
Abstract
Background:
Loneliness has a significant impact on the physical and psychological well-being of patients with cancer. However, the specific factors contributing to loneliness among patients with cancer within the context of Chinese culture remain poorly understood.
Objective:
The objective of this study was to identify the factors associated with loneliness among patients with cancer in China.
Methods:
A cross-sectional study was conducted using convenience sampling, involving a sample of 205 patients with cancer from a tertiary hospital in Guangzhou, China. Participants completed several validated questionnaires, including the Cancer Loneliness Scale (CLS), Hospital Anxiety and Depression Scale (HADS), Cancer-Related Negative Social Expectations Scale (C-rNSES), and Social Support Rating Scale (SSRS). Multiple linear stepwise regression analysis was employed to explore the relationships between loneliness and psychosocial factors.
Results:
The median score for loneliness among patients with cancer was 13, with an interquartile range of 8. The multiple linear stepwise regression analysis revealed that negative social expectations, social support, and depression were significantly associated with loneliness in this population. Collectively, these factors accounted for 50.1% (R2 = .501) of the variance in loneliness.
Conclusions:
The findings of this study highlight the importance of addressing negative social expectations and depression and improving social support to prevent or reduce loneliness among patients with cancer. Health care providers should consider these factors when developing interventions aimed at preventing or alleviating loneliness in this population.
Loneliness has become a significant public health concern due to its detrimental effects on physical and psychological well-being. 1 Loneliness is a feeling of isolation, characterized by a negative emotional state resulting from deficient social relations. 2 In the context of cancer, loneliness has tangible consequences for individuals, impacting their physical and psychological health. Research has demonstrated a correlation between loneliness and immune dysregulation, as well as various symptoms such as pain, depression, and fatigue. 3
Patients diagnosed with cancer are confronted with heightened vulnerability to loneliness due to the distinctive challenges arising from their illness and its treatment. The physical alterations resulting from cancer therapies, such as chemotherapy-induced hair loss, surgery-related scars, or impaired reproductive function, 4 can significantly impact self-image and give rise to heightened social stigma, ultimately fostering feelings of loneliness among individuals. 5 Furthermore, individuals with cancer often adopt coping mechanisms, such as social withdrawal and self-silencing, to navigate their illness, further intensifying their experience of loneliness. 6 Collectively, these factors contribute to the heightened prevalence of loneliness among patients with cancer.
It has been reported that nearly 50% of patients with cancer experience loneliness. 7 In addition, a meta-analysis 8 has reported that patients with cancer exhibit moderate levels of loneliness. Loneliness among patients with cancer is influenced by various psychosocial factors. Extensive research has established the significant impact of anxiety, depression, and negative social cognition (especially negative social expectations) on loneliness.9-12 Moreover, factors such as time since diagnosis, marital status, and social support have emerged as crucial determinants influencing feelings of loneliness. 8 Currently, much research about loneliness in patients with cancer has concentrated on Western countries.11,13 However, there is limited research exploring the associated factors of loneliness within the context of Chinese culture. The experience of loneliness in this population is presumed to be influenced by unique social circumstances, social understanding, and cultural norms that differ significantly between Western and Eastern countries. For example, Western cultures often prioritize open self-expression and encourage individuals to share their emotions and seek social support. 14 In contrast, Eastern cultures, including Chinese culture, emphasize the suppression of emotions and the importance of maintaining harmony within social relationships. 15 In addition, Chinese traditional life values avoid death, while the West faces death directly. 16 These cultural differences can influence individuals’ cancer experiences and psychological status (eg, loneliness), as well as their willingness to disclose and discuss their feelings. Therefore, the goal of this study is to examine the associated factors of loneliness in Chinese patients with cancer.
This study builds upon the conceptual framework of the stress process model 17 and selected literature.9,10 The stress process model 17 posits that stressors elicit responses that are influenced by mediating variables, such as cognition and social support. In the context of this study, the stressor is represented by the experience of cancer, cognition is reflected in negative social cognition (ie, negative social expectations), 12 and the response is reflected in feelings of loneliness, anxiety, and depression. In addition, some research has consistently highlighted the relationship between anxiety, depression, and loneliness, identifying anxiety and depression as factors associated with loneliness.9,10 Drawing from the stress process model and building upon previous research,9,10 this study aims to investigate the factors associated with loneliness in patients with cancer, specifically focusing on negative social expectations, social support, anxiety, and depression.
Therefore, this study aims to address the gap in the literature and investigate the relationships between anxiety, depression, negative social expectations, social support, and loneliness among patients with cancer. By understanding the interplay of these factors, medical staff can develop targeted interventions to mitigate loneliness and improve the overall well-being of individuals living with cancer.
Purpose
The primary objective of this study was to investigate and identify the specific factors associated with loneliness among patients diagnosed with cancer. By exploring these factors, we aimed to enhance our understanding of the unique challenges faced by this population and inform the development of targeted interventions to address loneliness in patients with cancer.
Methods
Participants
Patients with cancer were recruited from a public tertiary hospital in Guangzhou, China. The inclusion criteria were as follows: (1) age equal to or greater than 18 years; (2) diagnosed with cancer; and (3) ability to read, understand, and communicate in Chinese. Patients who were unaware of their disease conditions were excluded from the study.
The sample size was determined based on the recommendation of having at least 10 subjects per variable for a multiple linear regression model. 18 This study encompassed a total of 17 variables. Considering the attrition rate of 10%, the minimum required sample size was 189.
Measures
Sociodemographic and Clinical Questionnaire
A Sociodemographic and Clinical Questionnaire was administered to collect information on participants’ sociodemographic characteristics (eg, age, sex, marital status, and education level) and medical history, including the type of cancer, time since diagnosis, and cancer metastasis condition.
Cancer Loneliness Scale
The Cancer Loneliness Scale (CLS), developed by Adams et al 12 and validated in a Chinese version by Cui and Sun, 19 was used to measure the frequency of loneliness experienced by the participants. The scale consists of 7 items that assess the level of loneliness on a 5-point Likert scale, ranging from 1 (never) to 5 (always). The total scores range from 7 to 35, with higher scores indicating a greater sense of loneliness. The Chinese version of the CLS has demonstrated favorable reliability and validity, with a Cronbach alpha coefficient of 0.912. 19
Social Support Rating Scale
The Social Support Rating Scale (SSRS) developed by Xiao 20 was utilized to assess participants’ social support status. The scale consists of 10 items that encompass 3 dimensions: subjective support, objective support, and the utilization of support. The total score ranges from 12 to 66, with higher scores indicating a higher level of perceived social support.
Hospital Anxiety and Depression Scale
The Hospital Anxiety and Depression Scale (HADS), originally developed by Zigmond and Snaith, 21 was used to evaluate symptoms of anxiety and depression among patients. The scale includes a 7-item anxiety subscale (HADS-A) and a 7-item depression subscale (HADS-D). Each item is rated on a 4-point Likert scale ranging from 0 (never) to 3 (almost all the time). Scores of 8 or higher on HADS-A or HADS-D indicate the presence of anxiety or depression. The Cronbach alpha coefficients for the Chinese version of the HADS-A and HADS-D are 0.753 and 0.764, respectively. 22
Cancer-Related Negative Social Expectations Scale
The Cancer-Related Negative Social Expectations Scale (C-rNSES), developed by Adams et al 12 and validated in a Chinese version by Cui and Sun, 19 was used to assess social cognitions related to cancer and its treatment. The scale consists of five items scored on a 6-point Likert scale, ranging from 1 (strongly disagree) to 6 (strongly agree). The total score ranges from 5 to 30, with higher scores indicating more severe negative social expectations. The Cronbach alpha coefficient for the Chinese version of the C-rNSES is 0.865. 19
Procedures
Data collection took place from May 2019 to April 2021 through self-report questionnaires. Eligible participants were identified from medical records and selected using convenience sampling. Each participant received a cover letter explaining the purpose of the study and emphasizing the voluntary nature of participation. Verbal informed consent was obtained from each participant before they were provided with the self-report questionnaires. Trained investigators distributed and collected the questionnaires on-site. Sociodemographic and clinical information was obtained from participants’ medical records. All data were anonymized and accessible only to the researchers. The study was approved by the Medical Ethics Committee of Nanfang Hospital of Southern Medical University (NFEC-2020-281).
Statistical Analysis
Data were recorded using EpiData 3.0 software by 2 independent investigators. Statistical analysis was performed using IBM SPSS Statistics 26.0. Categorical variables were presented as frequencies and percentages, while continuous variables were presented as medians with interquartile ranges (IQRs) due to their skewed distribution. Nonparametric analyses, such as the Mann-Whitney U test and Kruskal-Wallis H test, were employed to compare CLS scores between different groups. Spearman correlation analysis was used to evaluate the relationships between age, time since diagnosis, social support, negative social expectations, depression, anxiety, and loneliness. Factors showing statistical significance in univariate and correlation analyses were included in the multiple linear stepwise regression analysis, with a significance level for entry set at .05 and a significance level for removal set at .10. A P value less than .05 (2-tailed) was considered statistically significant.
Results
General Information Analysis
A total of 236 patients diagnosed with cancer participated in the study, and 210 of them (89.0%) completed the questionnaire. After excluding 5 questionnaires with incomplete or missing data, a total of 205 questionnaires (86.9%) were available for analysis. The characteristics of the participants are summarized in Table 1. The median age of the respondents was 52 years (IQR: 17), and the majority of the participants were women (62.0%). The median time since diagnosis was 3 months (IQR: 11). The distribution of cancer diagnoses among the participants was as follows: urological cancer accounted for 2.4% (n = 5), hematological cancer accounted for 6.8% (n = 14), respiratory cancer accounted for 15.6% (n = 32), gastrointestinal cancer accounted for 25.4% (n = 52), reproductive cancer accounted for 44.9% (n = 92), and other systems accounted for 4.9% (n = 10).
Univariate Analysis of Loneliness in Patients With Cancer (N = 205).
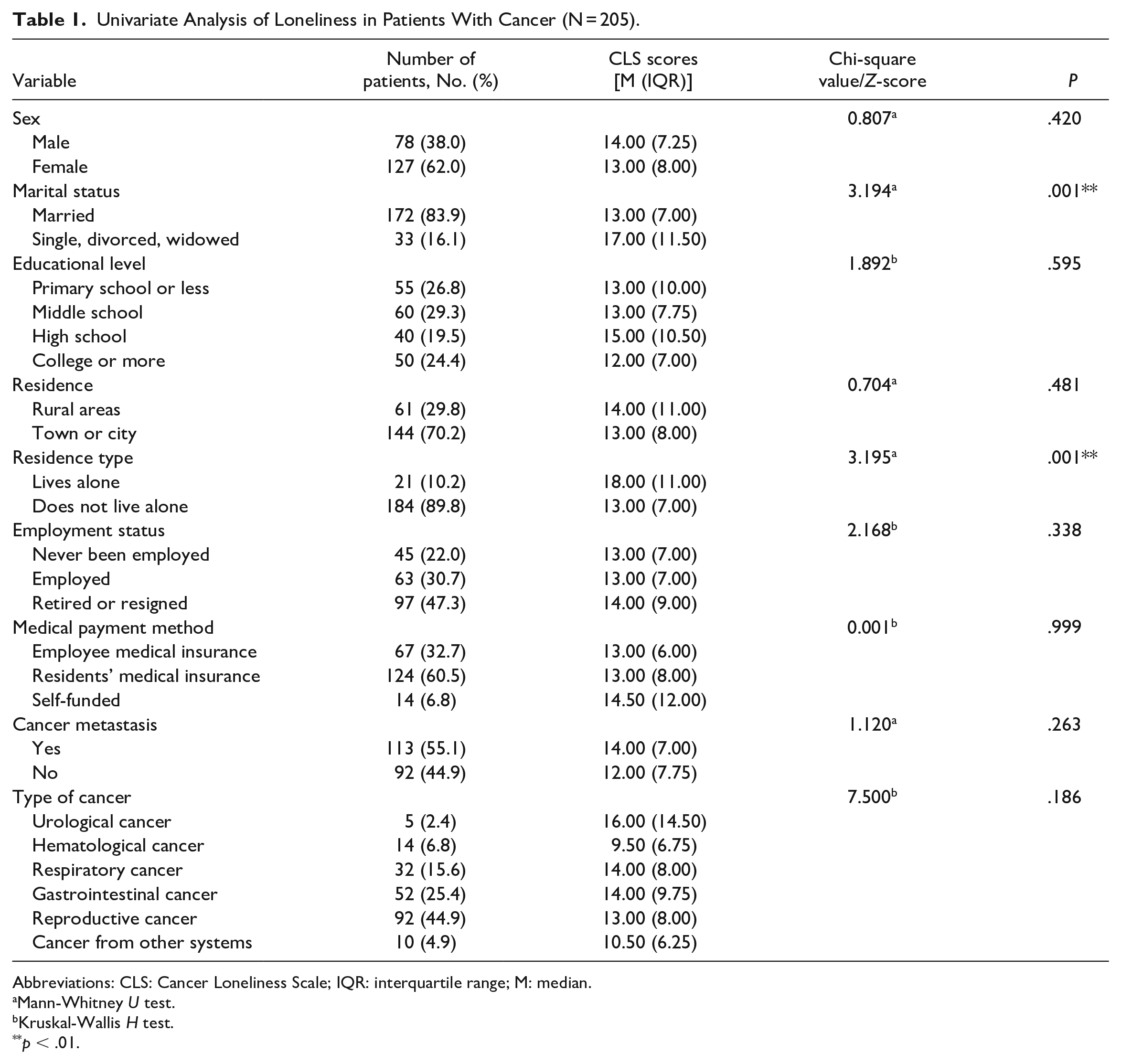
Abbreviations: CLS: Cancer Loneliness Scale; IQR: interquartile range; M: median.
Mann-Whitney U test.
Kruskal-Wallis H test.
p < .01.
Scores for Loneliness, Social Support, Negative Social Expectations, Anxiety, and Depression
Among patients with cancer, the median score for loneliness was 13 (IQR: 8). Only 15.1% of the patients with cancer reported no loneliness, while the remaining patients reported varying degrees of loneliness.
The median score for social support was 40.0 (IQR: 9.0). The median score for negative social expectations was 18.0 (IQR: 8.5). In addition, the median scores for anxiety and depression were 5.7 (IQR: 6.0) and 4.0 (IQR: 6.0), respectively. The prevalence of anxiety among patients with cancer was 27.8% (as determined by a HADS-A score of ≥8), while the prevalence of depression among patients with cancer was 21.5% (as determined by a HADS-D score of ≥8). The co-occurrence of anxiety and depression was found to have a prevalence rate of 15.1% (as determined by a score of 8 or higher on both the HADS-A and HADS-D).
Univariate Analysis
The analysis revealed significant differences in the level of loneliness based on marital status (Z = −3.194, P < .01) and residence type (Z = −3.195, P < .01). However, no statistically significant differences were observed in the other variables (Table 1). Furthermore, loneliness was found to have positive associations with depression (r = 0.566, P < .05) and anxiety (r = 0.524, P < .05). There was also a positive association between loneliness and negative social expectations (r = 0.447, P < .05), while loneliness was negatively associated with social support (r = −0.371, P < .05). Age and the time since diagnosis (months) were not found to be statistically associated with loneliness.
Multivariate Regression Analysis
The factors that demonstrated statistical significance in the univariate analysis were included in the multiple linear stepwise regression analysis. Before conducting the regression analysis, we assessed multicollinearity using the variance inflation factor (VIF). The VIF is a measure that assesses the amount of multicollinearity in a regression model by examining the correlation between independent variables. High levels of multicollinearity can distort the regression results and make the interpretation of coefficients challenging. A VIF value greater than 10 is considered indicative of multicollinearity. 23 In this analysis, the VIF values ranged from 1.10 to 2.41, indicating that multicollinearity was not a significant concern in the regression model.
The final regression model revealed that negative social expectations, social support, and depression were significant predictors of loneliness. Furthermore, the variables included in the final regression model collectively accounted for 50.1% of the variance in loneliness. This indicates that these variables when taken together explain a substantial portion of the variability in loneliness among participants. Detailed results and information regarding the significance levels and effect sizes of these predictors can be found in Table 2.
Multivariable Linear Regression Analysis of Loneliness in Patients With Cancer (N = 205).
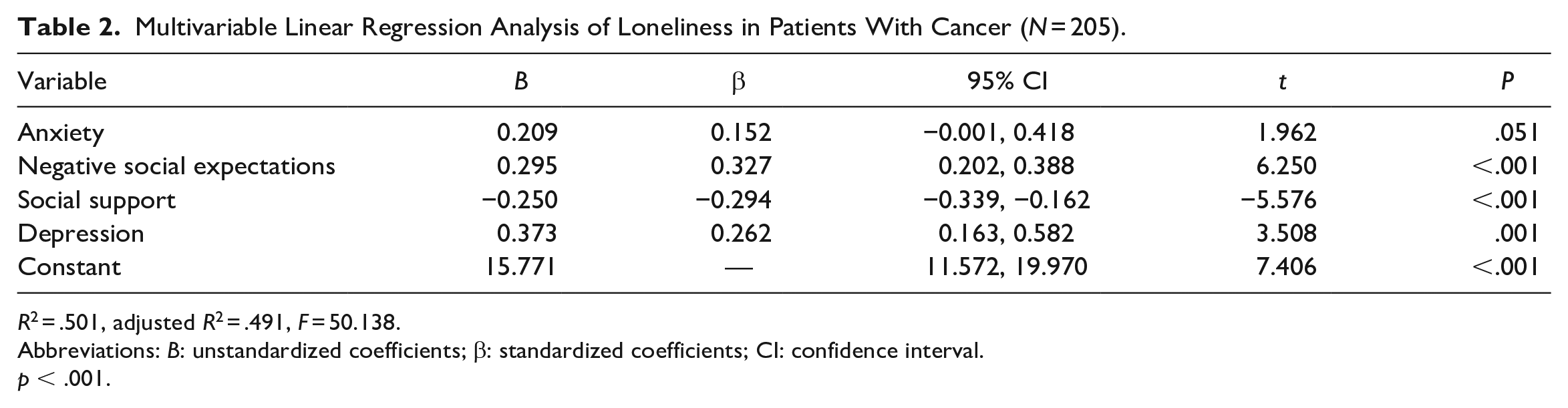
R2 = .501, adjusted R2 = .491, F = 50.138.
Abbreviations: B: unstandardized coefficients; β: standardized coefficients; CI: confidence interval.
p < .001.
Discussion
Our study highlights a high prevalence of loneliness among patients with cancer, with the majority of participants reporting varying degrees of loneliness. Only a small proportion (15.1%) indicated that they had never experienced loneliness, emphasizing the significant impact of loneliness in this population. The median score for loneliness on the CLS was 13 with an IQR of 8. The midpoint of CLS was 21, which suggests that, on average, Chinese patients with cancer experience a relatively low level of loneliness. Moreover, our findings indicate that specific factors are associated with increased levels of loneliness in this patient group. Patients with higher levels of negative social expectations, lower levels of social support, and higher levels of depression are more likely to experience greater levels of loneliness.
Negative social expectations were positively related to loneliness, which validates the stress process model. 17 Loneliness theory 24 further explains the mechanism through which negative social expectations contribute to loneliness. Negative social expectations can lead to negative interactions and perceptions of social constraints, perpetuating a cycle of loneliness. In the context of patients with cancer, negative social expectations may arise from the belief that others cannot fully comprehend or empathize with their cancer experience. 25 This perception of being misunderstood may lead patients to withdraw or refrain from discussing their thoughts and emotions related to cancer. Consequently, patients with cancer may experience isolation or separation from their social network, which in turn increases the risk of loneliness. 25
These findings highlight the importance of addressing negative social expectations in the care of patients with cancer. Promoting open communication, fostering empathy, and providing opportunities for patients to connect with others who have shared experiences can help alleviate negative social expectations. Combating negative social expectations and promoting social integration can contribute to alleviating loneliness and the overall well-being of patients with cancer.
Furthermore, our findings align with previous research demonstrating a negative correlation between social support and loneliness among patients with cancer. 26 This relationship validates the stress process model 17 and emphasizes the crucial role of social support in mitigating feelings of loneliness in this population. Cancer and its treatment can induce significant stress and emotional challenges for patients. The availability of social support from family members, relatives, and friends can serve as a protective factor by buffering the impact of stressors associated with cancer. 27 Supportive relationships provide emotional reassurance, practical assistance, and a sense of belonging, which can help individuals cope with the high-pressure events and difficulties they encounter throughout their cancer journey. In the context of family support, the acceptance and adaptability of spouses can have a significant impact on family relations. Spouses’ ability to understand and adjust to patients’ disease and physical changes, as well as their provision of substantial support, directly influences the overall family dynamic. 28 Medical staff can play a crucial role in facilitating this process by offering webinars or educational programs aimed at enhancing the acceptance and adaptability of patients’ spouses. 29 By strengthening family relations and improving support networks, feelings of loneliness can be alleviated. However, social support is not limited to the immediate family. It can also extend to the broader societal context. Unfortunately, in some areas of China and other societies, there are still prevalent stigmas and misconceptions surrounding cancer. Misguided beliefs, such as considering cancer as evil or contagious, can lead to social rejection and isolation of patients with cancer. Consequently, individuals diagnosed with cancer may choose to conceal their condition to protect their dignity and avoid social isolation and loneliness caused by stigma. 30 Addressing these societal issues requires comprehensive public education and awareness campaigns. It is crucial to educate the public about cancer as a disease, debunk myths and misconceptions, and foster a more empathetic and supportive environment. By promoting understanding and compassion, society can play a significant role in reducing the stigma associated with cancer and creating a more inclusive space for patients to receive the social support they need. Overall, our study emphasizes the importance of social support in reducing loneliness among patients with cancer. Medical staff should prioritize efforts to enhance social support systems, provide education and resources to patients and their families, and advocate for a compassionate and accepting society that empowers and supports individuals living with cancer.
Our study confirms the positive association between depression and the risk of loneliness, which is consistent with previous research findings.31,32 It may be attributed to the observation that depression is linked to physiological alterations, such as decreased energy levels and reduced participation in social activities, 33 thereby worsening the feeling of loneliness.
The prevalence of depression in our study was found to be 21.5%, indicating that depression is relatively common among patients with cancer. This highlights the importance of addressing and managing depression in the context of cancer care. The American Society of Clinical Oncology 34 recommends regular assessment of depression in patients with cancer throughout the treatment process, as identifying and effectively treating depression can have significant benefits in reducing the burden of cancer on individuals. Given the high prevalence of depression among patients with cancer and its association with increased loneliness, it is crucial for medical staff to incorporate depression assessment and follow-up into their regular clinical work. By addressing and managing depression effectively, health care providers can contribute to preventing or alleviating loneliness among patients.
Anxiety and depression commonly coexist in patients. 35 However, in our study, while anxiety showed a significant association with loneliness in the univariate analysis, it did not retain its significance in the multivariate regression analysis. This unexpected result deviates from previous studies that have reported a significant relationship between anxiety and loneliness.31,32 It is possible that other variables such as depression might have confounded the relationship between anxiety and loneliness, leading to the diminished significance of anxiety in the multivariate analysis. The correlation between anxiety and loneliness in patients with cancer needs further investigation.
Limitations and Strengths
Our study, like any research endeavor, has several limitations that should be taken into consideration when interpreting the findings. First, selection bias may have influenced our results since we conducted a single-center study using convenience sampling. To overcome this limitation, future studies should conduct a multi-center study, employ larger sample sizes, and utilize random sampling methods to ensure a more representative sample. Second, the cross-sectional design of our study restricts our ability to establish causal relationships between loneliness and its associated factors. Longitudinal studies that follow patients over time would be valuable in elucidating the temporal dynamics between these variables and providing a clearer understanding of their causal relationships. Another potential limitation is the social desirability bias that may have affected participants’ responses. As the questionnaire is collected on the spot, participants may have felt compelled to provide socially acceptable answers or downplay their experiences of negative social expectations or loneliness due to stigma. Future studies could consider implementing measures to minimize social desirability bias, for example, establishing a dedicated room for one-on-one questionnaire collection can mitigate certain biases. Despite these limitations, our study has several strengths. One notable strength is that it provides valuable reference values for medical staff working with patients with cancer. The prevalence rates of loneliness and associated factors reported in our study could serve as benchmarks for medical staff when assessing and addressing the psychosocial needs of patients with cancer. Furthermore, our study adds to the existing literature by exploring the relationship between negative social expectations, social support, anxiety, depression, and loneliness in the specific context of Chinese patients with cancer. This contributes to a more comprehensive understanding of the psychosocial factors associated with loneliness in this population.
Practice Implications
The findings of our study have important implications for clinical practice in the care of patients with cancer. Medical staff should be aware of the potential impact of negative expectations, depression, and social support on the loneliness of patients and incorporate these factors into their care strategies.
First and foremost, it is crucial to recognize and address negative expectations. Medical staff should engage in proactive and supportive communication with patients, creating an environment where patients feel comfortable sharing their thoughts and emotions related to their cancer journey. By fostering a safe and accepting environment, medical staff can help alleviate feelings of loneliness and promote a sense of connection.
Furthermore, enhancing social support is crucial in reducing the risk of loneliness among patients with cancer. Medical staff should actively involve family members, especially spouses, in the care process. Educating them about cancer, its effects, and the importance of providing emotional support and understanding can greatly enhance patients’ social support network. Webinars and educational programs can be offered to improve the acceptance and adaptability of patients’ spouses, strengthening family relations and promoting a supportive environment. 29 Public education also plays a significant role in combating loneliness in patients with cancer. Increasing awareness and understanding of cancer as a disease within society can help reduce misconceptions. It is vital to educate the public about the challenges faced by patients with cancer and encourage empathy and support. By fostering a more accepting and supportive society, we can alleviate feelings of loneliness and create a more inclusive environment for patients with cancer.
Depression, as evidenced by our study, was positively associated with loneliness, and should be a particular focus in cancer care. Collaborating with psychologists can be instrumental in providing appropriate interventions to alleviate depression, thus preventing its detrimental effects on loneliness.
Conclusions
In conclusion, our study highlights the prevalence and level of loneliness among patients with cancer and its associated factors. Health care providers should prioritize the assessment and management of depressive symptoms, negative social expectations, and social support in their care plans. By tailoring interventions to address these factors, health care providers can play a crucial role in reducing loneliness and improving the overall well-being of patients with cancer. Continued research and collaboration between health care providers, psychologists, family, and the community are essential to developing effective strategies to support patients with cancer and relieve their loneliness.
Footnotes
Acknowledgements
We are grateful to the participants for their willingness to complete the questionnaires. We acknowledge Nanfang Hospital of Southern Medical University for its support. We are grateful to the National Nature Foundation of China for its support of our research.
Author Contributions
Yawei Liu, Lin Xiao: Conceptualization, Methodology, Software, Validation, Formal analysis, Writing—review & editing, and Funding acquisition. Jingjing Lin: Software, Formal analysis, Investigation, Visualization, Data curation, Writing—original draft, and Writing—review & editing. Li Zheng: Resources and Investigation. Jun Zhang: Resources and Investigation. Lili Zhang: Project administration and Conceptualization. Yinghua Zeng: Investigation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (funding number: 72004088).