. The major finding is that both the interventions are equally beneficial in improving cognition and functional skills of older adults. Dementia among the older adults is one of the rising concerns in India, and approximately 4.1 million people have dementia. The incidence rate of dementia would double by 2030 and become three-fold by 2050, 26 warranting preventive and therapeutic approaches to cognitive decline in the older adults.
A change score of 1.5 in the GPCOG and 2.7 points in the HMSE supports CT. CT with attention (with or without distraction), problem-solving, concentration, verbal episodic memory, and mnemonic recall might increase the overall cellular activity and metabolic rate in the white matter of the brain. We also observed that 43% (n = 17) and 63% (n = 25) of the sample scored 13–14 points at baseline and post-training, respectively. Post-training, 18% of the older adults (n = 7) scored the maximum possible 15 points in the combine-GPCOG favors CT and MMT. The CT is supported by the fact that it induces brain plasticity mechanism and positive neurophysiological and neuroanatomical changes across the brain. 10 It might alter the structural connectivity of the brain and increase the cerebral blood flow in the prefrontal and posterior cingulate cortices, 10 which are responsible for memory, mental imagery, and willed actions. 27 Evidence exists that CT enhances verbal memory, visual memory, attention/concentration, recall of personal information, and face-name recall. 27 It had shown beneficial improvement in patients with Alzheimer’s disease and in those with mild cognitive impairment who are at risk of developing cognitive impairment. 28
A change score of 1.75 in the GPCOG and 2.4 points in the HMSE supports the MMT. The reason for these improvements might be that MMT stimulates the visuospatial working memory and also involves physical tasks that require concentration, memory, and orientation. During the practice session of stepping patterns of junior, basic, regular, and master levels, the participants were physically active and asked to memorize the pattern. Our findings are supported by Teixeira et al. 14 who showed that in the older adults, MMT, as a global cognitive stimulation, had a positive influence on the cognitive functions, particularly the concentrated attention, mental flexibility, and visual memory. On the other hand, a short duration of MMT in addition to multiple-modality exercises, over 24 weeks, showed similar practice gain on cognition and mobility among the older adults as opposed to multiple-modality exercises alone.15, 16
CT and MMT were equally beneficial on physical skills in older adults. Following CT or MMT, only five individuals scored below a cut-off score of cognitive decline in MMSE compared to 13 individuals who scored below 24 points at baseline. Compared to the baseline measurement (10%, n = 4), 33% of older adults (n = 13) attained functional independence, the maximum score of 8, in the Lawton IADL; this supports both the interventions. Similarly, 60% of older adults (n = 24) had a score of 7 points in the said measure post-training, compared to 30% (n = 15) at baseline. Most of the study participants were males and reported that laundry and food preparation were not their daily instrumental activities.
Limitations and Future Directions
The study findings should be cautiously interpreted due to the following limitations. First, this study had a small sample size, lacked a traditional control group, and did not conduct follow-up assessments. Second, 63% of participants (n = 25) had at least middle school educational qualifications (8 years of education) and better socioeconomic status. Third, the distribution of the sociodemographic characteristics of the study participants is not representative of the community-dwelling older adults. Fourth, the GPCOG and HMSE tools have floor and ceiling effects, warranting that future trials should use more sophisticated neuropsychological tests to measure the cognitive functioning of the older adults with cognitive decline. Fifth, issues with balance and risks of fall were not considered. The benefits of MMT and CT on mobility and quality of life would be of interest in a future trial. Last, the metabolic, emotional, and motivational factors that determine the cognitive functions of the older people were not taken into consideration. Depressive disorder is a common mental health morbidity in the older adults, which can have a significant impact on cognitive functioning,29, 30 warranting the use of PHQ-9 in future effective studies on CT and MT.
Conclusion
The MMT and CT regimes are equally beneficial in improving cognition and functional skills in the community-dwelling healthy older adults.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.