
Abstract
Background:
Primary care nurses play a critical role in team-based primary care in Canada. Despite their growing presence in interdisciplinary teams, comprehensive workforce data are limited.
Objective:
To describe demographic, employment, work setting, and patient population characteristics of primary care nurses across Canada.
Methods:
We conducted an online cross-sectional survey of registered nurses in primary care across Canada. The survey was informed by the structure, process, and outcome variables of the Nursing Role Effectiveness Model and previous project findings. We analyzed data using frequency distributions and measures of central tendency, focusing on 6 provinces with sufficient sample sizes: British Columbia, Alberta, Ontario, Quebec, Nova Scotia, and Newfoundland and Labrador.
Results:
Of 1092 eligible responses, most were women (94.8%), held a bachelor’s degree (88.2%), were unionized (73.7%), and worked in Ontario or Quebec (74.6%). Most were employed by regional health authorities (64.4%), worked full-time (81.4%), and were paid via salary (49.5%) or hourly wage (50.1%). While most worked in clinics (85.4%), others provided care in homes, schools, and community programs. Clinic funding models varied provincially, with block/global funding most common in British Columbia (34.2%), Quebec (54.0%), and Newfoundland and Labrador (61.5%), while Alberta primarily relied on billings (28.9%) and Ontario on both capitation (28.7%) and block/global funding (28.7%). Provincial variations were also observed in unionization, years of experience, and patient populations.
Conclusions:
This study provides the most comprehensive portrait of primary care nurses in Canada to date. Findings highlight provincial variations, offering valuable insights for workforce planning, policy development, and future research.
Introduction
Primary care nurse (PCN) is the job title often used to refer to registered nurses (RNs) who practice in primary care settings. 1 In Canada, each province and territory is responsible for the organization and delivery of health care. Primary care is usually the first point of contact in the healthcare system and involves the delivery of comprehensive, accessible, longitudinal, and coordinated patient-centered care. 2 Over the last 25 years, Canadian provinces and territories have introduced primary care payment and practice model reforms that have resulted in a variety of organizational structures and practice models, with considerable variability across jurisdictions.3-5 Payment-related reforms include changes to funding models that move away from service activity (eg, fee-for-service) to block funding (ie, lump sum) based on programmatic elements to population served (ie, capitation), or a mix of the 3 (ie, some combination of service activity, population, and/or lump sum). Practice model reforms have created and expanded team-based care, and PCNs now form the core of interprofessional primary care teams across many jurisdictions in Canada.6,7 PCNs provide a broad range of health services to diverse populations, including but not limited to: triage; preventative screening; prenatal, well-baby, and well-woman care; routine immunizations, health education, and self-management support; chronic disease management; patient and system navigation; mental health and addictions support; treatment of acute illnesses; and care coordination and implementation of targeted primary care programs.6-12 Research suggests that team-based models of primary care that include PCNs are well-positioned to improve access to and continuity of care, promote health equity, reduce health disparities, enhance patient outcomes, and increase cost-effectiveness.6,13-18 Systematic reviews have found that PCNs deliver appropriate, high-quality primary care.19,20
Limited Information on Primary Care Nurses
Despite the greater incorporation of PCNs in primary care, there is relatively little information available on this workforce. The Canadian Institutes of Health Information (CIHI) compiles Canadian nursing workforce data; however, CIHI includes PCNs with other RNs and nurse practitioners (NPs) working in a variety of non-hospital-based settings such as mental health and home care agencies, schools, prisons, community health centers and outpost nursing stations, public health organizations, and physician’s offices.21,22 Much of the available data on PCNs in Canada stem from qualitative studies and local surveys (eg, limited to one province).14,23-27 Moreover, the limited research available suggests that PCN integration into primary care settings is sub-optimal, resulting in role ambiguity and the underutilization of their scope of practice.24,28,29 Data from a recent national survey of rural and remote nurses, including NPs, RNs, and licensed practical nurses (LPNs), further highlight this role ambiguity and variability, as findings revealed that PCNs dedicated solely to primary care reported greater educational preparation and job resources but experienced inconsistencies in scope of practice and role utilization across settings. 30
Purpose
Using data from a cross-sectional national survey, we describe the demographic, employment, work setting, and patient population characteristics of PCNs in Canada. Our portrait of PCNs provides much-needed information on this important and growing workforce in primary care and can serve as the basis for a more detailed exploration of the relationship between demographic, employment, work setting, and patient population characteristics of PCNs and outcomes of team-based primary care.
Methods
As part of a mixed methods study, 31 we conducted an online cross-sectional survey via Qualtrics (Qualtrics, Provo, UT, USA) examining demographic, employment, work setting, and patient population characteristics of PCNs across Canada. We included survey respondents who reported practicing as an RN in a primary care setting, which includes family physician offices, patient homes, community health centers, university and school-based health centers, and other community-based settings, such as shelters. We excluded PCNs who worked in primarily administrative, teaching, or research positions; in public health, home care, hospital-based ambulatory care, or inpatient units/clinics; or in northern or remote community health centers/nursing stations (which generally require nurses to have advanced training).
The survey was available from October 2023 to March 2024. To recruit participants, the Canadian Family Practice Nurses Association, its affiliated provincial groups (eg, Primary Care Nurses of Ontario), and provincial nursing regulatory colleges (eg, College of Registered Nurses of Newfoundland and Labrador, British Columbia College of Nurses and Midwives) distributed study invitations with links to the survey to their members through various communication platforms, such as email newsletters, social media, and website postings. In Quebec, we emailed PCNs from the Ordre des infirmières et des infirmiers du Québec membership list. Members of the research team also asked their professional networks to share the study invitation. For email communications, we (or the professional associations sending emails on our behalf) used a modified Dillman approach 32 and sent reminders at 2 and 4 weeks after an initial email study invitation had been sent. All emails contained information about the study and links to both French and English versions of the survey. We offered a draw for 3 gift cards as an incentive to encourage survey participation.
We based survey questions on the structure, process, and outcome variables of the Nursing Role Effectiveness Model,33,34 findings from previous stages of the project (ie, document analysis, qualitative interviews), and consultations with research team members, which include experts in primary care research, nursing science, and primary care nursing roles. The survey gathered structure (eg, demographics, professional preparation, work setting and patient population characteristics, and contextual factors), process (eg, nursing activities, team effectiveness), and outcome (co-management) variables. For the current paper, we focused primarily on the structural elements contained in the data to explore the sample in depth. Future publications will examine the relationship between the structural variables and process and outcome variables. Both French and English versions of the survey were pre-tested; we made wording changes to improve question and response clarity and to ensure that both language versions of the survey were reflective of the same concepts.
We took a number of steps to ensure that the survey was completed by actual PCNs rather than automated “bots.”35,36 We reviewed the time to complete the survey, looked for inconsistent answers (eg, if total number of years practicing as a PCN was more than years practicing as an RN), included a question that purposely requested specific or nonsensical responses, added a Captcha verification question to the first page of the survey, and enabled fraud detection settings within the Qualtrics software to screen for potentially fraudulent responses.
Using SPSS software (v. 28; IBM Corp., Armonk, NY, USA), we merged data from the French and English surveys into a single file. We used frequencies and proportions (for categorical variables), and measures of central tendency (for continuous variables) to describe the demographic, employment, work setting, and patient population characteristics of eligible PCNs across Canada. We repeated the analysis for PCNs from 6 provinces (British Columbia, Alberta, Ontario, Quebec, Nova Scotia, and Newfoundland and Labrador) where there was sufficient sample size (minimum 28). Some nurses may work in more than one clinic or setting. We have noted in the table legends where nurses could indicate multiple responses. For other variables relating to clinics or settings, we asked nurses to refer to where they spent the most hours working in a typical week. To account for missing data, analyses for each variable were based only on respondents who provided a valid answer, and percentages were calculated relative to the number of responses for that specific item. Incomplete responses were treated as missing data and not included in the total sample size.
We obtained ethics approval from the relevant ethics boards in each study region. The survey included a letter of information and consent; PCNs implied consent by initiating the survey. We used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist as a guide to inform the reporting of this study.
Results
Of the 1234 respondents, 1092 met the eligibility criteria (Figure 1) and were included in the analysis, although not all eligible PCNs answered all survey questions. The majority of PCNs in our sample were women (94.8%), held a bachelor’s degree in nursing (88.2%), were part of a union (73.7%), and worked in Ontario or Quebec (74.6%) (Table 1). The majority of PCNs worked in clinics funded by the provincial government (61.4%), were employed by a regional health authority/organization (64.4%), worked full-time (81.4%), and were paid by either salary (49.5%) or hourly wage (50.1%). Over half of PCNs worked in an urban center (51.2%) and provided care to a general patient population (64.9%). While most worked in a clinic-based setting (85.4%), PCNs also worked in patients’ homes, schools, and community outreach settings (eg, shelters).
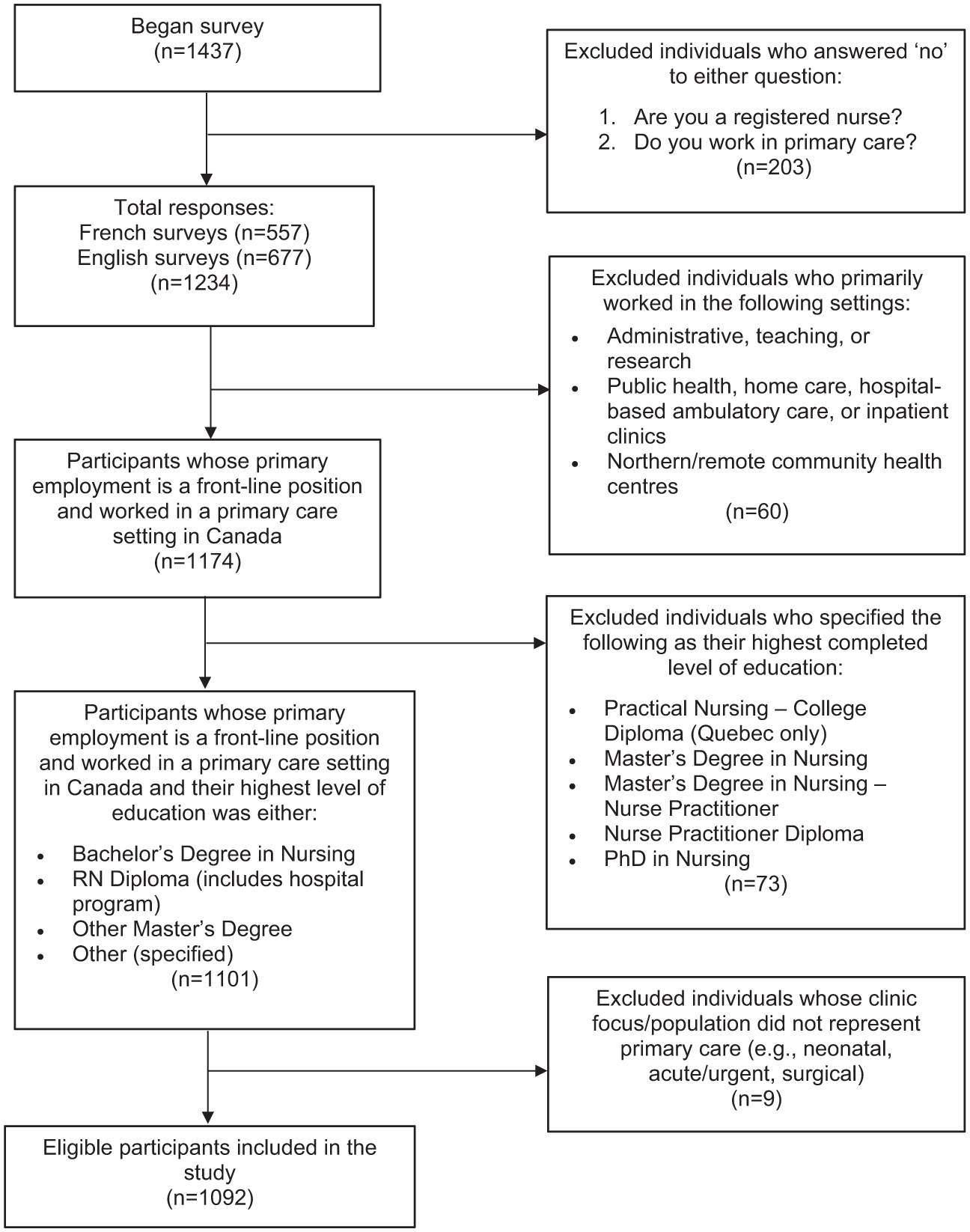
Derivation of study sample.
Demographic and Professional Characteristics of PCNs in Canada and in Select Canadian Provinces.
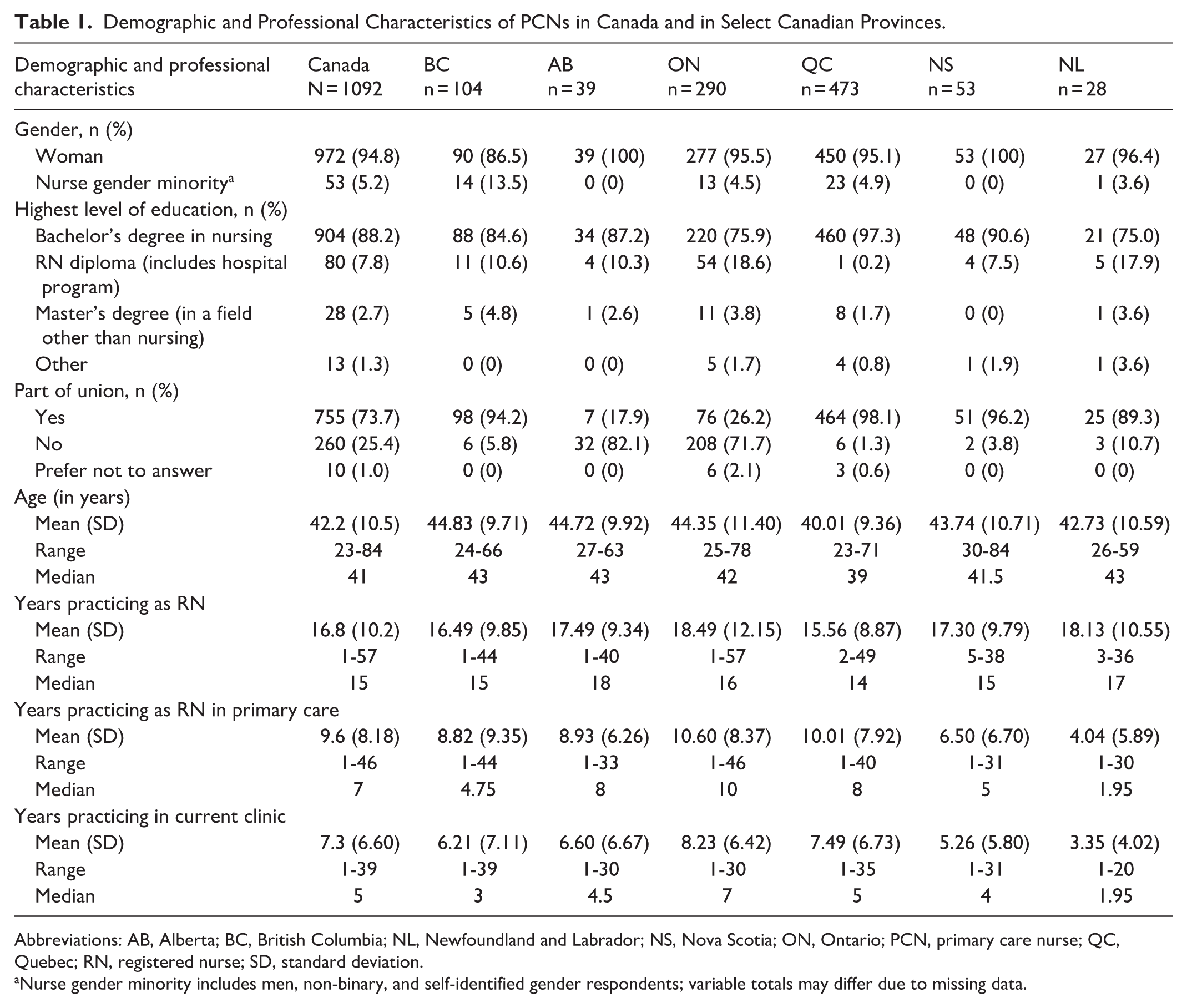
Abbreviations: AB, Alberta; BC, British Columbia; NL, Newfoundland and Labrador; NS, Nova Scotia; ON, Ontario; PCN, primary care nurse; QC, Quebec; RN, registered nurse; SD, standard deviation.
Nurse gender minority includes men, non-binary, and self-identified gender respondents; variable totals may differ due to missing data.
Examining PCNs at a provincial level revealed variation in employment, funding model and arrangement, source of payment, patient population, and work setting (ie, the location or environment in which nurses deliver primary care services such as clinic, patient home, hospital, etc.). The majority of PCNs in British Columbia (94.2%), Quebec (98.1%), Nova Scotia (96.2%), and Newfoundland and Labrador (89.3%) belonged to a labor union, compared to a minority of PCNs in Ontario (26.2%) and Alberta (17.9%). PCNs in Newfoundland and Labrador reported the lowest mean years practicing in primary care (4.0 years), and in their current clinic (3.4 years), while PCNs in Ontario reported the highest mean years practicing in primary care (10.6 years) and in their current clinic (8.2 years).
Clinic funding arrangement (the basis on which funding was determined) varied between provinces, with block/global funding making up the most commonly reported funding arrangement for PCNs in British Columbia (34.1%), Quebec (54.0%), and Newfoundland and Labrador (61.5%) (Table 2). PCNs in Alberta reported physician billings as the most common clinic funding arrangement (28.9%), while PCNs in Ontario most frequently reported capitation (28.7%) and block/global funding (28.7%). In Nova Scotia, a blended funding model was the most commonly reported clinic funding arrangement (46.2%). In all provinces, a substantial proportion of PCNs were unsure or did not know their clinic’s funding arrangement (13.5%-31.9%) or source of funding (19.2%-32.2%). A sizeable number of PCNs were unsure or gave incorrect answers with regard to clinic funding arrangements or source of funding (Supplemental Table 1).
Funding and Compensation Characteristics of PCNs in Canada and in Select Canadian Provinces.
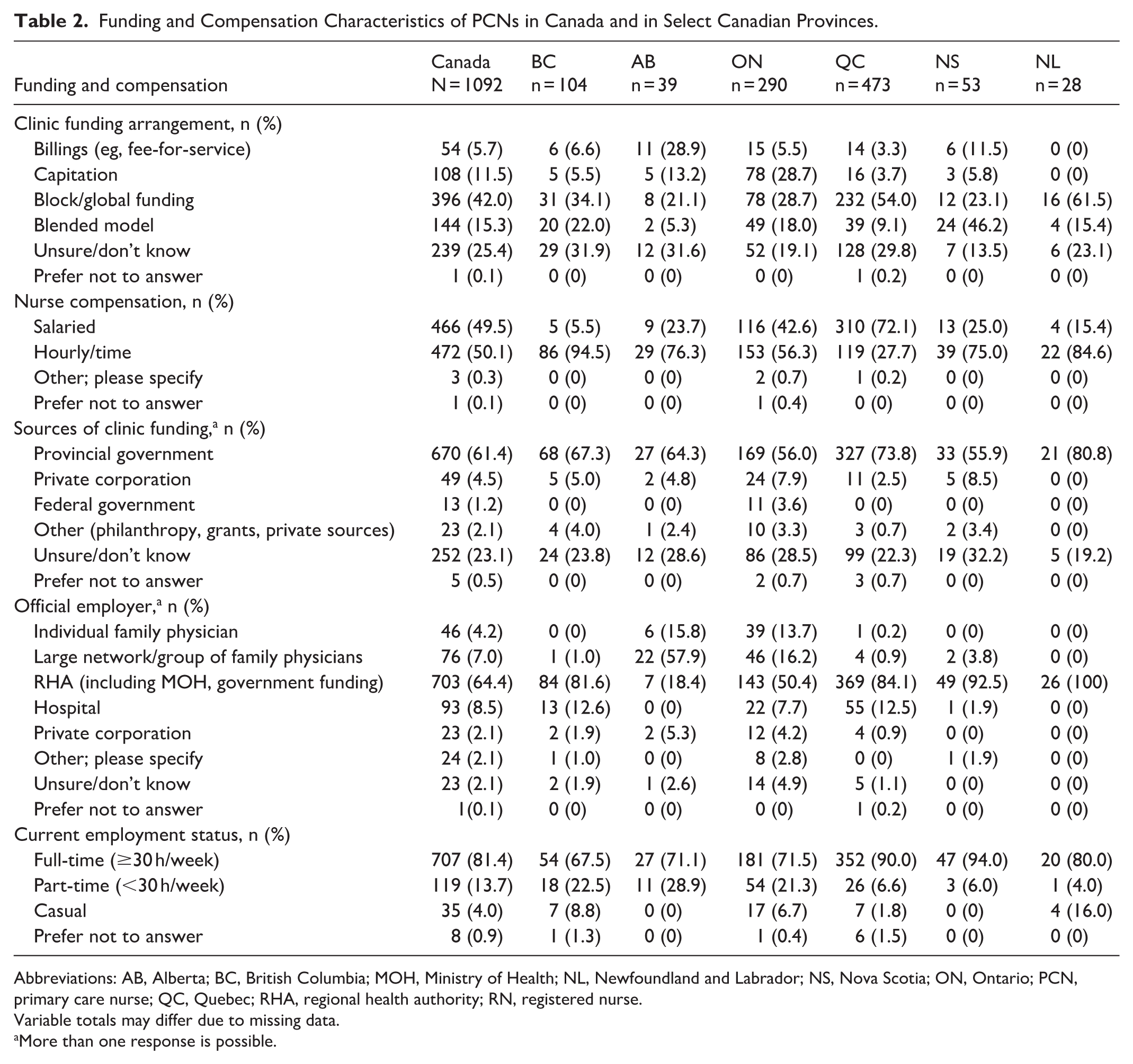
Abbreviations: AB, Alberta; BC, British Columbia; MOH, Ministry of Health; NL, Newfoundland and Labrador; NS, Nova Scotia; ON, Ontario; PCN, primary care nurse; QC, Quebec; RHA, regional health authority; RN, registered nurse.
Variable totals may differ due to missing data.
More than one response is possible.
PCNs were most commonly paid by hourly wage in all provinces except Quebec, where the majority of PCNs were paid by salary (72.1%). In all selected provinces, most PCNs reported that their clinic was funded by the provincial government. The majority of PCNs in British Columbia (81.6%), Ontario (50.4%), Quebec (84.1%), Nova Scotia (92.5%), and Newfoundland and Labrador (100%) reported that their official employer was a regional health authority or equivalent organization. By contrast, the majority of PCNs in Alberta (57.9%) were employed by a large network or group of family physicians.
A sizeable number of PCNs provided care to focused patient populations in British Columbia (66.3%) and Quebec (66.6%) (Table 3). PCNs in Alberta (97.3%) and Nova Scotia (100%) reported working almost exclusively in clinics, patient homes, and hospitals, while PCNs in British Columbia, Ontario, Quebec, and Newfoundland and Labrador reported working in other settings (eg, long-term care, schools, community outreach). PCNs in Ontario and Nova Scotia worked with a larger number of physicians than PCNs in the other selected provinces (based on visual inspection).
Work Setting and Patient Population Characteristics of PCNs in Canada and in Select Canadian Provinces.
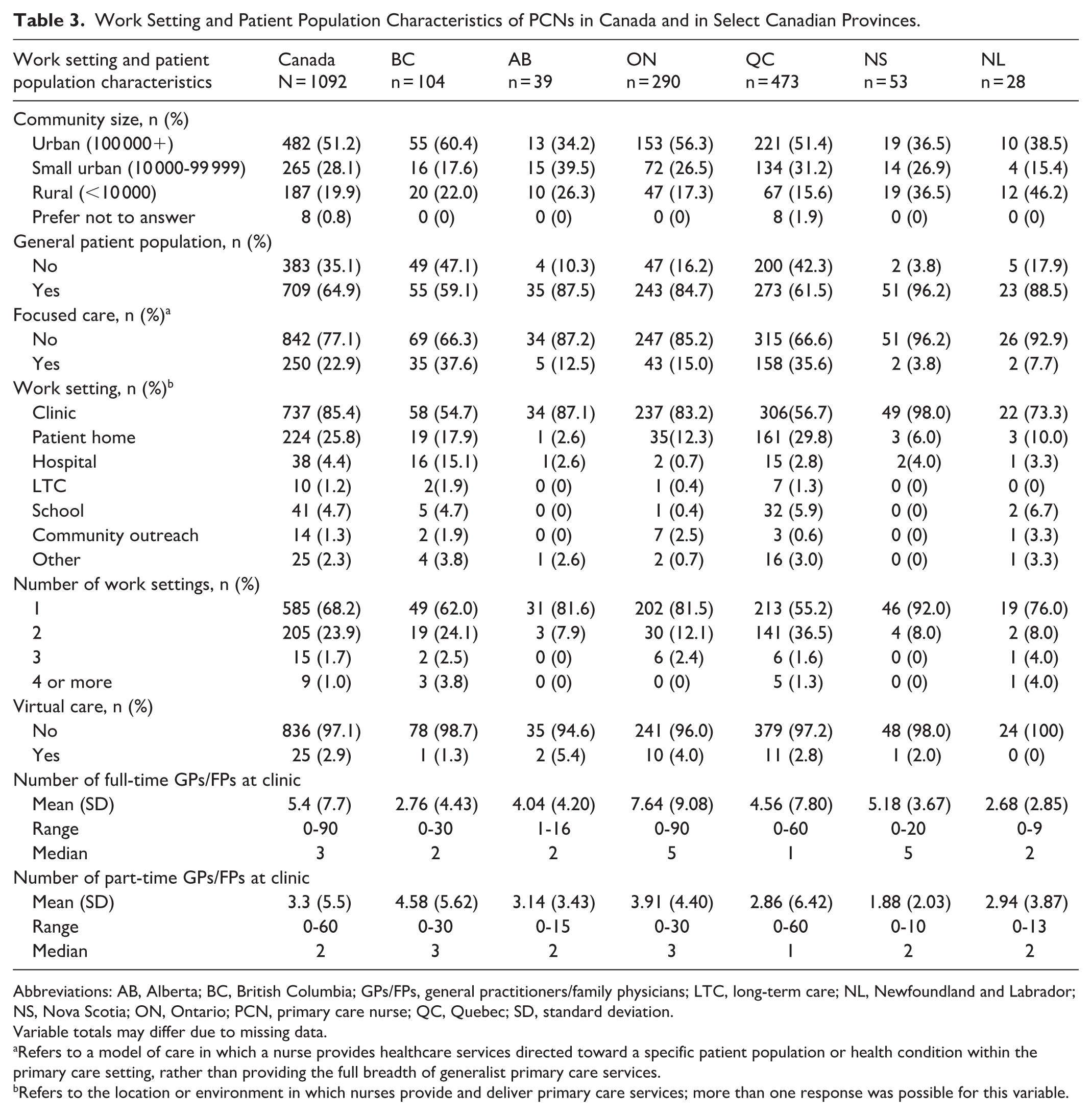
Abbreviations: AB, Alberta; BC, British Columbia; GPs/FPs, general practitioners/family physicians; LTC, long-term care; NL, Newfoundland and Labrador; NS, Nova Scotia; ON, Ontario; PCN, primary care nurse; QC, Quebec; SD, standard deviation.
Variable totals may differ due to missing data.
Refers to a model of care in which a nurse provides healthcare services directed toward a specific patient population or health condition within the primary care setting, rather than providing the full breadth of generalist primary care services.
Refers to the location or environment in which nurses provide and deliver primary care services; more than one response was possible for this variable.
The largest numbers of PCNs worked in health authority owned/operated Community Health Centers (43.3%) or Urgent and Primary Care Centers (32.7%) in British Columbia, Primary Care Networks (94.9%) in Alberta, Family Health Teams (53.4%) in Ontario, Centres locaux de services communautaires (Local Community Services Centers) (83.1%) in Quebec, Collaborative Family Practices (84.9%) in Nova Scotia, and Family Care Teams/Collaborative Team Clinics (60.7%) in Newfoundland and Labrador (Table 4).
Primary Care Model Where Primary Care Nurses Worked, by Province. a
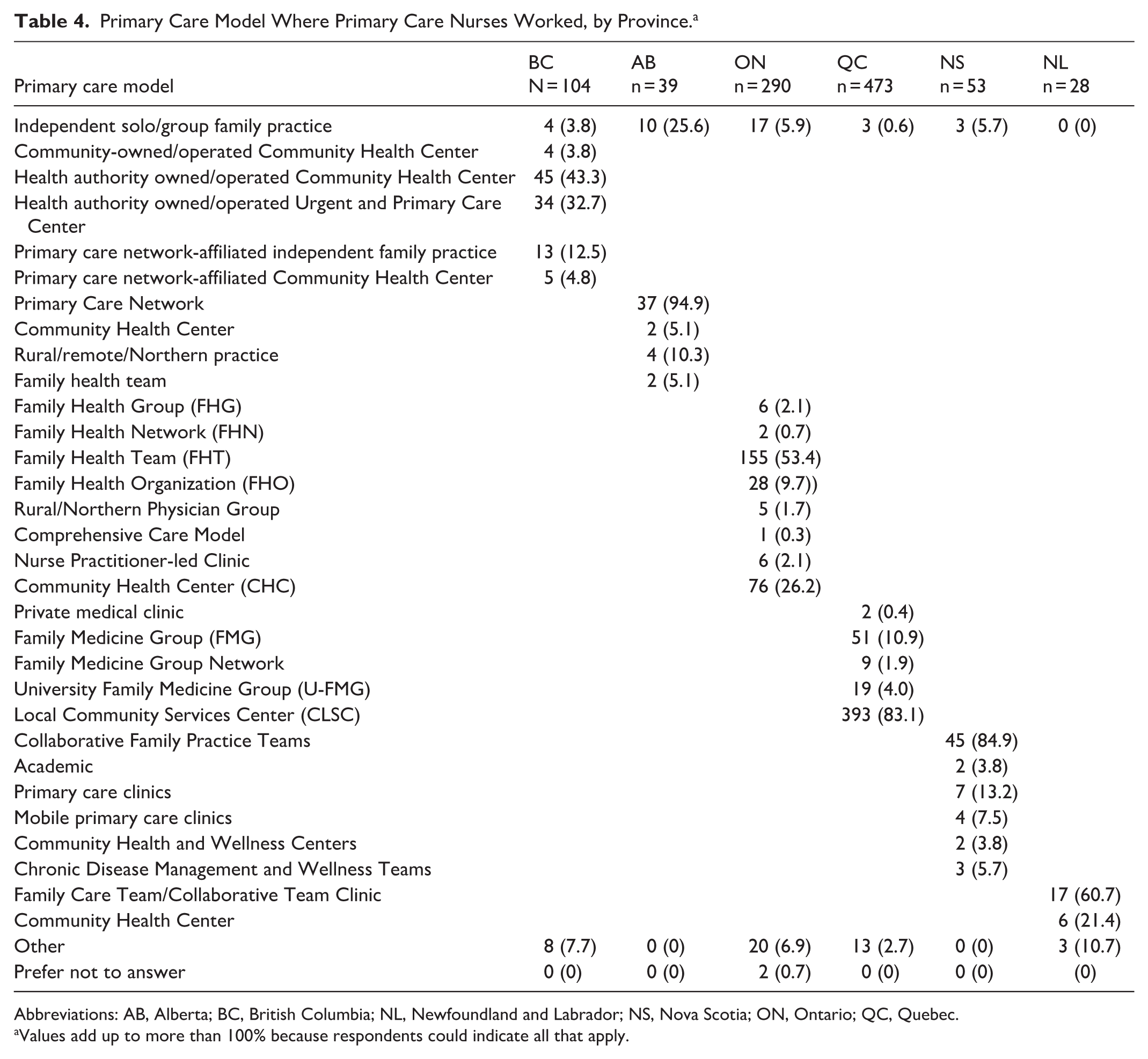
Abbreviations: AB, Alberta; BC, British Columbia; NL, Newfoundland and Labrador; NS, Nova Scotia; ON, Ontario; QC, Quebec.
Values add up to more than 100% because respondents could indicate all that apply.
Discussion
To our knowledge, this is the most comprehensive portrait of PCNs in Canada. The demographic profile of PCNs in our study, however, is consistent with provincial studies of PCNs across Canada. For example, the 58 PCNs in Al Sayah et al’s 25 Alberta-based qualitative study were predominantly women (98.3%), held bachelor’s degrees in nursing (75.0%), were a mean of 48 years old, and had 17 years of nursing experience, of which 6 years were in primary care. In Nova Scotia, Todd et al’s 27 survey of 41 PCNs reported that 95% were women who had an average of 13 years of primary care nursing experience. Similarly, Poitras et al 26 surveyed 266 PCNs working in Quebec’s family medicine groups and found that respondents were composed predominantly of women (97.7%), were working full-time (72.2%), held a bachelor’s degree (98.0%), and were an average of 39.8 years old with 16.7 years of nursing experience (6.3 years in the family medicine group). Similar to these studies, we found that PCNs are mostly mid-career women who have spent roughly half their nursing career in primary care. The majority of PCNs in Canada worked in Ontario or Quebec, a likely reflection of the 2 provinces’ large populations and long history of team-based practice model reforms.
This study provides new information on the employment conditions of PCNs in Canada, addressing a gap identified in a recent environmental scan conducted as part of our larger mixed methods project that found relatively little information on PCNs in team-based models of primary care in Canada. 37 Consistent with the data available on employers of PCNs in team-based models of primary care, most PCNs in British Columbia, Quebec, Nova Scotia, and Newfoundland and Labrador are employed by regional health authorities, while PCNs in Alberta and Ontario are employed by regional health authorities or physicians, depending on the specific funding model. 38 While the majority of PCNs in the survey were able to report individual-level employment data (eg, membership in a union, basis of compensation, employer), over one-quarter of respondents were unsure, preferred not to answer, or gave incorrect answers when asked about clinic funding arrangements or the source of funding. This finding suggests that self-reported data should be used cautiously to examine the relationship between clinic-level funding and performance, including nurse-level outcomes. These data also indicate that many PCNs ultimately misunderstand how the clinic in which they work is financed, which, to some extent, reduces the power of their advocacy and leadership in the organization of primary care. Future research should examine how different team, funding, and employment models affect PCNs’ integration into primary care settings, role ambiguity, and scopes of practice.
Our survey also sheds light on the settings in which PCNs work. While the majority of PCNs work in a clinic, many also provide home visits as well as services in other community and institutional settings. Some settings may differ from what is traditionally thought of as a primary care setting and may therefore be inadvertently overlooked in large-scale planning and policy. In addition, few PCNs reported providing virtual care.
Our study highlights the need for regular data collection about the primary care workforce. The survey findings fill a critical gap in Canadian health workforce data. Canada does not conduct regular workforce surveys in primary care that include or focus on PCNs. Up-to-date data on PCNs are needed for workforce planning and evaluation of primary care reforms, including expansion of team-based care. Some countries gather data on PCNs through annual health worker surveys or during the annual licensure renewal and registration process.18,21,38 Given that primary care forms a relatively small proportion of the overall workforce of non-physician health providers, gathering data through regular universal processes ensures that data are collected on these providers who would otherwise be difficult to identify and reach. Our survey instrument serves as a template for annual data collection; the findings highlight which data can be reliably collected from PCNs about primary care organizational characteristics.
Limitations
We are unable to assess response rate and representativeness given that there is no registry of PCNs across Canada. Moreover, despite an overall large sample size, analyses are limited by province-specific samples. Given the province-specific nature of primary care models, the smaller provincial samples may limit our ability to examine and/or compare specific payment and practice models. Like all self-report data, the survey may also suffer from recall bias. Notably, some variables have a high proportion of missing data or unusable responses that limit the utility of future analyses.
Conclusions
Using survey data, we have created the most comprehensive portrait of PCNs in Canada to date. The majority of PCNs in Canada were women with bachelor’s degrees in nursing who worked in Ontario or Quebec (2 populous provinces with long histories of team-based practice model reforms). The majority of PCNs work full-time in clinics funded by the provincial government, belong to unions, and are employed by a regional health authority/organization. While most PCNs work in a clinic setting, they also work in patients’ homes, schools, and community outreach settings (eg, shelters). There is provincial-level variation in employment, funding arrangements, payment source, patient population, and work settings, reflecting different approaches to primary care funding and practice models. These data provide important information regarding the characteristics, employment, work setting, and patient population of the primary care nursing workforce in Canada and highlight the need for regular and consistent collection of provincial primary care workforce data to inform planning and policy. Future research should consider the diversity of PCN work settings and the variability in employment and funding models on role integration and scope of practice. Having a clear understanding of these factors is necessary to optimize the deployment of PCNs and strengthen team-based primary care across Canada.
Supplemental Material
sj-pdf-1-wjn-10.1177_01939459251400048 – Supplemental material for A Portrait of Registered Nurses in Primary Care in Canada: A Cross-Sectional Survey
Supplemental material, sj-pdf-1-wjn-10.1177_01939459251400048 for A Portrait of Registered Nurses in Primary Care in Canada: A Cross-Sectional Survey by Maria Mathews, Jennifer Phung, Lindsay Hedden, Julia Lukewich, Dana Ryan, Toni Leamon, Deanne Curnew, Marie-Eve Poitras, Cloé Beaulieu, Leslie Meredith, Sarah Spencer and Nelly D. Oelke in Western Journal of Nursing Research
Footnotes
Ethical Considerations
Ethics for the cross-sectional survey portion of this study was reviewed and approved by the Newfoundland and Labrador Health Research Ethics Board (file no. 20240589). Ethics for the larger project was obtained from the Research Ethics British Columbia (No. H21‑03577); Nova Scotia Health Authority Research Ethics Board (File No. 1027833); Western University Research Ethics Board (Project ID 120004); and Comité central d’éthique de la recherche (CCER‑22‑23).
Consent to Participate
All participants were provided with a letter of information and a link to initiate the survey. If the participant proceeded with completing the survey, it represented the participant’s informed consent to participate.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research (CIHR) under grant no. 436627.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets analyzed for this study are not publicly available due to the need to maintain participant confidentiality; however, a portion of these data may be available from the corresponding author on reasonable request.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.