
Abstract
Because of their often-dramatic, life-threatening flight patterns and resulting pronounced health disparities, many refugees have a great need for medical treatment after arrival to their host countries. In Germany, refugees whose asylum application is not approved or whose duration of stay has not yet exceeded 15 months must request doctor visits, with a considerable amount of bureaucracy, from the local responsible authority. Since 2016, however, several federal states and municipalities in Germany have introduced electronic health cards (eHCs) which give refugees immediate and unbureaucratic access to the healthcare system. We examine whether being eligible for eHCs because of this policy change had an effect on multidimensional health indicators for refugees in Germany. For empirical identification, we take advantage of variation in policy adoption across German regions and over time. Relying on the IAB-BAMF-SOEP Survey of Refugees, we find that being eligible for eHCs because of the policy change improved the mental well-being and subjective health assessment of recently arrived refugees, while having no impact on physical health status. These results can be traced back to the moderating effect of facilitated healthcare access on post-migration stress, which is known to affect primarily psychological well-being. Moreover, facilitated healthcare access appears to alleviate potential language and cultural barriers faced by refugees with low health literacy (measured by the ability to read or write in the origin-country language). Altogether, the article illustrates how structural and institutional constraints may shape individual health outcomes of adult refugees.
Keywords
Introduction
Refugee 1 migration and integration have become prominent topics in research (Brell, Dustmann, and Preston 2020; Hatton 2020) and politics in recent years (OECD 2018), as migration figures have increased in response to war, persecution, and other forms of violent conflicts associated with events like the Arab Spring in late 2010 (Hatton 2020; Valdez 2020). The often life-threating events and stressful or traumatic experience that refugees encounter before and during forced migration (Brücker, Jaschke, and Kosyakova 2019), together with substandard living conditions and post-migration stress in host countries (Silove et al. 1999; Robjant, Hassan, and Katona 2009), create a specific burden for refugees compared to other migrants, particularly vis-à-vis health status (see Lindert et al. 2009; Sardadvar 2015). Especially common among refugees are mental health problems (Silove et al. 2007; Li, Liddell, and Nickerson 2016; Claassen and Jäger 2018; Kindermann et al. 2020) that can be difficult to detect in this population due to cultural and linguistic barriers, as well as communication and recall problems (Crumlish and O’Rourke 2010). Given the relevance of health status for individual educational achievements (Eide and Showalter 2011), economic integration (Chatterji, Alegria, and Takeuchi 2011), and social inclusion (Steptoe, Deaton, and Stone 2015), facilitated access to healthcare in the early phase after arrival in the host country may be essential for refugees’ well-being and integration prospects (Kindermann et al. 2020).
Against this background, this article addresses the important issue of whether earlier and improved access to the healthcare system has a positive effect on the mental and physical health outcomes of recently arrived refugees in Germany. Germany has evolved as the main refugee destination among high-income OECD countries in absolute and relative terms (Brücker, Kosyakova, and Vallizadeh 2020): from 2015 to 2018, 41 percent (1.6 million) of the 3.9 million first-time asylum applications in the EU-28 were submitted in Germany (Eurostat 2019). Two-thirds of the recently arrived refugee population in Germany came from Syria, Afghanistan, Iraq, Eritrea, and Iran — countries affected by armed conflict, group persecution, and other human rights violations (Brücker, Jaschke, and Kosyakova 2019). Not surprisingly, refugees in Germany are associated with poorer mental health outcomes relative to the native population and other migrant groups (Brücker et al. 2019; Metzing, Schacht, and Scherz 2020).
In addition to the pronounced health risks that refugees face, they also encounter several limitations in their access to healthcare services in Germany (Wenner et al. 2020). Specifically, refugees whose asylum application was either rejected or is still being processed cannot receive medical treatment in Germany during the first 15 months of their stay, without the consent of nonmedically trained personnel from social and immigration offices, who act as so-called gatekeepers (Kroneman, Maarse, and Zee 2006; Rolke, Wenner, and Razum 2019). The barriers to accessing healthcare that refugees in Germany face likely result in health impairments and illnesses which go undiagnosed and which may have severe consequences for not only refugees’ health status and personal life situation (Bischoff et al. 2003; Robjant, Hassan, and Katona 2009) but also the financial costs of treating protracted illnesses (Bozorgmehr and Razum 2015). Recent policy changes in Germany, however, modified existing rules and introduced electronic health cards (eHCs), which allow refugees immediate, almost-unrestricted access to the healthcare system directly after they register in Germany (Wächter-Raquet 2016). The implementation of these policies, though, is subject to regional authorities and was adopted in only a few federal states and municipalities, creating pronounced regional and temporal variability in refugees’ access to healthcare. We investigate this important policy change in Germany to examine whether being eligible earlier for the eHC because of the policy change affects refugees’ health outcomes. Moreover, the national dispersal policies that determine refugees’ residential allocation in Germany 2 minimize the likelihood that refugee inflows into particular regions are driven by the availability of healthcare access, thereby providing an appropriate framework for causal inference and a valuable natural experiment. Given that refugees’ restricted access to the healthcare system is unique to neither Germany (Silove et al. 1999; Norredam, Mygind, and Krasnik 2006; Chase et al. 2017) nor refugees (Kullgren 2003), this article is of general interest for understanding the consequences of restricted health treatment services for vulnerable population groups in developed countries.
Using the rich, representative longitudinal data from the IAB-BAMF-SOEP Survey of Refugees, 3 we find that being eligible for eHCs because of the policy change indeed improved the mental well-being and subjective health assessment of refugees who arrived in Germany between 2013 and 2016, while having no effect on physical health. These results can be traced back to the moderating effect of facilitated healthcare access on post-migration stress, which is known to affect primarily psychological well-being (Silove et al. 1999; Robjant, Hassan, and Katona 2009). Our results further reveal that the early and facilitated healthcare access can alleviate potential language and cultural barriers often faced by refugees with low health literacy (measured by the ability to write and read in the origin-country language) (Murray and Skull 2005).
In the remainder of this article, we, first, outline the institutional policy context of refugees’ healthcare access in Germany. This section is followed by a review of the literature on refugees’ health risks, their access to the host-country healthcare systems, and the consequences of post-migration stress factors. The aim of this discussion is to form empirically testable hypotheses for the refugee population in Germany. We then present the data and operationalization of our dependent and independent variables. The results section discusses our findings on the policy change’s effect on refugees’ psychological and physical health outcomes, the mediating role of post-migration stress, and heterogeneity of the policy-change effects. In the final section, we draw our conclusions.
Policy Context
Since 1993, refugee access to healthcare in Germany has been regulated by the German social welfare law for asylum-seekers (Asylbewerberleistungsgesetz, AsylbLG, para.4), which restricts refugee access to the healthcare system for the first 15 months of their stay (Wenner et al. 2020). During this time, refugees, including those with pending asylum applications and those whose applications were rejected but whose stay in Germany is tolerated (Duldung), are only eligible for the primary, basic treatment of acute illnesses and pain and for further time-sensitive interventions (i.e., pregnancy) (AsylbLG, para.4). If they require a doctor’s visit, refugees must request it, either from the local authority for foreigners or the responsible social assistance office (Wächter-Raquet 2016; Wenner et al. 2020). Such decisions on medical treatment claims are made by employees without specific medical training; therefore, in many cases, a medical treatment requires a consultation with the local health authority beforehand, which can sometimes take months. Due to poor language concordance and potential miscommunication, this non-medically trained staff may constitute intermediaries that reinforce linguistic and cultural barriers to healthcare for refugees (Bischoff et al. 2003). Additionally, from the host society’s perspective, restricting access appears to be counterproductive as it substantially increases costs through delayed treatment (Bozorgmehr and Razum 2015) and the administrative burden through case-by-case accounting (Wenner et al. 2020). 4
Recent changes in policies concerning refugees in October 2015 (in particular, Asylverfahrensbeschleunigungsgesetz) included, inter alia, important amendments concerning refugee access to the health system (Grote 2018). In particular, it facilitated the possibility for Germany’s 16 federal states to sign a framework agreement with health insurance funds to care for and ensure health provisions for refugees in their first 15 months of stay. If federal states opt for a general agreement with health insurance funds and if administrative authorities at the lower regional level (district or municipality) decide to join, refugees with pending or rejected asylum applications who reside in affected territories, even in the first 15 months of stay, gain far more comprehensive access to the healthcare system than they would otherwise have gained. In such states, refugees obtain an eHC that treats them almost equivalently to “standard” official health insurance contributors in terms of services that they can receive. 5 Once in possession of an eHC, refugees can directly approach (independent) physicians and hospitals without pre-contacting the local authority for foreigners or the responsible social assistance office.
In some (urban) federal states — namely, Bremen and Hamburg, corresponding arrangements were already agreed upon in 2005 and 2012, respectively, on a voluntary basis with insurance funds (based on individual-case reimbursement of costs). After the reform in October 2015, however, large-scale implementation in other German federal states became possible. During the period of investigation (2013–2019), seven out of sixteen German federal states introduced eHCs for refugees with pending or rejected asylum applications in their territories, either ubiquitously or in selected districts or municipalities (for details, see Figure A1 and Table A1 in the Online Appendix). These regional and temporal heterogeneities create a quasi-experimental research setting.
Theoretical Background and Literature Review
Refugees’ Pre- and Post-migration Health Risks
In view of the existing health disparities linked to migrants’ legal status (see Hamilton, Hale, and Savinar 2019 for the United States; see Lindert et al. 2009 for meta analyses comparing labor migrants and refugees in various destination countries), refugees seem to be particularly vulnerable to severe health conditions for the following reasons. First, compared to economic migrants, refugees are less oriented toward the labor market in their migration decision and, therefore, less likely to be positively selected based on health (Chiswick, Lee, and Miller 2008). Second, refugees (often) suffer from various traumatic experiences in the home country and on their way to the destination country. Between 70 and 85 percent of recent refugees in Germany, for example, arrived from countries affected by wars or war-like situations or human rights violations, according to the Uppsala Conflict Database and the Political Terror Scale (Brücker, Jaschke, and Kosyakova 2019). Approximately one-quarter of these populations reported shipwrecks, two-fifths reported physical assaults, and 15 percent of female refugees reported sexual assaults during their migration experience (ibid.). Third, in destination countries, refugees often suffer from post-migration stress, which turns out to be an important determinant of refugees’ health outcomes (Porter and Haslam 2005; Li, Liddell, and Nickerson 2016). Fourth, refugees’ health literacy is typically low compared to other population groups (Wångdahl et al. 2014). As previous research for western societies indicates, lower health literacy may deter refugees from treatments they consider suspicious or morally or religiously unacceptable, thereby reinforcing health disparities (von Wagner et al. 2009; Wångdahl et al. 2014).
All of these challenges have important consequences for refugees’ health status: empirical evidence on refugee populations resettled in major western countries reveals severe mental health impairments among refugees, particularly compared to other population groups of similar age (Fazel, Wheeler, and Danesh 2005; Robjant, Hassan, and Katona 2009). At the same time, empirical evidence on refugees’ physical health is scarce. While some studies report a prevalence of physical health problems among refugees in various destination countries (Weinstein, Sarnoff, and Gladstone 2000; Gerritsen et al. 2006), comparison with other population groups suggests that refugees have, on average, better physical health status (Brücker et al. 2019; Metzing, Schacht, and Scherz 2020) and lower mortality rates (Norredam et al. 2012). In contrast to the previous literature, our data allow separate analyses of refugees’ mental and physical health status. As we show, such distinction might be crucial when considering the role of the refugees’ access to the healthcare system.
Refugees’ Access to the Healthcare System
Refugees are disadvantaged regarding no (legal) access to healthcare services in many host countries (Silove et al. 1999; Norredam, Mygind, and Krasnik 2006; Chase et al. 2017). For instance, although refugee access to medical screening upon arrival has been safeguarded in almost all EU-25 countries, in nearly half, pregnant women, children, and adult refugees face legal restrictions in access to healthcare (Norredam, Mygind, and Krasnik 2006). In most of these cases, only emergency care is available (ibid.). In other cases, bureaucratic obstacles, such as identity card requirements, can create insurmountable barriers for refugees (Norredam, Mygind, and Krasnik 2006; Alawa, Zarei, and Khoshnood 2019). Such restricted access to healthcare systems seems to deteriorate refugees’ health status (Robjant, Hassan, and Katona 2009; Coffey et al. 2010; Chase et al. 2017).
Beyond access to basic health treatment per se, some recent studies have emphasized the importance of timely and extended healthcare access for patients in general (Johannessen et al. 2001; Sampalis et al. 2001; Kullgren 2003; Arango et al. 2018). For instance, the negative effect of long waiting times during medical (surgical) operations on patients’ health status and life satisfaction following the intervention has been empirically documented (Sampalis et al. 2001). Likewise, a delayed treatment may not only increase treatment costs due to the aggravation of illness but also pose a risk to public health in the case of communicable diseases such as tuberculosis and HIV (Kullgren 2003). In terms of mental health risks, available clinical treatment approaches often seem to be ineffective for already-manifested illnesses such that great importance is attached to early detection and prevention (see Arango et al. 2018). The significance of accessible and comprehensive health services has been further shown for refugees, for whom reduced waiting times for health treatment can result in more effective care (McMurray et al. 2014). Taken together, the aforementioned research findings suggest that easy and direct access to treatment shortens the time to diagnosis and, thus, improves the success of a given therapy (Johannessen et al. 2001). This implication should be taken into account when examining the potential consequences of the above-described policy changes in Germany that allow refugees earlier access to the health system, as the following section does.
Hypotheses on the Role of (timely) Healthcare Access for Refugees’ Health Outcomes
In Germany, all refugees are technically eligible for primary basic treatment of acute illnesses and time-sensitive interventions. Moreover, all refugees will eventually have full access to the healthcare system, after a 15-month residency requirement (see the Policy context section). In this regard, it is not access to the healthcare system per se but rather facilitated and immediate access to extended healthcare that might be crucial for newly arrived refugees’ health outcomes. The following theoretical model illustrates the connections between early facilitated healthcare access and refugee health outcomes.
In particular, refugees who did not initially possess the eHC likely faced pronounced practical obstacles when consulting a doctor. Available evidence from a qualitative survey of 16 refugees in Germany in 2015 reveals that access to the healthcare system via the social and immigration authorities (i.e, without eHC) was “hurdle-packed, bureaucratically inefficient and incapacitating” (Spura et al. 2017, 468). This non-direct healthcare system access, in turn, delayed the start of medical treatment and may have worsened refugees’ health status and prevented them from experiencing self-efficacy regarding their own disease management. Likewise, general practitioners, social workers, employees of statutory health insurance organizations, 6 and the gatekeepers responsible for refugees’ admission to treatment report the eHC’s facilitating effect, such as reducing their personal workload and increasing treatment access for refugees (Rolke, Wenner, and Razum 2019). In fact, eHC acquisition resulted in greater utilization of medical services by refugees in Germany (Bauhoff and Göpffarth 2018; Claassen and Jäger 2018). Altogether, then, we hypothesize that refugees assigned to German regions that provide refugees with immediate access to the healthcare system via the eHC show better health outcomes than refugees assigned to German regions with restricted access to the healthcare system (H1).
Refugees traumatic events before, during, and after forced migration are strongly linked to their mental stress and disturbance, which are likely to stay undiagnosed without the eHC, because of refugees’ underutilization of healthcare services (see Nickerson et al. 2010 for Australia; Claassen and Jäger 2018 for Germany). In turn, the eHC may be less important for diagnosing physical diseases among newly arrived refugees because such health problems are likely to be detected during mandatory medical screening programs upon arrival. These routine medical examinations aim to identify potential infectious disease among or basic health needs of refugees (Bozorgmehr et al. 2016; Ossege and Köhler 2016). Therefore, the early and extended healthcare access to medical treatment could be particularly relevant to refugees’ psychological health outcomes and, to a lesser extent, their physical well-being. In this regard, the positive effect of being assigned to German regions that provide refugees with immediate access to the healthcare system via the eHC should be particularly visible for mental health outcomes (H2).
Some recent studies have argued that the stress that refugees experience in destination countries (a.k.a. post-migration stress) may heighten existing mental problems (Porter and Haslam 2005; Li, Liddell, and Nickerson 2016; Walther et al. 2020) and may be an even more important predictor of refugees’ mental health status than traumatic experiences before and during the flight (Beiser and Hou 2016). Hence, immediate and direct access to the healthcare system via the eHC may lower the likelihood of experiencing stress while trying to navigate the healthcare system in the following ways. First, the eHC may mitigate the consequence of perceived legal insecurity that refugees face while waiting for their asylum decisions. These feelings of legal insecurity appear to worsen psychosocial health and to increase the risk of anxiety and depression (Robjant, Hassan, and Katona 2009) and may exacerbate the trauma that refugees suffer in their origin countries or during flight (Coffey et al. 2010). Second, mental illness is often associated with social stigma (Weiss, Ramakrishna, and Somma 2006; Thornicroft et al. 2016). Accordingly, if refugees without the eHC delay contact with treatment admission officers (gatekeepers) for fear of discrimination and stigmatization, they could face further psychological stress due to lacking necessary medical treatment. Third, refugees’ lack of access to stable and secure housing (Adam et al. 2019) is an important post-migration stress factor, since life in temporary collective accommodations goes hand-in-hand with a lack of privacy, autonomy, and isolation from the local community (Porter and Haslam 2005). Fourth, post-migration stress might be a direct consequence of more complicated and indirect healthcare access without the eHC (Chase et al. 2017). Altogether, then, on the one hand, earlier and facilitated access to extended healthcare may alleviate the consequences of post-migration stress for refugees to some extent. On the other hand, refugees with safeguarded healthcare access may feel more secure and be more resistant to post-migration stress. Either way, the positive effect of being assigned to German regions that provide refugees with immediate access to the healthcare system via the eHC on health outcomes is likely to be (partly) mediated via post-migration stress (H3).
The lack of easily accessible extended healthcare might be particularly disadvantageous for refugees with communication problems (i.e., poor host-country language proficiency) or poor health literacy (i.e., a lack of knowledge about health and the healthcare system) (Wångdahl et al. 2014), since these refugees might be less capable of expressing their health-related problems in the German language (Spura et al. 2017). Both communication problems and poor health literacy, in turn, might reduce refugees’ trustworthiness and credibility for the treatment admission officers (gatekeepers) and, therefore, refugees’ approval chances for the treatment claim (Weisse, Sorum, and Dominguez 2003; Ashton-James and Nicholas 2016). Correspondingly, the negative effect of being assigned to German regions with restricted access to the healthcare system on refugees’ health outcomes should be stronger for (health)-illiterate refugees (H4).
Data and Method
IAB-BAMF-SOEP Survey of Refugees in Germany
For our analysis, we rely on the IAB-BAMF-SOEP Survey of Refugees in Germany, 7 a longitudinal survey of refugees and their household members conducted annually (Brücker et al. 2016). The target population for this survey is drawn from the Central Register of Foreigners (Ausländerzentralregister, AZR), the national registry of all foreign citizens in Germany. The survey covers all individuals seeking asylum or any other form of protection, irrespective of their current legal status, who arrived in Germany for humanitarian reasons between 2013 and 2016 and were registered in the AZR by January 2017. By using appropriate sample weights, the data allow us to make representative inferences for these refugee populations in Germany and their household members (Kroh et al. 2017). The survey was carried out in 169 representatively selected sampling points across Germany, allowing us to draw representative conclusions at regional levels.
The survey’s first wave was conducted between June and December 2016 and covered 4,465 adult refugees. The gross participation rate was approximately 50 percent of addresses originally drawn, which is substantially higher than in comparable surveys of the German population (Kroh et al. 2017). Interviews were conducted face-to-face with computer assistance (CAPI) and were supported by translators, if needed. Questionnaires were available in seven languages (Arabic, English, Farsi/Dari, German, Kurmanji, Pashtu, and Urdu) and with auditory instruments for survey participants who were illiterate. The second wave covered 67 percent of participants in the first wave and included an additional sample that resulted in data for 2,559 panel respondents and 2,897 first-time respondents (Brücker et al. 2019). The response rate for panel respondents in the third wave was 68 percent, while the panel stability amounted to 80 percent (Britzke and Schupp 2020). As a result, the data from the IAB-BAMF-SOEP Survey of Refugees in Germany include 7,950 adult persons (18 years and older) who contributed 14,436 person-year observations over three survey waves. Overall, 41 percent of respondents participated only once, 38 percent could be observed over two survey waves, and 22 percent participated over three waves.
Analytical Sample
We excluded refugees who arrived before 2013, refugees who had missing information on arrival year, and individuals who were identified as nonrefugees (526 person-year observations). The dates of arrival, the decision on asylum applications, the decision outcomes, and the place of first residence are critical for the definition of our treatment and control groups (see the Independent variables section). For this reason, we excluded refugees with more than one asylum application (632 person-year observations) and with missing or implausible information on the dates, asylum decision (1,851 person-year observations), and first place of residence (813 person-year observations). After these exclusions, we ended up with 5,922 respondents who contributed 10,614 person-year observations (74 percent of the original sample). Since the availability of our dependent outcomes vary by survey waves and by respondent groups, the size of the corresponding analytical samples differs. This issue is addressed in the subsequent section.
Dependent Variables and Method
To address refugees’ health status, we rely on a series of multidimensional indicators such as (1) symptoms of depressive illness and anxiety (PHQ-4, henceforth, depression and anxiety), (2) a mental component summary scale (MCS, henceforth, mental well-being), (3) a physical component summary scale (PCS, henceforth, physical well-being), (4) health satisfaction, and (5) self-rated health status. 8 The underlying survey questions regarding the utilized health indicators are illustrated in Table A4 in the Online Appendix. Table 1 presents descriptive statistics for the dependent variables in the pooled sample.
Descriptive Statistics of Dependent Variables.
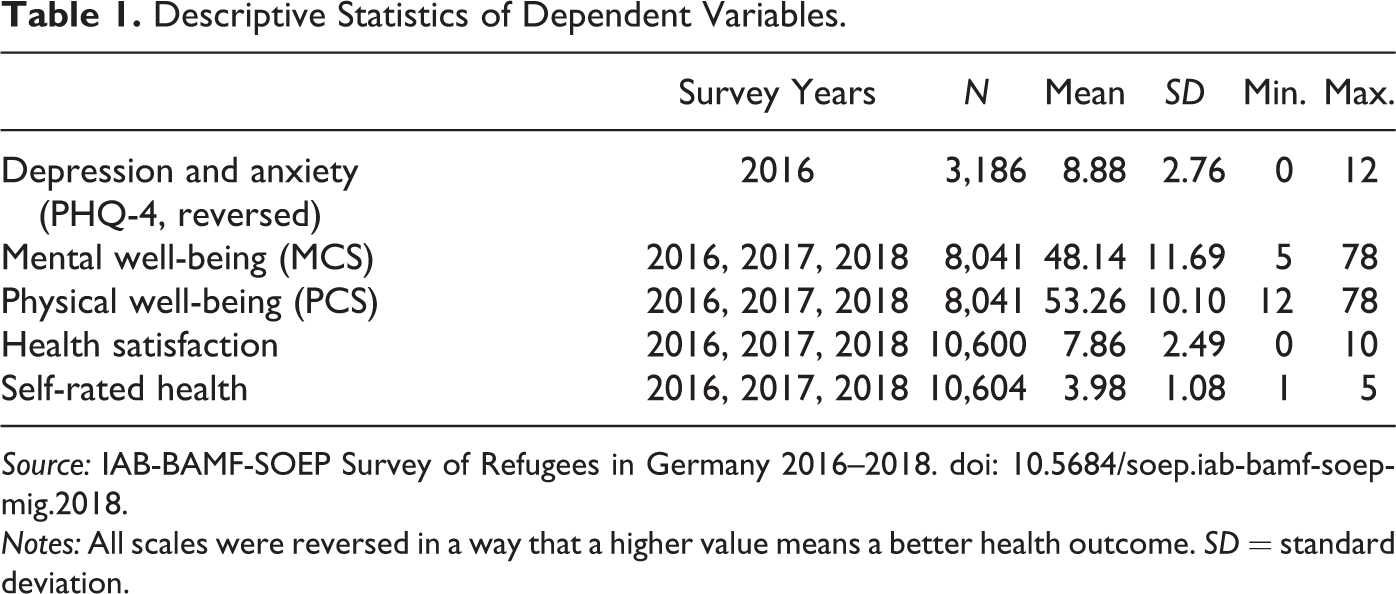
Source: IAB-BAMF-SOEP Survey of Refugees in Germany 2016–2018. doi: 10.5684/soep.iab-bamf-soep-mig.2018.
Notes: All scales were reversed in a way that a higher value means a better health outcome. SD = standard deviation.
The PHQ-4 is an established four-item measure of depression and anxiety (Löwe et al. 2010). The original scale ranges from zero to twelve, where a higher value corresponds to more reported symptoms. The threshold of six or greater indicates a “yellow flag,” and the threshold of nine indicates a “red flag” for the presence of a depressive or anxiety disorder (Löwe et al. 2010). The PHQ-4 was only available for first-time respondents in 2016. For the empirical analyses, we reversed the scale so that a higher value corresponds to a lower level of depression and anxiety (i.e., better health).
The sum scales for PCS and MSC are provided by the Socio-Economic Panel (SOEP) (Andersen et al. 2007) and are calculated based on the so-called short form version 2 questionnaire (SF-12v2; Ware et al. 2002). SF-12v2 is a widely used measurement instrument based on a series of questions related to self-reported assessments of symptoms such as physical and mental aspects of the health-related quality of life, particularly physical functioning, the role of physical and bodily pain in general health, vitality, and social functioning, and the role of emotional and mental health. Both scales — although they cannot replace clinical studies — have become established instruments with which to proxy respondents’ health status in the social sciences (Andersen et al. 2007). The SF-12v2 was collected for first-time respondents in 2016 and 2017 and for all respondents in 2018. Both the PCS and MCS sum scales vary from theoretical 0 to 100, where a higher value corresponds to a higher level of well-being.
The next two health indicators refer to the subjective assessment of one’s own health status. First, we consider satisfaction with current health, which is a self-stated measure on an 11-point scale that ranges from 0 (“totally unhappy”) to 10 (“totally happy”). Second, we refer to the self-rated current state of health that is scaled between 1 (“poor”) and 5 (“very well”). These measures reflect slightly different aspects of one’s subjectively perceived health situation and may provide a more comprehensive view on overall health status, since they combine mental and physical health status. Subjective health evaluations have become conventional ways to address the health status of the population of interest (Idler and Benyamini 2006; Huijts and Kraaykamp 2012).
In the multivariate analyses, we apply log specifications to the MCS, PCS, and PHQ-4 scales to consider the potential nonlinear relationships between the explanatory and dependent variables. Since the variables for the PHQ-4 are only available for one point in time, we apply a cross-sectional ordinary least squares (OLS) estimation with robust standard errors. The rest of the health indicators were surveyed more than once over waves; accordingly, we apply a panel random effects estimation with robust standard errors. 9
Independent Variables
Treatment and control groups
We define the treatment group in terms of having access to the health system as a consequence of the policy intervention, as outlined in the Policy context section (i.e., being qualified for an eHC via the policy change). Importantly, our analysis resembles an intention-to-treat framework because we do not have factual information about whether an individual actually possesses the eHC. Instead, belonging to the treatment or control group depends on the following four factors: the assigned residence (based on the survey question about respondents’ first or longest place of residence in Germany); the date of policy introduction (if the policy was implemented at all in the region); the length of stay in Germany; and the type and date of the decision on the asylum application.
Essentially, in the first 15 months of their stay in Germany, refugees receive benefits according to the Asylum Seekers Benefits Act (Asylbewerberleistungsgesetz), which restricts their utilization of health services to the basic provisions, as previously outlined. Upon approval of their asylum application or after 15 months, refugees with a pending or rejected asylum application receive the eHC and, therefore, gain comprehensive healthcare access. Correspondingly, respondents in our sample may qualify for the eHC not only via the policy change but also via their asylum application approval or the duration of their stay. To address potential heterogeneity within the control group, we consider the following categorization for our explanatory variable: Eligibility for the eHC via policy change (treatment); Eligibility for the eHC via status approval (control); Eligibility for the eHC via duration of stay (control); and Not eligible for the eHC (control).
In total, only five federal states — Berlin, Bremen, Hamburg, Schleswig-Holstein, and Thuringia — have introduced the eHC for refugees throughout their territories. In Brandenburg, Lower-Saxony, North Rhine-Westphalia, and Rhineland-Palatinate, only selected districts or municipalities have introduced the eHC. Figure A1 and Table A1 in the Online Appendix include a detailed overview of the localities with the eHC and information on the date when the policy was implemented for each region.
We define individuals as belonging to the treatment group — those eligible for the eHC via policy change — if the following conditions apply: (1) refugees reported their assigned place of residence in a region subject to the above-described policy intervention; (2) their asylum application was not yet decided by the date of the policy intervention (independent of the eventual decision type by the interview date); and (3) they arrived less than 15 months before the date of the policy intervention. Consider, for example, a refugee who arrived in July 2015, who was assigned to Berlin, and who had an asylum approval date of August 2016. The reform of the eHC implementation in Berlin took place in January 2016. Given that the policy intervention in Berlin occurred before the application approval and not later than 14 months after arrival, we define the refugee in the example as treated (i.e., eligible for the eHC via policy change).
We define refugees as eligible for the eHC via status approval if their asylum application was approved by the interview date and if this approval occurred within the first 15 months of their stay in Germany. For respondents assigned to regions subject to the eHC reforms, approval should occur before the reform’s date. Accordingly, the refugee in the example above would be defined as eligible for the eHC via status approval if the asylum approval date was December 2015 or earlier.
Refugees are defined as eligible for the eHC via duration of stay when their duration of stay exceeded 14 months and (a) the decision on asylum applications had not yet been received (or refugees were rejected and their stay in Germany was tolerated), as of that date, or (b) their asylum application was approved and the date of approval fell after the date when the duration of stay exceeded 14 months. For respondents assigned to regions subject to the eHC reform, the 15 months or longer duration of stay should occur before the reform’s date. The refugee in our example would be defined as eligible for the eHC via duration of stay if the arrival date was October 2014 or earlier. In all other cases (i.e., assigned to a district without the reform and no decision or a negative decision on the asylum application and the duration of stay does not exceed 15 months by the interview date), refugees are defined as not eligible for the eHC.
In our data, roughly twelve percent of the person-year observations were eligible for the eHC via policy change (see Table A2 in the Online Appendix). The control group is considerably heterogeneous. In total, 82 percent were eligible for the eHC via either status approval or duration of stay, while six percent faced restrictions in healthcare access. This distribution varies considerably over the survey waves and respondent type (first and panel respondents). Refugees with eHC access via the policy change waited, on average, 2.6 months before being eligible. This wait was more than twice as long for refugees with eHC access via status approval (6.5 months), while the censored waiting times of non-eligible refugees amounted to 11 months.
Post-migration stress
To address the role of post-migration stress, we include several factors that have been identified in the literature as particularly important for refugees’ health status (see Li, Liddell, and Nickerson 2016 for a review). These factors include living in reception centers or communal accommodation, as opposed to private housing, having members of the nuclear family overseas, experiences of discrimination based on origin, the feeling of being welcome in Germany, and worries about the prospects of staying in Germany.
Literacy
Unfortunately, our data do not allow a straightforward measurement of health literacy among refugees. Instead, we proxy health literacy via a dummy indicator for being CO (country of origin) illiterate, which is defined as being unable to read or write in the origin country’s mother tongue or official language. Corresponding language skills were surveyed based on a self-reported scale from 1 (“Not at all”) to 5 (“Very good”). As previous research indicates, illiteracy correlates negatively with health literacy (von Wagner et al. 2009; Wångdahl et al. 2014).
Confounders
Generally, a natural experimental research design ensures that the lack of information on confounders is randomly distributed across regions because refugees’ regional allocation is exogenously driven (i.e., assignment to the treatment and control groups is exogenous); therefore, omitting any observables and unobservables should not bias our results so long as they are not related to health outcomes. However, a natural experiment such as ours allows for more noise than a controlled laboratory experiment. For this reason, we control for commonly observed predictors of individual health in our multivariate analyses (Mascini and Van Bochove 2009; Nickerson et al. 2010). These predictors include (1) socio-demographics such as origin country (group) fixed effects (aggregated into Syria, Afghanistan, Iraq, Eritrea, Iran, the remaining Middle Eastern and North African (MENA) countries, Russia, the remaining states of the former Soviet Union, the West Balkans, the remaining countries in Africa, and the rest of the world), gender, age and age squared, having a partner, and having children in the household and (2) pre-migration human capital characteristics such as years of education and years of work experience. The controls specific to migrants and refugees in particular include months of stay (until the interview) and having a traumatic experience (during escape).
There is some empirical evidence that larger municipalities are more likely to implement the eHC for refugees to reduce the administration of related costs and workload (Rolke, Wenner, and Razum 2019). 10 Therefore, to account for the local context of reception in the assigned region, we include municipality-level population density, district-level hospital bed density, the unemployment rate, median income per capita, share of foreigners, and share of the politically far-right votes in the 2017 federal election. We further control for region fixed effects measured via the federal state of the first residence to further absorb potentially important, time-constant links between the local context of reception and individual health. Finally, to absorb any systematic differences related to survey design, we control for the survey wave and survey sample. Descriptive statistics for the control variables are presented in Table 2; details on the variables’ construction are presented in Table A5 in the Online Appendix.
Descriptive Statistics on Control Variables.
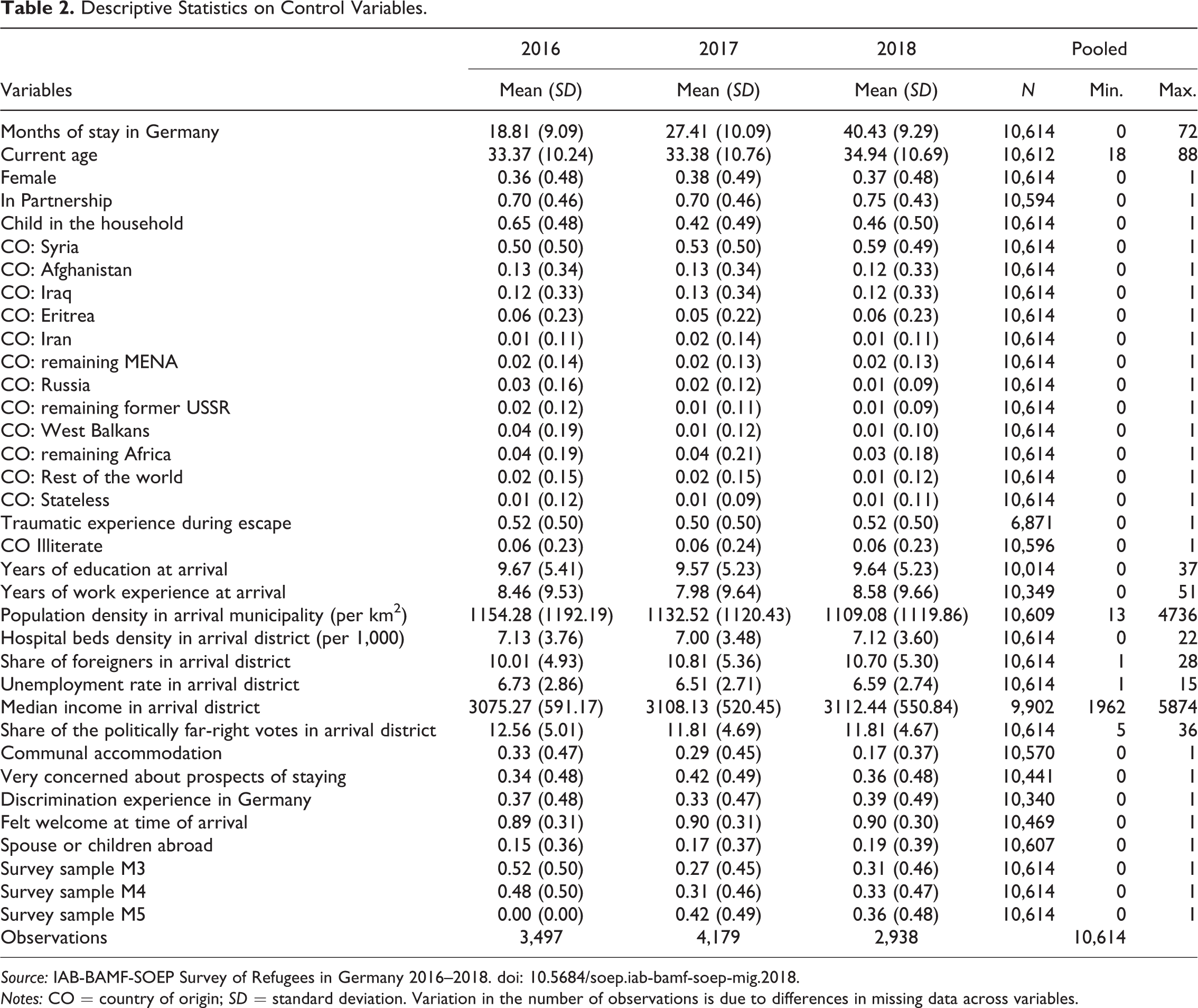
Source: IAB-BAMF-SOEP Survey of Refugees in Germany 2016–2018. doi: 10.5684/soep.iab-bamf-soep-mig.2018.
Notes: CO = country of origin; SD = standard deviation. Variation in the number of observations is due to differences in missing data across variables.
To address missing information, we use multiple imputation with chained equations (van Buuren 2012). We construct 25 imputed data sets that use all available information from the full models and additional variables that may be correlated with the used model variables in some way. Respondents with missing information on health outcomes and on asylum decisions were included in the multiple imputation but not in the analyses. Missing information was present to varying degrees, with a maximum of 35 percent in the measure for traumatic experience (during escape) (see Table 2, column 7). Note that we refrain from imputing the missing dates of arrival or asylum decision because such missing information is likely to not be random and to correlate with education and literacy (see Table A3 in the Online Appendix).
Results
Effect of the Policy Change on Refugee Health Outcomes
Results from the multivariate regressions of the health outcomes on eHC eligibility and the entire set of explanatory variables are presented in Table 3. We build our models gradually by starting with inclusion of the treatment measure (Models with a subscript 1), followed by inclusion of individual-, origin-country-, and regional-level controls (Models with a subscript 2) and measures of post-migration stress (Models with a subscript 3).
Multivariate Regressions of Health Indicators.
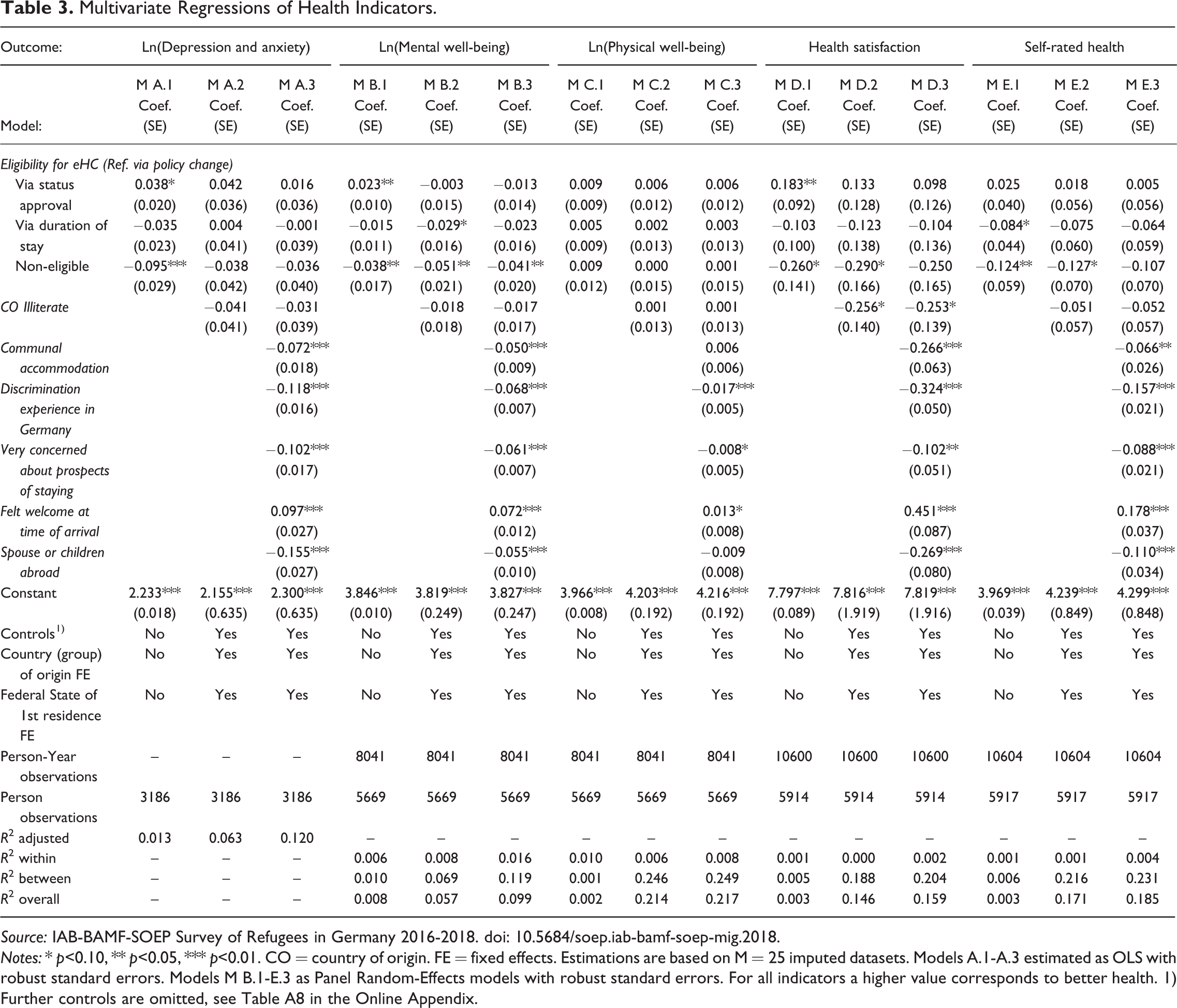
Source: IAB-BAMF-SOEP Survey of Refugees in Germany 2016-2018. doi: 10.5684/soep.iab-bamf-soep-mig.2018.
Notes: * p<0.10, ** p<0.05, *** p<0.01. CO = country of origin. FE = fixed effects. Estimations are based on M = 25 imputed datasets. Models A.1-A.3 estimated as OLS with robust standard errors. Models M B.1-E.3 as Panel Random-Effects models with robust standard errors. For all indicators a higher value corresponds to better health. 1) Further controls are omitted, see Table A8 in the Online Appendix.
Starting with depression and anxiety, our results imply a positive effect of eHC eligibility via policy change on refugees’ health outcomes (Model A.1). In particular, refugees who were not eligible for the eHC had ten-percent lower scores than refugees eligible via policy change. However, these differences fade after including further model covariates (Model A.2). For mental well-being, we similarly find a positive effect of the eHC via policy change (Models B.1), and this conclusion strengthens even after including further model covariates (Model B.2). Accordingly, we observe a five-percent lower score of mental well-being for refugees who were not eligible for the eHC compared to refugees eligible via the policy change, net of the model confounders. In turn, we do not find that eHC eligibility via policy change had any statistically significant effect on physical health compared to refugees who were not eligible for the eHC (Model C.1 and C.2). The differences between refugees eligible for the eHC via policy change and those eligible via status approval or duration of stay were also not statistically significant. Turning to the subjective health status measures, we again observe a positive effect of eHC eligibility via policy change compared to refugees who were not eligible at all. Specifically, non-eligible refugees were likely to report a 0.26-point lower health satisfaction (Model D.1) and a 0.12-point lower self-rated health (Model E.1). The corresponding effects remain statistically significant in the full models (Models D.2 and E.2).
In elaborating on these results in light of our hypotheses, we expected a positive effect of being assigned to regions with immediate access to the healthcare system via the eHC on health outcomes compared to being assigned to regions with restricted access to the healthcare system (H1). Since we find that eHC eligibility via policy change improved only mental well-being, health satisfaction, and self-rated health status and only compared to refugees who were not eligible, our results only partly conform to our expectations. 11 For depression and anxiety symptoms, although we observe a significant negative effect of being non-eligible, the effect reduces in size and becomes non-statistically significant in the full model. However, the statistical uncertainty might be an artifact of a smaller sample size: depression and anxiety symptoms were only surveyed in the first wave. Next, we expected that the eHC policy change would be particularly visible for mental health outcomes (H2). Given that we find a positive effect of eHC eligibility via policy change only for mental well-being and subjective health status, H2 is empirically supported. Accordingly, the provision of early, easy, and nonbureaucratic access to healthcare services, as implemented by the eHC, apparently has considerable positive effects on refugees’ mental health outcomes.
The Role of Post-migration Stress and Health Illiteracy
To test whether post-migration stress factors mitigated the positive effect of earlier healthcare access on refugees’ health outcomes (H3), we turn next to the models that include the covariates that approximate post-migratory living conditions. Indeed, the positive effect of being eligible for the eHC via policy change on refugees’ mental well-being is reduced in size — although it remains statistically significant — after controlling for post-migration stress factors (Model B.3). In turn, this relationship is explained for health satisfaction (Model D.3) and self-rated health (Model E.3). That is, refugees with facilitated access to healthcare services seemed to be less subject to post-migration stress than their counterparts who were eligible via another way or who were not eligible at all. These results are mostly consistent with our expectations.
In focusing on the results of the post-migration stress variables, the observed patterns conform to prior literature findings (see Li, Liddell, and Nickerson 2016 for an overview). In particular, living in reception centers or communal accommodation reduced refugees’ health outcomes significantly (except for physical well-being). Likewise, experiences of discrimination, worries about prospects of staying in Germany, and separation from family members may have negatively shaped refugees’ health outcomes.
Finally, we expected health-illiterate refugees to particularly benefit from eHC eligibility via policy change regarding their health outcomes (H4). The underlying argument is that health literacy facilitates refugees’ healthcare access by allowing more effective communication with government authorities and overcoming bureaucratic hurdles in the absence of the eHC. Table 4 presents the corresponding empirical exercise by showing the gap due to being CO illiterate (expressed in terms of average marginal effects) for different treatment types. Among refugees not eligible for the eHC, CO-illiterate refugees had a 22-percent worse score on depression symptoms and anxiety compared to CO-literate refugees. Among refugees subject to the eHC policy change, we observe the opposite patterns: CO-illiterate refugees had a 9-percent improved score. In turn, the differences for the other treatment categories were not statistically significant. These results are, thus, in line with H4. However, no such relationship could be confirmed for other health outcomes, which contrasts with H4.
Effect of Illiteracy on Health by eHC-Access.
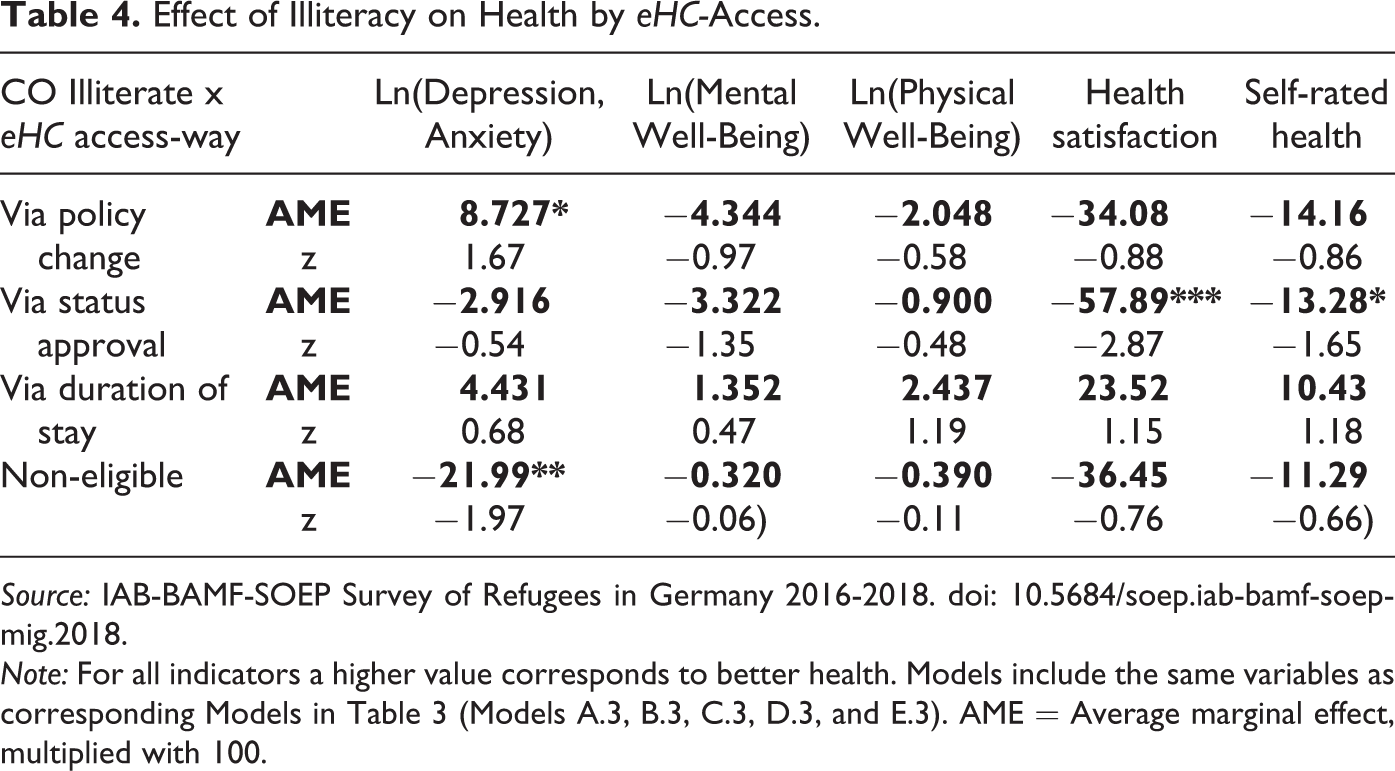
Source: IAB-BAMF-SOEP Survey of Refugees in Germany 2016-2018. doi: 10.5684/soep.iab-bamf-soep-mig.2018.
Note: For all indicators a higher value corresponds to better health. Models include the same variables as corresponding Models in Table 3 (Models A.3, B.3, C.3, D.3, and E.3). AME = Average marginal effect, multiplied with 100.
Discussion
Our article contributes to understanding how structural and institutional constraints may shape individual outcomes by investigating the consequences of the restricted healthcare access refugees face in Germany but also in many other refugee-host countries (Norredam, Mygind, and Krasnik 2006; Chase et al. 2017). Such policy constellations are not unique to refugees but also true for undocumented migrants in many cases (Kullgren 2003). Given their often-dramatic, life-threatening flight patterns and disproportionately high incidence of physical and psychological problems, refugees’ restricted access to healthcare services may not only deteriorate their health status but also have adverse economic and societal consequences for the host society. To facilitate refugees’ (earlier) access to the healthcare system, several federal states and municipalities in Germany have introduced electronic health cards (eHC), which allow an immediate, direct, nonbureaucratic, and comprehensive utilization of healthcare services. Whether and to what extent this policy change has had an effect on the physical and psychological health outcomes of recently arrived refugees in Germany is addressed in this article. By focusing, not on access to the healthcare system per se, but on easier and immediate access to extended healthcare, we add a nuanced aspect to the literature. For empirical identification, we exploit a unique policy reform in Germany that provides exogenous variation in (the timing of) local healthcare access for refugees. The national dispersal policies on refugees’ spatial assignment to their first place of residence allow us to circumvent the potential problem of regional (self-)selection and to make causal inferences on the reform effects.
Our analyses show significant health improvements in terms of psychological well-being, health satisfaction, and self-rated health status among refugees if early general access to the health system (i.e., in the first 15 months of the stay) is provided. For refugees’ physical well-being, we find no impact of immediate access to treatment. These findings could be due to the fact that refugees’ (often) traumatic experiences before, during, and after forced migration particularly affect their mental stress and disturbance, which are likely to stay undiagnosed without the eHC because of refugees’ underutilization of healthcare services (Nickerson et al. 2010; Claassen and Jäger 2018). In turn, existing mandatory screening programs upon arrival might be effective instruments for early diagnosing of physical diseases (Bozorgmehr et al. 2016; Ossege and Köhler 2016). At the same time, with an average age of just over 30 years of age, refugees are fairly young and have relatively good physical health, despite often-serious traumatic experiences before and during their flight (Brücker, Jaschke, and Kosyakova 2019; Metzing, Schacht, and Scherz 2020). Accordingly, the provision of early, easy, and nonbureaucratic access to healthcare services, as implemented by the eHC, apparently has considerable positive effects on refugees’ mental health outcomes.
Another two important inferences from our analysis relate to the role of (1) post-migration stress and (2) CO illiteracy. Similar to prior empirical studies (Silove et al. 1999; Robjant, Hassan, and Katona 2009; Walther et al. 2020), we observe that substandard living conditions, unclear staying perspectives, an unfriendly social environment, and separation from family are crucial hurdles for refugees’ psychological and physical health outcomes. Moreover, post-migration stress seems to mitigate the positive effect of earlier healthcare access, which means that refugees without such access are more vulnerable to an inferior post-migration environment. Regarding CO illiteracy, the reform’s effect seems to be particularly beneficial for CO-illiterate refugees regarding depression symptoms and anxiety. Due to language and cultural barriers, refugees often face disadvantages in making their first appointments with specialists (Murray and Skull 2005). As our results reveal, the eHC’s introduction can alleviate potential language and cultural barriers faced by refugees. Note that our sample is restricted to refugees with non-missing information related to recall and memory (such as recalling dates and assigned regions) and is, therefore, likely to be positively selected on human capital characteristics. 12 In this regard, our estimates represent only the tip of the iceberg: the patterns might become more visible for the entire refugee population.
Altogether, our results highlight that the eHC introduction improved the mental well-being of recent refugees in Germany through the provision of immediate access to mental healthcare services. By enabling easier navigation of the healthcare system, the eHC introduction additionally operates as a meaningful engine in mitigating refugees’ post-migration stress. Hence, our conceptual approach and empirical results provide new insights into the mechanisms linking early facilitated healthcare access and psychological health outcomes of recently arrived refugees in developed economies. Accordingly, our article reinforces the conclusion of Riosmena et al. (2015) on the importance of focusing on both structural and cultural explanations to understand the reasons for health differences between foreign- and native-born populations. Furthermore, our findings illustrate that considering multidimensional indicators of health outcomes is crucial since the consequences of restricted access to extended health services among refugees are only adverse for psychological health impairments and illnesses, both of which are at higher risk to remain undiagnosed (Bischoff et al. 2003; Robjant, Hassan, and Katona 2009). Lastly, our article not only contributes to a long-standing debate on the consequences of restricted healthcare access on newcomers’ health status but also allows investigation of its causal impact by relying on a quasi-experimental design.
From a policy perspective, a comprehensive nationwide introduction of the eHC for refugees could benefit both refugees and the German economy and welfare state (Bozorgmehr and Razum 2015). Free access to health services and early detection of depression, emotional distress, and psychiatric disorders, combined with effective treatments, may promote refugees’ long-term integration into the German labor market and society. Clearly, there is great potential in a nationwide introduction of the eHC for refugees, and this potential is highly transferable to other countries because refugees’ access to health services is restricted in most parts of the world (Norredam, Mygind, and Krasnik 2006; Chase et al. 2017).
Although this article focused on early access to (extended) healthcare for refugees, delving deeper into the quality of healthcare that refugees can access could be a fruitful avenue for future research. If demand for healthcare services increases, not only the supply but also the quality of healthcare services must be ensured. There is some evidence on pronounced regional disparities in the quality of healthcare services in Germany; the available capacity of relevant specialists (e.g., psychotherapists) is often already insufficient for the population in Germany without the recently arrived refugee cohorts (Albani et al. 2010). Moreover, standard therapeutic offerings in western European health systems such as Germany’s are often unable to address humanitarian migrants’ specific needs due to a lack of therapists specifically qualified to treat posttraumatic stress disorder (Leopoldina 2018) and a lack of targeted measures by non-specialists, such as the provision of stress management techniques by laypersons or social workers (Bajbouj et al. 2018).
In addition, future research should address refugees’ disproportional exposure to pandemics such as COVID-19 (WHO 2020). In these times, limited or delayed access to healthcare services may become even more jeopardizing for refugees’ health outcomes for the following reasons. First, many refugees still live in collective accommodations that restrict the possibility of social distancing. Second, refugees with mental illness may be particularly vulnerable to the effects of widespread panic and threats. Third, pressure on the healthcare system due to virus outbreaks may push back non-urgent treatments of psychiatric illnesses, particularly treatments that involve interactions with group attendance. Finally, reduced personal communication with authorities might result in delays of granting authorities’ consent for visiting a doctor or a hospital, thereby increasing the health risks of refugees without eHC access.
Supplemental Material
Supplemental Material, sj-docx-1-mrx-10.1177_0197918320980413 - Does Facilitated and Early Access to the Healthcare System Improve Refugees’ Health Outcomes? Evidence from a Natural Experiment in Germany
Supplemental Material, sj-docx-1-mrx-10.1177_0197918320980413 for Does Facilitated and Early Access to the Healthcare System Improve Refugees’ Health Outcomes? Evidence from a Natural Experiment in Germany by Philipp Jaschke and Yuliya Kosyakova in International Migration Review
Footnotes
Authors’ Note
Philipp Jaschke and Yuliya Kosyakova contributed equally and are listed in alphabetical order.
Acknowledgements
We would like to thank Hannes Kröger for sending the conversion tool for health indicators to us; Sekou Keita for valuable comments on the earlier version of this manuscript; and all those who commented on the earlier presentations of this work at the following events: the XI European Conference of the Fondazione Rodolfo De Benedetti (FRDB) in Calabria (June 2019), the Leibniz Institute for East and Southeast European Studies (IOS) Tuesday Seminar Series in Regensburg (July 2019), the Summer Meeting of the International Sociological Association (ISA) Research Committee on Social Stratification and Mobility (RC28) in Princeton, New Jersey (August 2019), and the European Consortium for Sociological Research (ECSR) 2017 conference in Lausanne (September 2019). We also thank the editor and three anonymous reviewers for their insightful comments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material for this article available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.