
Abstract
Internationally, research on mental health literacy (MHL) is increasing. However, the complex interplay between MHL components is not fully understood due to methodological limitations. We aimed to investigate the reciprocal links between beliefs, recognition ability and attitudes towards depression and schizophrenia in Ghana using the novel network analysis approach. A total of 410 participants from the general population of Ghana were included in a vignette-based study focusing on the Western concepts of depression and schizophrenia. Participants provided their impressions of a hypothetical person described in a vignette depicting either the Western concept of depression or schizophrenia symptoms. They then completed a set of validated MHL instruments, along with providing demographic information. Our findings indicated that spiritual causal attribution was the most influential variable in the network model for depression, whereas personal stigma emerged as the variable with the greatest impact in the model for schizophrenia. There was a reciprocal link between personal stigma and psychosocial causal attributions across the mental disorders and religiosity was positively linked to seeking professional help for these disorders. There was a bidirectional link between help-seeking preferences and causal attributions across the two disorders. Spiritual causal attributions were inversely related to professional help-seeking for both disorders. These findings emphasize the intricate interconnections between beliefs and attitudes towards depression and schizophrenia. Uncovering cultural and belief systems that are not explicitly expressed, as well as addressing stigma and incorporating the Western nosology of mental disorders, could promote mental well-being.
Mental Health Literacy (MHL), coined by Anthony Francis Jorm and his colleagues, refers to individuals’ understanding of mental disorders, enabling identification, management and prevention. MHL comprises four main aspects: (a) preventing mental disorders; (b) knowledge on first aid strategies for mental disorders; (c) self-help for mild to moderate mental disorders; and (d) recognizing specific mental disorders (Jorm et al., 1997). MHL plays an essential role in enhancing mental well-being and combating stigma (Adu et al., 2021a; Jorm, 2012). For instance, correct recognition of the Western concept of mental disorders was linked to early professional help-seeking for these conditions (Kitchener & Jorm, 2006; A. Wright et al., 2007). There is also evidence supporting the link between the endorsement of social support as mental health help-seeking and MHL (Jung et al., 2017). Attributing the causes of mental disorders to the Western concept of mental health nosology (i.e., biological and psychosocial factors) correlated with more positive attitudes towards mental health and improved mental health outcomes. However, spiritual causal attributions of mental disorders have been associated with negative attitudes towards mental health, such as stigma and reduced inclination to seek help for mental health issues (Adu et al., 2023; El-Khoury et al., 2004).
Stigma surrounding mental disorders is prevalent across various populations. For example, in the case of depression and schizophrenia, the mental disorders of focus for this study, research has identified key differences in societal perceptions. Schizophrenia patients are often viewed as more dangerous and unpredictable compared to individuals with depression (Angermeyer & Matschinger, 2003). Additionally, studies have shown that participants tend to express greater social distancing attitudes towards individuals with schizophrenia than those with depression (Martensen et al., 2020). The literature has also indicated a higher prevalence of mental health stigma among Africans compared to Western countries. For instance, Ghanaian medical students have shown higher levels of mental health stigma than their Australian counterparts (Lyons et al., 2015). The experience of mental health stigma has been linked to various negative well-being outcomes, including feelings of isolation and loneliness. Individuals experiencing mental health stigma may be denied jobs, housing or educational opportunities. Many are also hesitant to seek help for fear of being stigmatized, which could delay treatment and worsen their conditions (Adu et al., 2021a; Javed et al., 2021).
Moreover, several other factors have been identified that link to MHL, such as sex, education, trust, and religiosity (Cavanagh et al., 2022). Notably, the literature has revealed mixed findings concerning MHL and stigma, since high MHL levels have been associated with both reduced and increased stigma (Simões de Almeida et al., 2023). Of note, a plethora of evidence has reported that females exhibit better MHL compared to their male counterparts in terms of recognition ability and the Western view of help-seeking for mental disorders (Koopmans & Lamers, 2007; Mackenzie et al., 2006). Cultural and traditional masculinity sex roles are significant barriers that hinder men’s willingness to seek help for mental health issues (Addis & Mahalik, 2003). Similarly, educational levels have been found to directly relate to the Western view of MHL, such as recognizing symptoms of depression and schizophrenia (Lee et al., 2020). Moreover, the international literature has emphasized age as a significant influential factor of MHL. Older age predicted better help-seeking for mental disorders (Mackenzie et al., 2006), whereas younger individuals are more likely to recognize mental disorders (Hadjimina & Furnham, 2017). Nevertheless, the influence of religiosity on MHL has not shown a consistent trend in the literature. In some contexts, such as Ghana, higher levels of religiosity have negatively impacted MHL, with pentecostal pastors being more likely to adopt a diabolical explanatory model of mental health (Asamoah et al., 2014). Conversely, in other contexts like China, higher levels of religiosity have been associated with better MHL and reduced social distance towards individuals with mental disorders (Wang et al., 2019).
Clearly, the field of MHL research is expanding globally. However, a significant gap exists in the literature concerning the African continent, particularly sub-Saharan Africa, including Ghana. Thus, the majority of studies have been conducted with samples that can be described as Western Educated, Industrialized, Rich and Democratic (WEIRD; Henrich et al., 2010). Additionally, prior research has often failed to identify the central and highly influential variables among the studied factors. This limits the ability to develop targeted interventions and guide efforts to mitigate poor mental health outcomes. In other words, research fails to identify the most critical variable(s) within the constellation of constructs used in a particular study, whose change could lead to a ripple effect in others. In some cases, the influence of certain variables on the outcome variable is either underestimated or overestimated due to the lack of evidence regarding the complex patterns of the relations between variables, which could yield valuable insights into effective intervention strategies (Hevey, 2018). For instance, in a network analysis, researchers discovered that social factors, which were not originally part of the health behaviour model, were significant predictors of vaccination attitudes (Langley et al., 2015). This suggests that this methodology has the potential to aid in developing a conceptual framework that integrates various factors into health outcomes, enhancing our understanding of health behaviours.
Largely, health research has traditionally approached phenomena in isolation. For example, the current dataset has been previously analysed in segments using regression models (e.g., Adu et al., 2023). While this approach offers valuable insights for health-related interventions, it is not suitable for exploring the complexities associated with the interconnected factors as theorized by the current biopsychosocial approach to health. Thus, a significant methodological limitation found in the current MHL literature is the tendency to linearly treat MHL components as cause (independent) and effect (dependent) in various studies (e.g., Adu et al., 2024). This approach is rigid and arbitrary, overlooking the interconnectedness and reciprocal nature of MHL components, as well as their relative influences compared to other factors. This highlights the need for a specific statistical approach that can examine these components collectively within a single study (Hevey, 2018; Medvedev et al., 2021).
In recent times, the field of health psychology has embraced the novel and advanced network analysis to examine the complex interaction between biological, social, and psychological factors and their influence on health and well-being (Hevey, 2018). This suitable method reflects the current biopsychosocial view to health. The network analysis reveals unique relations between variables and confirms theorized connections, a promising avenue for understanding and addressing the dynamics of health-related variables (Hevey, 2018; Huth et al., 2023). This method quantifies the significance of each variable within the network, highlighting central variables for targeted interventions (Borsboom & Cramer, 2013; Haslbeck & Waldorp, 2018). While we did not formulate specific hypotheses due to the nature of the current analysis, the present study aimed to model the complex interplay between MHL regarding the causes of mental disorders, help-seeking preferences, recognition ability, demographic factors, religiosity, and stigmatization concerning the Western concept of depression and schizophrenia in Ghana using the novel and advanced network analysis. The study intended to contribute to the understanding of mental health dynamics in Ghana by revealing the reciprocal interconnectedness of these factors, providing valuable insights for culturally tailored interventions. Furthermore, the study presented a novel approach to enhancing health research, a method suitable for analysing the recommended biopsychosocial influences on health, facilitating a comprehensive understanding of mental health issues. This approach could enrich the global literature on mental health by focusing on unique cultural contexts and could inform policymakers and practitioners about effective strategies to improve mental health outcomes in Ghana and other countries in sub-Saharan Africa.
The present study focused on major depression and schizophrenia, out of the 297 disorders in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (American Psychological Association [APA], 2013), because these two disorders are extensively studied in MHL research due to their global prevalence and economic impact. These disorders also carry substantial burdens in terms of caregiver demands and disability (Ahmed et al., 2018; Organization, 2001). For instance, during the COVID-19 pandemic, it was reported that the global Disability-Adjusted Life Years (DALYs) for depression increased by 16.4% between 2010 and 2021 (Mettananda & Mettananda, 2024). Additionally, both disorders are linked to stigma and significantly impact individuals’ quality of life, often resulting in substantial healthcare costs and decreased productivity (Javed et al., 2021; Tóth et al., 2023). The disorders are associated with distinct symptoms: major depression is characterized by a persistent low mood, fatigue, sleep disturbances and a loss of interest or pleasure in daily activities, while schizophrenia is commonly marked by hallucinations, delusions, disorganized behaviour and social isolation, which can profoundly affect an individual’s daily functioning and social relationships (APA, 2013).
Method
Participants
We recruited 410 participants from the general population of Ghana. The sample majorly comprised individuals with at least junior high school formal education. Among the participants, 66% (n = 272) were men, 34% (n = 138) were women and .3% (n = 2) did not specify their sex. Participants’ age ranged from 18 to 61 (Mage = 27.6, SD = 5.4). In terms of education, 72.4% (309) had completed a bachelor’s degree, 14.6% (60) had a master’s degree, 9.5% (39) had completed senior high school and .5% (2) were junior high school leavers.
Power Analysis
Monte Carlo sample size simulation-based methods have recommended that a minimum sample size ranging from 250 to 350 participants is required to achieve valid and reliable parameters, such as sensitivity, specificity and weight correlations for psychological network analysis consisting of 20 nodes or fewer (Constantin et al., 2023). Therefore, the current sample size is sufficient to achieve a higher statistical power.
Procedure
The study received ethical approval from the Institutional Review Board (IRB) of the researcher’s previous institution, HSE University, Moscow. The snowball through convivence sampling method was employed for data collection, utilizing online platforms such as Facebook, WhatsApp, email, Twitter and Instagram. Despite online data collection limitations, this method was chosen for its cost-effectiveness and rapid access to a diverse population, and this approach was particularly suitable given Africa’s growing mobile-cellular subscription rate (Wright, 2005). Participants provided informed consent to participate in this study by clicking a button after reading the content of the consent information. They were made aware that their results may be published or used for academic purposes, including reports, presentations and public documentation, in aggregate form. Although Ghana has numerous local dialects, the questionnaire was exclusively presented in English, the country’s official language and medium of instruction at all levels in the education system. Demographic details were collected initially, followed by the main assessment measures. The deidentified dataset from the current study is not publicly available due to participants’ consent restrictions. However, the data can be made available to researchers upon reasonable request to the current author.
Measures
We adapted the online Computer-Assisted Telephone-Interview (CATI) scale, which was orignally developed in Australia (Reavley & Jorm, 2011) to assess MHL, including recognition ability, causal attributions, help-seeking and stigmatization regarding depression and schizophrenia. Each subscale (or component of MHL) of this comprehensive measure of MHL is described in the sections below. Since the original CATI scale was an interview-based questionnaire, the current study modified the questions into a survey format using an internet platform (SelectSurvey.net). The questionnaire has been used in similar studies internationally (Jorm et al., 2005; Yoshioka et al., 2014). The current study did not pilot-test this scale, since it is an already established measure of MHL (Hertzog, 2008). Firstly, participants were presented with two vignettes depicting unlabelled mental disorder symptoms, one for depression (‘John’) and another for schizophrenia (‘Peter’). After reading the scenarios, participants responded to questions about recognition ability, attitudes, causal attributions, and help-seeking recommendations. See Supplemental Material for the full vignettes.
The social stigma component on the CATI scale was assessed using a five-point Likert scale with five items, measuring participants’ willingness to interact socially with the hypothetical person in the vignette, with responses ranging from 1 = ‘strongly disagree’ to 5 = ‘strongly agree’. A sample item was: ‘Would you be happy to go out with Peter/John on the weekend?’ Internal consistency, using Macdonald Omega (ω), was very good for both depression (ω = .88; M = 3.67, SD = .85) and schizophrenia (ω = .89; M = 3.42, SD = .93).
The personal stigma category on the CATI scale was measured using an eight-item scale measuring participants’ personal attitudes towards the hypothetical individuals in the vignettes. The scale uses a five-point Likert scale, ranging from 1 = ‘strongly disagree’ to 5 = ‘strongly agree’. An example item reads: ‘John/Peter could recover if he wanted.’ We obtained the following internal consistency for both depression (ω = .50; M = 2.74, SD = .52) and schizophrenia (ω = .60; M = 2.85, SD = .60).
The perceived stigma scale on the CATI scale assesses participants’ perceptions of societal attitudes towards the hypothetical individuals with depression and schizophrenia. The scale includes eight items, and it uses the same statements and response rate as that of the personal stigma; however, the stems of the sentences started with ‘Most other people believe that. . .’. Internal reliability for depression (ω = .70, M = 3.16, SD = .67) and schizophrenia (ω = .74, M = 3.33, SD = .67) was acceptable.
The causal attribution subscale of the CATI scale measures how individuals ascribe causes to mental disorders on a scale of 1 = ‘strongly disagree’ to 5 = ‘strongly agree’. Participants indicated the extent to which they believed specific events contributed to the mental disorders presented in the vignettes. The psychosocial causes subset consisted of four items: ‘Traumatic experiences (neglect, childhood abuse, etc.)’, ‘Social disadvantages (poverty or debt)’, ‘life stressors’ and ‘not being able to think clearly’. Three items focused on biological causes: ‘a virus’, ‘brain chemical imbalance’ and ‘biogenetics’; and two items explored spiritual causes: ‘spiritual/demonic possession’ and ‘punishment from God’. Due to the limited number of items, these subcategories exhibited moderate internal consistency coefficients (Lee et al., 2016). Depression: psychosocial causes (ω = .57, M = 3.37, SD = .72), biological causes (ω = .57, M = 2.52, SD = .77), and spiritual causes (Spearman-Brown reliability coefficient = .60, M = 1.52, SD = .69). Schizophrenia: psychosocial causes (ω = .67, M = 3.09, SD = .77), biological causes (ω = .63, M = 2.72, SD = .77), and spiritual causes (Spearman-Brown reliability coefficient = .42, M = 2.04, SD = .91).
The help-seeking preferences subscale of the CATI scale asked participants to indicate how certain individuals could help the hypothetical persons in the vignettes. Helpers were categorised into three groups: ‘spiritual helpers (pastor, herbalist, traditional healer [Odusini])’, ‘professional helpers (psychiatrist, counsellor, psychologist, general practitioner/family doctor, nurse)’ and ‘social support (lecturer/teacher, close friend, close family member/friend)’. Responses were rated on a five-point Likert scale: 1 = ‘strongly disagree’, 5 = ‘strongly agree’ was used. Due to the limited number of items within the subscales (Lee et al., 2016), internal reliability coefficients ranged from adequate to good for depression (professional: ω = .74; social support: ω = .72; spiritual: Spearman-Brown reliability coefficient = .27) and for schizophrenia (professional: ω = .85; social support: ω = .81; spiritual: Spearman-Brown reliability coefficient = .52).
We measured religious importance with an adopted version of the Centrality of Religiosity Scale (CRS-10) (Huber & Huber, 2012). This scale was not pilot-tested, since it is an already established measure of religiosity. This scale has been used among similar samples within the context of the current study (Asamani & Mensah, 2016; Hertzog, 2008). A sample item of this scale included ‘To what extent do you believe that God or something divine exists?’ This five-item scale used a five-point Likert scale ranging from 1 = ‘not at all’ to 5 = ‘very much so’. Reliability of the scale was very good (ω = .80, M = 2.49, SD = .80).
Data Analysis
Data preparation and descriptive analysis were computed using jamovi (Version 1.2; Jamovi Project, 2020), while the network analysis was conducted using RStudio software (version 4.1.2; Team, 2021). The Missing Completely at Random (MCAR) test (Little, 1988) revealed that data were not missing at random (MCAR, p < .05). As a result, the Expectation Maximization (EM) algorithm data imputation technique was utilized to address the few missing data points (Malan et al., 2020). We applied the exploratory network analysis to explore the interrelation between causal beliefs, help-seeking preferences, recognition ability, demographic factors, religiosity and stigmatization concerning depression and schizophrenia. The Bayesian Gaussian graphical models (BGGM) package, accommodating both continuous and non-continuous variables, was employed for the estimations (Williams & Mulder, 2020). The relations between nodes were computed as posterior means, considering the effect of other variables. A partial correlation matrix was created, retaining associations within 95% credible intervals (CI) not including zero, indicating a strict significant p-value. BGGMs were computed for each disorder, with networks visualized through the ‘qgraph’ in R library, which is based on the Fruchterman-Reingold algorithm. The network layout was averaged across the BGGMs to allow for better comparison (Epskamp et al., 2012; Fruchterman & Reingold, 1991). Of note, nodes without connecting edges signified non-significant relations, not absence of association.
We further evaluated the predictability (i.e., the relative influence of each variable in the model) of all factors. By implication, a highly predictable variable has its variability accounted for by its connections to other variables within the network. This concept helps us to understand how certain variables influence or are influenced by others, providing insights into the interplay and dynamics among variables for targeted intervention. Predictability coefficients were calculated using the ‘mgm’ function in the R studio software (Haslbeck & Waldorp, 2018).
Results
Common Relations
The network of unique associations between MHL, demographic factors and attitudes regarding depression and schizophrenia can be found in Figure 1. The blue edges reflect significant positive relations between variables while the red edges signify negative relations. The strength of associations is shown by the thickness and depth of the colour of edges; a darker edge suggests a stronger correlation and vice versa (Hevey, 2018). Overall, we observed that attributing causes of depression and schizophrenia to spirituality was positively and uniquely linked to the endorsement of spiritual help for the hypothetical person in the vignettes. Endorsing psychosocial causes positively and distinctly related to personal stigma for both depression and schizophrenia. Religiosity was directly and independently associated with endorsing professional help for both depression and schizophrenia (see Supplement Table S1 for weight edges [relation strengths]).
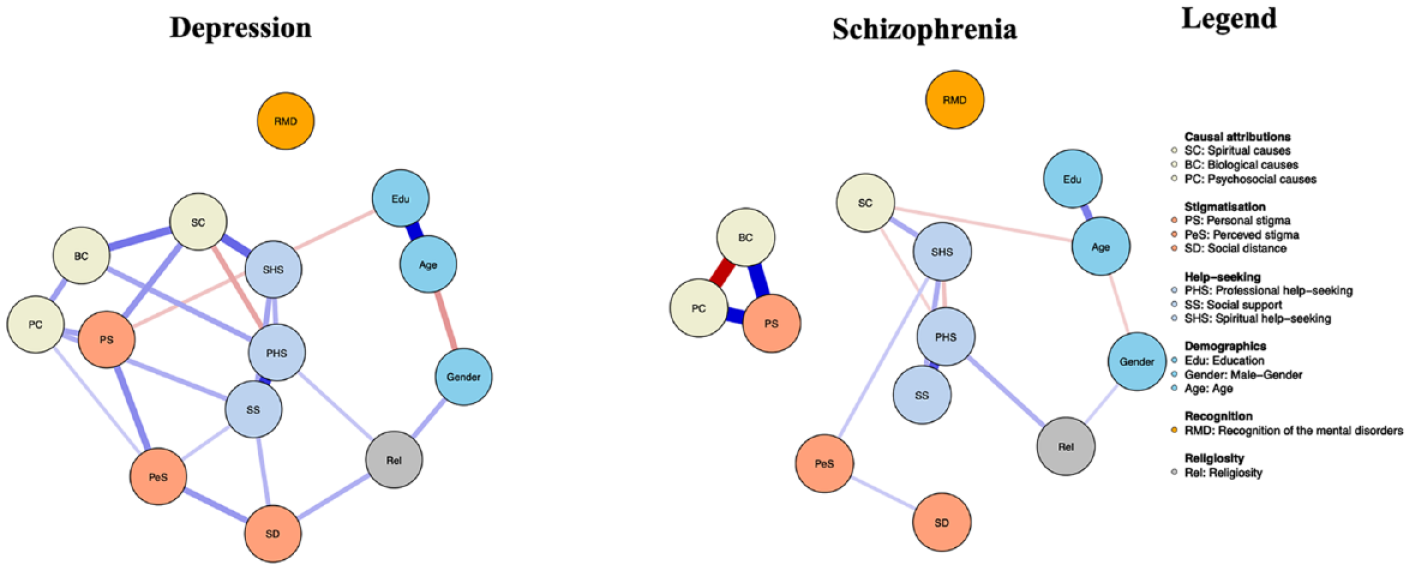
Bayesian Gaussian Graphical Models (BGGMs) of the networks of causal beliefs, help-seeking preferences, recognition ability, demographic factors, religiosity and stigmatization concerning depression and schizophrenia.
Differential Relation
Endorsing spiritual help-seeking for depression was directly and independently linked to personal stigma, and it displayed a negative relation with professional help-seeking for this disorder. Religiosity was distinctly positively linked to social distance for depression only. The endorsement of biological causes for depression increased with the endorsement of psychosocial causes and professional help-seeking for this disorder. Endorsing psychosocial causes of depression was independently and directly linked to preferences for social support and perceived stigma. Education protected against personal stigma towards depression (Figure 1; Supplement Table S1). However, for schizophrenia, the endorsement of psychosocial causes decreased with the endorsement of biological causes, and endorsing biological causes strongly and uniquely related with personal stigma towards schizophrenia. Preference for spiritual help-seeking deceased with the endorsement of professional help-seeking (Figure 1; Supplement Table S1).
Predictability Plot
Figure 2 illustrates the predictability plot, revealing that spiritual causal attribution related to depression had the most substantial impact in explaining variability among other nodes in the network. In the case of schizophrenia, personal stigma emerged as the most infliuential node contributing significantly to the variability observed across other nodes (Figure 2 and Supplement Table S2).
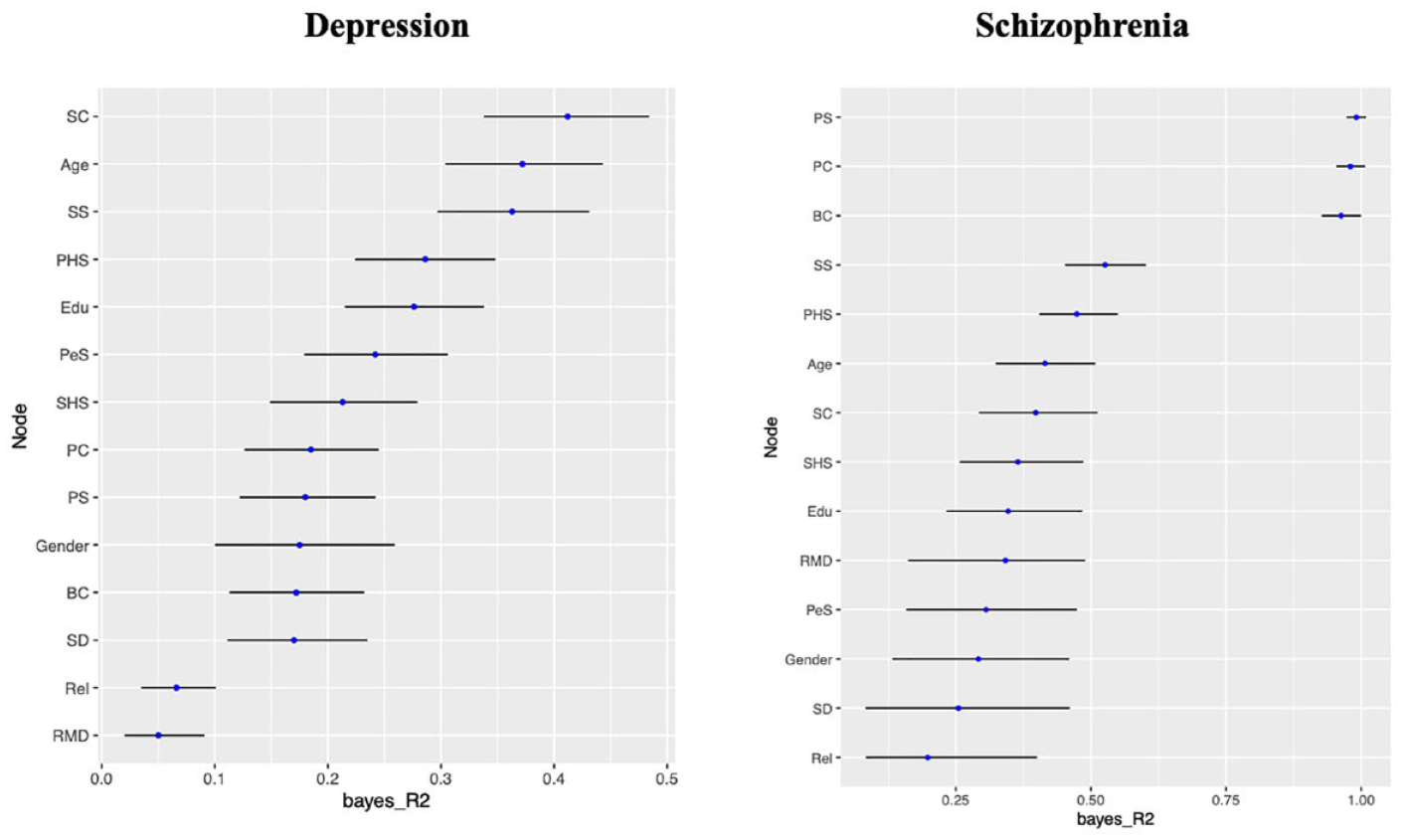
Bayesian Gaussian Graphical Models (BGGMs) of the predictability plot of causal beliefs, help-seeking preferences, recognition ability, demographic factors, religiosity and stigmatization concerning depression and schizophrenia.
Discussion
Our study examined the complex relations between MHL, regarding causal beliefs, help-seeking preferences, recognition ability, as well as demographic factors, religiosity and stigmatization regarding the Western perspective of depression and schizophrenia in Ghana. Findings indicated that spiritual causal attribution for depression and personal stigma towards schizophrenia were the most influential variables in the network. There was also a bidirectional link between help-seeking preferences and causal attributions across the two disorders. Religiosity was directly linked to endorsing professional help-seeking for the disorders. Moreover, there was a reciprocal link between personal stigma and psychosocial causal attributions across the mental disorders. Spiritual causal attributions were inversely related to professional help-seeking for both disorders. In sum, results showed complex relations among variables across the disorders.
The implications drawn from the predictability plot offer valuable insights into the complexities of mental health perceptions. In the context of depression, the considerable impact of spiritual causal attribution as the pivotal variable suggests that the variability in spiritual causal attribution was explained by its connection with other variables. In other words, this variable had the greatest impact on the overall structure, dynamics and outcomes of the network. This implies that individuals’ beliefs about the spiritual origin of depression are influential in shaping their attitudes and responses to the disorder. This highlights the potential effectiveness of interventions aimed at altering these casual beliefs to foster more positive responses and supportive behaviours towards depression. Such a finding was not surprising within the current context, since the literature has consistently reported that the majority of the population engages in spiritual causal attributions of mental disorders (Opare-Henaku, 2014; Salifu Yendork et al., 2018).
Conversely, for schizophrenia, personal stigma as the most influential factor means that individuals’ attitudes and biases significantly influence perceptions and interactions related to this disorder. This result was in line with previous literature, as personal stigma towards schizophrenia has been well documented in the literature. Possible reasons identified in this regard included societal misconceptions about the condition, fear of violent behaviours associated with schizophrenia, lack of understanding about mental health, negative media portrayals, and the influence of cultural beliefs (Gerlinger et al., 2013). Typically, it is common for many Ghanaians to label individuals with schizophrenia as being possessed by a ‘demon’, reflecting personal stigmatizing attitudes towards the condition. (Read & Doku, 2012). This finding underscores the importance of addressing and reducing personal stigma through targeted strategies, which could trigger broader positive changes in attitudes, interactions and support systems for individuals with schizophrenia. Prior research has reported that schizophrenia is highly stigmatized among African samples (Adu et al., 2021b; Broussard et al., 2012). In summary, addressing key influential factors, that is, spiritual causal attribution and personal stigma, can create a ripple positive effect throughout the network of attitudes and beliefs. In other words, our results indicated that better mental health campaigns may consider the most influential beliefs and attitudes regarding a particular mental disorder.
While previous studies have established that attitudes differ between depression and schizophrenia, with schizophrenia being more highly stigmatized than depression (Martensen et al., 2020), the current study offers a distinct perspective by identifying the most influential attitudes associated with these conditions. Unlike prior research that primarily focused on the comparative levels of attitudes, this study emphasized specific attitudes that significantly shape public perceptions regarding depression and schizophrenia. By identifying these influential factors, the study not only enhances our understanding of attitudinal dynamics but also provides actionable insights for designing targeted interventions. This focus allows stakeholders, such as mental health practitioners, to address the most impactful attitudes related to a particular type of mental disorder, ultimately fostering more effective strategies for reducing negative attitudes about mental disorders and promoting mental well-being.
Additionally, the absence of a detectable influence of religiosity on the endorsement of spiritual causal beliefs or preferences for seeking spiritual help in relation to the mental disorders in the present study implies that the link between spiritual causal attribution and spiritual help-seeking highlighted in the present study was independent of how religious the participants were. In order words, individuals’ specific beliefs about the causes of the mental disorders play a more significant role in shaping their help-seeking behaviours than their overall level of religiosity, contrasting with prior research (Opare-Henaku, 2014; Read & Doku, 2012). This suggests that the association between these factors could potentially be influenced by cultural norms and prevalent mental health beliefs. Consequently, it becomes evident that the impact of religious factors might not be universally applicable and definitive. This realization emphasizes the complex interplay of individual perceptions, beliefs and broader societal viewpoints. In essence, the dynamics at play are far more complex than a mere reliance on religious aspects and extend into a broader framework of personal, cultural and societal influences (Berry, 2022).
Another significant interconnection between the variables was the observation that endorsing psychosocial causes of depression was directly linked to preferences for social support. This means that the Western concept of mental health nosology related to causal attributions has the potential to positively influence the acceptance of the Western and secularized help-seeking preferences. While the Western approach to mental health has been criticized in recent times for being overly simplistic, lacking culturally specific relevance and predominately favouring the Western world (Henrich et al., 2010), the current evidence shows that such an approach in Ghana, a non-Western country, could partly be beneficial to better mental health outcomes. Such bidirectional relations between causal attributions and help-seeking preferences mean that the way individuals perceive the causes of their mental health issues influences the kind of help they seek, and the type of help they pursue can, in turn, shape or reinforce their beliefs about what caused the condition. Notably, although the recognition of mental disorders has been widely reported in the literature as contributing positively to better health outcomes, its influence in the current study was statistically not significant. Perhaps gathering additional data could help reach a threshold that allows for more robust inferences to be drawn in this regard. The ongoing syntheses of the current evidence underscore the significance of understanding cultural nuances and context when diagnosing and treating mental disorders (Jurcik et al., 2014). The evidence may support avenues that advocate potential benefits of integrating traditional faith-based approaches with Western methods within Ghana’s mental healthcare system (Gureje et al., 2020).
Strengths, Limitations and Future Research
The network links enhanced the comprehension of the complex interactions among MHL components, including causal beliefs, help-seeking preferences, recognition ability, as well as demographics, religiosity, and stigmatization related to depression and schizophrenia. This study pioneers the use of novel network analysis to explore these intricate relations, yielding insights into psychological attitudes and beliefs on depression and schizophrenia in Ghana. The power of network analysis revealed the dynamic predictive nature of variables within a single study, complementing review evidence (Read & Doku, 2012). Limitations of this study include: the sample employed does not fully represent the broader population of Ghana due to the use of a convenience sampling method, which could potentially lead to biased participant selection; potential bias arising from online surveys, favouring those with internet access and electronic devices (Wright, 2005). The adoption of a cross-sectional design precludes the establishment of causal links. Vignettes may be low in achieving ecological validity, and the utilization of self-report measures could introduce response bias, such as participants providing socially desirable answers (Grimm, 2010). Subsequent research should employ longitudinal and experimental designs to explore these variables using a more representative sample from Ghana, ultimately crafting practical and alternative effective interventions to tackle poor mental health outcomes within Ghana and other countries in the region. Future research could also aim to establish causal relations among these variables. It would be valuable to triangulate the current findings across diverse cultures and subgroups, utilizing different components of MHL and research methods, such as the sequential exploratory mixed-method approach (Ivankova et al., 2006). This approach could ethnographically explore the various components of MHL and their effects on mental well-being.
Conclusions
I modelled the complex links between causal beliefs, help-seeking preferences, recognition ability, demographics, religiosity, and stigmatization regarding depression and schizophrenia in Ghana using the novel network analysis. The results of the study showed that spiritual causal attribution had the most significant impact in the model for depression, while personal stigma had the strongest influence in the model for schizophrenia. Stigma was impacted by underlying causal beliefs regarding mental disorders. Results showed complex relations among variables across the disorders. Recognizing the unique cultural and societal elements surrounding depression and schizophrenia and addressing personal stigma specifically related to schizophrenia and causal attribution related to depression are essential for promoting better mental health among the sample. These findings provide valuable insights for future experimental research aimed at enhancing overall mental health and well-being.
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.