
Abstract
A Delphi (consensus) process was used to obtain national agreement on competencies for registered nurses (RNs) in primary care. A draft of competencies was developed by key informants. Following this, nurses with primary care experience/expertise completed a Delphi survey to rate the importance of competency statements on a six-point Likert scale. Statements not reaching consensus (agreement ≥80%) were modified and included in a second (final) round. The first survey was completed by 63% (n = 86/137) of participants and 84% (n = 72/86) of these participants completed the second survey. Most statements (n = 45) achieved agreement after the first survey; one statement was dropped and two were combined following the second round. The final list of competencies consists of 47 statements across six domains (professionalism; clinical practice; communication; collaboration and partnership; quality assurance, evaluation, and research; leadership). National competencies will help strengthen the RN workforce within primary care, improve team functioning, and support role integration/optimization.
A competent workforce of registered nurses (RNs) in primary care, providing care in collaboration with family physicians, nurse practitioners, and other clinicians, can address pressing issues facing our health care system, including the rising cost of care, care of aging populations, and an increasing prevalence of chronic diseases and patients with complex health care needs (Horrocks et al., 2002; Laurant et al., 2005; Poitras et al., 2018; Todd et al., 2007). The increasing number of RNs employed in primary care settings may offer solutions to care delivery challenges in Canada and internationally.
The Importance of Establishing Competencies for Registered Nurses in Primary Care
RNs who work in primary care fall under the broad category of community-based nursing in Canada, which also includes home care nursing and public health nursing (Community Health Nurses of Canada [CHNC], 2019; Lukewich, Taylor, et al., 2018). In 2016, there were close to 45,000 RNs working in Canadian community-based settings, including primary care. This number grew by 11,563 between 2007 and 2016 (Canadian Institute for Health Information [CIHI], 2017). RNs in primary care have completed either a college diploma or baccalaureate degree. In all provinces/territories, except for Quebec, newly educated RNs are required to complete a university baccalaureate degree (Canadian Nurses Association [CNA], 2020; Lukewich, Edge, et al., 2018). RNs function as generalists providing a broad range of services, including but not limited to, health education, health promotion, chronic disease prevention and management, acute episodic care, therapeutic interventions, well-women and well-baby care, and care coordination (Canadian Family Practice Nurses Association [CFPNA], 2017; CNA, 2011; Halcomb et al., 2016; Oandasan et al., 2010; Poitras et al., 2018). In Canada, RNs in primary care settings are known as “family practice nurses” or “primary care nurses” (herein referred to as RNs in primary care). Primary care represents an entry point for patients into the health care system and is usually carried out in a clinic/office setting. It applies the principles of primary health care (CNA, 2000; World Health Organization, 2018) and focuses on the delivery of health promotion, disease prevention, and management of episodic and chronic conditions with individuals and families (CNA, 2005; Starfield, 2009). There is variability in the characteristics and structures of primary care organizations across jurisdictions in Canada, such as funding mechanisms (e.g., global funding, fee-for-service, capitation), integration within regional networks, and compositions of interdisciplinary teams (Lukewich et al., 2014). Examples of primary care organizations include family health teams, community health centers, family medicine groups, and primary care networks.
Despite the increasing volume of RNs employed within primary care, there is a lack of consensus on their optimal role, the implementation of their role is not standardized, and education is not formalized. Widespread and uniform implementation of the RN role in primary care is lacking. RNs are working in primary care settings without clearly defined role expectations resulting in underutilization and missed opportunities to contribute to high-quality patient care (CNA, 2014). Establishing nationally recognized competencies for RNs in primary care is a needed solution to address issues related to integration and optimization of this role, particularly in regard to challenges that exist related to funding and practice models. Prior to the completion of this project, a standardized set of national competencies for RNs who work within primary care settings did not exist.
These competencies were developed and informed from standards of practice (e.g., Canadian Community Health Nursing Standards of Practice; CHNC, 2019), which are higher order directives that define the scope and depth of practice for RNs in a specific health setting. Competencies are a framework designed for the purposes of meeting these expected standards and define the integrated knowledge, skills, and attributes required of a RN to practice safely and ethically in a distinct practice setting. A standardized set of competencies can subsequently inform specific roles and activities, resulting in a more well-defined understanding of a RN scope within this unique setting. Competencies exist for many other areas of nursing including community-based nursing disciplines, such as public health and home care nursing. The Canadian Community Health Nursing Standards of Practice were used as an organizing framework in the development of competencies for these other community-based nursing disciplines (CHNC, 2009, 2010).
An environmental scan of literature focused on competency development for RNs in primary care indicated that competencies are being examined internationally; however, the level of focus on this subject matter varies considerably between countries and Canada lags behind international work in this area (Lukewich, Taylor, et al., 2018). A similar review of international literature confirmed that although there were some common themes in the development of competencies among countries (e.g., clinical practice, professionalism, communication, health promotion), standards for nurses working in primary health care have received limited attention overall, and tend to vary in the quality of the development process (Halcomb et al., 2016). In comparison to other community-based nursing areas (i.e., public health, home care; CHNC, 2009, 2010), the development of competencies for RNs in primary care has received significantly less focus. National and provincial/territorial nursing organizations recognize the need to develop competencies for RNs in primary care to further strengthen the optimization of this workforce across Canada (CFPNA, 2017; CNA, 2014; Registered Nurses’ Association of Ontario, 2012). In 2014, the Canadian Nurses Association published a report with findings from a scoping review and key informant interviews that summarized issues regarding the advancement of the RN role within collaborative interprofessional teams and recommended acquiring national consensus on competencies for this role (CNA, 2014). Similarly, a national primary care task force launched by the Registered Nurses Association of Ontario recommended acknowledgement of the unique competencies of RNs in primary care to support role optimization and expansion (RNAO, 2012). Defining competencies for RNs in primary care is a clear recommendation also stated in recent literature published both within and outside of Canada, such as Australia, the United Kingdom, New Zealand, Brazil, and South Africa (Australian Nursing & Midwifery Federation, 2014; Berkowitz, 2016; Halcomb et al., 2016; Lukewich, Taylor, et al., 2018; Oandasan et al., 2010; Smolowitz et al., 2015; Strasser et al., 2005; Witt & de Almeida, 2008). However, the only known research related to competency development for RNs in primary care in Canada was a single project conducted in the province of Ontario that developed a primary care nursing competency framework. The six distinct competency domains that emerged are as follows: Professional, Expert, Communicator, Synergist, Health Educator, and Lifelong Learner, and a consensus on a list of respective competency statements was reached (Moaveni et al., 2010). This study relied on a small sample size (n = 27) of experts from Ontario; thus, findings are not generalizable to all provinces/territories in Canada.
Purpose
The purpose of this study was to develop competencies that reflect the unique contributions of RNs in primary care to support the integration and optimization of this role across Canada. The following research question was addressed: What are competencies that best represent the practice of RNs in primary care across Canada?
Methods
Design
A Delphi (consensus) process (de Loë et al., 2016; Hsu & Sandford, 2007; Yousuf, 2007) was used to obtain national agreement on competency statements for RNs in primary care. Ethics approval was obtained by Newfoundland and Labrador’s Health Research Ethics Board (Ref #: 20190681).
Procedures
Delphi Round #1
The initial draft of competencies for RNs in primary care was informed by an environmental scan of international literature (Lukewich, Taylor, et al., 2018), feedback from CFPNA members (CFPNA, 2017), a panel of key informants (researchers, stakeholders, project partners) with expertise and experience in primary care nursing, and a review of competencies of related practice areas (Canadian Council of Registered Nurse Regulators [CCRNR], 2018; Canadian Interprofessional Health Collaborative, 2010; CHNC, 2009, 2010). The Community Health Nurses of Canada’s Canadian Community Health Nursing Standards of Practice was used as a guiding framework (CHNC, 2019). The panel of key informants sought to build upon existing entry-to-practice competencies for RNs (Canadian Association of Schools of Nursing, 2014; CCRNR, 2018; College of Nurses of Ontario, 2018) and to complement, rather than duplicate, existing published competencies in similar areas. The initial draft consisted of 49 statements organized within six overarching competency domains, namely (1) Professionalism; (2) Clinical practice; (3) Communication; (4) Collaboration and partnership; (5) Quality assurance, evaluation, and research; (6) Leadership. This initial draft of competency statements was translated into French (and back translated to verify accuracy of translation) by a professional translator knowledgeable in health care terminology. This draft underwent two Delphi survey rounds to obtain national agreement.
Delphi Round #2 and #3
Two consecutive online surveys were completed to obtain consensus on the developed competency statements. Panel participants for the Delphi survey process were identified by the research team through snowball sampling, online searches, and professional organizations (e.g., Canadian Family Practice Nurses Association and its provincial groups). The panel was comprised exclusively of nurses with knowledge, expertise, and/or experience related to RNs in primary care, representing all provinces/territories and the five domains of nursing practice (i.e., clinical practice, education, research, policy, administration; CNA, 2015). A total of 137 participants were identified. Participants were sent an email invitation by a research assistant, the project lead, and/or a member of the project team who was familiar with the contact, followed by reminders approximately one-week apart. The email invitation contained information about the study and a link to the online competency development survey. Participants were asked to report on the importance of each competency statement using a six-point Likert scale (i.e., 1 = not important at all; 6 = extremely important) and offer written feedback/suggestions. Consensus on a competency statement was set a priori and defined as at least 80% agreement (a mean score of at least 5.0), based upon recommendations and consensus levels used in previous Delphi studies (Galipeau et al., 2017; Hsu & Sandford, 2007; Phillips et al., 2014). The survey was translated into French (and back translated to verify accuracy of translation) by a professional translator knowledgeable in health care terminology, and pre-tested in English and French before distribution to determine readability and feasibility of the online platform (i.e., Lime Survey). At the end of the first survey round, the research team met via teleconference to review the data and modify statements. Only modified statements underwent review in a second survey round, and only participants who had completed the first round were asked to complete the second survey round.
Analysis
Data analysis was performed with IBM SPSS Version 22. Participant demographic characteristics and level of consensus for each competency statement was examined using descriptive statistics, including frequencies and percentages. Comparison of participant demographic characteristics between survey round one and round two was performed using Pearson’s χ² tests (p ≤ .05) to assess representativeness of the panelists in the second round. Comments/suggestions on survey items were transcribed into a single report by the research assistant for review and discussion by the research team members.
Results
Table 1 displays participant demographic characteristics. The first Delphi survey round was completed by 86/137 individuals (63% response rate) between April and May 2019, and 72/86 of these first round individuals completed the second Delphi survey round (84% response rate) between June and August 2019. There were no significant differences between participant characteristics in round 1 and round 2. The participants represented all domains of primary care nursing, had differing levels of nursing experience, and represented all provinces and territories of Canada (Table 1). The highest proportion of participants were from Nova Scotia (round 1 = 20.9%; round 2 = 20.8%), British Columbia (round 1 = 14%; round 2 = 16.7%), Quebec (round 1 = 11.6%; round 2 = 11.1%), and Alberta (round 1 = 11.6%; round 2 = 9.7%). The largest number of respondents worked as front-line nurses (round 1 = 43.5%; round 2 = 38.9%). A high number of participants also reported working in sectors related to management/supervision/administration (round 1 = 31.8%; round 2 = 30.6%) and education (round 1 = 25.6%; round 2 = 26.4%). Other roles consisted of research, policy/decision-making, consulting, and clinical nurse education.
Participant Demographic Characteristics.
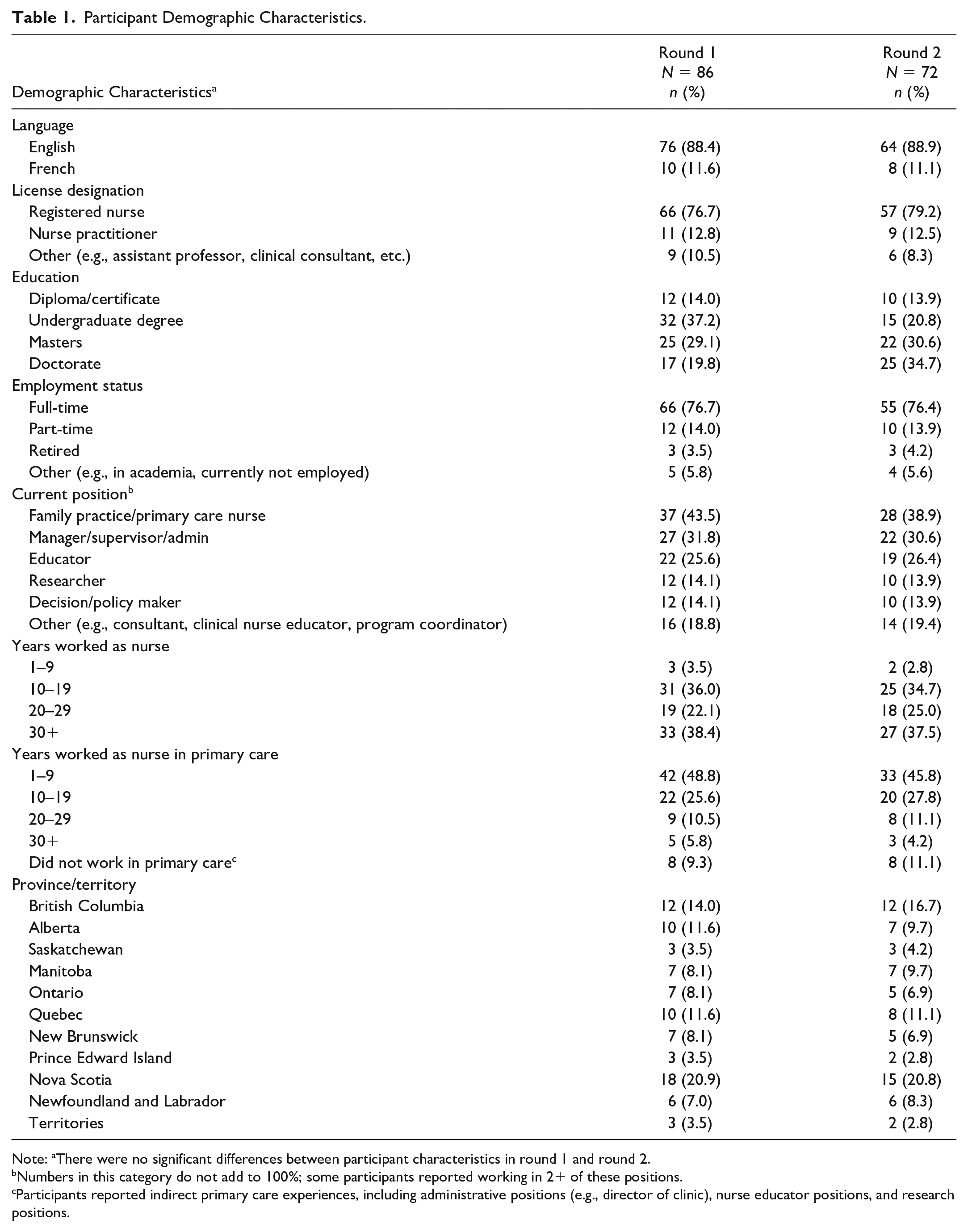
Note: aThere were no significant differences between participant characteristics in round 1 and round 2.
Numbers in this category do not add to 100%; some participants reported working in 2+ of these positions.
Participants reported indirect primary care experiences, including administrative positions (e.g., director of clinic), nurse educator positions, and research positions.
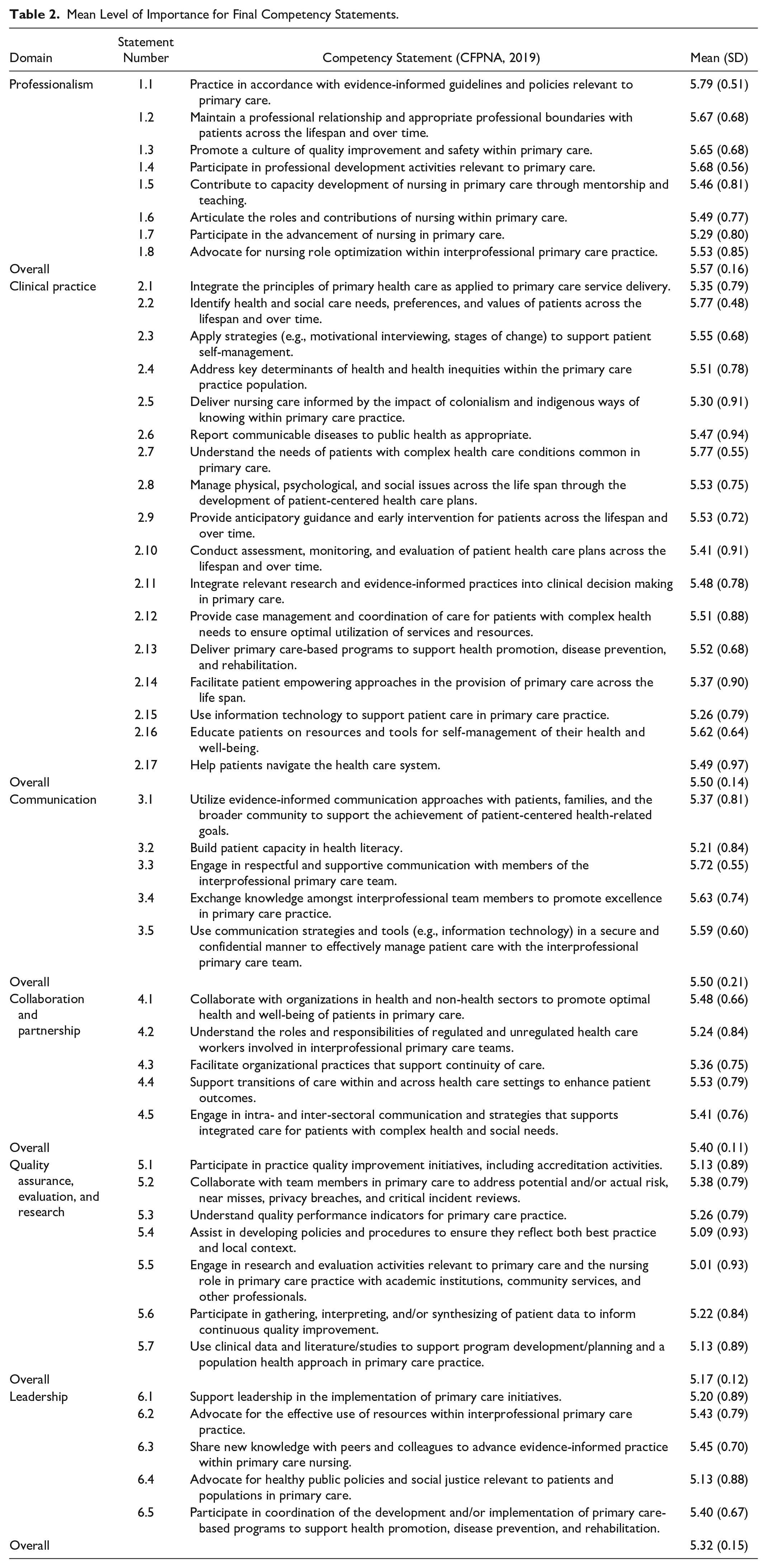
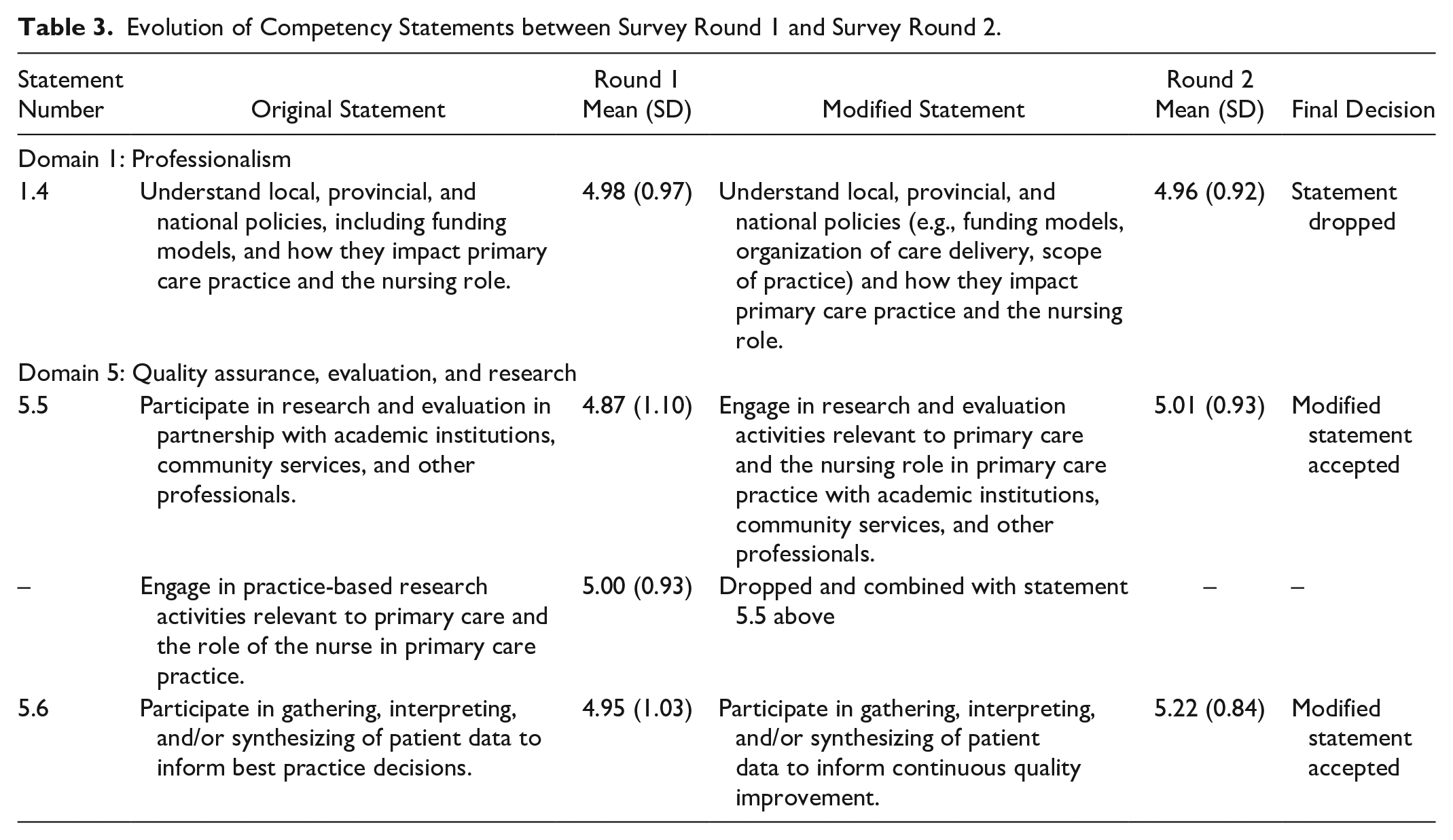
The majority (n = 45) of statements achieved agreement after the first survey. Specifically, the finalized list achieved 92% agreement by the panel (5.43 ± 0.19, range 5.01–5.79). The round 1 statement that reached the highest level of rated importance was statement 1.1, “Practice in accordance with evidence-informed guidelines and policies relevant to primary care” (Domain 1: Professionalism; 5.79 ± 0.51, Table 2). Conversely, the round 1 statement that obtained the lowest level of rated importance was statement 5.5, “Participate in research and evaluation in partnership with academic institutions, community services, and other professionals” (Domain 5: Quality assurance, evaluation, and research; 4.87 ± 1.10, Table 3). Of the 49 statements that were included in the first Delphi round, three statements did not meet consensus and one statement received a score of 5.00. These were modified (two were combined into a single statement) for inclusion in the second (final) Delphi survey round. All three modified statements reached consensus following the second round (Table 3).
Mean Level of Importance for Final Competency Statements.
Evolution of Competency Statements between Survey Round 1 and Survey Round 2.
The final competency report, prepared by the authors of this article for the CFPNA, is published online and located on the CFPNA website (CFPNA, 2019). The final list of competency statements for RNs in primary care consists of 47 distinct statements, organized across six domains (Table 2). The final number of competency statements within each domain varies: Professionalism has 8 statements, Clinical practice has 17 statements, Communication has 5 statements, Collaboration and partnership has 5 statements, Quality assurance, evaluation, and research has 7 statements, and Leadership has 5 statements (CFPNA, 2019).
Discussion
This study sought to develop competencies that support the integration and optimization of RNs in primary care across Canada. These competency statements build upon existing RN entry-to-practice competencies to reflect and articulate the unique contribution of RNs in primary care. Competencies are represented by higher level statements than specific roles, activities, or tasks. Prior to the completion of this project, a standardized set of national competencies for RNs working in primary care settings did not exist. One unique contribution that distinguishes RNs in primary care from that of other settings is the delivery of health services “across the life span” and “over time.” That is, RNs in primary care serve individuals of all ages, from “cradle-to-grave,” and form long-term, continuous relationships with patients. This element of continuity of care is reflected throughout the competency statements and assists with defining nursing scope of practice within this distinctive role. In addition, the competency domains and statements identified in this study can serve as an organizing framework for mapping nursing roles and processes. For instance, a recent systematic review conducted by Norful et al. (2017) summarized the substantial body of international literature focused on the roles and responsibilities of RNs in primary care. Roles identified included, but were not limited to, wound care, vaccinations, ear syringe irrigation, diabetic foot examinations, checking vital signs, triaging patients, newborn/infant developmental assessments, maternal education on lactation/feeding, medication administration, chart audits, post-hospitalization follow-up, cervical PAP smears, maintaining/updating clinic policies and procedures, and asthma education. The diverse roles identified within this systematic review could serve as exemplars of the identified higher level competency statements, which could benefit front-line nurses in actualizing the competencies and policy-makers who are seeking to develop models of team-based care that will maximize the contributions of RNs to patient care. Furthermore, the review identified that RNs in primary care predominantly engage in clinical care, such as medication administration, therapeutic interventions, chronic disease management (e.g., diabetes, hypertension), and patient education. This aligns with the current study’s findings that the greatest number of competency statements fall under the “Clinical practice” domain. Norful et al. (2017) also identified that RNs shift between clinical and administrative roles, such as quality assurance monitoring, performing research within the practice, and completing requested patient forms and ensuring documentation is up to date. These roles align with competencies within the “Quality assurance, evaluation, and research” and “Leadership” domains.
The identified competencies can serve as a framework for performance evaluation of these nursing roles and aid researchers and other stakeholders (e.g., employers) to generate evidence on the effectiveness of the contribution of RNs in primary care to patients and the broader health care system. To date, limited research exists to assist with the evaluation of nursing contributions in the primary health care system, specifically in terms of nursing impact on patient, provider, and/or system level outcomes. A body of emerging literature in Canada has begun to explore the impact RNs have on health promotion and care delivery within primary care settings. For example, Ammi et al. (2017) used cross-sectional Canadian survey data from the international Quality and Costs of Primary Care (QUALICO-PC) study to examine associations between patient experiences of appropriateness and accessibility of care and the role of nursing in primary care clinics. The study concluded that while no specific dimension of nursing (type of nurse, level of autonomy, numbers in clinic) was significantly associated with these outcomes, effective collaboration between health care professionals was an important predictor of patient satisfaction overall (Ammi et al., 2017). Further research is needed to examine the role of RNs in primary care both in Canada and internationally (Lancet, 2019).
Furthermore, these competencies can help shape a skilled workforce of RNs in primary care, potentially lending improvement to areas such as access to care and cost of services. Given the growing number of RNs in the primary care workforce, recent research in this subject area has demonstrated a need for undergraduate programs to specifically target this role (Poitras et al., 2018). This competency framework can support the development of specific curriculum aimed at undergraduate students to enhance the readiness of these students to work in primary care settings. Clearly defined national competencies can also assist with the integration of this role by aiding employee recruitment through the formation of job descriptions, interview guides, and the use of orientation tools and other relevant materials (Halcomb et al., 2016). A set of standardized competencies will serve as a framework to develop a clearly defined scope of practice and assist with the removal of any ambiguity that currently surrounds the role (Freund et al., 2015). This will allow RNs to practice to their full potential in the primary care setting, optimizing interprofessional team functioning and the delivery of high-quality primary care services to patients across the lifespan, including those with complex health conditions and other vulnerable/disadvantaged populations.
Importantly, this study may help shape the development of similar competencies internationally (CNA, 2014; Freund et al., 2015; RNAO, 2012). The development of national competencies for RNs in Canada has the potential to catalyze similar research across the globe that will facilitate further integration of RNs in primary care. For instance, other countries may build upon this work to develop their own defined set of competencies for RNs in primary care that align with their own context (e.g., legislated scope of practice, standards of practice).
It is important to recognize that future research is warranted. The research team is engaged in a number of follow-up studies to accompany the current project. First, the team will conduct a national survey to assess the extent to which Canadian undergraduate baccalaureate and post-graduate primary care nursing programs have incorporated the competencies developed in this study into their current curriculum. This can inform nursing curricula regarding content related to primary health care nursing to enhance the readiness of nursing students to work in primary care settings. Additionally, the Canadian Nurses Association is currently making progress toward integrating these competencies into the Community Health Nursing Certification examination. The team will also assess the learning needs and practices of RNs in primary care settings across Canada with regards to the developed competencies. Engaging front-line RNs in primary care will serve as a means to validate competencies and determine the extent to which they are being actualized in practice settings.
There were some notable strengths and limitations that need to be considered when interpreting study findings. In 2016, de Loë et al. conducted a systematic review that included 63 studies that used a policy Delphi method to determine the nature of its use within research, including strengths and weaknesses. The high response rate achieved in the current study (i.e., survey round #1: 63%; survey round #2: 84%) aligns with the majority of Delphi studies identified in this review and is likely a result of the purposeful selection and recruitment of participants (de Loë et al., 2016). In some jurisdictions in Canada, integration of RNs into primary care settings has proceeded more slowly than in others; therefore, some provinces/territories may be more highly represented than others. For example, Nova Scotia formally introduced RNs into primary care over a decade ago and has an established post-graduate education program for RNs to acquire additional training in this community-based nursing area (i.e., Family Practice Nursing Education Program offered by the RN-Professional Development Centre; Registered Nurses Professional Development Centre, 2016). Thus, it is not surprising that the highest percentage of Delphi panelists were from this province. Furthermore, the final size of both Delphi panels (i.e., round #1 n = 86; round #2 n = 72) compares to what was originally proposed as appropriate for a Delphi study (i.e., 10–50 participants; Turoff, 1970). The panel in this study was slightly larger in order to capture expert opinions from all five domains of nursing practice across all jurisdictions in Canada. A limitation of the study is that not all invited participants proceeded to complete the survey, which could result in some level of response bias and impact generalizability of findings. There was also some degree of participant attrition between the first and second round; however, this number was small, and analysis determined that there were no significant differences in the characteristics of the two groups. This project is strengthened by the use of an iterative Delphi approach, which allowed for ongoing input from a national multidisciplinary team of researchers and key knowledge users in health care and policy. The Delphi survey was completed by a panel comprised exclusively of nurses with knowledge, expertise, and/or experience in primary care settings from across Canada. Future research will validate these competency statements across different models/contexts of primary care.
In summary, the integration of RNs in primary care is essential for the development and evolution of professional practice environments that support high-quality care. National competencies for RNs in primary care may contribute to primary health care system transformation by clarifying the roles associated with this position, supporting interprofessional team functioning, maximizing nursing scope of practice, and providing a framework to evaluate the effectiveness of this unique and vital role.
Footnotes
Acknowledgements
We would like to acknowledge members of the expert Delphi panel who took the time to participate in the national consensus process by completing the online surveys. We would like to thank participants who attended the competency development workshop at the 2018 CFPNA Biennial Conference (Winnipeg, Manitoba) who contributed to the development of the initial draft of competency statements. We thank Nancy Murray for her help preparing the electronic survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a Canadian Institutes of Health Research (CIHR) Project Grant (#399218) and contributions from the Canadian Nurses Association, Canadian Family Practice Nurses Association, and Canadian Association of Schools of Nursing.