
Abstract
Objective
Various prognostic factors are associated with the survival of patients with parotid mucoepidermoid carcinoma (MEC). The aim of this systematic review is to summarize the clinical and pathologic prognostic factors on survival outcomes in patients with parotid MEC.
Data Sources
Articles published from database inception to July 2020 on OVID Medline, OVID Embase, Cochrane Central, and Scopus.
Review Methods
Studies were included that reported clinical or pathologic prognostic factors on survival outcomes for adult patients with parotid MEC. Data extraction, risk of bias, and quality assessment were conducted by 2 independent reviewers.
Results
A total of 4290 titles were reviewed, 396 retrieved for full-text screening, and 18 included in the review. The average risk of bias was high, and quality assessment for the prognostic factors ranged from very low to moderate. Prognostic factors that were consistently associated with negative survival outcomes on multivariate analysis included histologic grade (hazard ratio [HR], 5.66), nodal status (HR, 2.86), distant metastasis (HR, 3.10-5.80), intraparotid metastasis (HR, 13.52), and age (HR, 1.02-6.86). Prognostic factors that inconsistently reported associations with survival outcomes were TNM stage, T classification, and N classification.
Conclusion
Histologic grade, nodal status, distant metastasis, intraparotid metastasis, and age were associated with worse survival outcomes. These prognostic factors should be considered when determining the most appropriate treatment and follow-up plan for patients with parotid MEC.
Mucoepidermoid carcinoma (MEC) is the most common subtype (30%-50%) of malignant parotid gland tumors.1-5 The World Health Organization classifies MEC into 3 grades: low-, intermediate-, or high-grade tumors. 6 The mainstay of treatment for parotid MEC is surgery, the extent of which depends on the location, stage, and grade of the tumor. 7 Postoperative radiotherapy is recommended for patients at high risk for locoregional recurrence based on pathologic features.7-9 Despite the multimodal therapy approach, the 5-year mortality of high-grade MEC remains poor, estimated at up to 48%.10-12 Previous studies have described various clinical and pathologic prognostic factors associated with survival outcomes in patients with parotid MEC, such as patient age and sex, tumor grade, size, stage, and nodal metastases. 13 Better understanding of these prognostic factors will allow for the identification of individuals at the highest risk of disease-related mortality. The ability to risk-stratify cases of parotid MEC will help avoid overmanagement of low-risk cases and undermanagement of high-risk cases.14,15
The effect of clinicopathologic prognostic factors, such as grade, TNM classification, sex, and age, have been investigated in various cohort studies but have not yet been synthesized and described in unity. The aim of this systematic review is to summarize and evaluate the current literature on the correlation of clinicopathologic prognostic factors with the survival outcomes of patients with parotid MEC.
Methods
This study was reported according to the PRSIMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-analyses). 16
Search Strategy
The search strategy was developed with the expertise of a health science librarian at the University of Toronto. This study’s population of interest was patients with parotid MEC; the intervention of interest was prognostic factors for survival; and the outcome of interest was all types of survival outcomes. A search string for the mucoepidermoid cancer subtype was combined with a search string for anatomic locations of the head and neck, salivary gland, and parotid gland. To not limit the search results, no search strings were used for predictors and clinical outcomes. MeSH terms (Medical Subject Headings) and free-text terms were used: mucoepidermoid, head and neck, parotid, salivary gland, neoplasm, cancer, tumor, and carcinoma. Search strategies for all databases were adapted from the OVID Medline strategy. The full search strategy is available in Appendix A (available online). The following databases were searched on July 25, 2020: OVID Medline, OVID Embase, Cochrane Central, and Scopus. The results of all searches were combined and duplicates were removed.
Selection Criteria
Randomized controlled trials and prospective and retrospective cohort studies were all considered for inclusion. Case reports were excluded, as were publications such as animal studies, reviews, editorials, abstracts, and conference posters. Studies were included if they met the following criteria: adult population (≥18 years old), ≥10 cases, patients diagnosed with parotid MEC, survival data, and at least 1 demographic or clinical prognostic factor for survival (eg, grade, TNM classification, stage, age, sex). Studies were excluded if they met any of the following criteria: nonparotid primary, parotid cancer not of MEC subtype, survival data not reported or extractable, prognostic factors not of interest (eg, type of treatment, molecular markers), and English version unavailable.
Screening for the inclusion of articles was performed independently in 2 steps by 2 reviewers using Covidence systematic review software (Veritas Health Innovation). The titles and abstracts were first assessed for inclusion criteria, and those deemed relevant were assessed with the full text for inclusion into the study. Disparities between observers were resolved through discussion. Cohen kappa (percentage agreement) was calculated for interobserver reliability.
Risk of Bias Assessment
Risk of bias was assessed with the QUIPS tool (Quality in Prognosis Studies),17,18 which has been validated and used in several studies.14,18-20 The QUIPS tool assesses 6 domains to evaluate the validity and bias in studies of prognostic factors: study participation, study attrition, prognostic factor measurement, outcome measurement, confounding, and analysis. Each domain is scored on a scale from 1 (low risk) to 3 (high risk) based on preset criteria. 21 Therefore, each study had a total score ranging between 6 and 18 points. Studies that score ≤9 points are considered low risk of bias. 14 Risk of bias assessment was carried out independently by 2 reviewers. Disagreements were resolved through discussion.
Quality Assessment
Quality assessment of the outcome variables was conducted with the GRADE tool (Grading of Recommendations Assessment, Development, and Evaluation).22,23 The GRADE tool is objectively used to assess each outcome based on several domains, such as risk of bias, inconsistency, indirectness of evidence, imprecision, publication bias, and effect size. A GRADE score is assigned through a preset scoring system: very low, low, moderate, and high. A score of very low indicates that the evidence for the outcome is very low in quality and that the true prognosis is likely to be substantially different from the estimate. A high score indicates that the evidence for the outcome is of high quality and that the true prognosis lies close to that of the estimate.
Data Extraction
Data were extracted by 2 reviewers and the following information was obtained from each study:
Study characteristics (eg, years, location, and number of patients)
Effect of clinical prognostic factors on survival (eg, age and sex)
Effect of pathologic prognostic factors on survival: T classification (tumor size), N classification (nodal disease), M classification (distant metastasis), overall TNM stage, and grade
Other prognostic factors
Survival outcomes
Data Analysis
The data set overlapped for 3 studies11,24,25 in the SEER database (Surveillance, Epidemiology, and End Results) and 3 studies13,26,27 in the National Cancer Database. In this situation, the data from Chen et al 11 and Xiao et al 27 were extracted and the other studies excluded from analysis, as the study periods by Chen et al and Xiao et al encompassed the other studies for the SEER and National Cancer Database, respectively. The heterogeneity among survival outcomes precluded a meta-analysis. If the results of at least 75% of the studies analyzing the effect of a specific prognostic factor on multivariate analysis pointed in the same direction, the findings were considered consistent. 14 If the results of <75% of the studies pointed in the same direction on multivariate analysis, the findings were considered inconsistent. If all studies showed no association on multivariate analysis, the findings were deemed to have no association. Prognostic factors with <2 studies with a multivariate analysis were qualitatively described. Studies that did not conduct a multivariate analysis were qualitatively synthesized.
Results
Study Selection
The database search identified 8503 abstracts from OVID Medline (n = 2358), OVID Embase (n = 3158), Cochrane Central (n = 15), and SCOPUS (n = 2972). After the removal of duplicate articles, 4290 articles were available for screening. After initial abstract and title screening, 3877 articles were excluded and 17 failed to be retrieved, resulting in 396 articles being sent to full-text review. After full-text screening, 378 articles were excluded and the remaining 18 were included in our analysis ( Figure 1 ). Cohen kappa for interobserver reliability was 0.64, indicating substantial agreement between the reviewers. 28
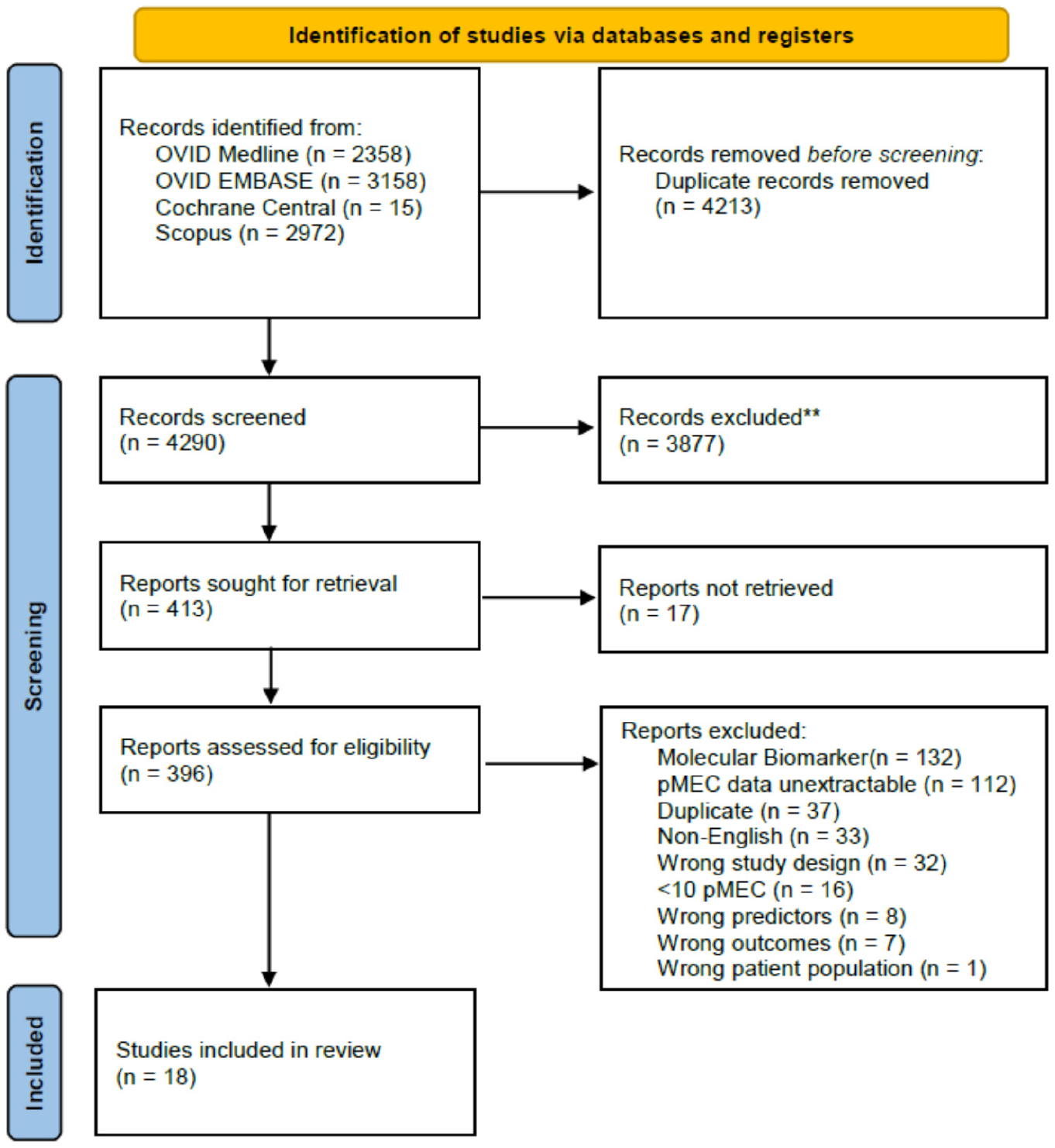
PRISMA flowchart. pMEC, parotid mucoepidermoid carcinoma.
Study Characteristics
The characteristics of the 18 studies are presented in Supplementary Table S1 (available online). Of the 18 studies, all were retrospective cohort studies: 10 (55.6%) from a single institution, 7 (38.9%) from a national database, and 1 (5.6%) from multiple institutions. Half the studies were from the United States (n = 9), with 4 from China. Of the 18 studies, 5 (27.8%) used overall survival (OS) alone as an endpoint; 4 (22.2%), OS and another survival measurement; 3 (16.7%), recurrence-free survival (RFS) alone; 2 (11.1%), determinant survival alone; 1 (5.6%), cancer-specific survival alone; and 1 (5.6%), disease-specific survival (DSS) alone. Other outcomes were survival and relative survival.
Risk of Bias and Quality Assessment
Nine studies were evaluated as low risk (QUIPS score ≤9 points) and 9 as high risk. The average risk of bias score for all studies was 9.7 (high risk), with scores ranging from 7 to 13. The QUIPS score for each study is shown in Supplementary Table S1 (available online).
Of the 14 prognostic factors, 9 (64.3%) had very low-quality evidence, 4 (28.6%) low, 1 (7.1%) moderate, and none had high-quality evidence ( Table 1 ).
GRADE Assessment by Prognostic Factor (18 Studies).
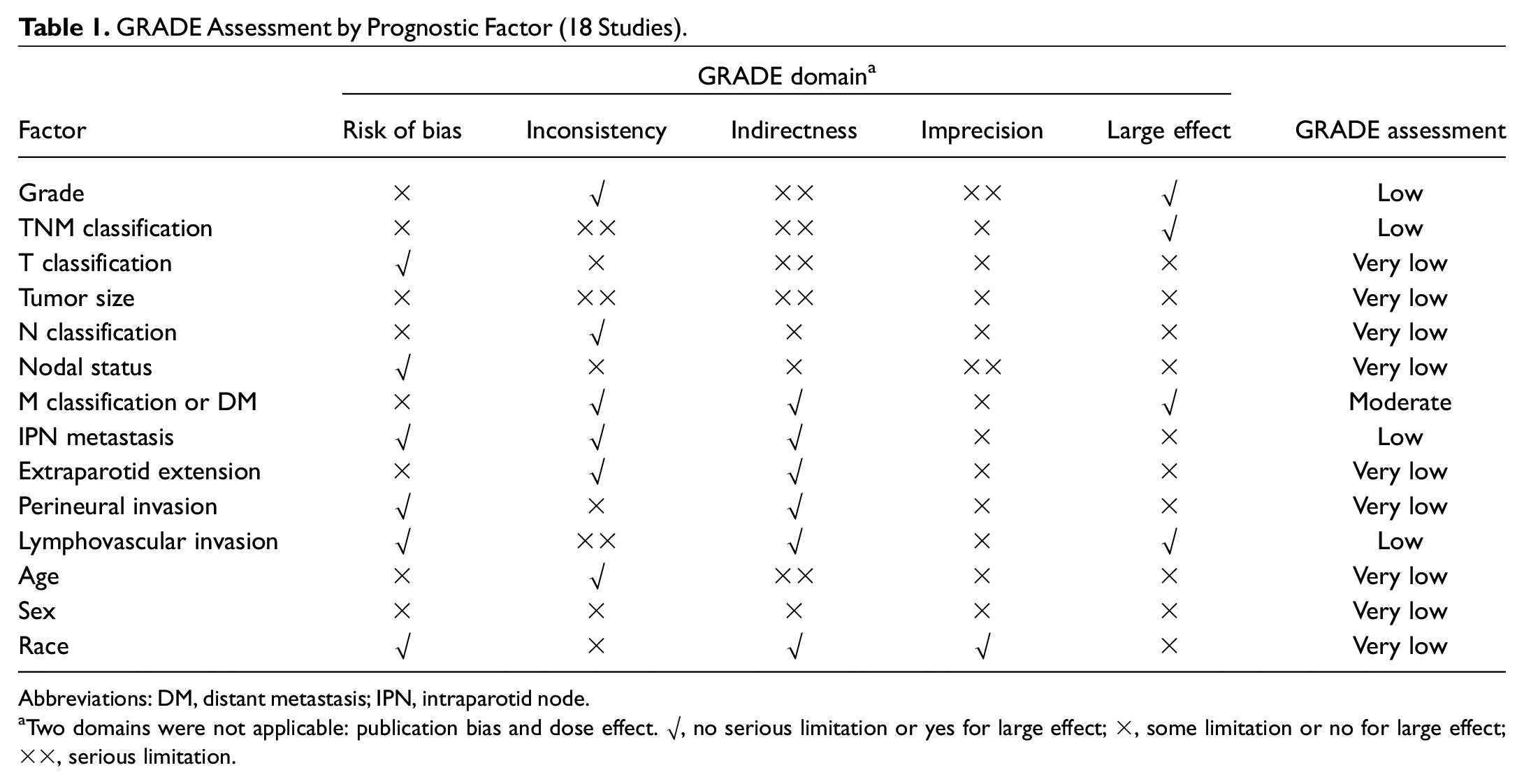
Abbreviations: DM, distant metastasis; IPN, intraparotid node.
Two domains were not applicable: publication bias and dose effect. √, no serious limitation or yes for large effect; ×, some limitation or no for large effect; ××, serious limitation.
Prognostic Factors
Overview
Of the prognostic factors in this study, histologic grade was the most frequently studied, in 15 of the 18 articles, followed by age (n = 11), T classification/tumor size (n = 10), N classification/nodal status (n = 10), sex (n = 9), overall TNM stage (n = 6), intraparotid node (IPN) metastasis (n = 3), perineural invasion (n = 3), extraparotid invasion (n = 2), M classification/distant metastasis (n = 2), lymphovascular invasion (LVI; n = 2), and race (n = 2). Factors examined in just 1 study were not included in our analysis, such as comorbidities, laterality, marital status, muscle invasion, and bone invasion. Additionally, type of treatment was not analyzed as a prognostic factor, as it is dependent on the medical provider.29,30 Prognostic factors that consistently had a significant association with decreased survival consisted of increased histologic grade, nodal status, M classification, IPN metastasis, and age. Prognostic factors that inconsistently reported associations with survival outcomes were overall TNM stage, T classification, and N classification. Prognostic factors with only 1 multivariate analysis were excluded in the quantitative analysis: tumor size, extraparotid extension, perineural invasion, LVI, sex, and race. A summary of the prognostic factors affecting survival outcomes is presented in Table 2 .
Prognostic Factors Affecting Survival Outcomes on Multivariate Analysis.
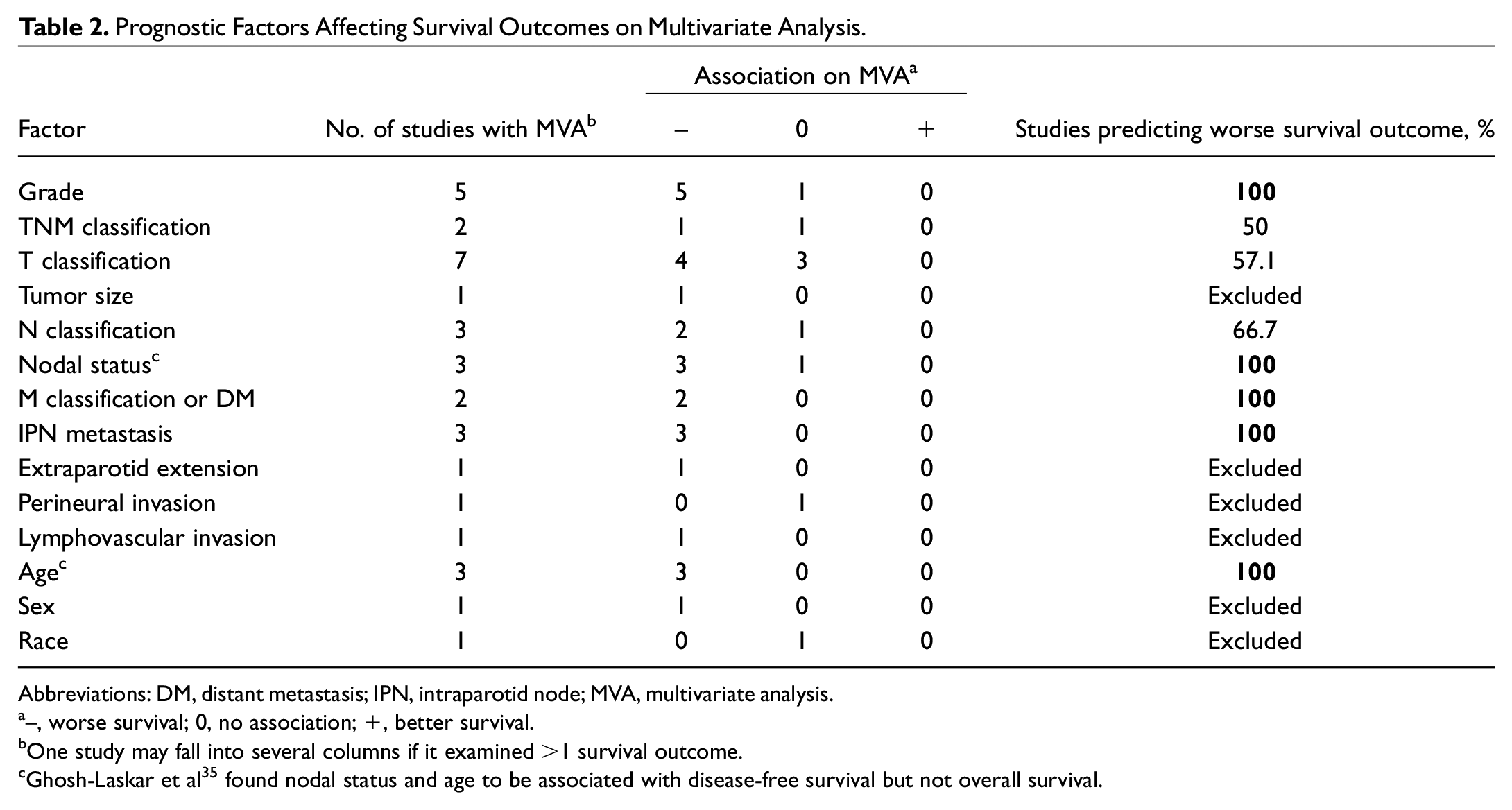
Abbreviations: DM, distant metastasis; IPN, intraparotid node; MVA, multivariate analysis.
–, worse survival; 0, no association; +, better survival.
One study may fall into several columns if it examined >1 survival outcome.
Ghosh-Laskar et al 35 found nodal status and age to be associated with disease-free survival but not overall survival.
Histologic Grade
Twelve studies10,11,27,31-39 reported on the effect of grade on survival, with the majority assessing for OS (n = 5, 41.7%). The system used to assign tumor grade varied among the studies. Yet, it is generally accepted that the designation of parotid MEC as well differentiated or grade 1 is considered low grade, while designations of poorly differentiated or grade 3 are considered high grade. Three studies,33,39,40 all published between 1968 and 1991, used the 2-tier classification of well differentiated/low grade and poorly differentiated/high grade. Eight studies10,11,31,32,34-36,38 categorized tumor grade into a 3-tiered system of low, intermediate, and high grade, with some authors using their own grading system 34 or either the Armed Forces Institute of Pathology or World Health Organization 2017 classification.10,32,38 One study 27 used a 4-tiered grading system: I (well differentiated), II (moderately differentiated), III (poorly differentiated), and IV (anaplastic). However, grades I and II were combined into a low-grade category and grades III and IV into a high-grade category to follow the 2-tiered system.
In 6 studies,10,11,27,32,35,38 higher grade was significantly associated with worse survival, with 5 of these studies10,11,32,35,38 showing grade as an independent prognostic factor: 1 study 11 cited a hazard ratio (HR) of 5.66 (P < .001) on multivariate analysis and 2 studies32,38 reported odds ratios (ORs) ranging from 2.12 to 3.48. The effect sizes are available in Supplementary Table S2 (available online). For OS at each grade level, 3 studies10,31,35 reported on 5-year OS based on the 3-tiered grading system. The studies reported that the 5-year OS ranged from 84% to 100% for low-grade tumors, 80% to 97.5% for intermediate grade, and 52.0% to 73.3% for high grade. The remaining 6 studies10,33,34,36,37,39 provided descriptive data on the survival of patients with parotid MEC depending on grade, and all showed a trend toward worse survival for patients with higher-grade disease.
TNM Stage
Six studies12,13,25,27,32,35 analyzed the effect of TNM stage on survival. Three studies25,32,35 identified a significant association between higher TNM classification and worse survival on univariate analysis. Ghosh-Laskar et al 35 reported on disease-free survival (DFS) and OS. They found that OS was not significant on univariate analysis but DFS was. However, the significance of DFS was lost on multivariate analysis.
T Classification and Tumor Size
Seven studies10,12,13,25,31,32,38 and 2 studies11,34 evaluated T classification and tumor size as prognostic factors of survival, respectively. Of the 7 studies measuring T classification, 4 (57.1%) found that increased T classification was associated with decreased survival on multivariate analysis.10,13,25,31 Of the 2 studies evaluating tumor size, only 1 noted a significant association between larger tumor size (>4 cm) and worse DSS (HR, 1.79; P < .03). 11
N Classification and Nodal Status
Nine studies reported on the effect of N classification or nodal status (positive vs negative) on survival. Six studies10,11,27,32,35,38 evaluated the association of survival with nodal status, 5 (83.3%) of which stated that positive nodal status was significantly associated with poorer survival. However, just 3 of these studies11,32,35 showed nodal status as an independent predictor of survival. Three studies12,13,25 examined the effect of N classification on survival. Of these, 2 found an independent and significant association between N classification and survival.13,25
M Classification and Distant Metastasis at Diagnosis
The presence of distant metastasis at diagnosis was significantly associated with poorer survival in 2 studies.11,25 One study 11 found that the presence of distant metastasis is associated with decreased DSS (HR, 5.80; P < .04). The other study 25 similarly reported that M classification is an independent prognostic factor for OS (HR, 3.104; P = .002) and cancer-specific survival (HR, 3.554; P = .002).
IPN Metastasis
IPN metastasis refers to the group of lymph nodes located within the parenchyma of the parotid gland and is suggested to be the sentinel nodal basin in parotid cancer. 41 This is distinct from the regional lymphadenopathy traditionally included in the staging system of the American Joint Committee on Cancer (eighth edition). 42 Three studies12,32,38 investigated the effect of IPN metastasis on survival outcomes. All 3 showed that positive IPN metastasis is associated with negative RFS on multivariate analysis, with 2 of the 3 multivariate models including nodal status as a confounding variable.12,32 The study periods ranged from 2000 to 2018 and comprised 434 patients with parotid MEC.
Extraparotid Extension
One study 11 examined the effect of extraparotid extension on survival outcomes and showed that the presence of extraparotid extension is associated with worse DSS on multivariate analysis.
Lymphovascular Invasion
Two studies12,38 investigated the effect of LVI on survival outcomes. One study identified LVI as an independent prognostic factor for RFS (OR, 9.576; P < .001). However, Shang et al 12 analyzed the effect of LVI in high-grade parotid MEC and found no association with RFS.
Perineural Invasion
Four studies12,31,32,38 evaluated the effect of perineural invasion on survival outcomes. Only 1 study 38 (n = 1/4, 25%) had a significant association between perineural invasion and worse RFS. However, this association was lost on multivariate analysis.
Age, Sex, and Race
Nine studies11-13,31,32,34,36,38,43 examined the effect of age on survival, and 4 studies11,13,31,43 (44.4%) found that older age was associated with decreased survival, with 3 of these studies also showing that age is an independent prognostic factor.11,13,31 Two studies34,36 showed similar trends without conducting a formal analysis, while 2 (22%) identified no association.32,38 The most common age categorization used is <50 or >50 years, with 3 of the 9 (33.3%) studies32,36,38 examining age as a prognostic factor based on this categorization.
Eight studies11-13,32,34,36,38,43 examined the effect of sex on survival, and 3 studies11,13,43 (37.5%) suggested that sex is a significant prognostic factor of survival, with females having better survival than males. Of these 3 studies, though, only 1 study 13 evaluated sex as an independent prognostic factor of survival (HR, 0.83; P = .008).
One study 11 examined the effect of race on DSS and found no association on multivariate analysis.
Discussion
This comprehensive review identified 18 studies that analyzed the effect of clinicopathologic factors on survival outcomes in patients with MEC published from 1968 to 2020. Fourteen clinicopathologic factors were identified. Prognostic factors that consistently had a significant association with decreased survival were increased histologic grade, nodal status, M classification, IPN metastasis, and age, while TNM stage, T classification, and N classification were inconsistently associated with survival outcomes.
In this review, high tumor grade was the most frequently studied independent prognostic factor on survival. The effect of grade on survival for patients with parotid MEC is similar to that of MEC elsewhere in the head and neck.44-46 Although grade consistently predicted survival, there is a large degree of variability in the grading systems used, such as the initial 2-tiered classification 47 or more recent 3-tiered system (low, intermediate, and high grade)34,48 and 4-tiered grading system (I [well differentiated], II [moderately differentiated], III [poorly differentiated], and IV [anaplastic]).13,25 In this review, 3 of the 12 studies that reported on grade used a 2-tiered scheme in their analysis (risk of bias, 11), while 8 studies categorized tumor grade into the 3-tiered system (risk of bias, 9.5) and 1 study used a 4-tiered system (risk of bias, 10). Variability with the grading system used in research studies poses a significant challenge in synthesizing the available data and may lead to clinical ambiguity. Furthermore, there is variability in categorizing intermediate-grade malignancy, as some classify it as low-grade carcinoma and others as high grade. Therefore, additional work is needed to develop a unified, central grading system for MEC to standardize the language and understanding surrounding this entity.
In terms of the individual components of the TNM classification system, T classification was examined the most with 7 studies, followed by N classification with 3 studies and M classification with 2 studies. The majority of studies with multivariable analysis that reported on T classification (n = 4/7, 57%), N (n = 2/3, 67%), and M (n = 2/2, 100%) found that these variables were independent prognostic factors of survival outcomes. Among the 4 studies that investigated the role of TNM classification as a prognostic factor, just 1 showed a significant association between TNM and survival on multivariate analysis. This finding is in contrast to the consistent relationship between grade and survival outcomes identified in this study. This may be due to the fact that the TNM classification system primarily depends on the anatomic involvement of the cancer to predict survival outcomes; as such, important factors such as tumor pathology and biological markers are not considered. Another possibility is that the prognostic significance of the TNM classification system may be more evident within a cancer grade, rather than between grades. Therefore, more research is needed examining the effect of TNM classification on parotid MEC survival, while controlling for confounders such as treatment, IPN metastasis, and extraparotid invasion. Additionally, future research should focus on delineating the effect of TNM classification on survival based on the specific outcome measure used. Among the studies, TNM classification was associated with OS and cancer-specific survival outcomes on univariate analysis. However, the associations between TNM classification and these outcome measures were not analyzed on multivariate analysis.
The association between sex and survival outcomes in patients with parotid MEC is indetermined among the studies. Yet, previous studies on head and neck malignancies noted that female sex was associated with better survival outcomes.46,49,50 Several theories on the reason behind the difference in survival based on sex have been proposed: differences in health care access and utilization, with increased health care–seeking behaviors among females vs males49,51-53; biological factors such as the presence of female sex hormones, suggested as a protective factor against distant metastasis49,54; and genetic differences such as having double the X chromosomes, which plays a role in immune defenses.49,55
Several limitations were identified in this study. First, there was significant heterogeneity with the survival outcomes reported. This precluded the possibility of conducting a meta-analysis. Second, there is considerable heterogeneity with regard to the treatment protocols across the studies. Although all studies involved surgery, adjuvant therapy ranged from chemotherapy to radiation therapy or both. Furthermore, some studies investigated novel therapies, such as surgery with 125I seed brachytherapy for parotid MEC. 31 While some studies included treatment as a variable in multivariable analysis,24,25,32 others did not. 13 Last, the studies were limited by a high risk of bias and largely low quality of evidence. As such, the conclusions drawn from this systematic review are negatively affected.
Conclusion
Increased histologic grade, nodal status, M classification, intraparotid metastasis, and age were associated with worse survival in patients with parotid MEC. These prognostic factors should be incorporated in the clinical evaluation, patient counseling, and management strategy for patients with parotid MEC.
Supplemental Material
sj-docx-1-oto-10.1177_01945998221086845 – Supplemental material for Clinicopathological Predictors of Survival for Parotid Mucoepidermoid Carcinoma: A Systematic Review
Supplemental material, sj-docx-1-oto-10.1177_01945998221086845 for Clinicopathological Predictors of Survival for Parotid Mucoepidermoid Carcinoma: A Systematic Review by Emily YiQin Cheng, Joo Hyun Kim, Elysia M. Grose, Justine Philteos, Marc Levin, John de Almeida and David Goldstein in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-2-oto-10.1177_01945998221086845 – Supplemental material for Clinicopathological Predictors of Survival for Parotid Mucoepidermoid Carcinoma: A Systematic Review
Supplemental material, sj-docx-2-oto-10.1177_01945998221086845 for Clinicopathological Predictors of Survival for Parotid Mucoepidermoid Carcinoma: A Systematic Review by Emily YiQin Cheng, Joo Hyun Kim, Elysia M. Grose, Justine Philteos, Marc Levin, John de Almeida and David Goldstein in Otolaryngology–Head and Neck Surgery
Footnotes
Acknowledgements
We thank Kaitlin Fuller, MLIS, health science librarian at the University of Toronto, for her help and expertise with the search strategy.
This article was presented at the Canadian Society of Otolaryngology–Head and Neck Surgery 75th Annual Meeting; September 17-19, 2021 (virtual).
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.