
Abstract
During the COVID-19 pandemic, older people were exposed to high levels of anxiety and stress leading to loneliness and depressive disorders. The purpose of the present study was to investigate the effects of anxiety, positive coping, perceived social support, and perceived stress on depression and loneliness among older people during the COVID-19 pandemic. This was a cross-sectional online/telephone survey. A non-probability convenience sampling method was used. Participants were 112 people aged 60 years and above, without cognitive impairment, who experienced confinement (from March 2020 onward) and had access to the internet or telephone. A path analysis model showed a direct significant effect of anxiety on both, depression (β = .68, P < .001) and perceived stress (β = .65, P < .001), as well as an indirect effect of anxiety on loneliness via perceived stress (β = .65) * (β = .40); and social support (β = −.21) * (β = −.20). The model showed adequate fit χ2(df = 4) =5.972, P = .201; RMSEA = 0.066 (0.000, 0.169), CFI = 0.992; TLI = 0.970. Anxiety had a significant effect on depressive symptoms as well as on loneliness via perceived social support and perceived stress. According to our findings, in order to reduce depressive symptoms and perceived loneliness, it is essential to develop timely interventions that decrease levels of anxiety and stress and increase levels of perceived social support in older people, particularly when there are any restrictions, physical or contextual, that prevent face-to-face contact. This can be achieved by implementing preventive community-based programs, enhancing accessibility to mental health services, and collaborating with local support groups, among others.
The COVID-19 pandemic affected older persons’ mental health, presenting a challenge for health and social systems.
Our results show the intricate and significant links between loneliness, depression, stress and social support in older adults, particularly in the context of social isolation (due to the pandemic) in the Latin American region.
This research suggests that to alleviate symptoms of depression and loneliness in older adults, it’s crucial to implement interventions that minimize anxiety and stress while fostering a sense of social connection. This is especially vital when physical or situational limitations hinder in-person interactions. Effective strategies might include improved access to mental health resources and community-based initiatives.
Introduction
The pandemic of the coronavirus disease 2019 (COVID-19) presented an unprecedented challenge to public health.1,2 Several studies have highlighted the important impact of the COVID-19 pandemic on people’s mental health, especially among older adults.3-6 Findings from the Canadian Longitudinal Study on Aging showed that older adults had twice the odds of depressive symptoms during the pandemic compared with the pre-pandemic period. Subgroups, characterized by lower socioeconomic status and poor health-related factors, experienced a greater impact. 1
In general, older adults feel lonelier, have smaller social networks, and are more isolated due to life events, such as retirement or losing loved ones. 7 In addition, living alone, loneliness, and social isolation are well-known risk factors for psychological disorders such as suicide, depression, and anxiety in advanced life. 8 Furthermore, during the COVID-19 pandemic, social isolation had effects on vulnerable populations’ mental health, including older people. 9 The World Health Organization (WHO) has released a statement raising awareness about the possible impact of social isolation on psychological well-being during the pandemic.10-12 Social isolation increased the level of anxiety and depressive symptoms in older individuals and depressive symptoms were more common in those who felt lonely and lacked social support.13-16 In addition, health-related risk factors (including loneliness), pre-existing chronic conditions, and low social participation are significant determinants of the increase in the prevalence of depressive and anxious symptoms during the pandemic.1,13,17,18 Finally, a recent study confirms the detrimental effects of social isolation on older compared with younger adults, 19 including the development of depression, anxiety, 13 and loneliness, leading to serious consequences that include functional decline, disability, and even increased mortality.1,10,14,20
Regarding the effect of anxiety on depression, Yildirim et al found that anxious symptoms significantly influenced depressive symptoms. This influence was notably stronger among older individuals aged 65 to 74, females, singles, those with insufficient knowledge about the pandemic, and those who hadn’t experienced a similar outbreak previously. 21 Furthermore, these individuals reported psychological effects such as feelings of loneliness and distress during the pandemic, which amplified their depression levels. 21 Similarly, in another study, the anxiety level of senior citizens increased during the second wave of the COVID-19 pandemic, so they became lonely, which in turn increased their distress level. 22 Some studies have shown higher levels of depressive symptoms and lower status of well-being among fearful individuals who had a higher level of concern about contracting the SARS-COV 2 virus.19,23,24 Finally, one systematic review covering several countries found that older people were psychologically affected by the pandemic, and their increased anxiety level increased their depression level. 23
In Chile, 15.6% of the population are older adults, and a rise to 20% is expected for 2025. Confinement during the COVID-19 pandemic resulted in great stress and concern for Chilean older adults. The increase in anxiety feelings as well as health problems such as memory problems, feeling down, and sleeping problems were associated with increased depressive symptoms during the COVID-19 confinement. In addition, a significant association between augmented loneliness and increased depressive symptoms was found. 25
Given the growing population of older people in Chile, it is significantly important to consider the level of depression and loneliness among Chilean older adults who experienced social isolation during the COVID-19 pandemic. The purpose of the present study was to investigate the effects of anxiety, positive coping, perceived social support, and perceived stress on depression and loneliness among older people during the pandemic of COVID-19. The findings of this study will allow a better understanding of how COVID-19 pandemic affected older people’s mental health and the importance of assessing, monitoring, and treating, after the pandemic, the variables considered in this research, in order to diminish depressive symptoms and loneliness.
Materials and Methods
Study Design, Setting and Participants
This was a cross-sectional online/telephone survey. A non-probability sampling method was used whereby participants volunteered to take part in the research, employing a voluntary response sampling approach. Between September and December 2020, the survey was originally completed by 137 respondents from the Chilean general population. Inclusion criteria were: age ≥ 60, acceptance of informed consent, and self-identification as older people. Exclusion criteria were: self-reported cognitive impairment, dementia or personality disorders, individuals who did not disclose their age (unanswered), and individuals who did not identify themselves as male or female (unknown or unanswered). After applying the inclusion and exclusion criteria, a final sample of 112 participants was selected for the path analysis.
This study was approved by the Scientific Research Ethics Committee of Hospital Clínico - Universidad de Chile, through Approval No. 044 of July 15, 2020 (No.: 1132/20).
Recruitment
Potential subjects were invited to participate in this study through various announcements using flyers posted at medical offices, primary and secondary healthcare centers, community boards, and advertisements in social networks. Data collection was carried out through an online form or telephone survey (for those potential participants who didn’t have access to the Internet), according to the participants’ preference. At the beginning of the survey questionnaire (see supplemental material), they were informed about the purpose of the study, and were asked to give their consent by checking “yes” or “no” on a box (verbal consent was given for surveys carried out by phone). Their data was processed anonymously, and they could withdraw and stop the survey at any time without any negative consequences. The data collected from each participant was stored in an electronic form. To protect the confidentiality of participants, each one of them had an ID code assigned.
Instruments
Coping strategies: BRIEF-COPE, 35 This inventory identifies the different types of coping mechanisms. The abbreviated version consists of 28 items divided into 14 coping mechanisms. The responses are coded in the following manner across all statements: 1 = I haven’t been doing this at all 2 = I’ve been doing this a little bit 3 = I’ve been doing this a medium amount 4 = I’ve been doing this a lot. It has been validated in Chile showing reliability over 0.6 in each coping mechanism and a construct validity of 4 factors. 36
Data Analyses
In order to characterize participants, descriptive analyses were performed. A theoretically driven path analysis model was carried out to study the effects of anxiety, positive coping, perceived social support and perceived stress on depression and loneliness. Data were cleaned and analyzed in Stata version 14.2 (StataCorp, College Station, TX, USA). Path analysis was chosen because it includes the complex web of relationships of a reality that is also complex. Path analysis does not require reducing the number of effects or omitting relevant associations. As an advantage, path analysis models may be understood as closer to the reality of the investigated phenomena. 37
Results
Participants
The survey was originally completed by 137 respondents (aged 60 years and above) from Chilean general population. Participants were excluded based on: rejection of informed consent (2 cases), self-reported cognitive disorder (1 case), personality disorder (2 cases), people who didn’t identify themselves as man or woman (don’t know + didn’t answer: 3 cases), people who answered they weren’t older adults 60 years or above (9 cases), people who didn’t report their age (9 cases). Some of these criteria apply to the same cases, so the number of participants was reduced to 112, and the resulting database had no missing values. Demographics are shown on Table 1. Participants had a mean age of 71 years (M = 71.7, SD = 7.44), were mainly women (81.2%), and half of them were married or living with a partner (50.8%).
Participants demographics (n = 112).

Model
Goodness of fit indexes for the path analysis suggested an adequate or close-fitting model: χ2(df = 4) = 5.972, P = .201; RMSEA = 0.066 (0.000, 0.169), pclose = 0.326; CFI = 0.992; TLI = 0.970; CD = 0.678; SRMR = 0.037. Figure 1 shows standardized coefficients and statistical significance for every path in the model. The model included 2 covariances (drawn from bivariate analyses): positive coping and perceived social support were correlated (β = .52, P < .001), and depression and loneliness were correlated, too (β = .32, P < .001). The model also presented a direct significant effect of anxiety on depression (β = .68, P < .001), but indirect effect of anxiety on depression via positive coping was statistically non-significant in this model. Effect of anxiety on loneliness was considered only via perceived social support and perceived stress. Indirect effect of anxiety on loneliness was a sum of 3 paths, all of them statistically significant: anxiety -> perceived social support -> loneliness (β = −.21) * (β = −.20); anxiety -> perceived stress -> loneliness (β = .65) * (β = .40); anxiety -> perceived social support -> perceived stress -> loneliness (β = −.21) * (β = −.17) * (β = .40). The total effect of anxiety on loneliness was 0.042 + 0.26 + 0.014 = 0.316 ≈ 0.32. In this model, anxiety had a direct effect on perceived stress (β = .65, P = P<.001), only second in size to the direct effect of anxiety on depression. Anxiety had an indirect effect on perceived stress via perceived social support (β = −.21) * (β = −.17) = 0.0357 ≈ 0.04, resulting in a total effect of anxiety on perceived stress 0.65 + 0.04 = 0.69.
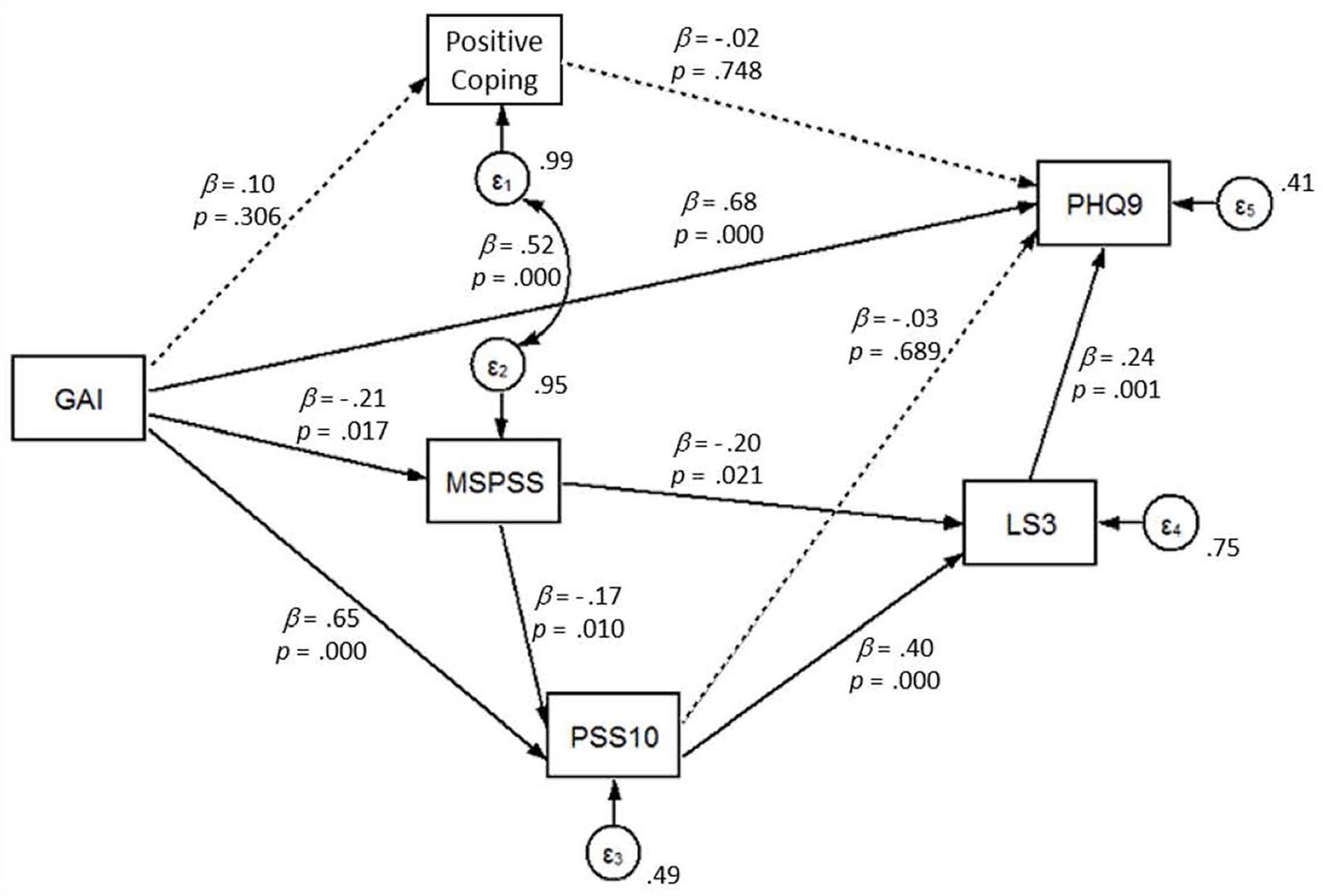
Path analysis modeling the relationships between observed variables: anxiety, positive coping, perceived social support, perceived stress, loneliness and depression.
Figure 1 shows the path analysis modeling the relationships between observed variables: anxiety, positive coping, perceived social support, perceived stress, loneliness and depression.
Discussion
During the COVID-19 pandemic, older people experienced anxiety and stress leading to loneliness and depressive disorders. As a result, psychosocial performance was compromised, affecting quality of life in this population with social support becoming even more important in this scenario of health crisis. The contribution of this study is to clarify the interaction approaches between anxiety, positive coping, perceived social support, perceived stress, depression, and loneliness among older people during the COVID-19 pandemic.
This study found a direct significant effect of anxiety on depression. Several studies have shown an association between anxiety and depressive symptoms in older people. For instance, a study conducted in the Netherlands identified that among 457 older adults with anxiety disorder, 11.6% had major depressive comorbidity, and an additional 6.3% had other depressive syndromes. 38 Another study involving 290 older adults identified anxiety as a risk factor for having depression (OR: 1.87; 95% CI: 1.57-2.22). 39 Since levels of anxiety worsened during the pandemic, it was expected to find an effect of those symptoms on depression.
The model also showed an effect of anxiety on loneliness via perceived social support and perceived stress. Social support has a protective role for lonely people which could strengthen one’s self-efficacy in coping with the uncertainty of the future. 40 The literature has shown that high and increasing levels of loneliness contributed to greater symptoms of depression and anxiety during the pandemic. 41 In addition, social support has a buffer effect on perceived stress by reducing or avoiding the triggering of a stress appraisal. 42 According to Panayiotou and Karekla, 43 perceived social support has a positive, direct effect on perceived stress—and quality of life—, but does not act as a moderator between anxiety and these 2 variables. Although mediating and moderating effects are not the same, the present study had a different result than Panayiotou and Karekla, 43 because, in our model, anxiety had both, a direct effect and an indirect effect on perceived stress via perceived social support. Thus, in our study, older people who experienced anxiety symptoms and who considered they were supported by others, were less likely to feel stressed.
Our study did not find a relationship between perceived social support and depressive symptoms, though it did identify a significant association with loneliness. This latter variable has been strongly associated with depression in older adults and in turn, greater social isolation and less social support have been found to be correlated with increased loneliness. 44 A longitudinal cohort study conducted in China investigated the associations between loneliness, social isolation, depression, and anxiety among 634 older adults. It concluded that loneliness was significantly associated with higher depression scores at follow-up. Persistent social isolation, in turn, was linked to an increased likelihood of moderate to severe loneliness and correspondingly higher depression scores. The authors of this study concluded that loneliness is a robust predictor of changes in depressive symptoms. 45 Furthermore, literature shows a positive impact of perceived social support on individuals’ psychological well-being during challenging times, particularly in buffering stress during challenging periods such as a pandemic. 46 Lastly, research focusing on a demographic group of individuals aged 50 and above identified increased feelings of loneliness, reduced physical activity, being female, and retirement status as risk factors contributing to heightened symptoms of depression and anxiety during COVID-19. 47 These findings collectively emphasize the intricate and significant links between loneliness, depression, and social support in older adults, particularly in the context of social isolation and the global pandemic.
According to our findings, anxiety plays an important role in the presence of depression and loneliness through low perceived social support and high levels of stress. Therefore, in order to prevent or decrease loneliness and depressive symptoms among older adults, it is important to address anxiety, particularly in uncertain situations like a pandemic. Evidence-based interventions identified in the literature encompass several strategies. In a recent meta-analysis, it was found that online-based interventions have proved effective in reducing general anxiety during the COVID-19 pandemic in the general population. 48 One study, carried out with older participants without cognitive impairment in nursing homes, found that internet-based cognitive behavioral therapy reduced anxiety significantly post-intervention. 49
Müller et al 10 emphasize the importance of increasing coping skills during confinement, especially for older adults who feel lonely. 10 Santini and Koyanagi 50 highlight the need for a review of public policies, and further research to understand the mental health implications of loneliness experienced during a pandemic. 50 To address the challenges of social isolation and cope with loneliness, leading health organizations, such as the World Health Organization (WHO), recommend social connection strategies. This includes the use of social networks, video calls, mobile applications and telemedicine. 51 This approach is supported by a study in Japan, where Nakagomi et al 52 found that the use of the internet for communication among older adults served as a protective factor, reducing the likelihood of depression onset.
Building upon these social connection strategies, it is also vital to consider comprehensive support. Financial measures should be combined with social support actions. 53 In particular, individuals at risk are encouraged to remain active, engage in suitable physical exercise, maintain a healthy diet, and limit their consumption and dissemination of COVID-related information. Utilizing available technological resources, such as social networks, is also recommended.23,53,54 Moreover, health authorities must adapt their organizational structures to facilitate access to mental health resources for those most in need. 55
To build upon and deepen the understanding of these findings, further research could focus on analyzing the influence of potential risk factors for loneliness, including anxiety, social support, and stress amongst the older population. The insights gained from the present study offer a foundation for such investigations, underscoring the complexity of addressing mental well-being in older adults, especially during unprecedented challenges like a pandemic.
Strengths and Limitations
To our knowledge, this is one of the few studies, carried out in Latin America, which focused on exploring older people’s mental health during the COVID-19 pandemic. This study aimed to investigate the impact of the COVID-19 pandemic on older individuals. Since there was no pre-existing data available for comparison, we were unable to determine whether anxiety, coping mechanisms, social support, perceived stress, loneliness, and depression increased, remained stable, or decreased among the older population. Our model should be tested on a longitudinal study to determine causality. In addition, a voluntary response sampling approach was used. Our sample was recruited through different strategies including distributing flyers at medical offices, healthcare centers, and community services, and utilizing online advertisements on social media. Although the sampling method and recruitment strategies were convenient and cost-effective, they might have resulted in a selection bias. Even though there was an overrepresentation of females in our sample (81.25%), a recent meta-analysis showed that, independent of age, women experienced more anxiety during the COVID-19 pandemic. 56 Additionally, this sample might not be representative of older people who are not connected with services or those who are not internet users. The limited size of our sample prevented us from conducting further analyses to examine potential variations in the outcomes according to sociodemographic factors such as age, gender, etc.
Conclusions
The main findings of this study indicated that anxiety had a direct significant effect on depression as well as on perceived stress, meaning greater anxiety symptoms predicted more depressive symptoms. In addition, the effect of anxiety on loneliness was considered only via perceived social support and perceived stress. Furthermore, social support mediated the relationship between anxiety and stress. Therefore, in order to reduce depressive symptoms and feelings of loneliness, it is essential to generate timely interventions that decrease levels of anxiety and stress and increase levels of perceived social support in older people, particularly when there are any restrictions, physical or contextual, that prevent face-to-face contact. These findings could inform public policies to create support strategies for the older adult population who present greater social isolation and loneliness. Finally, more research based on representative older people population, exploring a wide range of mental health problems, and with cohort samples are still needed to confirm causal associations.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241273187 – Supplemental material for Effects of Anxiety, Stress and Perceived Social Support on Depression and Loneliness Among Older People During the COVID-19 Pandemic: A Cross-Sectional Path Analysis
Supplemental material, sj-docx-1-inq-10.1177_00469580241273187 for Effects of Anxiety, Stress and Perceived Social Support on Depression and Loneliness Among Older People During the COVID-19 Pandemic: A Cross-Sectional Path Analysis by Maryam Farhang, Izaskun Álvarez-Aguado, Javier Celis Correa, Maria Cecilia Toffoletto, Miguel Rosello-Peñaloza and Claudia Miranda-Castillo in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors would like to thank study participants. We would also like to thank Núcleo de Estudios en Subjetividades y Políticas de Igualdad- Universidad de Las Américas, as well as Núcleo de investigacón en el cuidado integral de la comunidad y educación en salud- Universidad de Las Américas.
Author’s Note
Javier Celis Correa is also affiliated to Universidad de Artes, Ciencias y Comunicación, Santiago, Chile.
Author Contributions
M.F. is the principal investigator of this project and wrote the first draft of the manuscript, C.M.-C. contributed to the original design of the project and to the manuscript writing and revision, I. A.A., M.C.T., M. R. P., contributed to manuscript revision, J. C. C was involved in data analysis. All authors have approved the final version of this manuscript.
Data Availability Statement
The datasets used during the current study available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: M.F. received funding from National Fund for Scientific and Technological Development through the grant ANID FONDECYT 3190275 as well as Fondo Concursable Proyectos Regulares de Investigación 2022UDLA: NDI-31/22. M.F and C.M-C were supported and funded by the ANID Millennium Science Initiative Program ICS2019_024 and ICS13_005 to perform this study. Finally, C.M-C. received funding from the National Fund for Scientific and Technological Development through the grant ANID FONDECYT 1191726.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Scientific Ethics Committee of Hospital Clínico - Universidad de Chile.
Informed Consent Statement
This study was approved by the Scientific Ethics Committee of Hospital Clínico - Universidad de Chile, through Approval No. 044 of July 15, 2020 (N°: 1132/20).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.