
Abstract
Background:
People with chronic illnesses may struggle to adapt psychologically to the illness experience and have feelings of identity loss, self-diminishment, and biographical disruption. This may limit people’s ability to engage in optimal self-management. Systemic sclerosis is a debilitating, stigmatizing, and life-limiting progressive chronic illness with significant disfiguring effects. Little is known about the identity management process in people with disfiguring and debilitating conditions such as systemic sclerosis.
Purpose:
The purpose of this study was to generate a grounded theory explicating the process of maintaining a sense of self in people living with systemic sclerosis.
Methods:
Fifteen women with systemic sclerosis were recruited to ensure representation of a range of illness duration and progression. Semi-structured interviews were conducted, transcribed, and analyzed using open, selective, and theoretical coding.
Results:
A basic social process of “maintaining self” was generated from the data that explained the women’s experience of living with systemic sclerosis and how they tried to hold on to their identity. Three core categories were identified. Adapting to changes are the behaviors that participants struggled through to carry on with their everyday lives. Dismantling of self was a distressing internal process where participants lost their sense of self and purpose. Restoring self was a transformative process that allowed participants to rewrite and rebuild their biographies.
Conclusions:
Findings suggest that the management of identity was important for understanding how people adapt to life with systemic sclerosis. This study can help nurses better understand how to support patients holistically with the management of systemic sclerosis.
Keywords
Many people, young and old, experience chronic, debilitating, disfiguring, and stigmatizing conditions. Some examples include burns,1-3 disfigurement due to head and neck cancer, 4 rheumatoid arthritis,5,6 and lupus erythematosus. 7 Scleroderma (systemic sclerosis) is a rare autoimmune rheumatic disease that presents with abnormal fibrotic and collagen overproduction resulting in the hardening of the skin and primarily affects the face, hands, and fingers, which is referred to as localized sclerosis. Systemic sclerosis presents on the face and hands but progresses to the internal organs creating pulmonary, cardiac, and gastrointestinal fibrosis. 8 Systemic sclerosis is a debilitating and life-limiting progressive chronic illness that not only presents with physical disfigurement but can also have stigmatizing effects which may challenge how an individual copes or adapts psychologically.9-12 Given the profound consequences, systemic sclerosis was chosen for this study.
Nurses may have little knowledge or experience with patients who are living with a debilitating and disfiguring condition. As a relatively rare condition, patients with systemic sclerosis have expressed their wish that nurses better understood the physical and psychological effects. 11 Appearance is a major concern for individuals living with systemic sclerosis, as are the physical changes that take place, which may create problems with quality of life, stigma, depression, anxiety, fear, loss, uncertainty, and diminishment of roles.10-14 When taken together, appearance and one’s sense of self contribute to one’s sense of identity. 15
What is known about identity management in disfiguring and debilitating illnesses is that living with a chronic illness obliges one to make life changes.16-19 Identity development is instrumental to a person’s sense of purpose, self-concept, and authenticity.11,20,21 Living with a rapidly disfiguring chronic illness can create an experience of loss of self.11,12 However, even with a disfiguring chronic illness, there are moments of positive self-growth that can redefine a sense of purpose and sense of self.22,23
The purpose of this study was to explore the experiences of women living with systemic sclerosis to better understand their unique experience, with a broader purpose of contributing to the growing body of knowledge about identity management across a range of clinical conditions. In this study, we focus on women because systemic sclerosis tends to affect women at a greater rate than men. By understanding patients’ process of living with and adapting to their rare condition, nurses will be able to better care for individuals living with systemic sclerosis, incorporating realistic interventions drawn from the women’s experiences to maximize quality of life as the disease progresses.
Methods
Study Design
This study used grounded theory as a qualitative approach to generate a theoretical understanding of how women living with systemic sclerosis process their experience. Grounded theory was selected as the methodological approach because it focuses on the social process of living with and working through an experience. 24 The study was approved by the University of Wisconsin-Milwaukee Institutional Review Board (approval #18.285).
Setting and Sample
This study was conducted in a midwestern US city. The inclusion criteria for this study were (1) self identifies as a woman, (2) at least 18 years of age, (3) English speaking, and (4) reports a diagnosis of systemic sclerosis for at least 1 year. Having a diagnosis of systemic sclerosis for at least 1 year was important because many individuals struggle with the onset of symptoms, specifically Raynaud’s, which can be a symptom of several autoimmune diseases. Many participants stated that an official diagnosis took almost a year from symptom onset, diagnostic testing, and finally a diagnosis. Exclusion criteria for this study were (1) participants who lived outside the United States and (2) participants who underwent a lung or stem cell transplant. Given how rare systemic sclerosis is and the time from symptom onset to a final diagnosis, other comorbidities were not considered as exclusion criteria because the accelerated progression of systemic sclerosis can make it difficult to decipher if the comorbidities were brought on by systemic sclerosis prior to an official diagnosis or after, which would potentially make the lived experience different.
To secure a sample that could allow for a wide breadth of trajectory and clinical manifestations and given the progressive nature of the condition, purposive sampling was used to recruit participants. Originally 16 participants qualified and were recruited for this study; however, 1 participant was lost to follow-up.
Procedure
Initial recruitment was done through paper flyers that were distributed to local rheumatology clinics associated with a major academic health system. Recruitment flyers were also distributed to local sclerosis support groups. Due to low participant response (n = 5), recruitment was also done electronically through the National Scleroderma Foundation website where participants were given an email to contact the primary investigator (PI). All participants who were interested (n = 73) were screened for inclusion and exclusion criteria prior to being enrolled in the study. Interviews were scheduled based upon the participant’s availability.
The consenting process and interviews were conducted either by phone (n = 10) or in person (n = 5). Consent documents were given to the participants to read or were sent to the participant’s personal email as an attachment. In both cases, the participants were given the opportunity to ask questions about the study and the consent forms. The consents were either signed (in person) or were verbal and recorded (by phone).
Data collection consisted of a semi-structured interview composed of questions to uncover the participants’ descriptions and experiences with identity and how they managed their identity with the progression of systemic sclerosis. All interviews were collected by the PI to maintain consistency in interview style and technique. In-person interviews took place either in the participant’s home or a designated place chosen by the participant. Phone interviews took place in the PI’s closed private office. Interviews took an average of 1 to 2 hours to complete depending on the extent to which the participant was willing to share their experience.
The initial interview questions were informed by a review of relevant literature and served as a starting point for the interview conversation. During the interview, the interviewer intentionally added probing questions driven by the information and response that the participant provided. Additional probing questions were also added to later interviews as themes were identified during the comparative analysis process that necessitated additional knowledge and insights from the remaining participants (see interview guide in Supplemental Material). Study enrollment was terminated when theoretical saturation was achieved. For sample descriptive purposes, participants were asked to complete a demographics questionnaire and describe their level of skin sclerosis involvement using a self-report Modified Rodnan Skin Score, which had a range from 0 to 51, with a higher number indicating more severe skin involvement. 25
Both in-person and telephone interviews were digitally recorded using a mini hand-held recording device, transcribed by a professional transcription service, and verified for accuracy by the PI. Interviews were deidentified at the time of transcription. Participants were assigned pseudonyms to maintain confidentiality. The printed transcripts were retained in a locked file cabinet, and the electronic data files were retained in the PI’s password-protected computer.
Data Analysis
Data analysis was completed following grounded theory methods. 26 An iterative constant comparative process was used as each transcript was analyzed to identify similarities and differences emerging from the data, develop core categories, and eventually achieve data saturation. With each interview, and repeated at the conclusion of all interviews, each transcript was analyzed with line-by-line open coding and coded in the margin. The next step was selective coding, taking the concepts that were identified from open coding and synthesizing them to core categories. In the third step, theoretical coding allowed for the development of a conceptual model based on the relationships that were identified from the core categories. Memoing and field notes from each interview contributed to the data analysis.
Trustworthiness was ensured using the criteria established by Lincoln and Guba. 27 Credibility was achieved through peer debriefing where the researcher shared data with an expert in qualitative research and through member checking with later participants in the study to confirm the accuracy of the analysis and findings by reviewing the findings with the participants. Dependability was ensured by maintaining an audit trail of all data collected and the analysis, which included field notes and memos. Confirmability was achieved by having a colleague familiar with the grounded theory review the audit trail for accuracy and agreement with the data analysis process.
Results
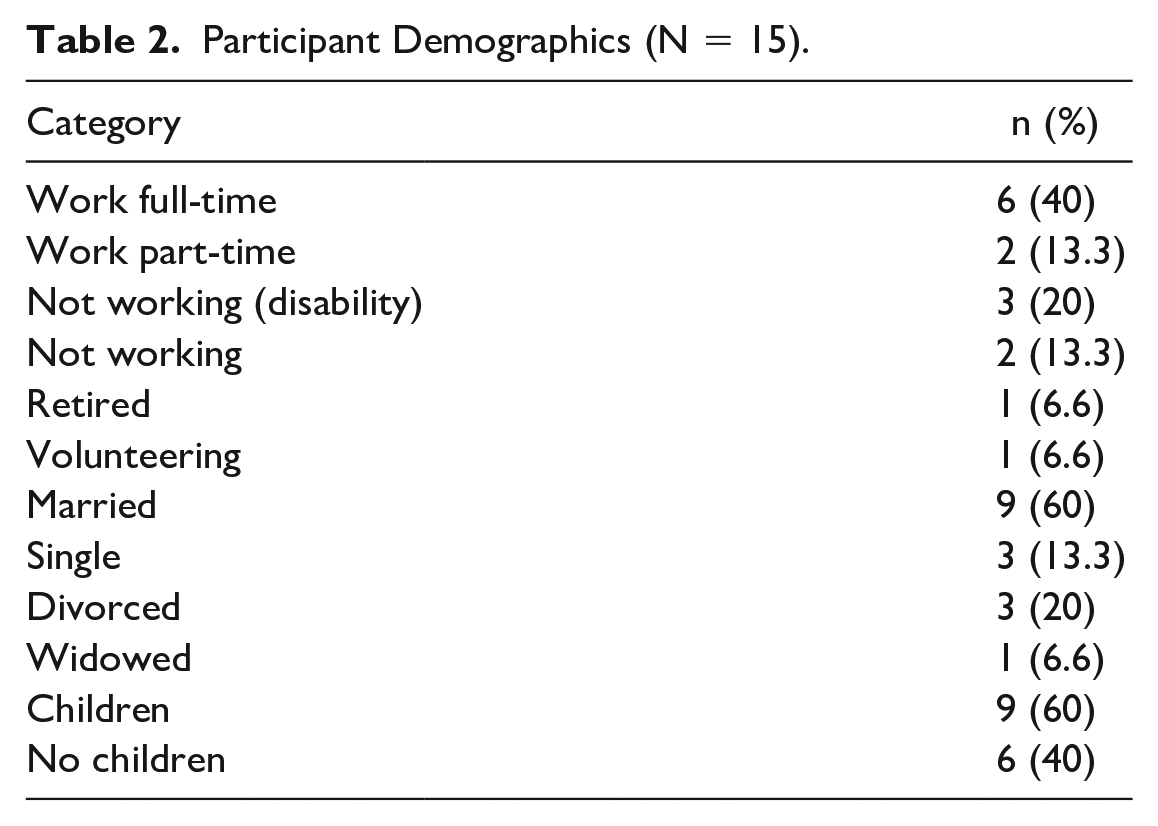
The 15 participants ranged in age from 34 to 69 years and had lived with systemic sclerosis between 1 and 15 years (Table 1). Characteristics of the sample are displayed in Table 2. Prior to the interview, participants were asked to provide a subjective self-report of their skin sclerosis using the Rodnan Skin Score assessment tool (Table 3). Primary involvement tended to be concentrated on the hands and fingers. Number of years living with systemic sclerosis and total Rodnan Skin Score demonstrated the heterogeneity of the disease and the unique individual experience of living with systemic sclerosis.
Participant Age and Years Living with Systemic Sclerosis.

Abbreviation: IQR: interquartile range.
Participant Demographics (N = 15).
Rodnan Skin Score.
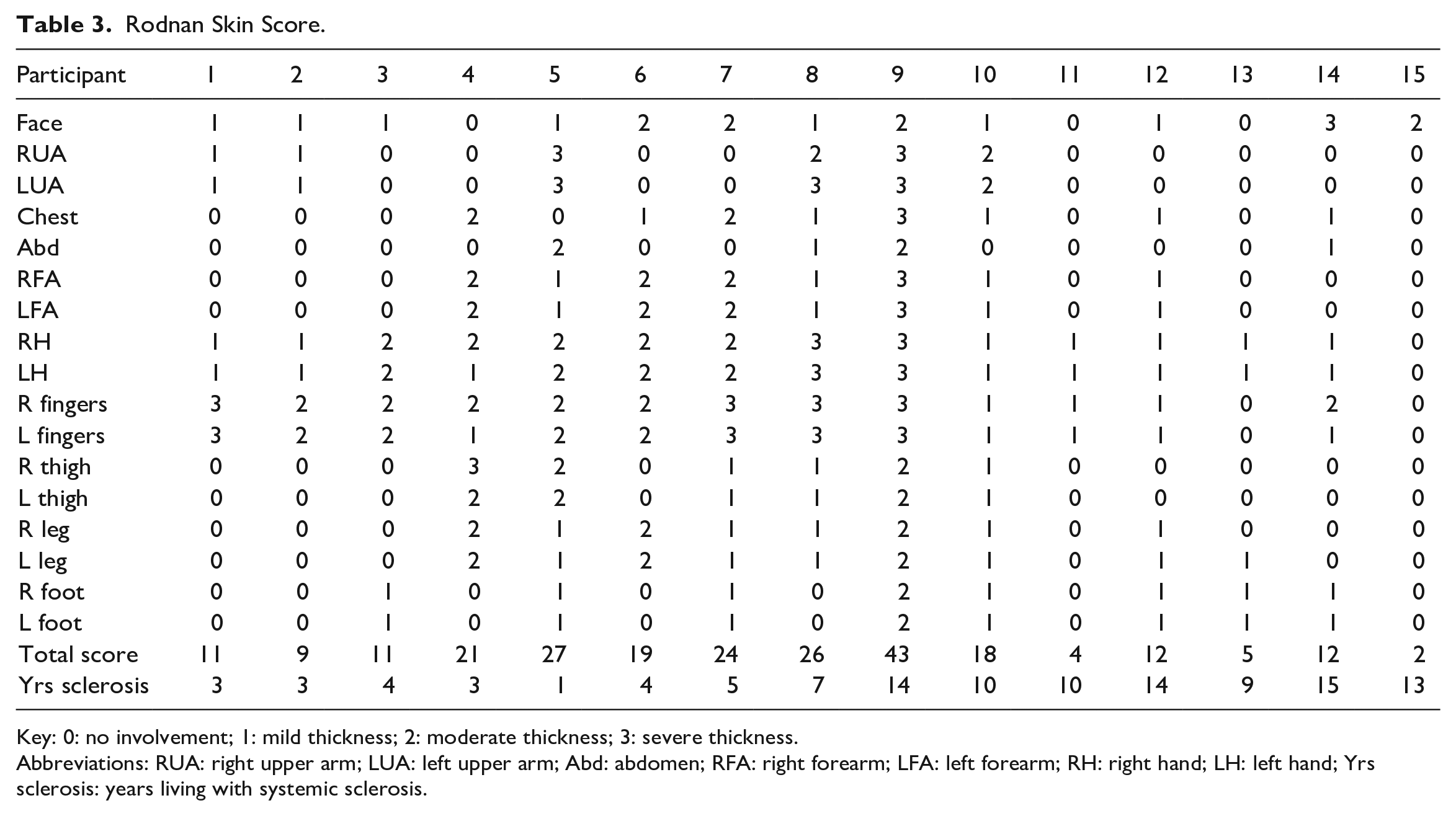
Key: 0: no involvement; 1: mild thickness; 2: moderate thickness; 3: severe thickness.
Abbreviations: RUA: right upper arm; LUA: left upper arm; Abd: abdomen; RFA: right forearm; LFA: left forearm; RH: right hand; LH: left hand; Yrs sclerosis: years living with systemic sclerosis.
Three major categories were identified from this analysis. These categories describe the phases, or steps, that the participants moved through in an effort to better understand what was happening to their bodies while simultaneously trying to safeguard self and finally accept and live with systemic sclerosis. These three categories are (1) adapting to changes, (2) dismantling of self, and (3) restoring self (Figure 1). Together they form an overarching basic social process of “maintaining self” in the presence of systemic sclerosis.
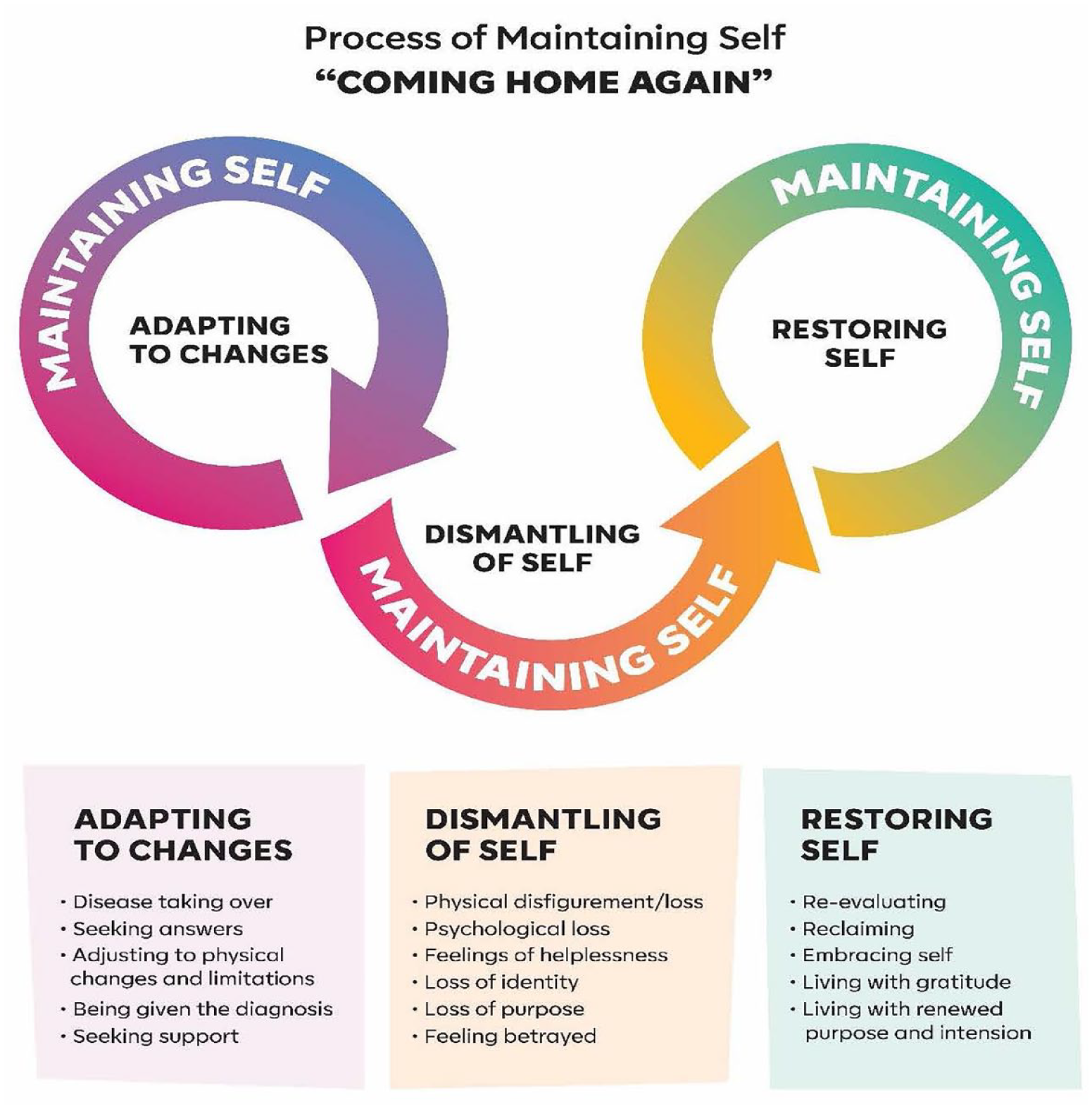
Process of maintaining self—“coming home again.”
Adapting to Changes
Adjusting to the many changes taking place in their bodies and in their lives was challenging. Many of the changes focused on how they needed to begin to limit activity and deal with the physical changes taking place within their bodies. Many perceived that the limitations decreased their overall quality of life. Learning to listen to their bodies and coming to terms with how they were changing were important factors to master.
. . . then I started counting stairs and realized that after stair number 7, I had to take a break. But it took forever just to get inside the apartment to the point where I had to request a downstairs apartment . . . I count every step. (Rebecca)
For participants who had primarily internal organ involvement, it was more difficult for people to understand why they did not have the stamina to keep going. They felt judged by others. One participant stated, “People judge that you have a broken leg or that you have Down’s syndrome, and people can see that you look different, but if it’s in the inside . . . they don’t understand.” (Melissa)
Participants with young children found it difficult to explain what was happening and why they looked different or could not even smile easily anymore: “It was very painful to hear [questions from my niece and nephew] and try and explain to a 9- or 10-year-old that I can’t smile anymore. They didn’t understand it” (Jessica).
Throughout this period, participants were also finding ways to protect their sense of self and identity. One participant stated, “I do stuff! . . . That’s kind of what I’ve been doing. I pretty much do as much as I can . . . I don’t give up” (Heather). Many participants kept living their lives and doing what they needed to do and did not see the need to worry. Although they could not hide the physical changes taking place on their face, trying to hide and move through the symptoms and not letting others see that they were in pain or discomfort was a way of holding on to the sense of self while at the same time trying to adapt to these changes. Being reluctant to ask someone for help forced participants to continue with their daily activities and keep to a routine, thus protecting their sense of self.
Dismantling of Self
Participants expressed how living with systemic sclerosis had taken away pieces of themselves that they will never get back. Dismantling of self is how many of the participants felt as they saw their bodies and life changing right before their eyes. For many of the participants, the change in their life experience was happening before it was supposed to. Systemic sclerosis stole their life and identity. Many felt like they lost the opportunity to have the life that other people of their age would have. Losing one’s identity was a major concern and an unintended consequence of living with systemic sclerosis. Brenda related, “I’ve lost a lot in my life. I feel like I’ve lost the opportunity to have the life that other people, other women my age would have.” Another participant explained that Losing one’s identity was such a big thing to the disease. It’s the emotional toll that I took when all of this happened . . . I lost identity. I lost who I was. Initially, scleroderma took away every part of my identity (Jessica).
Participants explained that their feelings of loss of self grew out of feeling useless and helpless. They felt like they were losing their purpose. Many discussed their diminishing roles and the difficulty of being present with their spouse, children, and friends and feeling dependent on others: “I’m dependent on so many people now . . . I’m mad at myself for having sclerosis” (Ruth). Some described themselves as feeling betrayed and trapped by the disease and that there was nothing they could do about it. Samantha stated, “I look like a freak. I feel unattractive . . . I feel horrible. I feel trapped by this disease. I can’t do anything. I have no confidence anymore . . . I’ve changed a lot.”
Physical changes, especially to the face, contributed greatly to their sense of loss of self. Looking in the mirror and not recognizing who you are was upsetting, and for some, disturbing: I have a different face, and for years I was . . . I don’t know her. I look in the mirror and I don’t know her. My nose is different, my lips, my cheekbones . . . When I look in the mirror, I don’t see me or the person I love . . . it’s not the face I grew up with. (Rebecca) When I look in the mirror sometimes, I want to curse the disease because I can see it changing what I look like. (Debra) I hold on to pictures so I don’t forget what I looked like. (Catherine)
Restoring Self
Restoring self was seen as a way of rebuilding and reclaiming self, and it takes place over time. Restoring self was a way of trying to bring back something that was taken away. Participants reported that they see themselves as having a physical outer self and an inner self, and both contribute to one’s identity and sense of self.
I’d say that I have a pretty strong sense of myself inside and that means more to me than what I see on the outside . . . this helps me. (Rachel) As far as my spirit, I think I still kept my spirit, my sense of humor. I’d say that I lost the part of me that was superficial. Who I am as a person . . . my identity pretty much stayed the same. (Rebecca) I found myself reaching inside . . . pulling parts of myself out that I didn’t even know I had. It feels like coming home again. (Jessica)
Restoring self was also seen as a way to finally embrace self and for participants to open up space for acceptance and for living life with intension and a renewed purpose.
I . . . I just appreciate the little things in life. I wake up and I’m happy just to get out of bed. I appreciate the day. Being grateful is amazing, and I want to help others with this disease. I have this disease, and I’m going to make the best of it. I still have so much left to offer others. (Ruth)
The Basic Social Process: Maintaining Self
Maintaining self was the basic social process encompassing phases of adapting to changes, dismantling self, and restoring self and was seen as being instrumental for someone living with systemic sclerosis. There was a strong desire to find ways in which to hold on to one’s sense of self. It was a way for someone with systemic sclerosis to hold on to who and what they knew themselves to be. Physical and social activity were important, and many continued to find ways to adapt and carry on with their daily lives. Participants tried to maintain their normal routines even if they were having a day filled with pain or physical challenges. When physical activity became limiting and at times burdensome, for example, not being able to even get out of bed some days, maintaining self unveiled itself by participants reaching inside themselves and displaying to themselves and others that who they were on the inside had not changed. This reflection was also seen as a way of restoring self. Jessica stated her view that “It’s [scleroderma] not a death sentence . . . it’s a life sentence. It has helped me find me again.” Helping and supporting others who were living with systemic sclerosis and living life with gratitude were some of the strongest characteristics of maintaining self when physical limitations were restrictive: I’ve tried not to change as much as I can so to keep my norm and keep who I am. I continue to keep doing things that I’ve always done with my kids, even if I don’t feel like it . . . maintain and holding on to the familiar. (Debra)
Discussion
Throughout this study, participants were able to discuss both positive and meaningful experiences of living with systemic sclerosis within a process of adapting to change, dismantling self, and restoring self, which ultimately led to maintaining self. Maintaining self allowed participants to hold on to their identity as much as possible while at the same time rewriting and rebuilding their biographies, leading them to live with renewed intention and purpose.
Living with a chronic illness requires one to actively construct changes in one’s life.16-19 This study revealed the many changes that women living with systemic sclerosis needed to make in order to adapt while, at the same time, finding the determination to maintain their identity.
Adapting to changes was a major challenge for individuals living with systemic sclerosis. These changes included managing a limited activity level and growing insecurities related to maintaining independence, a declining physical body, and becoming dependent on someone else. These findings are congruent with previous systemic sclerosis studies by Nakayama et al, 28 Mouthon et al, 29 and Flurey et al, 30 where many of the same concerns and themes related to losing one’s sense of self and adapting to changes were experienced. When comparing the findings from this study with the findings from Flurey et al, 30 who focused on the experience of men living with systemic sclerosis, it was clear that identity and sense of self were important for both women and men to maintain and protect. These findings are also similar to studies focusing on other chronic illnesses such as epilepsy and heart failure,31,32 which found that participants struggled with losing their independence and fear of having to live with a frail and failing body. These same concerns were clearly voiced by the participants in this study.
Participants experienced a range of signs and symptoms as systemic sclerosis progressed, to which they needed to adapt. Many expressed how frustrated they were with trying to find an answer to what was going on within their bodies. This initial frustration was focused on the lack of information they received from their physician, who often dismissed their symptoms as being minor, echoing findings of a study by Gumuchian et al 10 of individuals living with systemic sclerosis who experienced dissatisfaction navigating the health care system and the difficulty that participants had trying to communicate to their physicians about what they were experiencing. Women with heart failure expressed a lack of faith in physicians, and this lack of faith came from feeling dismissed by physicians and not being taken seriously when presenting with the same symptoms over and over again. 32 Not having a physician who understood what was going on made this experience even more frustrating.
Seeking support was a strong, positive, self-initiated intervention for coping with and living with systemic sclerosis during the process of adapting to changes. Support provided not only emotional strength but also a way to process what was happening to their bodies and within their daily lives. Being in the presence of others living with systemic sclerosis made participants feel like they were not alone and saw themselves as living similar lives. Their shared experiences provided a sense of belonging and comfort. These were similar findings expressed in both studies by Nakayama et al 28 and Flurey et al, 30 for individuals living with systemic sclerosis.
Dismantling of self can be described as a sense of breaking down. Participants in this study described how systemic sclerosis had stolen their lives and taken their identities with it. Their bodies and lives changed right before their eyes. Many described feelings of uselessness, helplessness, and betrayal. Loss quickly became a personal truth the moment participants realized their inability to manage their physical and personal lives. The chronic illness literature is abundant, with studies revealing how one’s life is disrupted by a chronic illness, especially if a chronic illness forces a person to drastically alter one’s way of life.33-36
Biographical disruption, or the feeling that there was a break in one’s planned life continuity related to roles and identity, 37 and feeling trapped by systemic sclerosis were strong feelings conveyed by many of the participants. This and other studies have revealed the connection between a person’s adaptation to the many changes necessary and their struggles with self-identity. Clarke and Bennett, 17 in their study of men and women living with multiple chronic conditions later in life, reported that individuals described their body changes and accompanying personal disruptions as undermining their sense of identity.
Restoring self was seen as a journey about reclaiming one’s identity; the journey was often a deeply reflective process that began with allowing oneself to let go of what one was still trying to hold on to, followed by re-evaluating what one still can do, and reclaiming who the person they always knew was inside. The inner self was seen as comprising one’s inner core values, personality traits, and beliefs, and for many, it remained the same. Similarly, in a study of anorexia nervosa, 38 identity and reclaiming were seen as being connected to defining a purpose and a sense of belonging. Restoring self also allowed for embracing self, which often opened up space for participants to be grateful and for them to contribute and support others living with systemic sclerosis.
The findings of this study add to the growing body of explorations related to adaptation to a chronic illness and identity disruption. Much of the recent literature exploring identity appears to be related to gender, sexual identity, and marginalized individuals.39-42 There continues to be an abundant amount of recent research exploring the connection between the psychological impact related to a chronic illness34,36,43-45; however, there continues to be a paucity of research specifically addressing the connection between identity and chronic illness, including systemic sclerosis.
Strengths and Limitations
A major limitation to this study was that it was limited to women’s experiences and did not address gender differences. Another limitation of this study was not collecting participant data on race or ethnicity, which limited understanding the contribution of race and ethnicity in the process of identity management in individuals living with systemic sclerosis. A third limitation relates to how clinically heterogeneous participants were in relation to the progression of systemic sclerosis. Living with systemic sclerosis is a unique experience for each person, and the progression of systemic sclerosis does not follow a similar or predicted path for everyone; therefore, disease activity and severity of the disease may impact adjustment to systemic sclerosis. Several participants were living with systemic sclerosis for 10 years and had little internal involvement, while others had been living with systemic sclerosis between 1 and 4 years and had significant internal involvement. The difference in the rates of disease progression may have had an impact on the process of identity management, and as a result, the findings may not be transferrable to everyone living with systemic sclerosis, making the individual’s timelines of experiences unique to the person. A final limitation is that there likely was selection bias toward participants who had achieved a positive relationship with living with systemic sclerosis. Several strengths of this study were the wide range in ages, number of years participants were living with systemic sclerosis, and national representation.
Implications for Nursing
Self-management can lead to better outcomes for people living with a chronic illness.46,47 It is clear from this study that identity is also an important component in self-managing the chronic illness experience of systemic sclerosis. Nursing is uniquely prepared and positioned as providers of direct patient care and within health care teams to not only assist with symptom management but also assist patients through the experience of learning to live with systemic sclerosis. Lessons learned from this study clearly indicate that an interdisciplinary team is needed to help patients navigate through the systemic sclerosis experience. Similar to chronic obstructive pulmonary disease (COPD) and congestive heart failure (CHF) patient education and disease management programs, there needs to be a nurse-led sclerosis program where not only patients receive education but also nurses regularly check in and follow up with patients, especially when symptoms are at their worse. Pain, fatigue, and complications related to activity are important to managing systemic sclerosis.48,49 Staying physically active is important to self-managing rheumatic diseases. 50 Nursing interventions directed at maintaining self can include asking patients to provide a list of physical activities that they enjoy along with which ones are most important to them. Having patients journal symptom experiences and then coordinate that to a time of the day that might be best to engage in physical activity could help with participation. Another intervention focused on activity would be to replace several support group meetings with physical activities, such as walking or yoga. Assisting individuals in recognizing that changes are taking place, while at the same time partnering in helping restore a sense of self, may be an effective intervention leading to better quality of life and health outcomes and to maintaining one’s identity for individuals living with systemic sclerosis.
Future studies could include developing a patient-centered navigation intervention program, which has shown to have positive outcomes among persons with Parkinson’s disease 51 and congestive heart failure. 52 Future research must include race and how race impacts the experience of living with systemic sclerosis. Findings from this grounded theory study may also serve as the groundwork for quantitative studies addressing concepts such as feelings of helplessness and reclaiming self and incorporating these into other self-management interventions focused on physical and community activities.
Conclusion
The findings in this study elucidate the process of maintaining the sense of self and identity among women with systemic sclerosis. Maintaining self allowed participants to hold on to their identity as much as possible while at the same time rewriting and rebuilding their biographies, leading them to live with renewed intention and purpose. When caring for systemic sclerosis patients, it is important for nurses to keep in mind how important identity is to one’s sense of self, and nurses should actively pursue interventions that help to maintain self.
Supplemental Material
sj-docx-1-wjn-10.1177_01939459231214600 – Supplemental material for Process of Maintaining Self in Individuals Living With Systemic Sclerosis: A Grounded Theory Study of American Women
Supplemental material, sj-docx-1-wjn-10.1177_01939459231214600 for Process of Maintaining Self in Individuals Living With Systemic Sclerosis: A Grounded Theory Study of American Women by Donald Miller and Jennifer Doering in Western Journal of Nursing Research
Footnotes
Acknowledgements
We want to thank all the brave women who willingly wanted to share their experience of living with systemic scleroderma. It was an honor to be able to give voice to your experience. We also want to recognize the National Scleroderma Foundation for their support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding awarded through the Harriet H. Werley Award for Nursing Research 2017 from the Research Committee of the College of Nursing, The University of Wisconsin—Milwaukee.
Ethical Approval
The study was approved by the University of Wisconsin–Milwaukee Institutional Review Board (approval #18.285).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.