
Abstract
Background:
Coronary heart disease (CHD) is an impending global pandemic in developed countries as well as developing countries and economies in transition, such as India. A significant increase in the incidence of myocardial infarction (MI), one of the most common types of CHD, is being reported in India, and the incidence and severity of the disease are more among the youth in Kerala. Studies assessing the association between psychological factors and MI are few in India.
Methods:
We adopted a case-control study design. A total of 150 cases (with MI) and 150 controls (without MI and matched for age and gender) from a tertiary care hospital in Trivandrum, Kerala, India, were selected using convenient sampling method, between September 2016 and August 2017.
Results:
As compared to 33.3% of the controls, 50.7% of patients with MI had type D personality characteristics. Multivariate logistic regression analysis after adjusting for the confounders indicated a positive and statistically significant association between type D personality and MI: OR = 4.14, 95% CI = 2.19–8.85, P = 0.003.
Conclusion:
Type D personality is associated with MI.
Psychological factors influence triggering of myocardial infarction (MI). Therefore, a detailed psychological evaluation of all patients with MI should be carried out at admission to a hospital along with clinical evaluation for identifying psychological factors which would have influenced the current admission. Preventive measures should be undertaken to limit the negative effects of psychosocial factors associated with MI, both in the hospital and community.Key Messages:
Type D personality is characterized by an experience of increased negative distress, including anxiety and inhibition of social interactions. 7 Previous studies had found that type A personality was a major factor in the development of CHD among healthy middle-aged men. 8 A 22-year follow-up study, however, found that type A behavior is not a predictive factor in the development of CHD. 9 The concept of type A behavior reflects a heterogeneous hodgepodge of behavioral symptoms and signs. 10 On the other hand, type D construct is a homogenous subgroup with clear and stable personality traits having a comprehensible conceptual basis in psychological theory. 11
Denollet et al. 12 were the first to propose ‘type D’ or ‘distressed’ personality type. They stated that individuals with this personality characteristic experience high levels of negative affectivity (NA) and high levels of social inhibition (SI) at the same time. They experience negative emotions all the time and will not express these emotions while interacting with others owing to the fear of negative response in return. This suggests that it is not only the negative emotions that risk an individual for CHD but also the pattern of their style of coping with these emotions. Individuals with increased NA are liable to have frequent incidences of dysphoria, anxiety, and irritability. They are also likely to have a negative outlook of themselves and tend to search for looming troubles in the world. 7
Type D is related to low heart rate variability (HRV) levels and bad lipid profiles and could lead to pathophysiological changes amounting to cardiac autonomic imbalance. 13 A prospective study demonstrated a link between type D personality and hyperlipidemia in patients with MI.12, 14 Type D was an important predictor of coronary artery spasm, which can eventually lead to MI and sudden death. 15 Type D personality also predisposes to increased psychological distress and unhealthy lifestyle behaviors, 6 leading to cardiac diseases.
Studies assessing the association between type D personality and MI among the Indian population are very limited, and there are no studies on Keralites. Therefore, this study was undertaken with the primary objective of evaluating the association between type D personality and MI in Keralites.
Materials and Methods
Study Design and Setting
This was a case-control study. The setting was a 650-bedded tertiary care hospital in Kerala, with more than 40 medical specialties and over 2,500 out-patients taking service on a given day.
Selection of Participants
We used a convenient sampling method and recruited as cases 150 patients who were admitted to the inpatient wards of cardiology with the first episode of MI (incident cases) diagnosed as per the hospital protocol (patient symptoms including angina, abnormal ECG changes, and elevated cardiac Troponin [Troponin T—high sensitivity]) and satisfying the inclusion criteria (natives of Kerala living in and around Trivandrum District, between the age of 25 and 65 years, both males and females, admitted during the study period [August 2017–September 2018]). An equal number of age- and gender-matched consecutive patients (n = 150) who satisfied the inclusion criteria were selected from the in-patient wards of General Medicine Department as controls. Patients with unproven MI, history of any other cardiac disease, hypertension, diabetes, cognitive impairment, current or past history of psychiatric illness, or other major diseases (AIDS, cancer, chronic obstructive pulmonary disease [COPD], and physical deformations); those on antipsychotic medications; non-consenting patients; and all unstable patients were excluded from the study. We obtained data for excluding patients with other major diseases from the hospital medical records or directly from the patients. Controls who were similar in age and sex to the cases were recruited around the same date and evaluated for risk factors of CHD, to ensure that the underlying exposures were not affected by the time of recruitment.
Study Variables
A standard demographic questionnaire was designed for recording details on gender, domicile, age, religion, marital status, living status, education, occupation, monthly income, and details of consumption of alcohol, smoking, and regular physical exercise.
Type D personality scale is a 14-item scale comprising two subscales: a 7-item subscale that measures NA (items 2, 4, 5, 7, 9, 12,13) and a 7-item subscale measuring SI (items 1, 3, 6, 8, 10, 11, 14). Respondents rate their personality on a 5-point Likert type scale, which ranges from 0 = false to 4 = true (items 1 and 3 are reverse-scored). The NA and SI scales can be scored as continuous variables (range 0–28) to assess these personality traits independently. A cut-off of 10 was made to dichotomize participants: Scores ≥10 indicate type D personality, and scores <10 indicate non-type D/NA or non-type D/SI personality. 12
The instrument was available in English but it was not available in Malayalam (the native language). Therefore, we used the “forward translation and back translation” method to translate the English version of the questionnaire to Malayalam. In the first step, the researcher took the help of two bilingual subject experts and translated the original English version into Malayalam (forward translation). The difference in the translations by the bilingual experts was examined and discussed with experts, and a consensus was reached. The final version was translated back to English (back translation) by two English Professors who did not know anything about the questionnaires. The differences in the two back translations was examined and discussed with the English Professors, and a final consensus was reached. The back translation was compared with the original questionnaire and an acceptable difference was found between the two. The translated Malayalam version was pre-tested among five myocardial patients, and the patients were asked to comment on the items. The patients reported that certain words are ambiguous and that certain expressions are not good. The forward translators, MMT and KAJ reviewed the comments received from the pre-test patients, and changes were accordingly made in the final version. The content and face validity of both English and Malayalam instruments were checked by experts in the field of social work, psychology, sociology, cardiology, and nursing, and they endorsed good content and face validity.
The reliability of the questionnaire has not been tested earlier among the study population (MI patients). Therefore, we decided to validate the questionnaire in this group. We used the test–retest reliability method to check the reliability of the English and Malayalam questionnaires. Both the English version and the translated Malayalam version had good reliability scores, “r” above 0.70.
Sample Size
Based on the proportion of cases and controls with type D personality (34.3% and 32.2%, respectively) in a previous study in a similar setting, 17 the estimated minimum sample size for this study was 221 with a 90% confidence interval (CI) and 90% power. To improve the accuracy of the results, an additional 79 samples were added, and thus, the total sample size was estimated to be 300. Accordingly, 150 each of the cases and controls were recruited.
Data Collection
The details of the medical conditions of the patients admitted to the in-inpatient wards of the Cardiology Department (cases) and Medicine Department (controls) were obtained from the electronic medical records of the hospital. Permission for accessing the electronic medical records was obtained from the hospital management, and permission for including the patient in the study was taken from the treating physicians. We initiated the data collection procedures only after receiving the approval for the study from the Institutional Human Ethics Committee of the hospital.
MMT obtained informed consent from the study participants after explaining the purpose as well as the risks and benefits of participating in the study. The questionnaire was handed over to them with the request to return the completed questionnaires within 3–4 hours. The methodology adopted for collecting the data was self-administration by the patients.
Data Analysis
The statistical analysis was performed using IBM SPSS version 20.0 software. Frequencies and percentages were calculated for the categorical variables. We employed the chi-square test to identify the statistical significance of the association of categorical variables such as sociodemographical and psychological factors with MI. Univariate and multivariate analysis (binary logistic regression) was used to find the association between type D personality and MI. P value < 0.05 was considered as statistically significant.
Results
The study participants (150 cases and 150 controls) were recruited from diverse backgrounds and socioeconomic status. The controls included patients with viral fever (dengue, chicken guinea, hepatitis A), bacterial infections (typhoid fever, scrub typhus, leptospirosis), urinary tract infection, urticaria, pyelonephritis, and acute gastroenteritis. The median time of administration of the questionnaires to the patients was within one week of their presentation to the hospital.
The majority of the cases were from urban areas (84 [56.0%]), whereas the majority of the controls (94 [62.7%]) belonged to rural areas (P = 0.004), and 30 (20.7%) of cases were divorced or unmarried as against 16(10.7%) the controls. A larger proportion of cases were reported to be consuming alcohol (91 [60.7%] of cases vs 70 [46.7%] of controls, P = 0.02) and were smoking (89 [59.3%] of cases vs 39 [26.0%] of controls, P ≤ 0.001) as well (
Demographical Profile of Cases and Controls
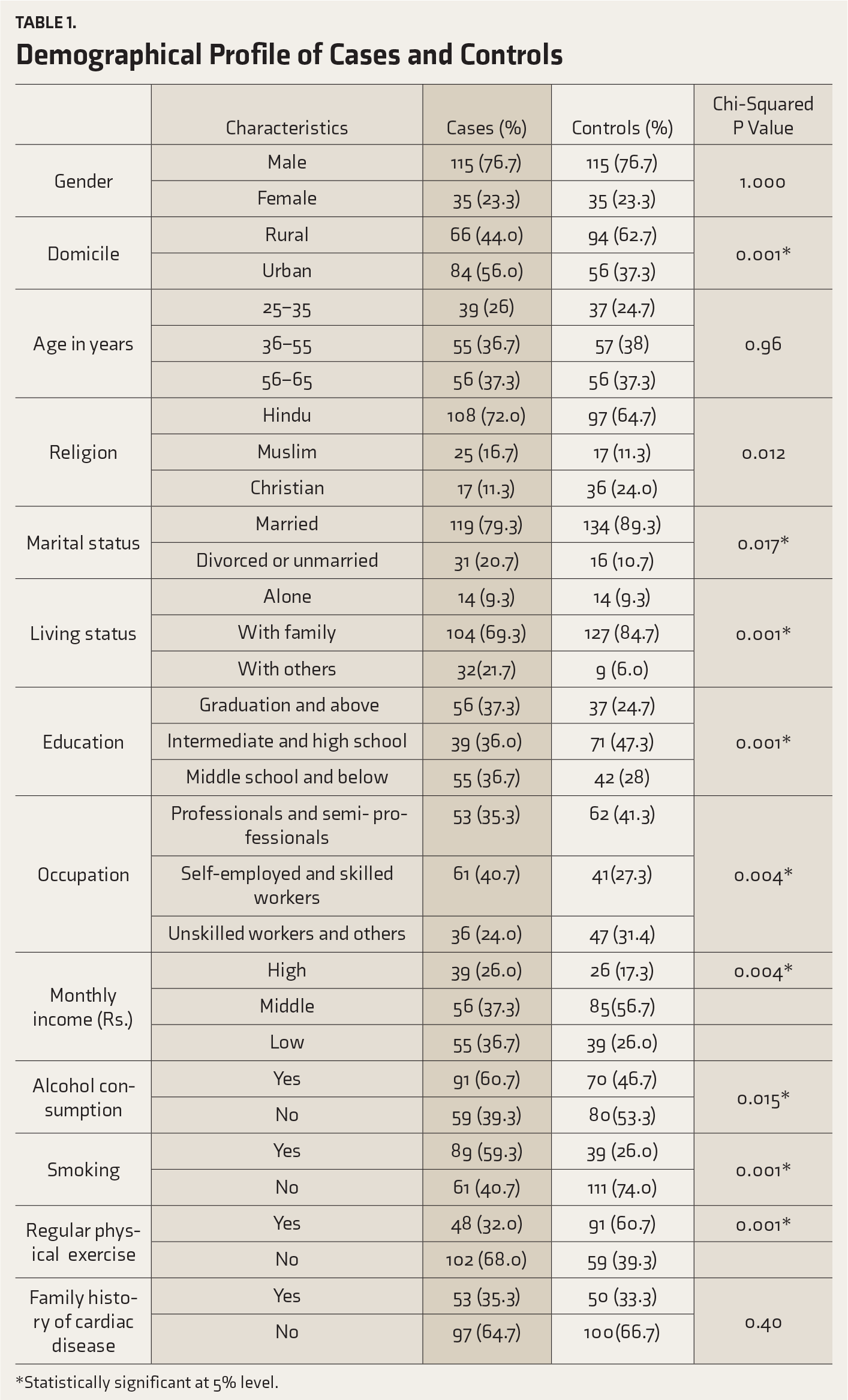
*Statistically significant at 5% level.
Among the cases, 76 (50.7%) had type D personality as compared to 50 (33.3%) of the controls. There was a statistically significant association between type D personality and MI (P = 0.002). Univariate logistic regression analysis revealed that type D personality was positively and significantly associated with MI: OR = 2.05, 95% CI = 1.29–3.28, P = 0.002 (
Association Between Type D Personality and Myocardial Infarction
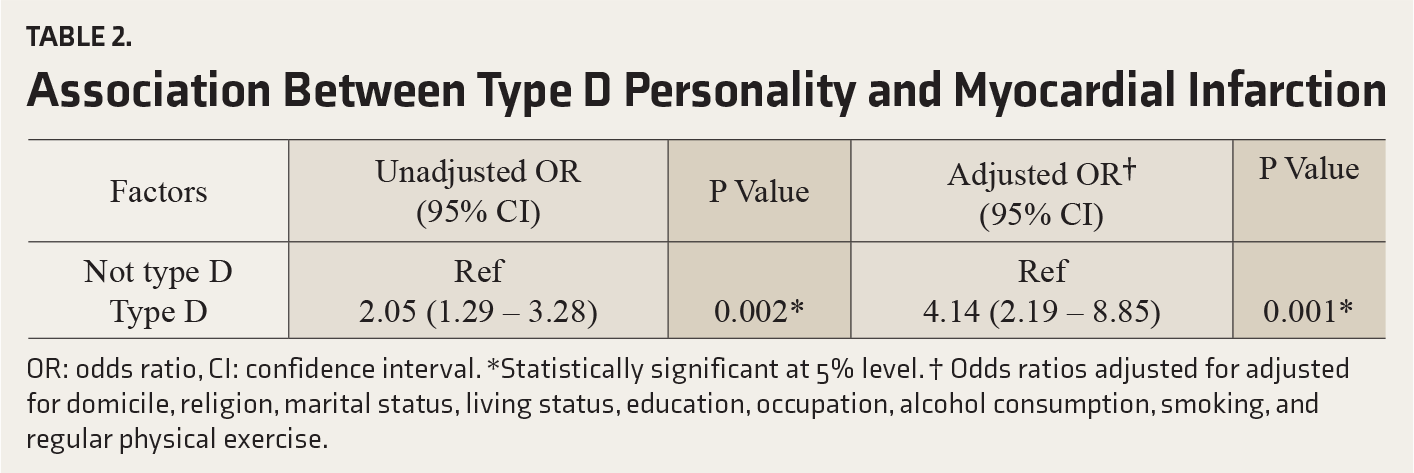
OR: odds ratio, CI: confidence interval. *Statistically significant at 5% level. † Odds ratios adjusted for adjusted for domicile, religion, marital status, living status, education, occupation, alcohol consumption, smoking, and regular physical exercise.
Discussion
The univariate analysis of our data revealed a positive and statistically significant association between type D personality and MI. The association remained significant in the multivariate analysis after adjusting for confounding factors (domicile, religion, marital status, living status, education, occupation, alcohol, smoking, and regular physical exercise). Our results are comparable with the observations of Svansdottir et al., 14 who also found that individuals with type D personality are at a higher risk for MI. Martens et al. 18 also had found that individuals with Type D personality have >2.5-fold higher risk for MI, re-infraction, and mortality.
Studies on the proportion of type D personality characteristics among the MI population in India are few. A recent study by Menon et al. reported a proportion of 24% of type D personality characteristics among patients with MI. 19 Studies conducted in other countries have reported a significantly varying proportion of type D personality among patients with MI.20, 21
Studies have indicated that persons with type D personality experience negative emotions. They are unlikely to express these in their social interactions. 7 Type D persons have higher psychological distress and unhealthy lifestyle behaviours, 16 and these are recognized as causative factors for the incidence, progression, and adverse prognosis of CHD. 22 This has been further affirmed by biological mechanisms associated with type D personality, which have been identified in previous studies. Lin et al. 13 stated that type D personality is associated with low HRV and increased total serum cholesterol and low-density lipoprotein (LDL) cholesterol levels, which are known to increase the risk of development of atherosclerotic plaques. Bagherian-Sararoudi et al. 14 observed that hyperlipidemia, which is one of the established risk factors for MI, is common among persons with type D personality. Contrary to the above, Jamil et al. and Yoshimasu and Fukuoka23, 24 indicated that it is not type D but type A behavior pattern that is a significant predictor for cardiac diseases.
Our study has implications in three domains: psychological assessment and diagnosis, psychological treatments, and prevention of MI. While assessing a patient with cardiac problems, type D personality, along with other psychosocial factors, also may be considered along with the clinical factors. Psychological treatments or interventions for cardiac patients are often not viewed seriously. These treatments should aim at facilitating early recovery from the disease and healthy life after recovery. Type D personality or other psychological problems do not usually trigger cardiac problems suddenly but might trigger them slowly. Hence, early detection and initiation of proper preventive strategies can be effective.
There are both strengths as well as limitations in our study. To the best of our knowledge, this is the first well-designed study in India assessing the association between Type D personality and MI. We used a case-control design with higher internal validity to realize the study objectives. A demographically matched comparison group was included, controlling for age and sex. Standardized questionnaire that has been validated internationally and was further validated in our population was used. Our study had a robust sample size necessary to demonstrate an association between type D personality and MI. The limitations of our study include the retrospective non-randomized design, usage of a convenient sampling method, and recruitment of patients only from Kerala. Every case-control study is prone to “recall bias,” and our study also has the same limitation. Even though we adjusted for the potential confounding variables, there may be other variables that were not part of this study, and those might have influenced our results. It is important to note that the questionnaire has not been used earlier in our cardiac in-patient settings, and the test–retest reliability of the questionnaires is yet to be established using a large sample size. The previous mental status of cases or controls was not evaluated. The possibility of having overestimated the perceived levels of psychosocial risk factors of cases, who had an acute coronary event (MI), cannot hence be ruled out.
Conclusion
Type D personality characteristics are found to have a statistically significant association with MI. Further prospective studies are required to establish this finding in the Kerala population.
Footnotes
Acknowledgments
We are grateful to Professor A Joseph, Director, Academics; Dr CC Kartha, Sr Advisor, SOCOMER; and Dr PM Saffia, Vice Dean, Academics, Kerala Institute of Medical Sciences Trivandrum, for their unwavering support and sharing pearls of wisdom with us during the drafting of this article. We are also thankful to Ms Ann Elizabeth Thomas, Biostatistician, KIMS, Trivandrum, and Ms Greeshma Ravidran, Biostatistician, AIMS, Cochin, Kerala, for their support in statistical matters.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.