
Abstract
Background:
Virtual care is increasingly used to improve access to primary care. However, the roles of primary care nurses (ie, nurse practitioners [NPs], registered nurses [RNs], licensed practical nurses [LPNs]) in virtual care delivery are not clearly defined. A better understanding of these roles can improve their integration and optimization in virtual primary care delivery and the availability and quality of virtual primary care.
Objectives:
The purpose of this scoping review was to identify and map the international literature on nurses’ roles in virtual care delivery in primary care.
Methods:
Following the Joanna Briggs Institute methodology, we searched academic databases for published literature and webpages for gray literature sources. We included studies that described the roles of nurses (NPs, RNs, LPNs) in providing virtual primary care. We excluded studies that focused on nurses’ use of digital technologies without nurse-patient interaction.
Results:
After screening potential sources, we included 34 sources from countries such as the United Kingdom, Canada, the United States, Australia, and Sweden. Most were specific to RNs (n = 12) or did not specify a regulatory designation (n = 12). Primary care nurse roles in virtual care were mostly related to care coordination, chronic disease management, and triage and assessment using various modalities (eg, telephone and video). Many factors influenced nurses’ roles in virtual care, such as patient/nurse experiences, training/support, access to resources/equipment, and ethical/privacy concerns.
Conclusions:
Nurses are well-positioned to provide virtual care based on their diverse roles across primary care settings; however, their roles could be better optimized to improve primary care access and quality.
Introduction
Virtual care involves the use of information communication technologies (such as telephone or video) in interactions between patients and/or providers that do not occur in the same physical space. The COVID-19 pandemic catalyzed the use of this care delivery approach to improve access to primary care, particularly for patients who live in rural or remote geographies, have economic challenges, or experience competing priorities at home/work.1,2 Primary care is the first point of contact individuals have with the healthcare system 3 (differing from primary healthcare as an approach to care that involves primary care delivery, policy action, and empowerment4,5); this makes virtual care particularly relevant to explore in primary care. Family physicians and nurse practitioners (NPs) have professional autonomy to use their judgment to interchange in-person and virtual delivery.6,7 Unfortunately, the process taken by other nurses in primary care to shift their roles between in-person and virtual care is poorly understood. Although there is evidence that nurses improve patient, provider, and system outcomes (eg, weight loss, blood pressure, glycemic control, smoking cessation, physician workload, and adverse events),8-11 their integration and optimization in primary care has progressed at different speeds internationally.12,13 Nurses’ contributions to virtual care requires further research as countries increase nurses’ involvement in primary care environments.
Role Clarity in Virtual Nursing Practice in Primary Care
NPs (advanced practice nurses who diagnose and treat as primary practitioners) and registered nurses (RNs; nurses who provide care and support in varying capacities) are commonly identified in the literature as key providers in primary care delivery, though titles used to identify nurses in primary care differ internationally. 14 Licensed practical nurses (LPNs; nurses with a reduced scope of practice compared to NPs and RNs) have also been identified globally as potential contributors to primary care delivery, 15 however, there is less published literature about this designation within the primary care context. Nurses’ scopes of practice across designations are informed by legislation and professional regulation and standards (ie, referred to as legislated scope of practice), and this applies to both in-person and virtual care.16,17 Nurses’ scopes of practice are further informed by factors such as the organization where they are providing care (eg, funding model, availability of infrastructure); nurse training/education (ie, individual competencies 18 ); the needs of the patient/population receiving care (informed by the complexity, predictability, and risk associated with patient disease/condition) 16 ; and geography (nurses in rural and remote settings often practice more autonomously with expanded scopes of practice than nurses who work in urban settings).19,20 This is often referred to as the nurses’ professional scope of practice.
Nursing roles refer to the responsibilities, activities, and tasks carried out through interventions, programs, and/or initiatives in practice.21,22 Improving the understanding of nurses’ roles across regulatory designations, primary care practice settings, and virtual care modalities is integral to optimize team-based primary care.22,23 Role clarity also promotes appropriate task-shifting (ie, reasonable redistribution of tasks from a more highly qualified professional to another 24 ), which has the potential to improve clinical (eg, prevent and manage cardiovascular disease, diabetes, and mental health concerns) and system (eg, cost) outcomes in primary care. 25 Clarifying the roles of nurses in providing virtual care in primary care will inform the adoption of virtual care delivery by nurses and has the potential to improve the reach of service delivery and increase panel size within primary care settings. 26
Guiding Framework
We used the Nursing Care Organization Framework 27 (NCOF; Figure 1) to define key concepts, collect and analyze data, and map study results. The NCOF 27 outlines dimensions in the organization of healthcare services that can influence the delivery of patient care by nurses (ie, scope of practice, staffing, work environment). Notably, “scope of practice” is the language used in the NCOF, though it is referring to the scope of services delivered by nurses and not the scope of practice as it is commonly defined in the literature (ie, the roles, functions, and activities carried out by nurses based on their professional legislation, education, and competence 16 ).
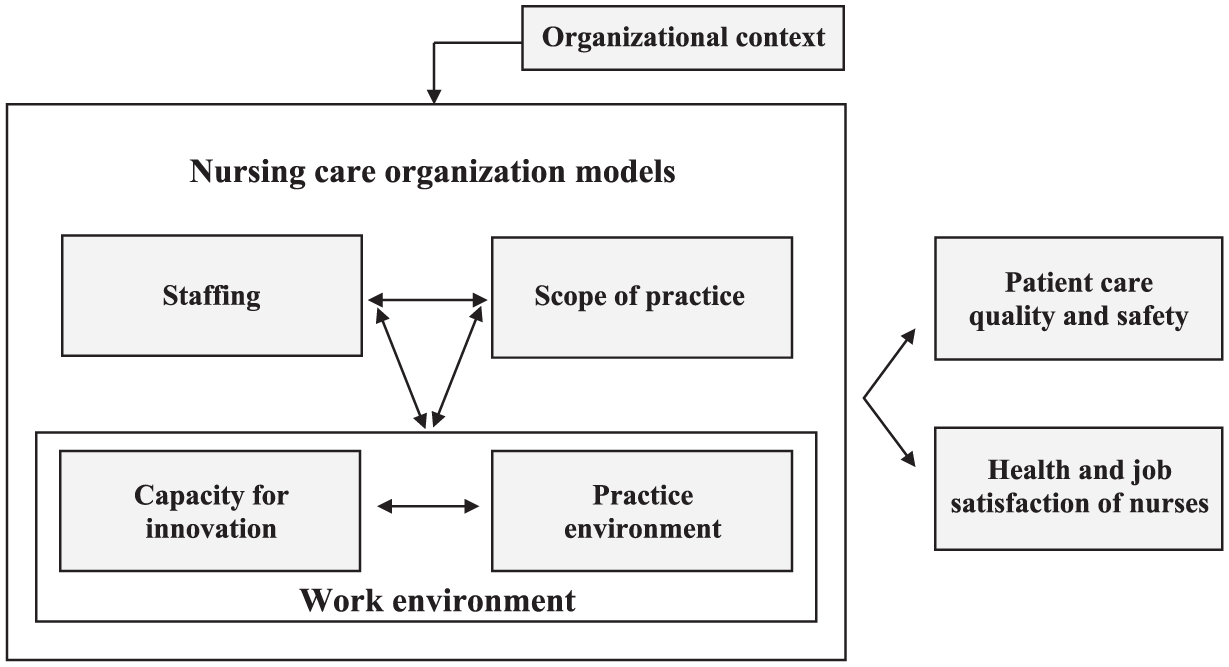
Nursing Care Organization Framework.
Purpose and Objectives
The purpose of this scoping review is to identify and map the international literature surrounding nurses’ (ie, NP, RN, LPN) roles in virtual care delivery across primary care practice settings, including differences across urban and rural geographies. The research objectives of this review are to:
Outline the roles that NPs, RNs, and LPNs perform to contribute to virtual care delivery in primary care practice settings;
Describe the key characteristics of primary care practice settings that involve virtual care delivery by NPs, RNs, and LPNs; and
Identify barriers and facilitators to role enactment for NPs, RNs, and LPNs in virtual care delivery in primary care practice settings.
For the purpose of this review, “role enactment” will refer specifically to the application of behavior and knowledge (ie, carrying out activities/tasks) that align with professional expectations. 28
Methods
Design
We conducted this review based on the Joanna Briggs Institute (JBI) scoping review methodology 29 and a protocol published a priori. 30 We report results following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) checklist. 31 Prior to beginning the review, we conducted a search of CINAHL, JBI Evidence Synthesis, Cochrane Database of Systematic Reviews, Google Scholar, and Embase to determine if any systematic or scoping reviews had already been published or were in development on this topic, and we found no published reviews.
Search Strategy
In consultation with a health sciences librarian (M.S.), we developed a search strategy aimed at locating both published and unpublished sources. We conducted preliminary searches in CINAHL and MEDLINE databases to identify text words in titles and abstracts, and index terms of relevant articles. We used these words to develop a full search strategy adapted for each included database (ie, CINAHL, MEDLINE, Embase, and PsycINFO) using unique keywords and index terms (Supplemental File). In addition to the database searches, we screened relevant systematic reviews, reference lists of included sources, and used the descendancy approach 32 to identify primary studies that were not present in our original searches. To locate gray literature, we searched ProQuest Dissertations and Theses Global, Google Scholar, and webpages of national nursing organizations (eg, Canadian Nurses Association, Australian Primary Health Care Nurses Association), digital health-focused organizations (eg, Digital Health Canada), and primary care networks/centers, among others. Database searches were conducted on June 21, 2022 and updated on May 28, 2024.
Eligibility Criteria
We included English and French published sources that used any qualitative, quantitative, or mixed-method design and various types of gray literature (eg, dissertations/theses, organizational/government reports, and nursing-specific policies), and did not place any location or publication date restrictions on search criteria. We excluded commentaries and conference abstracts.
We used the Participants, Concept, Context framework 33 to outline the content eligibility criteria for this review. The “Participants” and “Concept” components align with the scope of practice (nurse roles) dimension of the NCOF, and the “Context” component aligns with the overall organizational context where the NCOF is situated for this review.
Participants
We included sources that involved nurses from any regulatory designation (ie, NP, RN, LPN) practicing in primary care, as well as sources that did not specify nurse designation (eg, referred to generally as “nurses” in primary care). This included nurses across community types (ie, urban, rural, and remote); primary care was viewed broadly for nurses in rural areas who often practice within a community health scope (ie, public health, primary care, and home care). 34 Search strategies included generic and primary care-specific nurse titles used across countries (eg, general practice nurse and family practice nurse). 14 We excluded sources that focused on student nurses and nurses who were not licensed to practice. We also excluded nurses who require additional training (beyond entry-to-practice) for their roles, such as registered psychiatric nurses, specialized nurses (eg, foot care nurse and diabetes nurse specialist), and clinical nurse specialists (ie, advanced practice nurses who engage in roles beyond clinical practice, including leadership, research, and education, to address complex healthcare concerns in a specialized area 35 ).
Concept
We only included sources that focused on the roles of nurses in the delivery of virtual care within primary care. With respect to nurse roles, a nurse action component was required within nurse-patient interaction(s); these interactions could have involved patient presence (eg, delivering care remotely via telephone) or not (eg, consulting another provider remotely regarding patient assessment/concerns). Nurse roles must have been initiated in primary care settings. We excluded sources that involved nurses using technology for administrative purposes (eg, sending digital reminders to patients) as there was no care delivery component. We required that nurse roles were explicitly stated or able to be interpreted clearly based on the description of virtual care being delivered (ie, not grouped alongside other providers).
Context
The context for this review included both primary care and virtual care. Other terms used to refer to primary care (eg, general practice and family practice) and virtual care (eg, telehealth, digital healthcare) internationally were included in our search strategy. Sources involving virtual care delivery using any modality (eg, telephone, video, text message, and e-mail) were included. Studies that were situated in community health without a primary care focus (eg, specialty clinics, call centers, and prisons) were excluded. We also excluded studies that referred to the use of digital healthcare but did not involve nurse action that directly impacted patients’ plan of care (eg, using electronic medical records, using simulation for clinical-based training/education, research study recruitment, and disease reporting).
Selection of Information Sources
Search results were entered into Covidence for screening and review. We used the eligibility criteria to develop a tool for title/abstract and full-text screening. To pilot the screening process, 2 researchers (C.V., D.R.) independently screened 5% of the total results (random sample of various designs, n = 86 studies) and achieved 85% agreement.29,30 Discrepancies were discussed with the supervising researcher (J.L.), and the tool was refined to improve clarity. We then used the updated tool to screen titles/abstracts of remaining articles and to complete full-text screening of sources for eligibility.
Data Charting
Following the selection of eligible full-text sources, we completed a pilot test of the extraction procedure using a pre-determined data extraction tool informed by the NCOF and developed by the research team. Data situated within the scope of practice dimension (in the NCOF) included demographic details (eg, level of education/specialty training), professional designation, and role(s) performed. Further, we described primary care practice characteristics (eg, geographic location and team composition); the nature of virtual care delivery, including type of virtual intervention (eg, consultation, prescription renewal); patient population receiving care (eg, demographics and current illness/disease), delivery source (eg, telephone and video); and any barriers or facilitators that contributed to virtual care delivery. We developed a legend to ensure each component was clear for all researchers involved in the extraction. The pilot test for the extraction included 2 researchers (C.V., D.R.) who independently extracted 5 randomly selected sources across different study designs. We resolved discrepancies through discussions with the supervising researcher (J.L.) and amended the extraction tool to improve clarity. Following the pilot test, we extracted data from all full-text articles that met our inclusion criteria.
Synthesis of Results
We inductively analyzed data and the NCOF was used to map review findings deductively using 4 separate tables that correspond to the study objectives. The reciprocal relationships that exist between scope of practice (nurse roles), staffing, and work environment concepts of the NCOF were considered in the analysis of findings. Nurse roles were deductively categorized using the Registered Nurse Virtual Primary Care Practice Guide developed by the Innovation Support Unit within the Department of Family Medicine at the University of British Columbia. 36 This guide includes 6 role categories (ie, care coordination, chronic disease management, triage and assessment, health education, COVID-specific care, health promotion and disease prevention). These role categories were further analyzed and defined by describing specific nurse roles. When we described barriers and facilitators to nurse role enactment, we separated these factors by patient characteristics, work environment, and scope of practice and staffing (as per the NCOF).
Results
The PRISMA diagram (Figure 2) outlines the process for identifying and screening published and gray literature sources for inclusion following our most recent search (May 2024). In total, 34 sources were included in this review (Table 1).
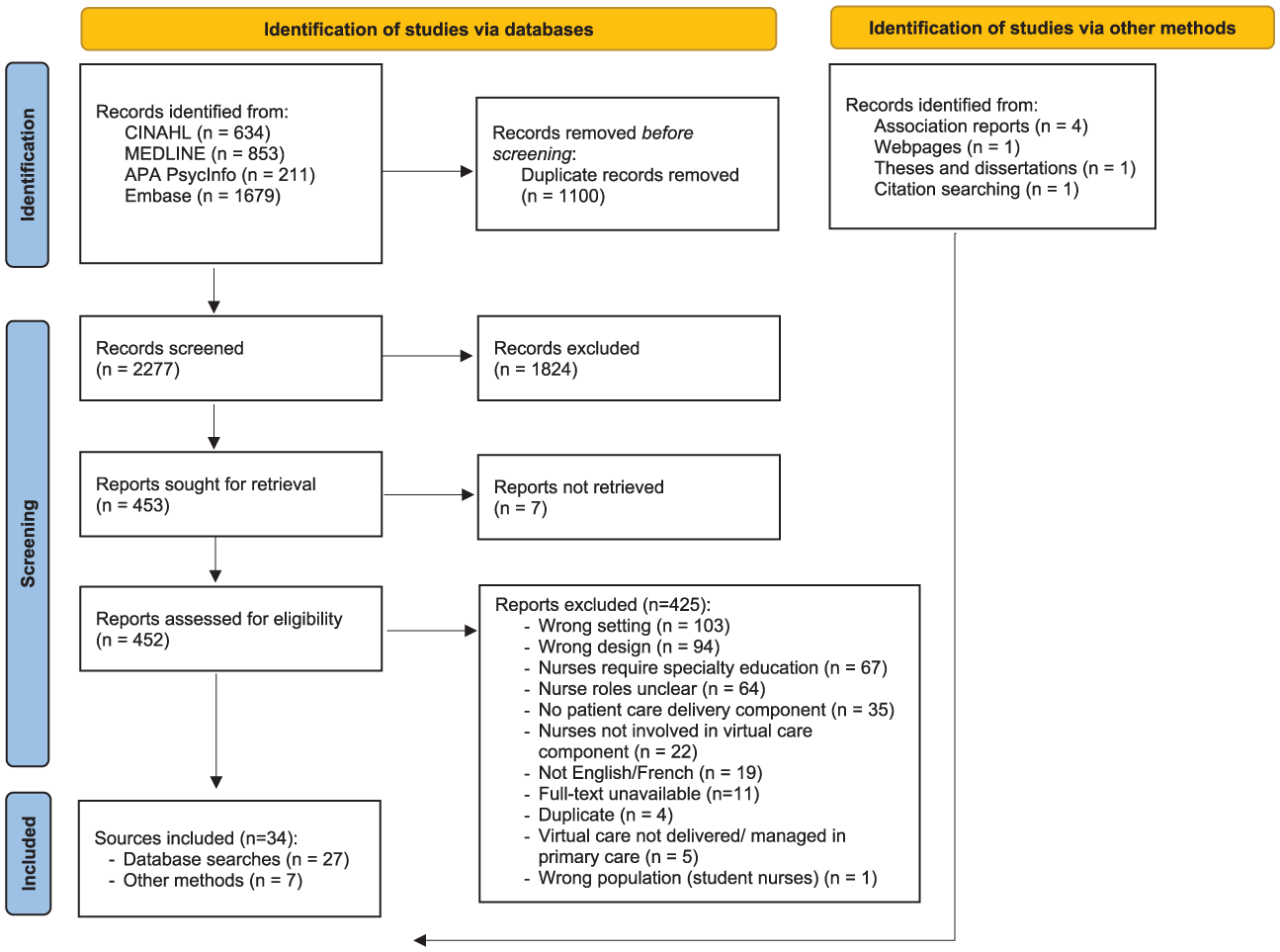
PRISMA diagram outlining the search results.
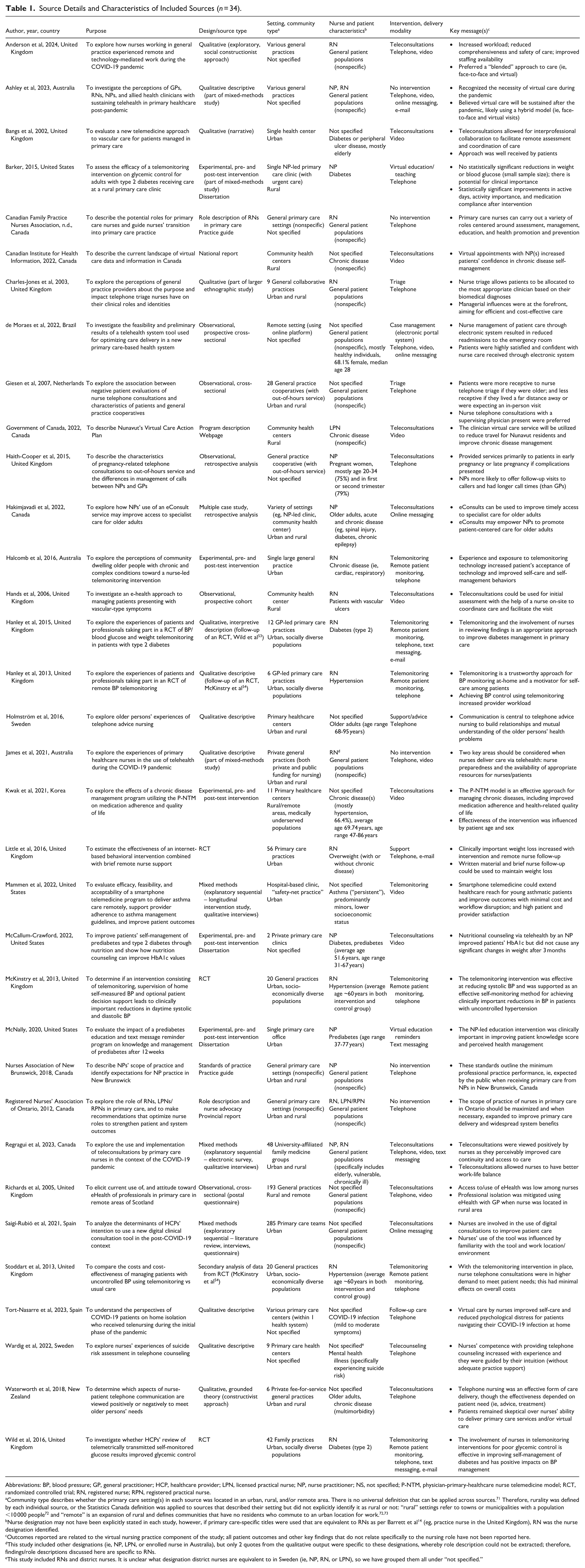
Source Details and Characteristics of Included Sources (n = 34).
Abbreviations: BP, blood pressure; GP, general practitioner; HCP, healthcare provider; LPN, licensed practical nurse; NP, nurse practitioner; NS, not specified; P-NTM, physician-primary-healthcare nurse telemedicine model; RCT, randomized controlled trial; RN, registered nurse; RPN, registered practical nurse.
Community type describes whether the primary care setting(s) in each source was located in an urban, rural, and/or remote area. There is no universal definition that can be applied across sources. 71 Therefore, rurality was defined by each individual source, or the Statistics Canada definition was applied to sources that described their setting but did not explicitly identify it as rural or not: “rural” settings refer to towns or municipalities with a population <10 000 people 72 and “remote” is an expansion of rural and defines communities that have no residents who commute to an urban location for work.72,73
Nurse designation may not have been explicitly stated in each study, however, if primary care-specific titles were used that are equivalent to RNs as per Barrett et al 14 (eg, practice nurse in the United Kingdom), RN was the nurse designation identified.
Outcomes reported are related to the virtual nursing practice component of the study; all patient outcomes and other key findings that do not relate specifically to the nursing role have not been reported here.
This study included other designations (ie, NP, LPN, or enrolled nurse in Australia), but only 2 quotes from the qualitative output were specific to these designations, whereby role description could not be extracted; therefore, findings/role descriptions discussed here are specific to RNs.
This study included RNs and district nurses. It is unclear what designation district nurses are equivalent to in Sweden (ie, NP, RN, or LPN), so we have grouped them all under “not specified.”
Characteristics of Included Sources
Sources were published between 2002 and 2024 and were conducted in the United Kingdom (n = 12), Canada (n = 7), the United States (n = 4), Australia (n = 3), Spain (n = 2), Sweden (n = 2), as well as Brazil, Korea, The Netherlands, and New Zealand (all n = 1). Sources comprised 29 published research studies and 5 studies retrieved from the gray literature. The published studies used qualitative (n = 13; qualitative descriptive, interpretive description, grounded theory, case study); experimental (n = 8; pretest-posttest, randomized controlled trial); observational (n = 5; cross-sectional, cohort); or mixed-methods (n = 3) designs. The 5 unpublished sources identified from the gray literature included national or provincial reports (n = 2), practice guides (n = 2), and 1 program description webpage. Many sources were specific to RNs (n = 12), fewer sources focused on NPs (n = 6), and LPNs (n = 1); however, several did not specify nurse regulatory designation (n = 12) or were relevant across multiple designations (n = 3). The virtual care modality also varied but was identified across sources. Most frequently, nurses were using the telephone to deliver virtual care (n = 23); other modalities included video calls and messaging/e-mail (using online platforms and mobile devices/smartphones). Many sources involved nurses using multiple different modalities for care delivery (n = 13).
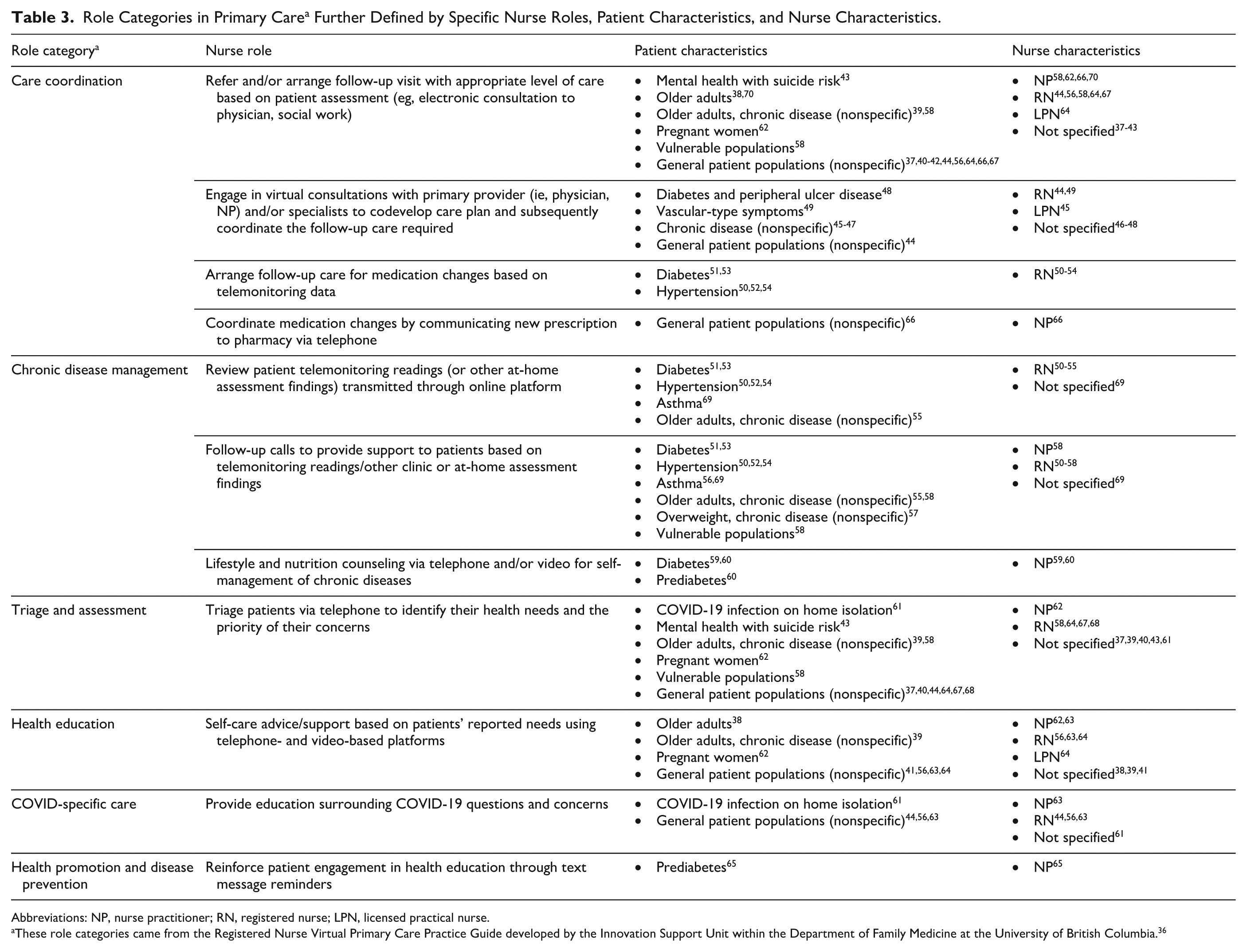
Categorization of Primary Care Nurse Roles in Virtual Care
Nurses carried out a variety of roles in their delivery of virtual care. Table 2 maps nurse roles to regulatory designations according to the 6 role categories outlined in the Registered Nurse Virtual Primary Care Practice Guide. 36 Table 3 presents role categories in primary care further defined by specific nurse roles, patient characteristics, and nurse characteristics. Most often, nurses were involved in roles related to care coordination (n = 25), such as referring and/or arranging follow-up visits (eg, electronic consults) with the appropriate level of care based on assessments37-43; and engaging in virtual consultations alongside patients and their primary provider(s) (ie, physicians, NPs) and/or specialist(s) to codevelop care plans and arrange follow-up care.44-49 Nurses were also involved in chronic disease management (n = 13), including reviewing telemonitoring readings/other at-home assessment findings transmitted through online platforms50-55; providing patient support via telephone after reviewing these findings50-58; and delivering lifestyle/nutrition counseling to promote self-management of chronic disease.59,60 Nurses’ roles also included triaging and assessing patients to identify their health needs and the priority of their concerns (n = 11)37,39,40,43,61; health education (n = 7; eg, self-care advice/support38,39,41,56,62-64); COVID-specific care (n = 4; eg, education related to COVID-19 questions/concerns44,56,61,63); and health promotion and disease prevention care (n = 1; eg, reinforcing patient engagement in health education 65 ). Notably, roles categorized under chronic disease management may have also involved an element of health education, and promotion and disease prevention related to the patients’ chronic disease, accounting for compounded roles in this category (ie, more than 1 role within each role category outlined in the Registered Nurse Virtual Primary Care Practice Guide 36 ).
Breakdown of Nurse Role Categories in Virtual Care a by Nurse Designations.
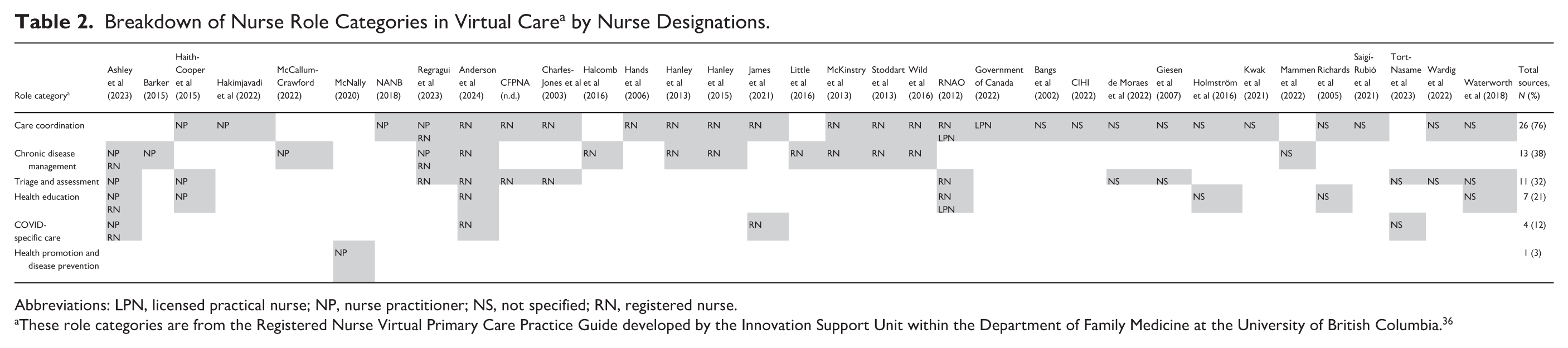

Abbreviations: LPN, licensed practical nurse; NP, nurse practitioner; NS, not specified; RN, registered nurse.
These role categories are from the Registered Nurse Virtual Primary Care Practice Guide developed by the Innovation Support Unit within the Department of Family Medicine at the University of British Columbia. 36
Role Categories in Primary Care a Further Defined by Specific Nurse Roles, Patient Characteristics, and Nurse Characteristics.
Abbreviations: NP, nurse practitioner; RN, registered nurse; LPN, licensed practical nurse.
These role categories came from the Registered Nurse Virtual Primary Care Practice Guide developed by the Innovation Support Unit within the Department of Family Medicine at the University of British Columbia. 36
Patient Characteristics and Specific Primary Care Nurse Roles
Overall, and not unexpectedly, the services nurses delivered virtually varied across patient populations (Table 3). Many studies included general patient populations (unspecified diseases/conditions; n = 10), which exemplified the broad range of patient populations who can receive nursing care via virtual delivery. Patients with different chronic diseases were represented across sources, including diabetes or prediabetes (n = 6), hypertension (n = 3), and asthma (n = 1); 5 studies referred generally to populations with chronic diseases. Other studies described the roles of nurses in virtual care delivery with older adult populations (n = 4), pregnant women, 62 vascular surgery patients, 49 COVID-19 patients, 61 and mental health patients with a risk of suicide. 43
When a source focused on general patient populations in primary care, nurses were most often arranging or referring patients to other providers for follow-up with the appropriate level of care (care coordination)37,40-42,44,56,64,66,67; or triaging patients via telephone to identify the priority of their concerns (triage and assessment).37,40,44,64,67,68 Patient populations with different chronic diseases relied mostly on nurse contributions in coordinating follow-up care related to their chronic disease (care coordination)45-48,50-54; and/or reviewing assessment findings that were collected remotely from patients at home (chronic disease management).50-55,69 Patients with COVID-19 diagnoses relied on nurses delivering COVID-specific care virtually, such as triaging and providing education/guidance surrounding COVID-19. 61
Characteristics of Primary Care Practice Settings
Setting, Funding Model, Team
Nurses delivered virtual care in different primary care settings, such as NP-led clinics59,70 and hospital-based primary care clinics, 69 though most settings were described using basic terms (eg, primary care practice, general practice, community health center, primary healthcare center) and lacked detail regarding the specific practice model. Many studies involved team-based or collaborative environments (n = 11; eg, general collaborative practices, general practice cooperatives, family medicine groups, primary care teams),37,42,44,48,50,52,54,55,58,62,67 though the specific team composition (ie, other members of the team) was often not clearly stated but involved at least nurses and physicians. No notable differences were found in nurse roles within these team-based environments.
Funding models were only explicitly discussed by 2 sources; 1 source referred to their setting as private fee-for-service practices, 39 while the source had a fee-for-service element in their private practices (ie, funded by service delivery component) but also received national government funding 44 (interpreted as a blended capitation model).
Geographic Location
Sources were specific to urban areas (n = 11), rural areas (n = 6), urban and rural areas (n = 9), and 8 studies did not specify the geography of their study location. As there was no universal definition for “rural” that could be applied across sources, 71 we allowed individual sources to define rurality, or used the Statistics Canada definition when sources described their setting but did not explicitly identify it as rural or not: rural settings refer to towns or municipalities with a population <10 000 people 72 and remote is an expansion of rural and defines communities that have no residents who commute to an urban location for work.72,73 Some geographical areas were described in detail, providing information about the community/population served (eg, socially diverse populations,50,51,53 medically underserved populations 46 ). Sources that clearly presented rural-specific findings38,41,44-47,49,59,70 came from Canada (n = 3) and the United Kingdom (n = 2); and Australia, Korea, Sweden, and the United States (all n = 1). Rural settings included NP-led clinics, community health centers, and general practices/clinics. Rural-specific sources included nurses across designations: NP (n = 2), RN (n = 2), LPN (n = 2), and not specified (n = 3).
Within rural settings, nurses were mainly involved in care coordination (n = 8), health education (n = 2), chronic disease management (n = 1), and COVID-specific care (n = 1); this is consistent with findings across urban areas and settings in general whereby care coordination was the most common role category for nurses in virtual care. Nurses referred to other providers and/or arranged follow-up care37,43,46,49; or engaged in virtual consultations with primary providers and/or specialists to codevelop patient care plans.49,50,55-57 Nurse roles across the other categories were centered around self-care advice/support,37,43 lifestyle and nutrition counseling, 47 and education related to COVID-19. 49
Barriers and Facilitators
Table 4 presents barriers and facilitators that influenced nurses’ role enactment, organized by the NCOF. Overall, patient perceptions and experiences with virtual care, either positive or negative, were the most influential on nurse roles.37,39,40,46-48,50,51,55,56,61,63,65,67,69 When nurse roles were perceived to have an impact on quality of patient care (eg, improving self-care),48,50,51,56,61,70 patient advocacy,48,49,70 and continuity of care,39,47,49 nurses were more likely to deliver virtual care. Barriers included concerns with patient privacy (eg, safeguarding issues) and ethical care delivery (eg, during remote care delivery from home)41,56,58; equitable care delivery (eg, hearing and visual impairments)38,58; and accessibility of resources (eg, devices with necessary online platforms, high-speed broadband internet connection).56,58
Barriers and Facilitators to Nurse Role Enactment in Virtual Care Organized by Dimensions Within the NCOF.
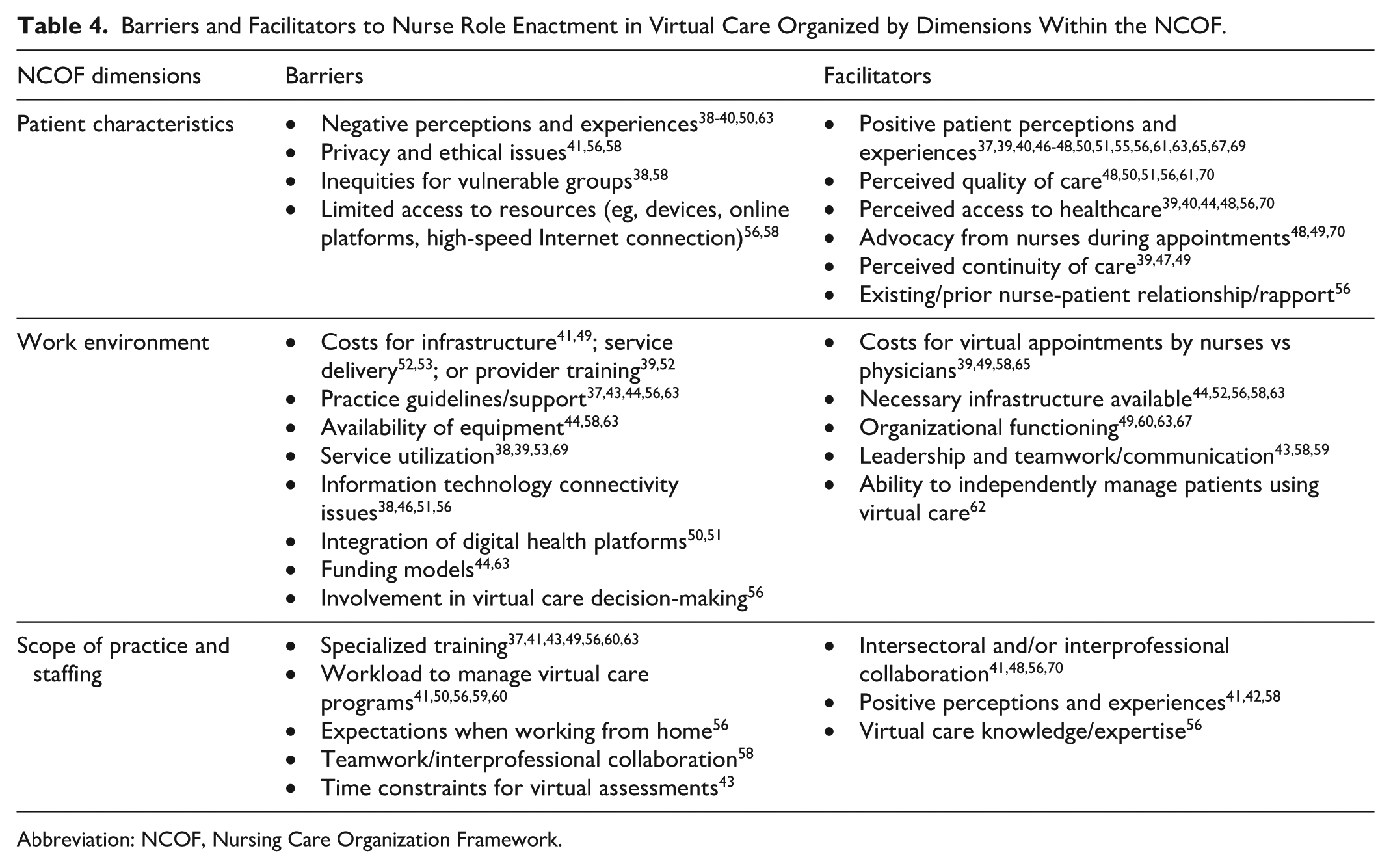
Abbreviation: NCOF, Nursing Care Organization Framework.
Lack of nurse training and practice guidelines/support in virtual care were major barriers to nurse role enactment.37,41,43,49,56,60,63 Increased workload (eg, more time required to set up virtual appointments)41,50,56,59,60 and service utilization (ie, longer visits, increased follow-up visits)38,39,53,69 were also commonly reported barriers. Other barriers, reported less frequently, to nurse role enactment in virtual care included reduced teamwork and collaboration (eg, during decision-making processes where physicians had the strongest voice)41,56,58; poor integration between digital health platforms, requiring multiple programs to be functioning simultaneously to deliver and manage care virtually50,51; primary care funding models (eg, fee-for-service) not favoring nurse involvement in virtual care delivery44,63; limited time designated to virtual appointments, restricting nurses from completing comprehensive assessments 43 ; and nurse expectations when working remotely from home (eg, work with children present, work even when ill). 56 Another factor – mode of delivery (eg, text message preferred over telephone interactions) – impacted patients’/providers’ experience with virtual care delivery depending on the context of the visit. 59
Some rural studies discussed factors that influenced nurse involvement in virtual care delivery specific to rural contexts. For example, the availability of suitable equipment and resources (eg, high-speed internet, computers) contributed to nurses’ successful involvement in virtual care delivery.38,41,44,46 Across many rural studies, training and practice guidance were noted as a barrier to role enactment,41,44,49 though this was more commonly noted in sources that were situated in urban areas or did not specify their geographical context.
Discussion
In this scoping review, we mapped the international literature that described nurses’ contributions to virtual care delivery across primary care practice settings and aimed to outline nurse roles, practice setting characteristics, and barriers and facilitators to role enactment. Our findings demonstrated that nurses’ roles in virtual care delivery are heavily focused on the areas of care coordination, chronic disease management, and triage/assessment. Nurse roles are contributing to key elements of patient care, including consulting other providers, arranging follow-up care/testing, monitoring remote collection of patient data, and assessing/prioritizing patient concerns. Further, nurses’ role enactment is influenced by a variety of factors specific to patient characteristics (eg, patient perceptions, privacy/ethical concerns), work environment (eg, costs, practice guidance/support), and/or scope of practice and staffing (eg, virtual care practice training).
Primary care nurses’ roles in coordinating patient care using virtual modalities underscore their pivotal role in transforming care delivery, which aligns with growing evidence that physicians are increasingly acknowledging the critical function of information communication technologies in effective care coordination. 74 It has also been found that when physicians collaborate with other providers, such as nurses, care coordination can be improved. 75 Therefore, nurses using virtual modalities can have a compounding improvement on coordination of care in primary care (ie, care coordination improved through the use of virtual modalities and collaboration). Beyond care coordination and other roles reported in this review, other virtual care roles such as mental health/behavioral management 76 and rehabilitation 77 were not identified, though there is potential for primary care nurse roles to extend to these patient populations. Also, no trends were noted in nurse roles across designations in this study, which might differ from what is actualized in practice; deliberate exploration of virtual nursing practice across individual designations (eg, NPs, RNs, and LPNs) could provide more concrete insight on how practice in this area varies based on nurse education/training.
Despite the global shift toward team-based models of care in primary care settings, 4 only a limited number of studies in this review investigated nurses’ roles within a team-based context. When teams were identified, they were not well described and lacked depth, which influenced our ability to understand the team impact on nurse roles. Studies have shown the interdependent nature of scopes of practice for nurses, physicians, and other providers in primary care, as the roles of one provider influence those of another15,78 contributing to nurses’ professional scope of practice. By generating evidence within team-based environments in primary care, we can better understand how nurses complement their colleagues in delivering comprehensive care (eg, how roles shift, narrow, or expand) and facilitating the optimization of each provider’s scope of practice.
A recent report by Canada Health Infoway 79 aimed at assessing the use of digital technology in nursing practice outlined nurses’ thoughts about technology in practice. The report noted barriers that prevented nurses from maximizing the value of digital technology in practice; many of these aligned with the barriers to role enactment in our study, including time constraints, equipment/technology constraints, and education and training. These barriers are also consistent across virtual care literature focused on other healthcare professionals, including family physicians during the COVID-19 pandemic80,81 and generally in primary care. 82 A report from the International Council of Nurses 83 has highlighted the need to address these barriers, among others (eg, integrated care delivery to coordinate both virtual and in-person services), at a global level to enhance nurses’ contributions to digital health initiatives in primary care. Other barriers were more contextual and not consistently reported; for example, when nurses had atypical work arrangements (ie, worked from home) during the pandemic, they were, at times, asked to work even when feeling unwell. 56 This would not be applicable in more typical work arrangements (eg, working in clinic). Understanding barriers and facilitators to role enactment in virtual nursing practice in primary care is needed to focus future research and policy efforts.
Resources developed to guide virtual nursing practice in primary care are largely focused on physician practice or healthcare professionals generally. These practice guides, standards of practice, and other resources6,84,85 are beneficial due to the unique considerations that are required in virtual care delivery; however, nursing is a distinct healthcare profession that requires nursing-specific knowledge to inform role enactment, limiting the value of these resources in nursing practice. Virtual care has been found to promote shorter visits, 86 which contradicts a barrier noted in this review, whereby virtual visits by nurses were found to be longer 38 or require more frequent follow-ups39,53,69 than in-person care. By understanding nurses’ roles in virtual care delivery across primary care settings, we can develop resources that are targeted at nursing practice (eg, standards of practice in virtual care, communication approaches in virtual interactions) to optimize their roles and improve the efficiency of virtual nursing practice.
Limitations
Studies included in this review did not consistently report on practice characteristics (eg, practice settings, geography). Although we made efforts to compare across practice characteristics where these were reported, the majority of our findings focused on virtual care delivery across primary care settings more generally. Select studies did not provide enough detail on nurse roles; therefore, role categories could be deduced, but specific exemplars of nurse roles could not be further defined, limiting the depth of our understanding of specific nurse roles. Roles could also have been skewed if nurses were specialty trained, but this information was not reported in the manuscript. Similarly, not all sources explicitly discussed barriers and facilitators, nor could this type of data be interpreted.45,54,57,64,66,68 Lastly, there were many studies that did not meet our language eligibility criteria (ie, English or French sources) and were excluded from our review. This may limit the generalizability of our findings to non-English or French-speaking jurisdictions/countries.
Conclusion
In conclusion, nurses make important contributions to virtual care across primary care settings. They are well-positioned to improve the availability of and access to primary care through their integration in digital health initiatives. They continue to face challenges with role enactment when delivering virtual care, which should be considered in future research and policy efforts to improve nurses’ competence in, and patients’ experiences with, virtual care delivery. All providers, including nurses, should also mindfully consider the challenges that infiltrate virtual care as they transition toward optimizing their virtual care roles across primary care settings.
Supplemental Material
sj-pdf-1-wjn-10.1177_01939459251397729 – Supplemental material for Nurses’ Contributions to Virtual Care Delivery in Primary Care: A Scoping Review
Supplemental material, sj-pdf-1-wjn-10.1177_01939459251397729 for Nurses’ Contributions to Virtual Care Delivery in Primary Care: A Scoping Review by Crystal Vaughan, Julia Lukewich, Maria Mathews, Lindsay Hedden, Marie-Eve Poitras, Shabnam Asghari, Michelle Swab, Dana Ryan and Ruth Martin-Misener in Western Journal of Nursing Research
Footnotes
Acknowledgements
We would like to acknowledge Katie Kehoe, Library Assistant at the Health Sciences Library at Memorial University of Newfoundland for her support with document delivery of included sources.
Ethical Considerations
This review involved the secondary analysis of published and/or publicly available sources; therefore, ethical approval was not required.
Consent to Participate
This study involved the collection of sources/literature and did not involve study participants. Informed consent was not applicable to this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Rural360 (with funds provided by the International Grenfell Association); Mitacs; Newfoundland & Labrador Support for People and Patient-Orientated Research and Trials (SUPPORT) Unit (Graduate Student Funding Competition; award/grant: N/A); the Canadian Nurses Foundation (award/grant: N/A); and the Seed, Bridge, and Multidisciplinary Fund (grant #20230220) at Memorial University of Newfoundland.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.