
Abstract
Aim:
This cross-sectional study explored the relationships among perceived stress, social support, positive coping, and mental health in frontline nurses caring for patients with COVID-19 in China.
Design:
A quantitative cross-sectional study.
Methods:
A convenience sample of 339 eligible frontline nurses was identified from a designated hospital for COVID-19 in Shanghai, China, between May 2022 and August 2022. Data from nurses were collected through an online survey that contained 4 measurement domains: perceived stress, social support, coping strategies, and mental health. Path analysis was used to analyze the data in SPSS 24.0 and AMOS 23.0.
Results:
The model tested in the path analysis fit the data well. The results demonstrated relationships among perceived stress, social support, positive coping, and mental health among frontline nurses caring for patients with COVID-19. Social support had a positive effect on positive coping strategies and a negative effect on perceived stress and mental health. In addition, path analysis indicated that social support moderated the relationship between perceived stress and mental health in nurses.
Conclusions:
Nurses experienced work-related mental stress while providing COVID-19-related care. Based on study findings, social support is expected to play a key role in stress management in nurses. Expanding opportunities for social support is an essential step for nurses to improve their mental health and quality of life.
The emergence of COVID-19 highlighted our lack of preparedness to manage a new pandemic due to the sudden and rapid spread of the virus worldwide. 1 Governments, along with ministries of health, have implemented various strategies to tackle COVID-19, but it remains neither controlled nor is its spread limited. 2 Health care providers are central to the control of local epidemics and have been frontline in caring for COVID-19 affected patients, especially nurses, who constitute the largest group of health care providers. 3 COVID-19 poses a considerable threat to human life and health because of its prevalence, its ability to act as a potent contagion with potential lethality, and the absence of a specific medicine for treatment other than symptomatic relief. 4 Moreover, COVID-19 ward duties, isolation, and quarantine days increase the likelihood that health care providers will be exposed to psychological perceived stress. 5 Among health workers, nurses have higher emotional disturbances and levels of perceived stress.6,7 Previous research revealed that the COVID-19 epidemic caused intense pressure and perceived stress to medical staff.8,9 Many studies have addressed the emotional problems and perceived stressors that nurses faced during the epidemic, reporting that health care providers also experienced depression and anxiety because of the COVID-19 outbreak.10-12
The association between perceived stress and mental health has been established in frontline nurses caring for patients with COVID-19.13,14 As frontline nurses are more likely to be in close contact with patients with COVID-19 and tend to stay with patients for long periods of time, they are particularly vulnerable to infection and may spread the virus among colleagues and to family members. Consequently, frontline nurses have reported fear, anxiety, isolation, and discrimination from society, which has led to increases in their levels of perceived stress.10,12 In addition, nurses experienced grueling work schedules when assigned to COVID-19 units in Shanghai, China–working 42 days straight–with each shift lasting 8 hours with a 1-hour break. During their work period, nurses were asked to live on the hospital campus, after which they were dismissed for a 14-day self-quarantine period. Under these high-pressure and extraordinary circumstances, many nurses reported a variety of psychological problems.7,12
In addition to the impact of COVID-19 on nurses’ mental health, coping strategies were also adjusted in response to evolving situations.13-15 Coping strategies have been shown to mediate the relationship between perceived stress and mental health.16,17 Coping is a psychological process that is focused on a person’s own interpretation of their situation and refers to the strategies and efforts employed by individuals to manage and adapt to the perceived stressors that they encounter.18, 19 Higher levels of perceived stress lead individuals to employ coping strategies to manage or alleviate stress; responses may include both adaptive and maladaptive coping responses. 20 Adaptive coping strategies that address underlying stressors and promote adaptive functioning are associated with better mental health outcomes. 20 Coping strategies mediate the impact of perceived stress on mental health by influencing individuals’ ability to manage stressors effectively and thereby mitigate the adverse effects of stress on their mental well-being. 17
In Lazarus and Folkman’s theory of stress and coping, social support plays a crucial moderating role in the stress-coping process. 19 It involves seeking assistance, comfort, or information from others in times of perceived stress. 21 The availability of social support can influence an individual’s perception of their coping resources and provide additional sources for dealing with perceived stress. 22 Strong social support systems are associated with better mental health outcomes, whereas ineffective coping and limited social support can lead to poorer mental health. 15 Social support moderates the relationship between perceived stress and mental health outcomes by mitigating the harmful effects of stress, improving emotional regulation, enhancing coping resources, and facilitating adaptive coping strategies. 23
Studies have emphasized the role of coping strategies in COVID-19-related anxiety and mental health.14,15 However, gaps remain in examining the relationships between perceived stress, coping, social support, and mental health among frontline nurses caring for patients with COVID-19. This study uses path analysis to study how these factors have impacted nurses’ mental health during the COVID-19 pandemic.
Theoretical Model
The theoretical model used in the study was based on Lazarus and Folkman’s perceived stress and coping theory (see Figure 1). Theoretical underpinnings were used to help interpret the findings revealed during path analysis. We tested the influences of nurses’ perceived stress and coping on their mental health and the moderating effect of social support on the relationship between perceived stress and mental health. Path analysis was employed to validate the hypothesized connections among mental health, social support, perceived stress, and negative coping: (1)
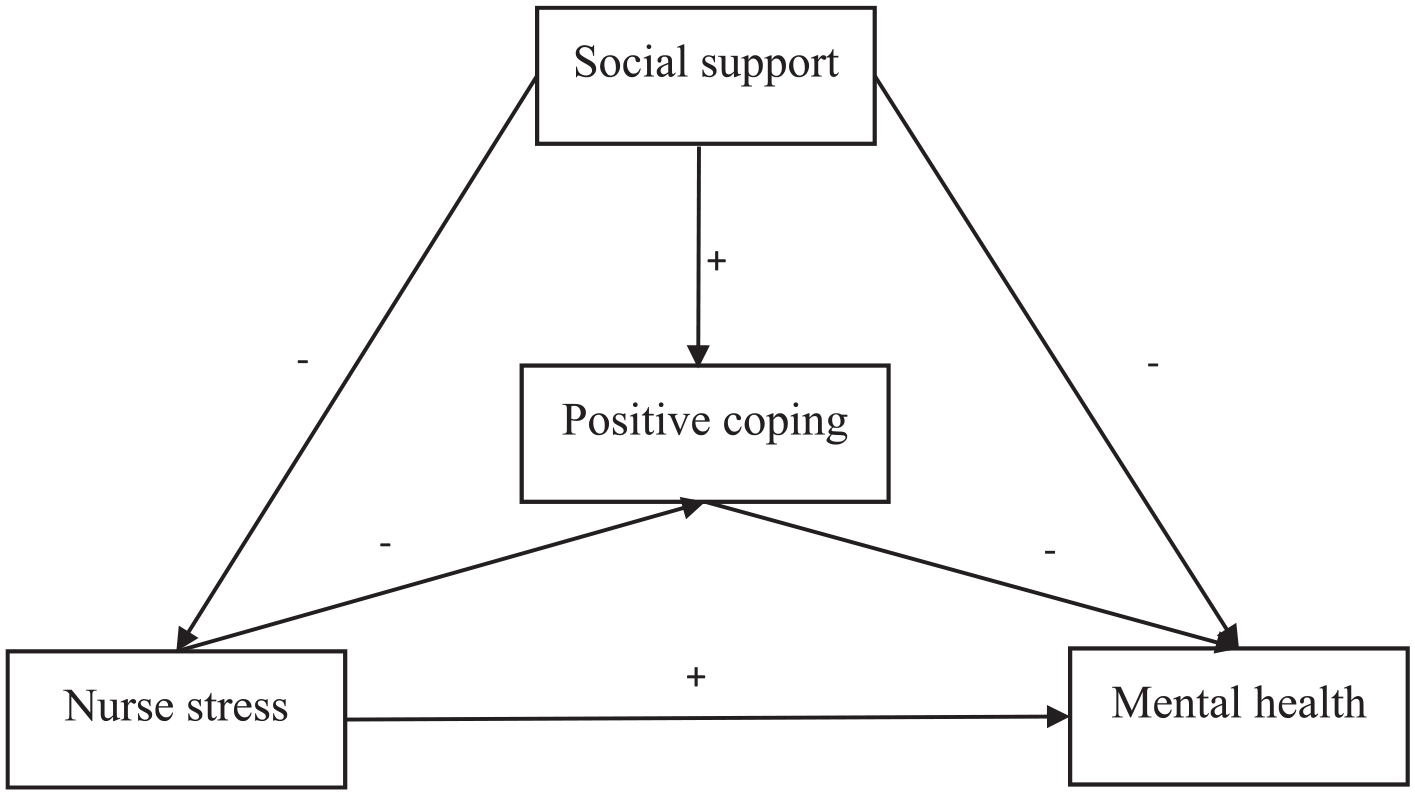
Hypothesized pathway.
Purpose
The aim of this study was to examine the relationships among perceived stress, social support, positive coping, and mental health in frontline nurses caring for patients with COVID-19 in China.
Methods
Design
The study was conducted using a quantitative cross-sectional survey design. Study reporting followed the Strengthening the Reporting of Observational Studies in Epidemiology statement. 24
Study Setting and Sample
This cross-sectional study was conducted from May 2022 to August 2022 at a designated hospital for infectious disease care that included infections caused by COVID-19. Confirmed COVID-19 cases were sent to this facility for quarantine. The nurses assigned to the COVID-19 ward came from different departments and took turns providing care in the COVID-19 ward. The work cycle lasted 56 days and included 42 days of 8-hour shifts followed by 14 days of self-quarantine. During the work period, nurses were not allowed to leave the hospital facilities, and during the self-quarantine period, they stayed in a designated hotel.
The study was approved by the Institutional Review Board of Shanghai Public Health Clinical Center (2022-S053-01). Nurse participants were identified through convenience sampling methods. Potential participants were approached, provided with an introduction about the study, and if they were interested and eligible, they were recruited. The objectives of the study were conveyed by research staff to volunteers. Written consent forms were secured from all study participants before the study survey began. The inclusion criteria for study participation included (1) nurse working on the COVID-19 ward; (2) aged ≥ 18 years; and (3) willing to volunteer to complete the online survey. Nurses who did not provide care for patients with COVID-19, such as general infection control nurses, were excluded. In total, 402 qualified study participants were approached, with 339 participants completing the survey. The response rate was 84.3%.
Data Collection
To limit in-person contact during the pandemic, data collection was conducted via an online survey. Other studies have reported that the validity of online surveys is consistent with that of traditional paper-and-pencil methods. 25 In the present study, a Chinese online survey platform, Wenjuanxing (known as Questionnaire Star, which is similar to SurveyMonkey) was used for survey self-administration. The invited participants were instructed to scan a study QR code using their mobile device and to complete the study survey. The time to fill out the survey was automatically recorded by the online survey platform and was found to take between 30 and 45 minutes. The study variables included socio-demographics, perceived stress, coping strategies, mental health, and social support.
Measures
Socio-demographic characteristics
Data on participant characteristics such as age, gender, marital status, educational level, number of working years, professional title, number of working days spent in the COVID-19 ward in 2022, and emergency department work experience were collected.
Chinese nurse perceived stress scale
The Chinese Nurse Perceived Stress (CNS) Scale was developed by Li and Liu 26 and is a 35-item tool based on the nurse perceived stress scale 27 and the source of perceived stress inventory. 28 The scale covers 5 dimensions: the nursing profession and work issues (7 items), workload and time allocation (5 items), the environment and resources (3 items), patient care (11 items), and management and interpersonal problems (9 items). Each item was measured on a 4-point scale (0 = never to 3 = always). The higher the total score, the greater the level of perceived stress. The CNS Scale has shown good reliability in Chinese samples 29 and has been widely used to assess work-related perceived stress in nurses in China.30,31 The total score of the CNS Scale was used in the final analyses. The overall Cronbach alpha coefficient (α) of the CNS scale in this study was 0.958.
Social support scale
The Social Support Rating Scale (SSRS) developed by Xiao was used to measure social support. 32 The SSRS comprises 10-items that measure 3 dimensions: subjective support (3 items), objective support (4 items), and utilization of support (3 items). The item scores of the SSRS are summed to generate a total support score that ranges from 12 to 66; the subjective support score ranges from 8 to 32, the objective support score ranges from 1 to 22, and the utilization of support score ranges from 3 to 12. A higher score indicates a higher level of social support. Scores were categorized as follows: Scores <22 indicated a low level of social support, scores ranging from 23 to 44 indicated a medium level, and scores ranging from 45 to 66 indicated a high level of social support. 33 The total score of the SSRS was used in the final analyses. The SSRS has been widely used to assess social support in Chinese studies.30,34 The overall Cronbach alpha coefficient (α) of the SSRS in this study was 0.769.
Coping strategies scale
The Simplified Coping Strategies Questionnaire (SCSQ) 35 was used to assess participants’ coping strategies. The SCSQ contains 20 items, and 2 subscales: positive coping styles (12 items) and negative coping styles (8 items). Each item uses a 4-point rating scale: 0 = never, 1 = seldom, 2 = often, and 3 = always. This questionnaire has been proven to have good reliability and validity in Chinese. 35 In this study, a positive coping score was used in the path analysis. The overall Cronbach alpha coefficient (α) in this study was 0.895. The Cronbach alpha coefficient (α) of the positive coping styles subscale in this study was 0.840.
Mental health scale
The version of the Symptom Checklist-90 (SCL-90) translated by Wang was used to measure mental health outomes. 36 The SCL-90 contains 90 items, with all the items scored on a 5-point scale from 1 to 5. A higher score indicates a lower level of mental health. In this study, the dimensions of depression (13 items), anxiety (10 items), and other (sleep and diet, 7 items) were used in the analysis for a total of 30 questions. The psychometric properties of the SCL-90 subscales for depression, anxiety, and interpersonal sensitivity have been validated in a previous study. 37 In this study, the Cronbach alpha coefficient (α) for these 3 dimensions was 0.956. The overall Cronbach alpha coefficient (α) for the SCL-90 was 0.991.
Data Analysis
We conducted data analyses by employing SPSS 24.0 and AMOS 23.0 (IBM Corp, Armonk, NY, USA). Path analysis was employed to validate the hypothesized connections among mental health, social support, perceived stress, and negative coping (see Figure 1). Categorical variables are represented as percentages or proportions, whereas continuous variables are presented as means and standard deviations (SDs). Initially, the Pearson correlation analysis was performed to scrutinize the relationships among mental health, social support, perceived stress, and positive coping. Path analysis was subsequently executed using the AMOS software to assess the proposed pathways and derive unbiased estimations of the structural path coefficients. The model with the most favorable fit indices and the least amount of information was retained. Evaluation metrics such as the χ2/df, goodness-of-fit index, root-mean-square error of approximation (RMSEA), Tucker-Lewis Index (TLI), and Comparative Fit Index (CFI) were utilized to gauge the goodness of fit for our envisaged model equation. 38 The standardized coefficients were employed to make comparisons regarding the impact of an independent variable on the dependent variable, expressed as beta (β) values. Missing data were addressed through utilization of the full information maximum likelihood method and statistical significance was defined as P < .05.
Results
Demographics of the Study Sample
A total of 339 nurses in Shanghai, China, were enrolled in the study. The age range of the study participants was between 21 and 47 years (mean = 30.0 years, SD = 5.6). Most of the participants were female (n = 318; 93.8%), and many held baccalaureate degrees (n = 210; 61.9%). More than half (54.28%) of the participants were married. The average number of years spent in nursing was 8.54 years with 66.7% of the sample having less than 10 years of professional experience. Most participants, 65.5% (n = 222), did not have working experience in the infectious disease department and 33.0% (n = 112) were new to the COVID-19 ward. When the study was conducted in 2022, the average number of working days spent in the COVID-19 ward at the study site was 58 days (ranging from 1 to 181 days). The details of the participants’ demographic data are presented in Table 1.
Socio-Demographic Characteristics of Participants (N = 339).

Abbreviation: SD: standard deviation.
Missing data.
Bivariate Correlations
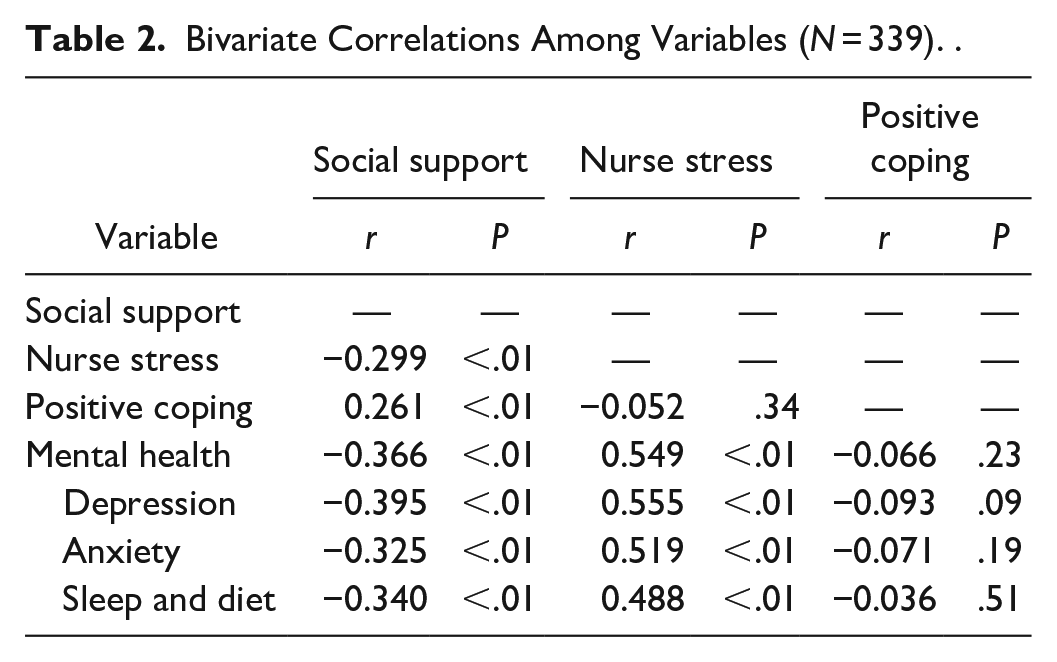
As shown in Table 2, the results of the Pearson correlation analyses suggest that social support was negatively correlated with perceived stress (r = −0.299, P < .01), negative coping (r = 0.216, P < .01), and mental health (r = −0.366, P < .05) and that perceived stress was positively correlated with mental health (r = 0.549, P < .05). However, there were no statistically significant relationships between perceived stress and positive coping (r = −0.052, P = .34) or between positive coping and mental health (r = 0.066, P = .23) in our analysis.
Bivariate Correlations Among Variables (N = 339). .
Path Analysis
Most of the hypothesized relationships were significant and were supported by the data; however, because the relationships between positive coping, mental health, and perceived stress were not significant (Table 2), we further suppressed these relationships to zero and evaluated the structural relationship of the model again. The model-fit indices of the final model also fit the data well (CMIN/DF = 2.460, RMSEA = 0.066, CFI = 0.984, TLI = 0.968). The path coefficients for all networks are shown in Figure 2.
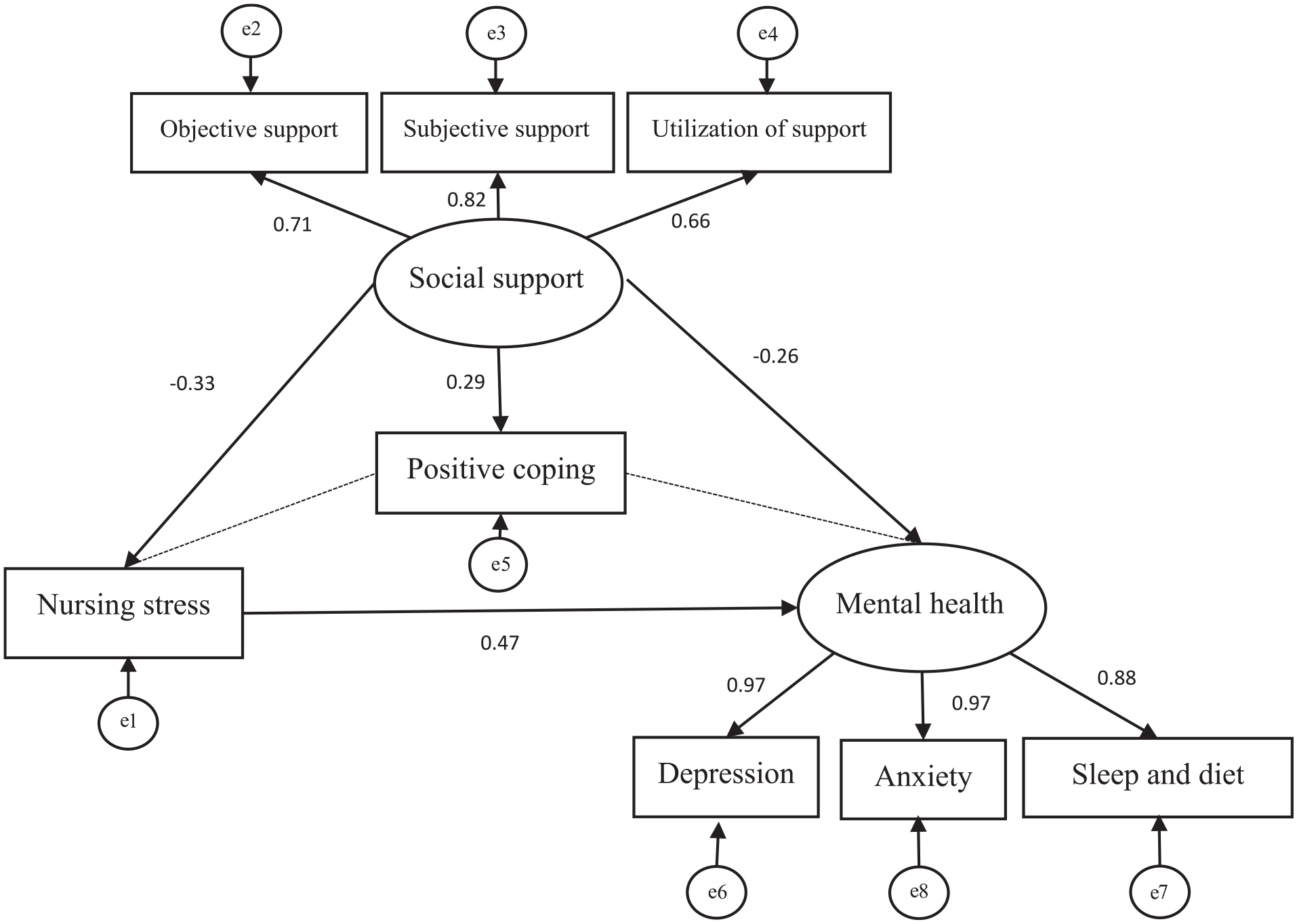
Final standardized parameter estimates model.
Figure 2 and Table 3 show the standardized direct, indirect, and total estimates of the study model. In this model, positive coping had a significant direct effect on social support (β = 0.29). In addition, social support had obvious effects on perceived stress (β = −0.33) and mental health (β = −0.25). Moreover, perceived stress had direct effects on mental health (β = 0.47), which can be moderated by social support.
Coefficients of the Path Analysis (N = 339).
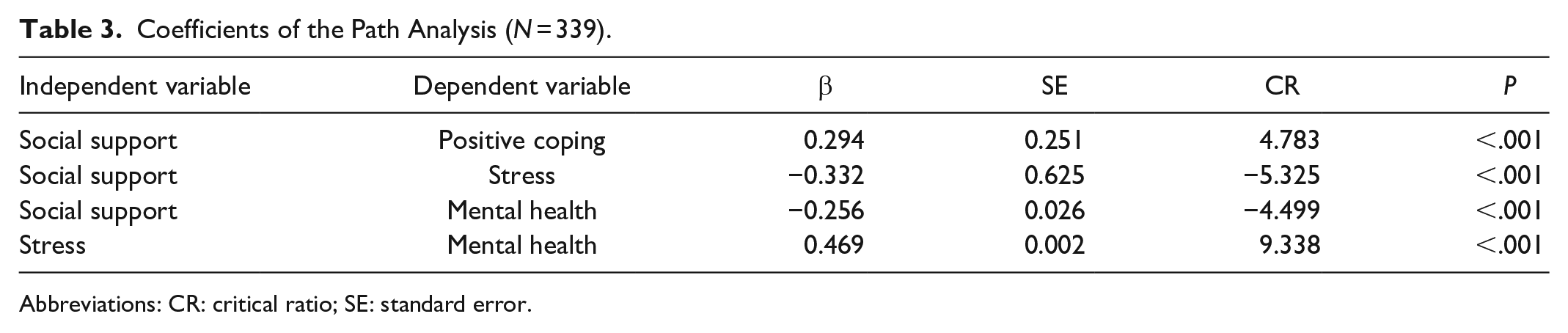
Abbreviations: CR: critical ratio; SE: standard error.
Discussion
The primary aim of this study was to investigate the interplay between perceived stress, social support, positive coping, and mental health among frontline nurses caring for patients with COVID-19 in China. The findings of this study confirmed that social support moderates the relationship between perceived stress and mental health. Additionally, social support has significant effects on positive coping strategies among nurses in Shanghai, China. This study represents one of the first studies to explore the relationships among perceived stress, social support, coping strategies, and mental health in frontline nurses.
In the present study, the total perceived stress of frontline nurses was 68.50 ± 15.78 points, indicating that frontline nurses in Shanghai’s COVID-19 wards exhibited relatively low levels of perceived stress. This finding is notably lower than the findings reported in Li’s et al’s 39 study and Xia and Luo’s 40 study, which were conducted with Chinese nurses during the pandemic. The reason for this discrepancy could be 3-fold. First, Shanghai is a metropolitan center with a well-established health system that has sufficient medical supplies and health care providers to contend with challenges posed by the COVID-19 epidemic. Second, over the past 2 years, China has accumulated invaluable experience in combating the COVID-19 pandemic, including learning effective strategies from countries outside of Asia. Third, in our study, a total of 227 nurses (66.96%) had work experience in emergency departments (eg, COVID-19 wards, Severe Acute Respiratory Syndrome (SARS) wards) which may have contributed to the decreased levels of perceived stress among nurses working in COVID-19 wards in 2022 compared with frontline nursing experiences in 2020 and 2021.
Study data from the CNS scale revealed that the highest scores belonged to 3 dimensions: workload and time allocation, the nursing profession and work issues, and patient care. During the COVID-19 epidemic in China, the number of patients admitted to the COVID-19 ward was high. While not all patients were symptomatic, a new influx of patients was admitted daily, resulting in a substantial burden to nurses due to their demanding workloads. In the intensive care unit of the COVID-19 ward, patients presented with complex medical conditions that necessitated a high degree of professional expertise from nurses. Regardless of whether they were assigned to the general or intensive care units of COVID-19 wards, nurses consistently struggled with elevated levels of work-related perceived stress, which encompassed issues related to workload and patients’ requests. Taken together, nurse managers should allocate and manage human resources wisely to reduce workloads and decrease work-related perceived stress in their nursing staff. In addition, focus should be given to expanding the nursing team’s capabilities, with frequent opportunities to expand knowledge and skill training, especially for critical care professionals.
This study demonstrated that social support had a positive effect on positive coping strategies and a negative effect on perceived stress and mental health in nurses. This sentiment is echoed in several previous studies that reported that the greater the level of social support, the lower the perceived stress level, 41 the better the mental health, 42 and the greater the level of positive coping. 43 Additionally, path analysis revealed that social support could moderate the relationship between nurses’ perceived stress and their mental health. In this study, the level of social support of frontline nurses totaled 33.49 ± 8.31 points, indicating that nurses relied on moderate levels of social support. However, the level of social support of nurses providing care for patients with COVID-19 was found by others to be lower than that of other nurses in China. 44 This may be because COVID-19 frontline nurses experience unique working conditions when assigned to COVID-19 wards: They worked in relatively confined environments, were distanced from family and friends, and lived alone after working hours and during their self-quarantine periods. As such, these nurses were particularly susceptible to isolation effects and may have found it difficult to perceive social support under these circumstances. To address this, the social support system for frontline nurses should be actively mobilized via technology. This may be achieved by creating various digital platforms to enhance communication and collaboration and provide mental health resources to promote improvements in overall well-being. Nurses should be encouraged to keep in touch with their families and friends to improve social support and remain connected with their community networks. The government and health care system should establish a robust social support system for these nurses, provide them with safer working conditions, and offer more financial assistance and rewards.
Limitations
There were several limitations to this study. First, the COVID-19 policies and resources available in Shanghai may differ from those in rural areas, limiting the generalizability of the findings of this study. Second, the cross-sectional design of the study restricts the capacity for establishing causal inferences and therefore limits the depth of insight into nurses’ perceived stress, social support, positive coping strategies, and mental health. Thus, future research studies should be longitudinal in nature to examine how the relationships among these variables unfold over time. Finally, all variables used in the analysis were measured using self-report scales, which may have led to potential bias in estimating associations (eg, social desirability and recall biases). Despite these limitations, this study offers important insights for nurse managers and governments to formulate and implement responses to address the COVID-19 pandemic that better account for the needs of frontline nurses.
Relevance to Clinical Practice
Infectious disease outbreaks such as COVID-19, as well as other public health crises, can cause physical and mental stress in health care providers, in particular. Health care providers are always at the frontline of any epidemic, continuing their duties, and responsibilities throughout difficult conditions. Owing to the nature of their scope of practice, nurses carry out one of the most vulnerable occupations in the fight against pandemics. They experience a variety of psychological difficulties under high pressure and put their own health at risk while providing care. First, nurse managers should allocate and manage human resources wisely to reduce workloads and decrease work-related perceived stress in their nursing staff. In addition, focus should be given to expanding the nursing team’s capabilities, with frequent opportunities to expand knowledge and skill training, especially for critical care professionals. Second, the social support systems of frontline nurses should be actively mobilized via technologies. Nurses should be encouraged to keep in touch with their families and friends to improve social support and remain connected with their community networks. The government and health care system should establish a robust social support system for frontline nurses, improve safe working conditions, and offer more financial assistance and rewards. Finally, further research should be initiated to identify various training programs for nurses that can help them further develop emotional competency, improve stress management, and employ various coping strategies to overcome their perceived stress.
Conclusions
This study provides evidence on how the COVID-19 pandemic has affected nurses caring for patients with COVID-19 in China and explores the relationships among nurses’ perceived stress, coping styles, social support, and mental health. This study shows that nurses experienced work-related mental stress while providing care to patients with COVID-19. Moreover, social support can play an important role in stress management in nurses and the findings suggest that improving social support can be beneficial for improving the health of nurses.
Footnotes
Acknowledgements
We gratefully acknowledge all the study participants; without them, it would not have been possible to complete this project. We thank Leilei Li for valuable comments on the manuscript and for providing help during its revision.
Author Contributions
Wei-Ti Chen and Lin Zhang share the role of corresponding author of this study and were both responsible for designing, guiding, organizing, and planning the study. Wenxiu Sun was responsible for quantitative data analysis and manuscript writing. Lei Shen, Jing Zhang, and Rongrong Jiang were responsible for quantitative data collection. Rachel Arbing critically reviewed and edited the paper.
Data Availability Statement
The data that support the findings of this study are available from the first author, Wenxiu Sun, upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication is a result, in part, from research supported by a scientific research project of the Shanghai Municipal Health Commission (No. 20214Y0090, PI: Wenxiu Sun; No. 202240298, PI: Lin Zhang), a scientific research project of the Shanghai Nursing Association (No. 2021QN-B01; PI: Wenxiu Sun). In addition, this project was partially supported by award NIMH [P30MH058107; PI: Shoptaw, Steven J.] and NIH/FIC [R01TW012392; PI Chen, Wei-Ti].
Ethics Approval
The study was approved by the Institutional Review Board of the Shanghai Public Health Clinical Center (2022-S053-01). Participants were presented with a Participant Information and Consent Form, which they were encouraged to review thoroughly. Any questions or concerns they had were addressed before their decision to participate. Those who willingly chose to take part provided their consent in writing by signing the designated consent form. Participants were explicitly apprised that their involvement was entirely voluntary, and they retained the prerogative to withdraw from the study at any point, without any repercussions or adverse consequences.