
Abstract
A large body of research on the “Healthy Immigrant Effect” (or “Paradox”) has reported an immigrant mortality advantage. However, other studies do not find such significant effects, and some even present contradictory evidence. This article is the first systematic meta-analysis that investigates the immigration-mortality relationship from a global perspective, examining 1,933 all-cause and cardiovascular mortality risk estimates from 103 publications. Our comprehensive analysis allows us to assess interactions between origin and destination regions and to reexamine, on a global scale, some of the most notable explanations for the immigrant mortality advantage, including suggestions that this paradox may be primarily the result of selection effects. We find evidence for the existence of a mild immigrant mortality advantage for working-age individuals. However, the relationship holds only for immigrants who moved between certain world regions, particularly those who immigrated from Northern Africa, Asia, and Southern Europe to richer countries. The results highlight the need in the broader migration literature for an increased focus on selection effects and on outcomes for people who chose not to migrate or who were denied entry into their planned destination country.
Introduction
Much of the debate on the relative health of immigrants (i.e., the “healthy immigrant paradox”) revolves around whether an immigrant health advantage exists (e.g., Palloni and Arias 2004). Most previous research has reported that immigrants are healthier and live longer than native-born residents in their destination country (Young 1986; Khlat and Darmon 2003; Anson 2004; Deboosere and Gadeyne 2005; Mackenbach et al. 2005; Nasseri 2008; Wallace and Kulu 2015; Gyamfi et al. 2017). Still, others have found no significant immigrant mortality advantage (Marmot, Adelstein, and Bulusu 1984; Nair et al. 1990; Balarajan 1996; Hedlund et al. 2008; Norredam et al. 2012) or even an immigrant mortality disadvantage (Uitenbroek and Verhoeff 2002; Regidor et al. 2008; Hermalin et al. 2009; Boulogne et al. 2012; Kaucher et al. 2017; Rodriguez et al. 2017).
In this article, we seek to advance discussion of the immigrant mortality advantage by balancing a global comparative perspective with a granular focus on immigrants’ origins and destinations. We conducted a large global-scale meta-analysis in which we aimed to include any study of international migration that compared immigrants’ mortality rates to those of the native-born population in their destination country. The large body of studies synthesized here allows us to examine overall mortality differences between immigrants and local populations, as well as the effects of gender, age, and study period on these differences. In addition, we can assess regional differences, comparing relative mortality for immigrants from all continents to immigrants in other continents and sub-continental regions. These global comparisons, in turn, provide insights and allow for careful reflections on some of the more prominent theoretical explanations offered for the healthy immigrant paradox. As our analysis shows, the immigrant mortality advantage is probably smaller than previously reported, is highly variable depending on context, and is largely due to selection processes.
We begin this article by summarizing existing reviews of the literature on immigrant mortality. We then review the effect of origin, destination, pre- and post-migration experiences, and selection processes on immigrant mortality. Next, we outline our unique contributions beyond those made by a recent systematic review and meta-analysis by Aldridge et al. (2018), before presenting our methods and outlining the advantages and disadvantages of our regional analytical approach. From there, we present our results, showing the existence of a small immigrant mortality advantage. We conclude by arguing that much of the observed immigrant mortality advantage can be explained by selection processes.
What Explains the Immigrant Mortality Advantage?
While empirical studies in multiple disciplines have frequently observed an immigrant mortality advantage (as we outlined in the introduction), questions remain regarding the possible mechanisms underlying this phenomenon. Migration scholars have suggested that immigrants’ experiences and outcomes are often shaped by both macro-level conditions, such as the properties of their origin and destination countries and the interaction between these properties (McKay, Macintyre, and Ellaway 2003; Aldridge et al. 2018), and individual-level characteristics, such as gender, age, and race (van Tubergen and Kalmijn 2005; Levels and Dronkers 2008). In previous work (Shor, Roelfs, and Vang 2017), we focused on demographic explanations for this advantage, such as gender- and age-related effects. Here, we shift our focus to geographic-related effects, as the current analysis allows us to examine variations in immigrant mortality by both origin and destination region. In particular, van Tubergen and Kalmijn (2005) have suggested that in studying various features of immigrants, we must consider three groups of contextual effects: “origin effects” (the origin country’s characteristics), “destination effects” (the destination country’s characteristics), and “setting effects” (the combination of origin and destination characteristics). Below, we expand on the potential theoretical relevance of focusing on both origin and destination effects and review the literature on pre- and post-migration health processes and selection effects, to which we return in our conclusion.
Origin effects
Honkaniemi et al. (2017) have suggested that immigrants’ health depends, to some degree, on the nation from which they emigrated. Klinthall and Lindstrom (2011) further argue that migrants from relatively less-developed countries grew up in environments with greater health risks, including exposure to pollution, lower quality of healthcare, and less access to preventive care early in life, potentially putting them at a disadvantage compared with migrants who grew up in more affluent countries. Earlier life experiences, including exposure to health risks and the quality of health care received, can affect health trajectories over the life course (Bengtsson and Mineau 2009). According to this logic, we may expect immigrants from more affluent sub-regions, such as Northern America, Australia and New Zealand, and Northern and Western Europe, to be healthier and to live longer than immigrants from poorer regions, such as much of Africa and Asia.
Racial or ethnic minority status may also affect post-migration health by playing a role in individuals’ ability to integrate in a new country (Galabuzi 2006). Racialized groups in any destination county often suffer from worse access to healthcare services, have more unmet needs, and are more likely to resist important health-maintenance practices (Fiscella et al. 2002; Napoles et al. 2005). For example, immigrant women from visible minority groups in Canada, the United Kingdom, and the United States are less likely to participate in cancer screenings, leading to delayed diagnoses and more adverse outcomes (Ahmad, Cameron, and Stewart 2005; Asanin and Wilson 2008; Amankwah, Ngwakongnwi, and Quan 2009; Ahmad et al. 2011; Crawford et al. 2016). Racism may also play a part in immigrants’ health, either directly, by increasing physiological stress responses (Brondolo et al. 2003; Williams, Neighbors, and Jackson 2003; Harris et al. 2006), or indirectly, by decreasing economic, housing, and employment opportunities and introducing barriers to healthcare utilization (Hyman 2004; Galabuzi 2006).
While early-life conditions and race/ethnicity may affect health during the life course, we must also consider the possibility of immigrant selection (both self-selection and selection by receiving countries) as a factor that might influence comparisons of longevity in the opposite direction. First, in some instances (e.g., immigration from India to the United States), high socioeconomic-status individuals in poorer regions may be better able to attempt migration because they have the means to pay for travel, to obtain sufficient education, and to acquire some command of the destination country’s language (if they do not already have a command of it). High socioeconomic-status individuals, however, are also more likely to be able to avoid some of the deleterious effects of poor conditions in their origin country by, for example, enjoying greater access to clean water, less exposure to common diseases, and the ability to at least partially mitigate stressors such as exposure to a violent environment. Having low exposure to health risks early in life helps establish more positive health trajectories over the life course (Bengtsson and Mineau 2009).
Destination effects
Immigrants’ health may also depend on the policies of the nation to which they emigrated. Immigrants who are not well-integrated into their destination country often have worse access to health care services (Ahmad, Cameron, and Stewart 2005; Crawford et al. 2016), which may partly stem from differences in policies toward immigration in receiving countries (Martinez et al. 2015). Migrant integration policies include both the degree of legal inclusiveness toward individual immigrants and the accommodation of cultural group differences (Koopmans et al. 2005). Both factors vary considerably among receiving countries and may affect immigrants’ ability to acclimate, as well as their willingness to utilize healthcare services (Ahmad, Cameron, and Stewart 2005; Crawford et al. 2016). Research has suggested that immigrants experience less stress and alienation if their host country is more welcoming to migrants (Wong, Yoo, and Stewart 2007). In addition, countries with healthcare systems that are more affordable and easier to access may provide disadvantaged populations, such as women and ethnic minorities, with relatively better care (Huddleston et al. 2015) and health outcomes (Cooper, Smaje, and Arber 1998; Stirbu et al. 2006). Taken together, we can expect better immigrant health outcomes in destination countries that provide better health support for the entire population and directly facilitate immigrants’ integration into the health system.
Pre- and post-migration health processes
Some explanations for the immigrant mortality advantage have focused on the importance of behavioral habits, diet, and nutrition (McDonald and Kennedy 2005). For example, previous research has suggested that tobacco, alcohol, and drug use rates are lower for many immigrant groups than for the native born and that immigrants’ diets and lifestyles are also healthier (Gordon-Larsen et al. 2003; Toilbert Kimbro 2009). However, other studies report a positive relationship between immigrants’ duration of residence in their new country and factors associated with poor health, such as obesity and higher body mass index (Antecol and Bedard 2006; Redstone Akresh 2007; Kaushal 2008; Oza-Frank and Cunnigham 2009; Peralta da Costa, Ferreira Dias and do Rosario Oliveira Martins 2017). Such findings suggest that healthier behaviors are likely to be observed primarily among the most recent immigrants rather than among those who have had time to assimilate.
Selection effects
Another significant body of work has investigated whether these observed immigrant mortality differentials reflect actual health processes or, instead, result from selection processes and data artifacts (Wallace and Kulu 2014). Better pre-migration health (relative to those in the origin country who are not immigrating; see Sorlie et al. 1993; Palloni and Arias 2004) and return migration following the onset of serious health conditions (also known as the “Salmon Bias”; see Abraido-Lanza et al. 1999) have been suggested as factors that can create a downward bias in observed immigrant mortality rates.
Selection can occur at both the country level and the individual level (Vang et al. 2017). Prospective immigrants who have better job market skills (e.g., higher education levels or language fluency) are more likely to be admitted into a country (and more likely to have above-average health because of higher income and/or a better ability to navigate the health care system; see Chiswick, Lee, and Miller 2008). In addition, many receiving countries select prospective immigrants directly based on their health (Gushulak 2007). At the individual level, healthier people in an origin country are better able to attempt migration (Palloni and Arias 2004), while immigrants who become ill may be more likely to return to their origin country (Abraido-Lanza et al. 1999). Both of these tendencies have the potential to artificially lower the observed immigrant mortality rate in the destination country. Whether selection occurs at the country or the individual level, its effect is similar: immigrants’ average health level appears higher than it would be in the absence of selection.
Unique Contributions of the Current Study
Several systematic reviews on immigration and mortality have been published in the last two decades. A review by McKay, Macintyre, and Ellaway (2003) examined studies of all-cause, cardiovascular, cancer, mental health, and physical health among migrants but did not attempt to draw broad conclusions about immigrant health relative to other populations. Vang et al. (2017) conducted a systematic review (of seventy-eight studies) of immigrants’ health in Canada and noted a general healthy immigrant effect, especially with respect to mortality from all causes combined (all-cause mortality) and among working-age adults. Another systematic review (of 43 studies) of immigrants to Scandinavian countries by Honkaniemi et al. (2017) suggested an immigrant all-cause mortality advantage for people from Southern Europe and the Middle East but also some excess risk for immigrants from other Nordic countries.
Meta-analyses have also been published on immigration and mortality over the last five years. A meta-analysis (of fifty-eight studies) in the United States found a 17.5 percent lower risk of mortality among Hispanics compared to other ethnic groups (Ruiz, Steffen, and Smith 2013). A later meta-analysis (of 28 studies) specifically focusing on immigrants from Latin America and the Caribbean to developed nations (Shor, Roelfs, and Vang 2017) showed modest immigrant advantages with respect to both all-cause and cardiovascular mortality that, like Vang et al. (2017), were strongest among working-age adults. Another meta-analysis (of eight studies) by Jin et al. (2015) found a cardiovascular mortality advantage among Chinese immigrants to Western nations. More recently, the first global systematic review and meta-analysis (of 96 studies), by Aldridge et al. (2018), examined immigrants’ relative mortality rates by cause of death, sex, and other factors, reporting a 25 percent to 30 percent all-cause immigrant mortality advantage (based on 16 studies) that was statistically significant for both men and women.
Collectively, these reviews make important contributions to the literature on immigrant health. However, they do not resolve the academic debate over the immigrant mortality advantage because they all employed relatively narrow selection criteria. Ruiz, Steffen, and Smith (2013) focused on Hispanic ethnicity, which combines immigrants from Hispanic countries with native-born persons with Hispanic backgrounds. The meta-analysis by Shor, Roelfs, and Vang (2017), while examining only immigrants, was limited in scope to immigrants from Latin America and the Caribbean. Similarly, Jin et al. (2015) only examined immigrants from China.
Aldridge et al. (2018) offered an analysis that comes closest in scope to our own, as it is the first comprehensive examination of immigrants’ mortality by multiple causes of death. Our own study differs from that of Aldridge et al., however, in three important ways. First, following Roelfs et al. (2013), we use a keyword search only as a starting point, complementing this approach with other iterative search strategies. As we note in greater detail in the methods section (and Online Appendix), this different search technique allowed us to locate and analyze almost twice the number of studies included in the Aldridge et al. analysis. Second, we chose to include studies that reported different metrics, such as standardized mortality rates (SMRs), rate ratios, odds ratios (logistic regression), and hazard ratios (proportional hazards regression), while Aldridge et al. included in their meta-analysis only studies that reported SMRs or mortality rate ratios. Third, we included all available studies published since the 1960s, while Aldridge et al. did not include studies published prior to 2001.
In sum, these differences in search strategy and study design allow us to offer a number of important contributions to the literature on the immigrant mortality advantage. Our wider inclusion criteria produced a larger number of studies for analysis, covering several decades and allowing us to detect potential time trends in the immigration-mortality association. Our data collection strategy also aimed to obtain multiple effect estimates from each study to enable subgroup analyses by origin, destination, sex, and age. Most notably, our article’s large scope allows us to examine systematically the interaction between origin and destination regions. Finally, our approach allows the reassessment of some explanations for the reported immigrant mortality advantage, including the potential role of selection processes.
Data and Methods
Search Strategy and Inclusion Criteria
The data and methods used in this article closely resemble those used in our previous meta-analysis on immigrant mortality (Shor, Roelfs, and Vang 2017). We used an iterative literature search process, beginning with a keyword search, as described in our previous work (Roelfs et al. 2010, 2011, 2015; Hogans et al. 2017). The full search algorithm used for Medline is shown in the Online Appendix, with the most relevant portions bolded. All unpublished work encountered during the search process was considered for study inclusion. Although our search was done in English, we were able to locate and translate the relevant portions of one article written in Dutch and one dissertation written in Spanish. We completed the literature search in June 2020. At the end of the search process, we identified 444 candidate publications (see Figure 1).
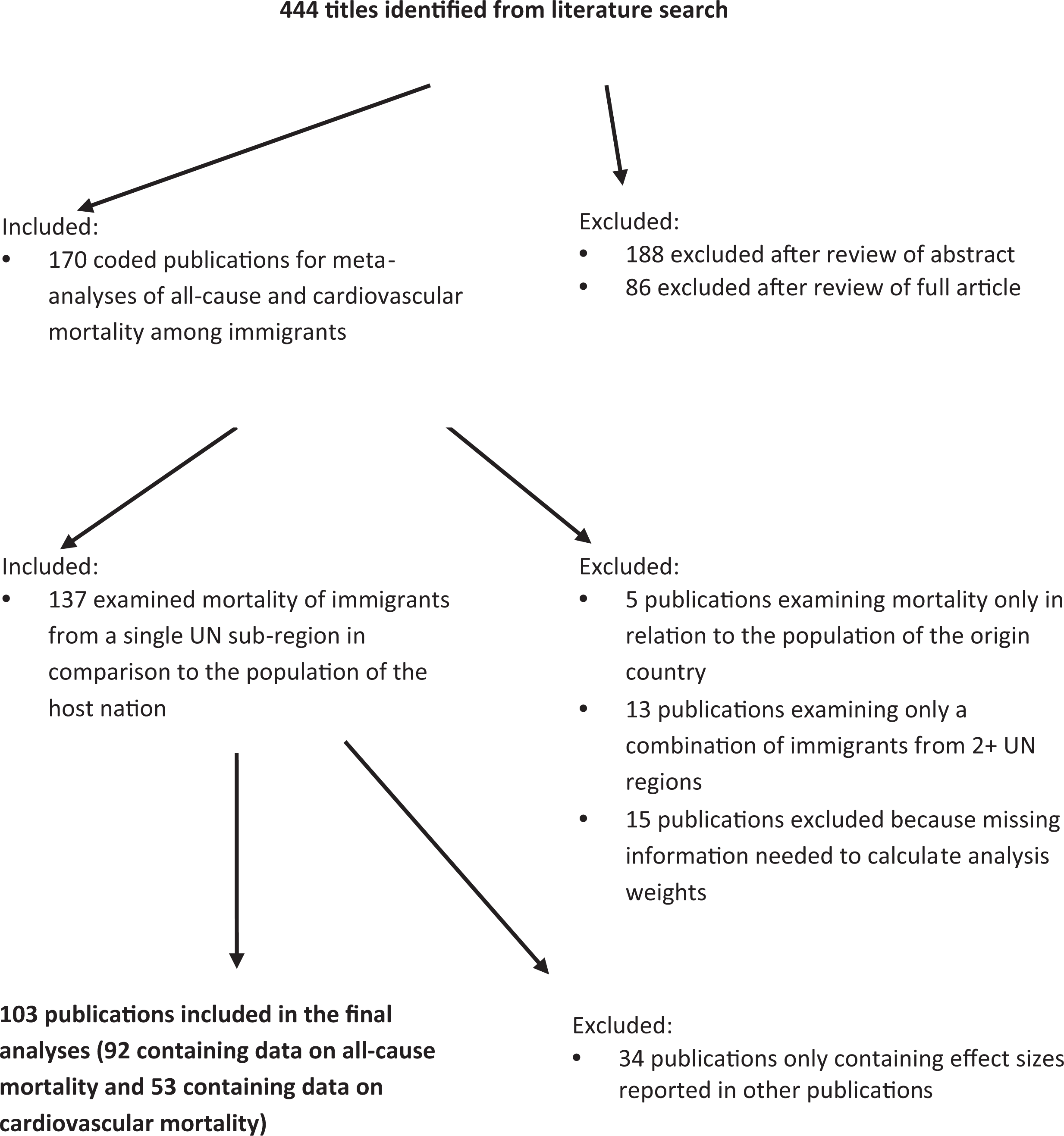
Search strategy and yield.
We jointly determined publication eligibility. Of the 444 candidate publications, 170 were deemed relevant to a meta-analysis of all-cause or cardiovascular mortality among immigrants. We fully coded these 170 articles (see Online Appendix for a list of the types of variables coded) and further examined each article to determine final eligibility for inclusion (see again Figure 1). When a given study reported results in multiple ways or when two or more studies reported results from the same population-years, we sought to maximize our ability to conduct subgroup analyses. For example, if results were available broken down by gender alone, by age alone, and by gender and age together, we always chose the set of effect estimates showing both gender and age variation. In addition, whenever possible, we used results from a multitivariate model, rather than one without statistical controls.
We judged 103 publications as eligible for inclusion in the current study. A publication was included if it (1) clearly compared a group of immigrants from a given country within a single UN-defined region or sub-region (UN Statistics Division 2020) to a control group in the destination country; (2) reported an effect size in the form of a rate ratio (or provided information sufficient to convert the results to rate ratio format); (3) had all-cause mortality or cardiovascular mortality as the outcome of interest; (4) reported information needed to calculate meta-analysis weights; and (5) reported effect estimates not already reported by another study. The 103 publications in the final dataset provided a total of 1,933 risk estimates, 1,306 of which (from 92 studies) were all-cause mortality risk estimates and 627 (from 53 studies) were cardiovascular mortality risk estimates.
In the present analysis, as mentioned above, we sought to isolate UN-defined regions and sub-regions of origin. In Table A1 in the Online Appendix, we provide a full listing and brief description of the studies included in our analysis. As the table shows, the present analysis covers a substantial portion of the globe in terms of origin regions and a substantial portion of developed nations in terms of destinations (data on immigrants to developing nations were much more sparse). The full dataset used in the analyses and codebook to the data are available in the Online Appendix.
Statistical Methods
We use a series of random-effects meta-analyses, weighted by the inverse of the effect estimate’s variance, to examine immigrants’ mortality relative to destination country populations. We produced estimates for all-cause and cardiovascular mortality across all origin regions and sub-regions, disaggregated by sex, age, and study baseline. We disaggregate by sex because previous research has suggested that the migration process differs by gender, including pre-migration risks and reasons for migration (Llacer et al. 2007), migration experiences (Farley et al. 2004; Zimmerman, Kiss, and Hossain 2011), and post-migration risks and integration trajectories (Gorman, Ghazal Read, and Krueger 2010). We disaggregate by age because the underlying conditions and experiences for children and adolescents who immigrate to a new country may be different from those of adults (Shor, Roelfs, and Vang 2017; Vang et al. 2017; Shor and Roelfs 2019). We disaggregate by study baseline year to account for the possibility that immigrant experiences have changed over time.
We focus here on pre-defined origin and destination geographical regions and sub-regions. On the one hand, the use of pre-defined regions/sub-regions excludes some studies or parts of studies from the analysis, such as those that aggregated immigration from multiple continents. For example, if a study reported statistical results for the Middle East including Northern Africa (as some did), we could not include the reported result in our analyses of either Northern Africa or Western Asia. This limitation results in a lower number of studies and effect estimates. However, it is important to note that our dataset remains robust even after excluding studies that reported on immigration from multiple continents together. Sensitivity analyses did not show an effect for including these studies on the overall results of the meta-analysis. In addition, we believe that the exclusion of multi-continent origins was justified, as it allowed us to maintain the separation between different world areas (which was part of the large majority of studies included in our analysis).
On the other hand, the decision to focus on regions and sub-regions, rather than on individual countries, entails the loss of finer details and of the ability to distinguish between immigration waves from unique countries when these waves were reported in the original studies. For example, some characteristic of immigrants coming from China may be quite different from those of immigrants originating from Japan, although both countries are located in East Asia. Nonetheless, a focus on origin countries would have meant excluding a relatively large number of studies from our analysis. Indeed, our preliminary review of the coded data suggested that sub-regions were commonly reported in many studies, instead of separating findings by specific origin countries. In addition, an attempt to report the results by individual origin countries would have produced many instances where results would have been based on a single study (which is not suitable for a meta-analysis) and a cumbersome presentation of the results, making reading and interpretation harder.
Finally, and related to the preceding limitation, the aggregation of specific destination countries into UN sub-regions has the potential to hide factors specific to any given nation. However, presenting results for all 23 unique destinations (countries) would have resulted in small sample sizes, as many specific origin-destination country pairings were examined by only one study. Still, we conducted additional analyses (not reported here) showing that splitting the analyses by destination country did not produce results that contradicted those reported in Table 1. To be sure, there is some heterogeneity between destination countries within a region, but this heterogeneity is more in terms of the association’s strength than direction.
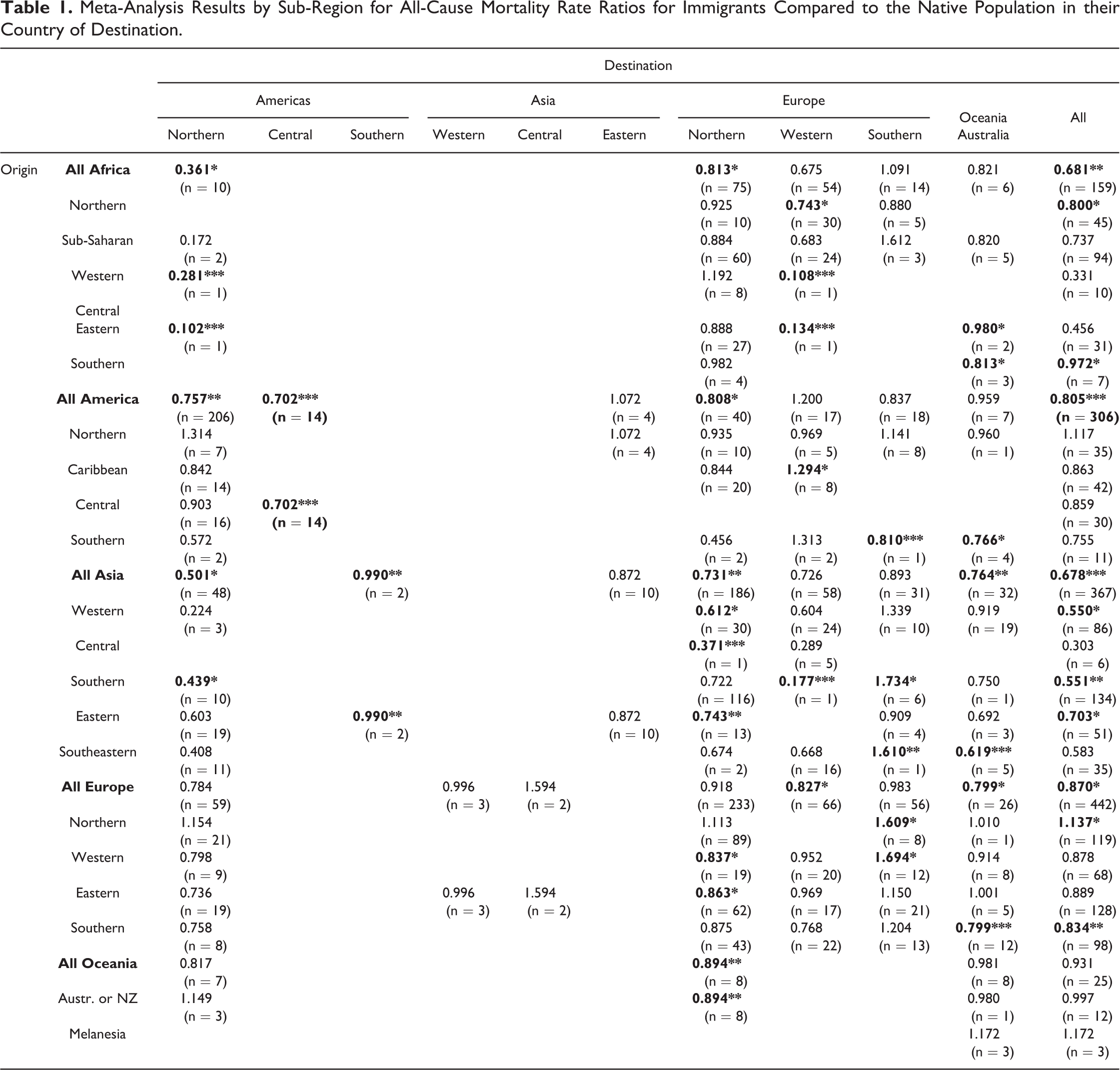
Meta-Analysis Results by Sub-Region for All-Cause Mortality Rate Ratios for Immigrants Compared to the Native Population in their Country of Destination.
All meta-analyses were performed in Stata 15.1, using the robumeta (Robust Meta-Analysis) package. Robust meta-analysis controls for correlations between risk estimates taken from within the same study (which occurs when a study reports multiple results by sub-groups). We used an assumed intra-study correlation of 0.8 for all analyses (as recommended by Tanner-Smith and Tipton 2013); robustness checks using alternative values for the intra-study correlation produced results identical to three digits past the decimal point. As explained in our previous work (Shor, Roelfs, and Vang 2017), we converted all point estimates into rate ratios and obtained the standard error for each effect estimate (when not directly reported) from other tests of statistical significance.
Findings
In Table 2, we present meta-analysis results for both all-cause and cardiovascular mortality. The results show immigrants’ mortality rates relative to those of the population in their destination country (most frequently, the native-born population). Overall, we found that immigrants had an 18.7 percent all-cause (RR = 0.813) mortality advantage. To explore heterogeneity within these results, we disaggregated the data by gender, age, and study baseline year. The subgroup analyses showed a mixture of non-significant results and results showing an immigrant mortality advantage. For all-cause mortality, the mortality advantage was equally evident for both men and women, was particularly salient among immigrants of working age (ages 30 to 60), and was stronger among studies using more recent data and methods (1990s+). The results showed a modest and non-significant cardiovascular mortality advantage for immigrants (RR = 0.906). This tendency toward non-significant cardiovascular mortality advantages was also evident when analyses were disaggregated by gender, age, and year.
Meta-Analysis Results for All-Cause and Cardiovascular Mortality Rate Ratios for Immigrants Compared to the Native Population in their Country of Destination.
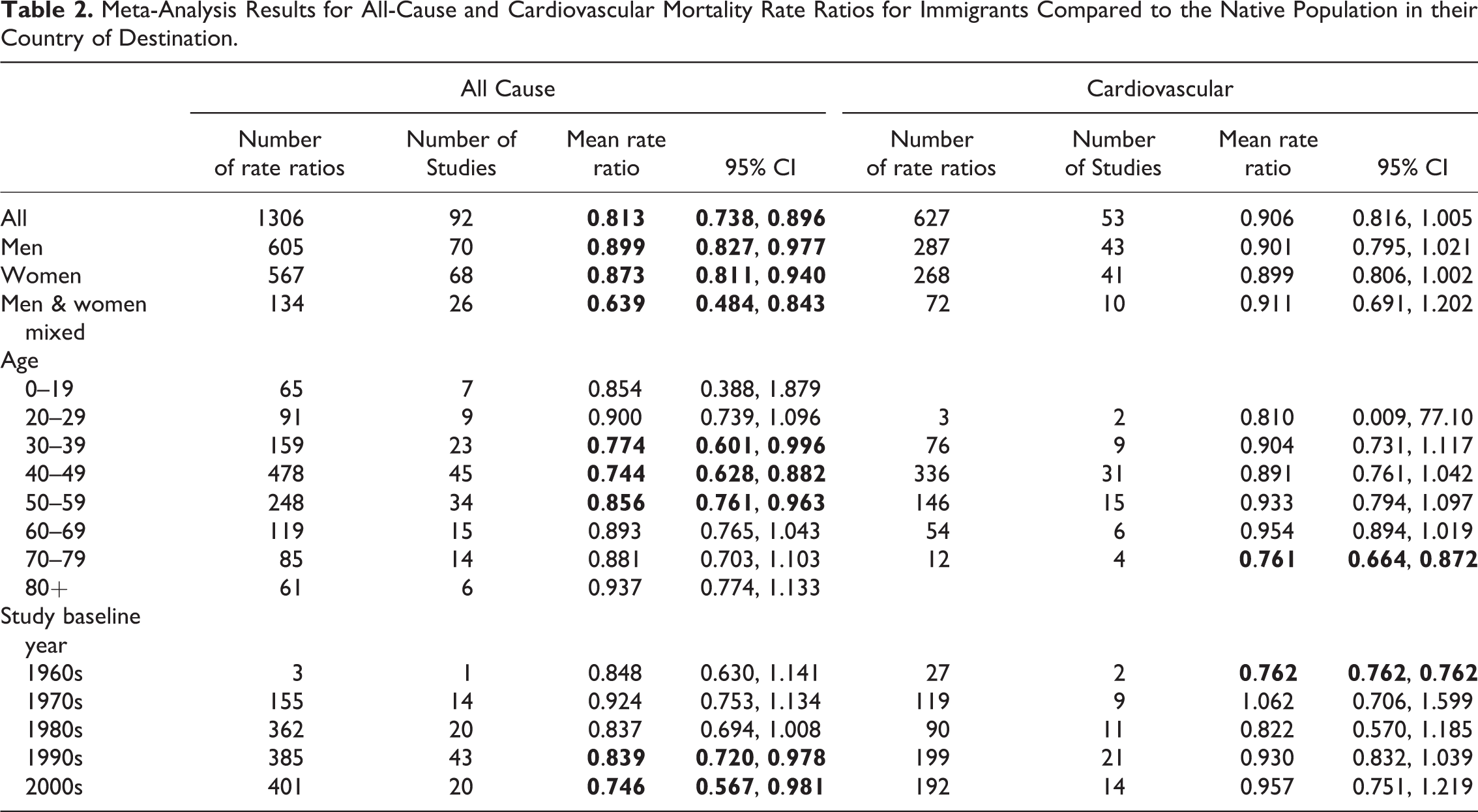
Table 1 presents the number of effect estimates and meta-analysis results by each combination of origin region/sub-region and destination sub-region for all-cause mortality (see Table A2 and Figures A1 and A2 in the Online Appendix for the corresponding analyses for cardiovascular mortality). Here, we find a few instances of immigrant all-cause mortality disadvantage. Such instances of a disadvantage were found for immigrants who moved from the Caribbean to Western Europe, for many who moved to Southern Europe from Asia or elsewhere in Europe, and for any immigrant from Northern Europe.
However, most combinations of origin and destination sub-regions showed either an all-cause mortality advantage or a non-significant relationship (see Table 2). Figure 2 shows that the largest significant mortality advantages (larger than a 20 percent advantage) were for immigrants from non-Western regions who moved to the West. These immigrants included people moving to Northern America from elsewhere in the Americas (almost all from Latin America and the Caribbean) who had a mortality advantage of 24.3 percent. Immigrants who moved to Northern America from Asia also showed a substantial mortality advantage (49.9 percent). Immigrants from Asia, too, had a substantial mortality advantage when moving to Northern Europe (26.9 percent) or to Oceania (23.6 percent). When considering immigration to all destinations combined, the strongest mortality advantages were for immigrants coming from Africa (31.9 percent) or from Asia (32.2 percent).
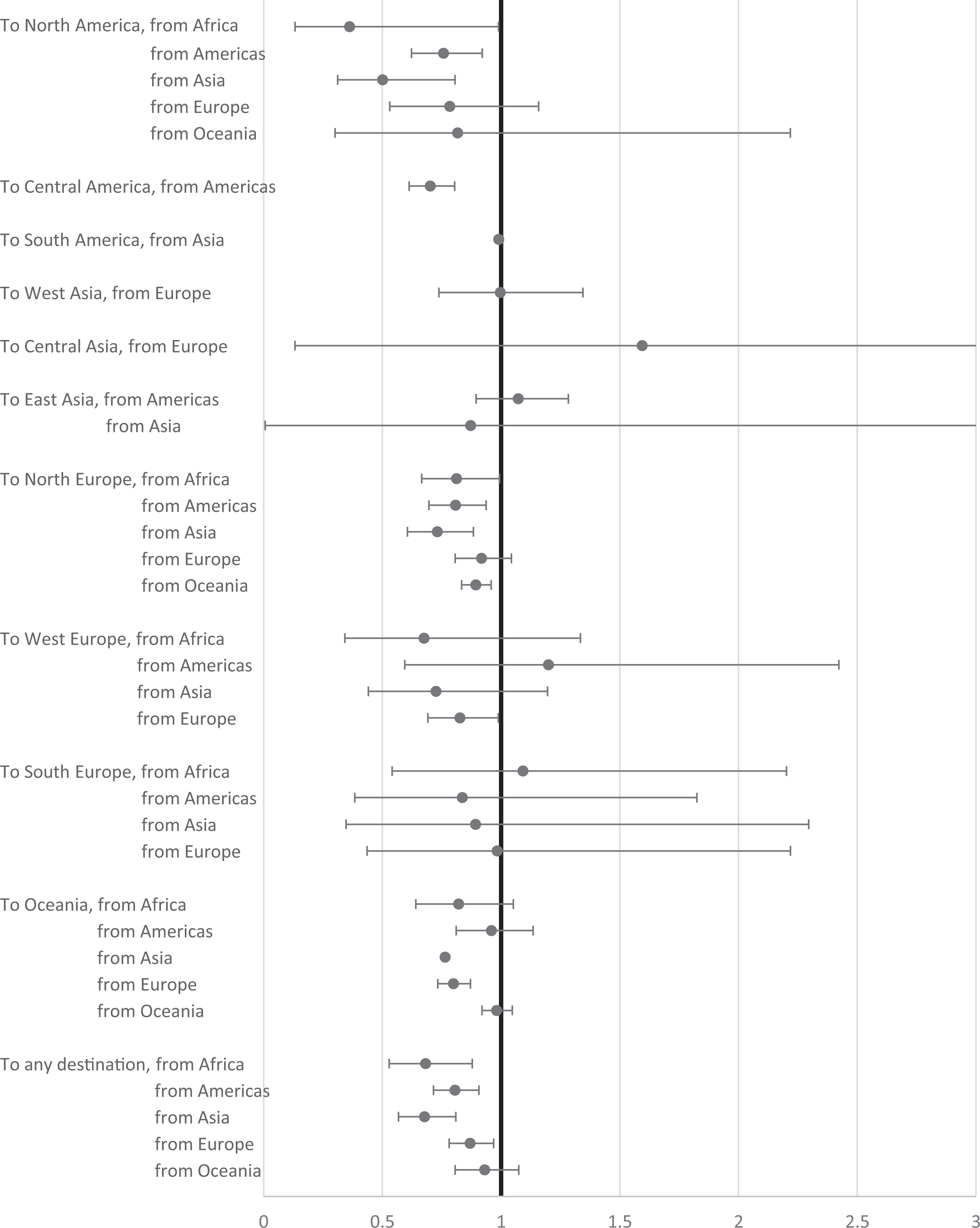
All-cause mortality meta-analysis results by destination sub-region and origin region.
Figure 3 offers a closer look at immigration origins, using the subset of data where immigrants come from single UN sub-regions (moving to any destination). These results supplement those of Figure 2, although they sometimes appear to diverge. For example, Figure 2 shows a mortality advantage of 31.9 percent for immigrants from Africa, while Figure 3 shows only mortality advantages of 20 percent and 2.8 percent for Northern and Southern Africa, respectively. The reason for such discrepancies is that Figure 3 unavoidably excludes a large portion of the data reported in Figure 2 (those data derived from entire continents). Still, Figure 3 shows particularly large mortality advantages for immigrants coming from Western (45.0 percent), Southern (44.9 percent), and Eastern Asia (29.7 percent). Immigrants from Northern Africa (20 percent) and from Southern Europe (16.6 percent) also showed notable mortality advantages. Overall, however, large immigrant mortality advantages were infrequently observed in our results.
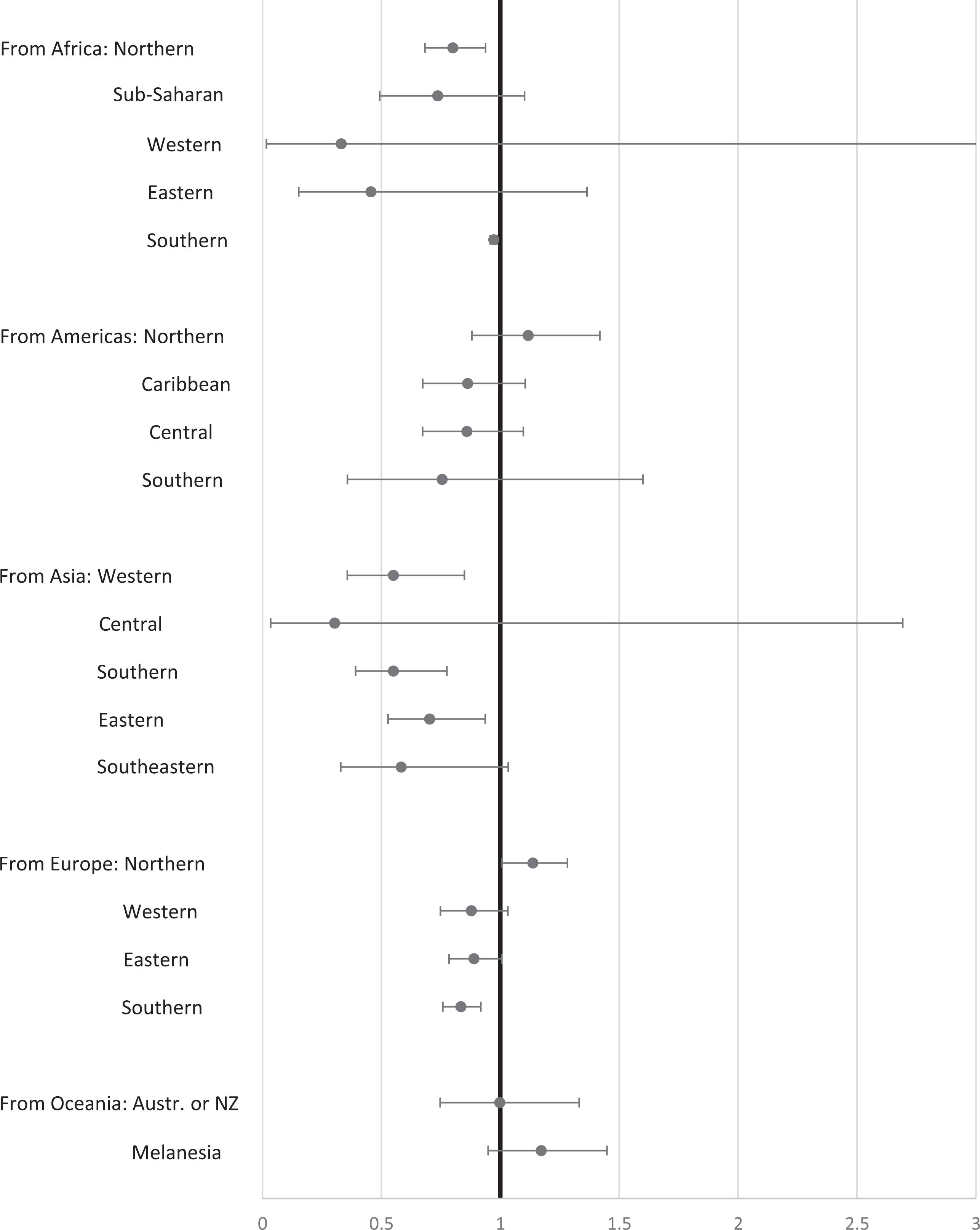
All-cause mortality meta-analysis results by origin sub-region (to all destinations).
Discussion
We conducted a systematic meta-analysis examining the immigration-mortality relationship from a global perspective, with a focus on the interaction between origin and destination regions. Our findings provide some support for the existence of a general migrant mortality advantage, though the strength of this advantage varies. The advantage is statistically significant for all-cause mortality, for both men and women, and for working-age individuals (between the ages of 30 and 60). This advantage holds most strongly for immigrants who moved from non-Western regions to the West, particularly those who immigrated from Africa or Asia. Most immigrants who moved between two richer nations did not enjoy a mortality advantage, and some even had a mortality disadvantage.
We found an overall all-cause immigrant mortality advantage of about 18.7 percent, a substantially smaller mortality advantage than the 30 percent advantage recently reported by another global meta-analysis (Aldridge et al. 2018). This difference might partly result from the fact that our meta-analysis covered a longer publication-period (1970–2020) than did Aldridge et al., who looked only at studies published between 2001 and 2017. Indeed, early publications reported a slightly lower mortality advantage on average. However, the main reason for this difference is that we were able to include a substantially larger number of studies reporting all-cause results in our analyses. While Aldridge et al. summarized the results of 16 studies reporting all-cause mortality, our own analysis relied on the results of 92 such studies, the majority of which (78) were published in 2001 or later. Our ability to include a substantially larger number of studies in our analysis is due to 1) also including studies that used logistic or proportional hazards regression and 2) using a search strategy less reliant on only keywords.
The larger number of studies in our analysis also meant that we located a much larger number of studies reporting on immigration from richer nations (Australia, as well as countries in Northern America and Northern and Western Europe). As we note above, such immigration was likely to show no immigrant mortality advantage or in some cases even a mortality disadvantage. As such, these studies on immigration from richer nations likely account for the lower all-cause mortality advantage we report here, compared with that reported by Aldridge et al. (2018).
Even considering these lower estimates of the immigrant mortality advantage, we caution that at least some of the advantage we document might stem from the well-known tendency of scholars and academic outlets to avoid reporting or publishing non-significant findings, often referred to as publication bias or “the file drawer effect” (Rosenthal 1991; Egger and Davey-Smith 1998; Berman and Parker 2002). This tendency can lead to over- or under-estimations of mean effect sizes in meta-analytic research. In the context of immigrant mortality studies, one might reasonably expect more studies showing either a null results or a migrant mortality disadvantage to remain unpublished. Indeed, we conducted Eggers tests, which showed the presence of potential publication bias, and funnel plots (see Figures A3 and A4 in the Online Appendix) confirmed the presence of such publication bias. Both funnel plots suggest that rate ratios greater than one (which would indicate instances of immigrant mortality disadvantage) were missing from both the all-cause and cardiovascular data, supporting the conclusion that the immigrant mortality advantage is likely even smaller than what we found in our analyses.
Our findings also suggest a u-shaped association with age, where the immigrant mortality advantage is only significant for older working-age immigrants (ages 30 to 60). The coefficients were closer to 1.00 and not statistically significant for both younger and older immigrants. These findings emphasize that the “healthy immigrant effect” may be limited to working-age immigrants. Those who immigrate before the age of 30 or after the age of retirement no longer enjoy mortality advantages, perhaps because they are not subjected to the same selection processes as are working-age individuals.
Our results seem to support selection explanations for the immigrant mortality advantage in two main ways. First, immigrants coming from the Caribbean to Western Europe actually had a higher mortality rate when compared with the native-born population. This finding is unlikely to be explained by racial discrimination, as immigrants from most of Africa and from Southern Asia mostly showed a mortality advantage. A more plausible explanation seems to be state selection. African immigrants to the West are likely to go through careful selection processes in which their pre-existing health, socio-economic status, education, and professional training play a significant role (Flahaux and De Haas 2016). Immigrants from Caribbean countries going to Europe, on the other hand, were often those who moved from French or Dutch colonies (Vezzoli and Flahaux 2016). Because having colonial status includes greater rights to migration (Vezzoli and Flahaux 2016), state-selection processes have less relevance.
Second, those moving within Northern America (from Canada to the United States and vice versa) or within Western Europe did not exhibit a mortality advantage over native-born populations, despite enjoying some advantages that may make immigrants’ lives easier (such as greater wealth, greater cultural affinity and familiarity, and a likely command of the local language or of a similar language). Both state selection and self-selection may again provide an explanation for this lack of relative advantage. It is easier to emigrate from Canada to the United States or from Denmark to Sweden than it is to come to one of these countries from Southern Asia or from Africa, both because of the travel involved in moving from such remote locations and because the countries themselves are likely to be less selective when accepting immigrants from their culturally similar neighbors (Ellermann and Goenaga 2019). Thus, it is more likely that immigrants from Western countries who do not enjoy good pre-existing health or possess unique professional skills will choose (and be allowed) to emigrate.
However, alongside this apparent support for selection explanations for immigrant mortality differentials, our findings also offer some potential support for explanations that focus on nutrition and a healthier lifestyle (Gordon-Larsen et al. 2003; Perez-Escamilla and Putnik 2007). Most notably, immigrants from most of Asia and from Latin America and the Caribbean to Northern America were among those who exhibited a substantial mortality advantage when compared to non-immigrant Northern Americans. While some of this effect may again be attributed to selective immigration patterns, scholars have previously suggested that in these regions, nutritional habits tend to be healthier, while drug and alcohol consumption, as well as tobacco smoking, tend to be relatively lower (Zaidi, Patel, and Bhopal 2003). Conversely, Northern Americans who have immigrated to Northern Europe exhibited a mortality disadvantage, perhaps due to bringing with them worse nutritional and exercising habits when compared to the native-born population.
Our results do not provide consistent support for explanations that focus on origin-country effects. First, most of the significant immigrant mortality advantages were for immigrants from poorer global regions and sub-regions, such as Africa and Asia. State-selection and self-selection effects can account for these findings. However, explanations that focus only on racial and ethnic minority status cannot account for our results. Those emigrating from regions where they were likely to be a visible racial/ethnic minority in their new country (e.g., most of Africa, Central America, and Asia) actually mostly had higher longevity rather than the lower longevity one would expect because of racial/ethnic disparities in health care access (Fiscella et al. 2002; Napoles et al. 2005; Ng et al. 2005). We also found inconsistent support for destination effects, which might have stemmed from differences in ideologies that support immigration and multiculturalism or correspond to more robust healthcare and welfare systems.
Our results, thus, join a growing trend within the migration literature of questioning both the magnitude and causes of the commonly reported immigrant mortality advantage (e.g., Diaz, Koning, and Martinez-Donate 2016; Maskileyson 2019; Morey et al. 2020). While our study design does not allow us to draw decisive conclusions, examining the interactions between origin and destination regions does appear to offer some indirect support for explanations that focus on selection effects. In this way, our article highlights the need to pay greater attention to how restrictions on immigration flows affect the health composition of immigrant populations. Studies of international migration tend to focus on those who were able to migrate rather than on those who aspired to migrate but did/could not (Carling and Collins 2018; Carling and Schewel 2018). A shift in focus to studies of people who ultimately chose not to migrate or who were denied entry into their (hoped-for) destination country would help expand understandings of migration processes and outcomes.
Supplemental Material
Supplemental Material, sj-docx-1-mrx-10.1177_0197918321996347 - A Global Meta-analysis of the Immigrant Mortality Advantage
Supplemental Material, sj-docx-1-mrx-10.1177_0197918321996347 for A Global Meta-analysis of the Immigrant Mortality Advantage by Eran Shor and David Roelfs in International Migration Review
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.